

Effect of Sevoflurane on the Proliferation of A549 Lung Cancer Cells
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Preparation and Culture
2.2. In Vitro Study
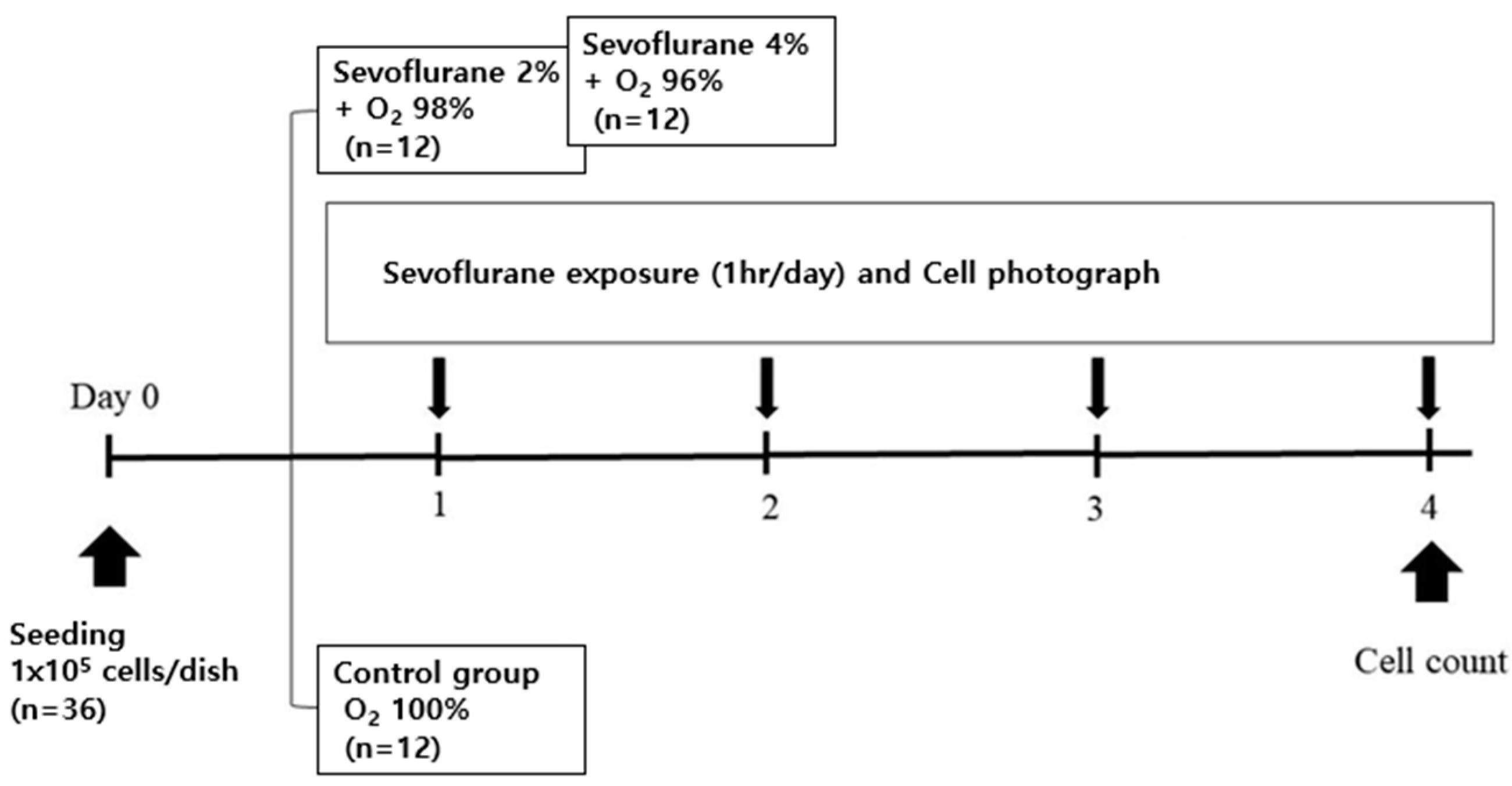
2.2.1. Sevoflurane Exposure with Oxygen (Figure 1)

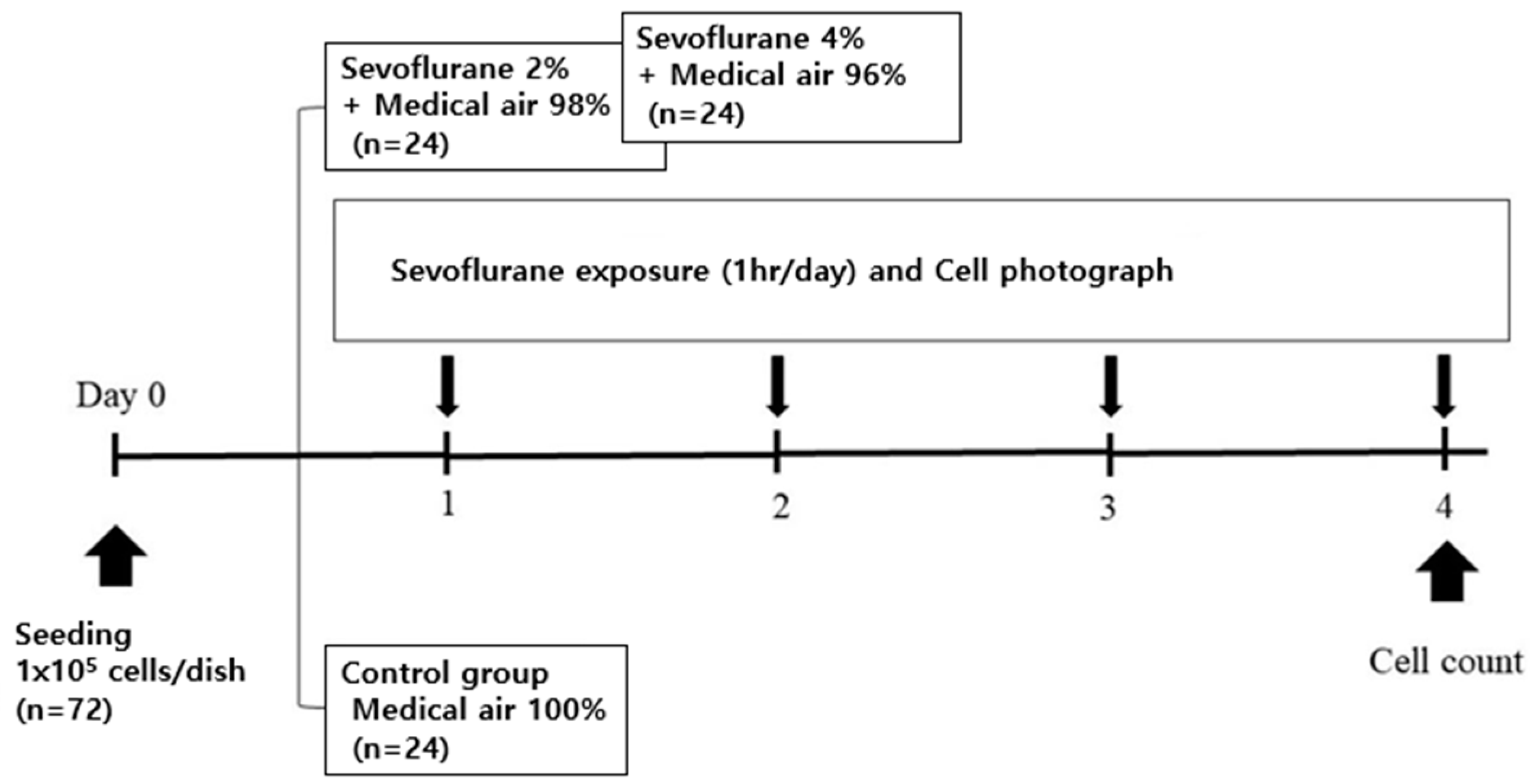
2.2.2. Sevoflurane Exposure with Air (Figure 2)

2.2.3. Cell Viability Analysis
2.3. In Vivo Study
2.3.1. Animal Preparation
2.3.2. Xenograft Mouse Model
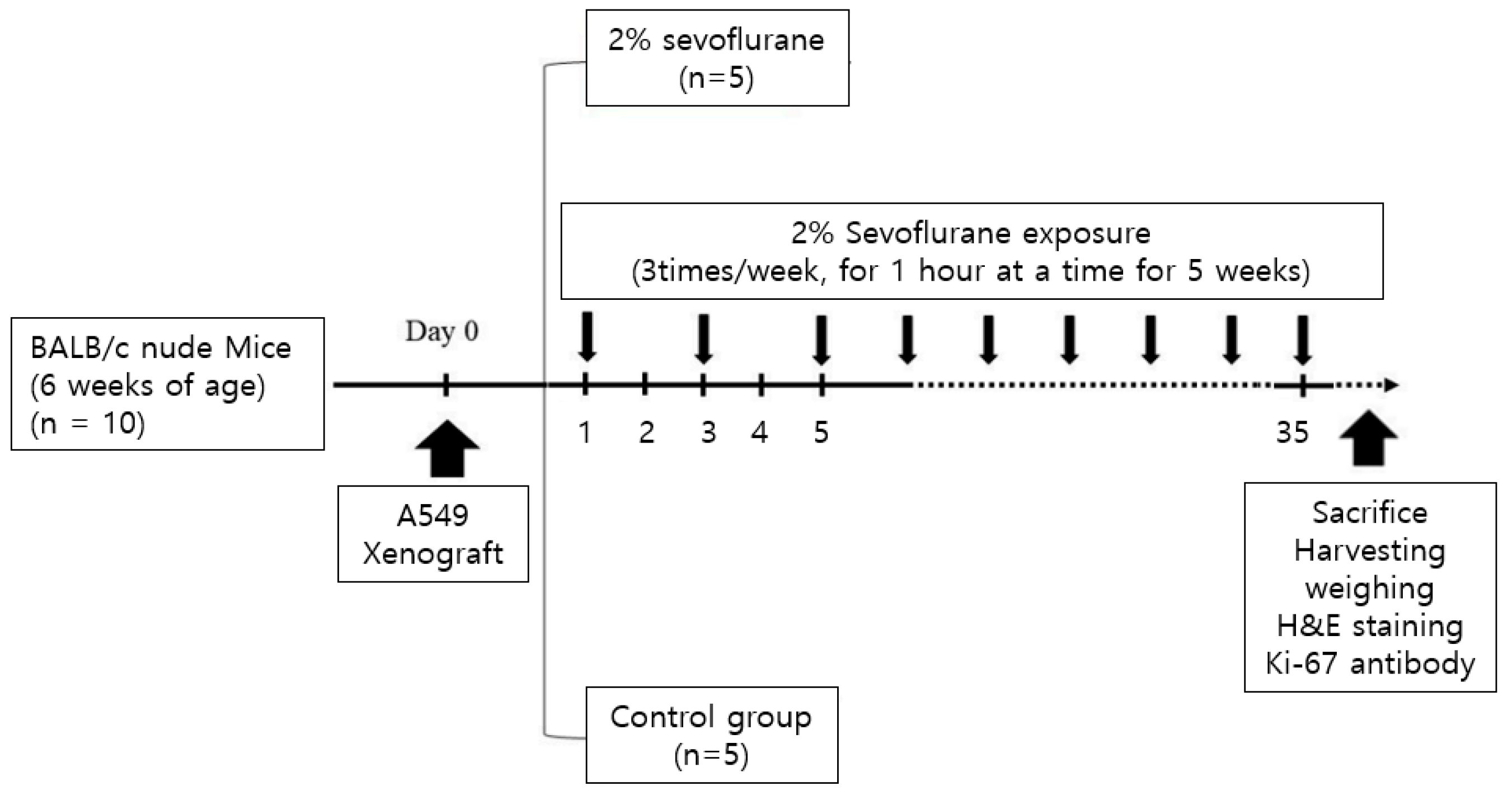
2.3.3. Sevoflurane Exposure with Air (Figure 3)

2.3.4. Measurement of Tumor Size and Mouse Weight
2.3.5. Sacrifice, Harvesting, and Weighing the Resected Mass
2.3.6. Hematoxylin and Eosin Staining and Immunohistochemistry Cell Preparation
2.3.7. Analysis of H&E Staining and Ki-67 Immunohistochemistry
2.4. Statistical Analyses
3. Results
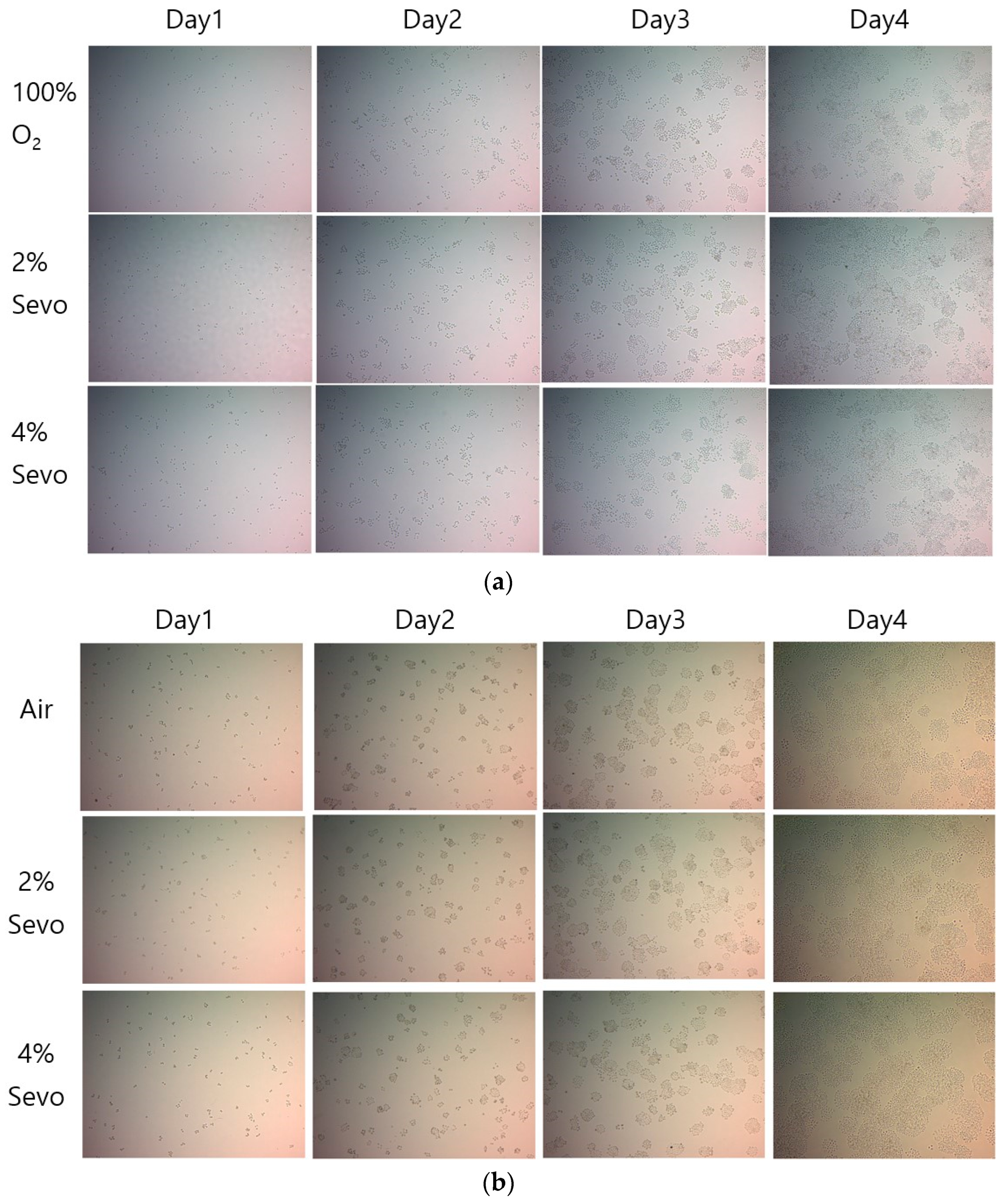
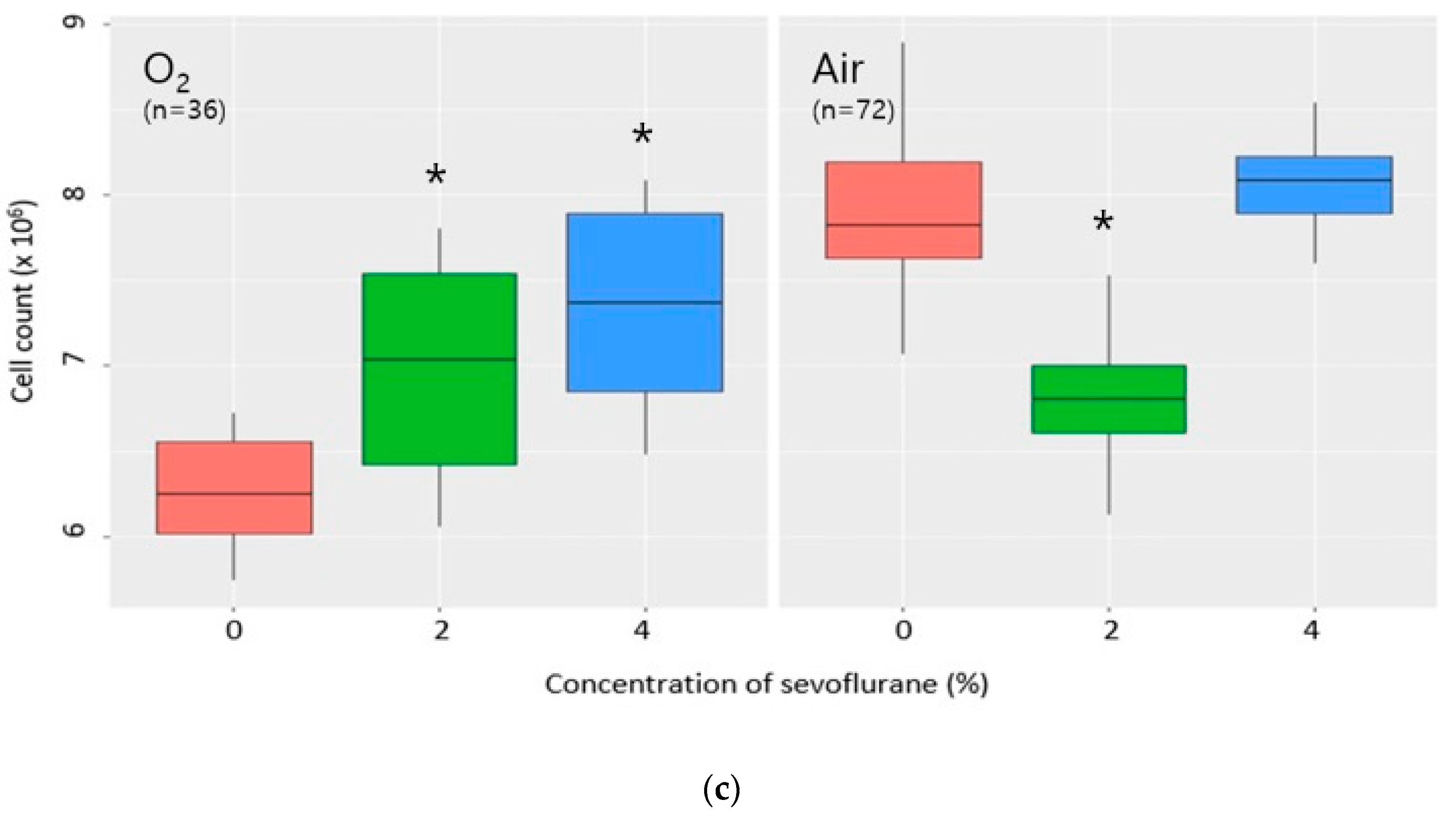
3.1. In Vitro Study
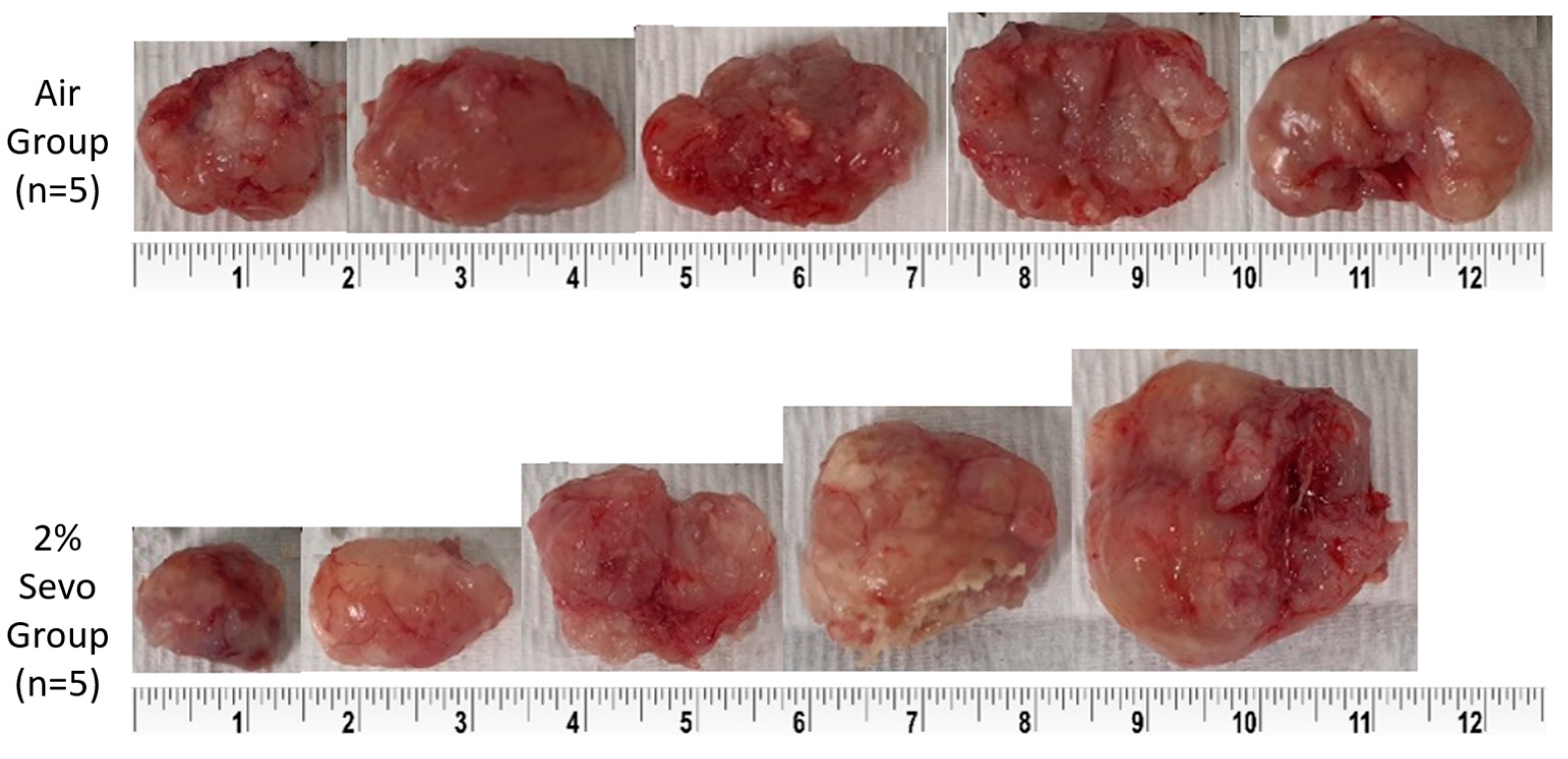
3.2. In Vivo Study
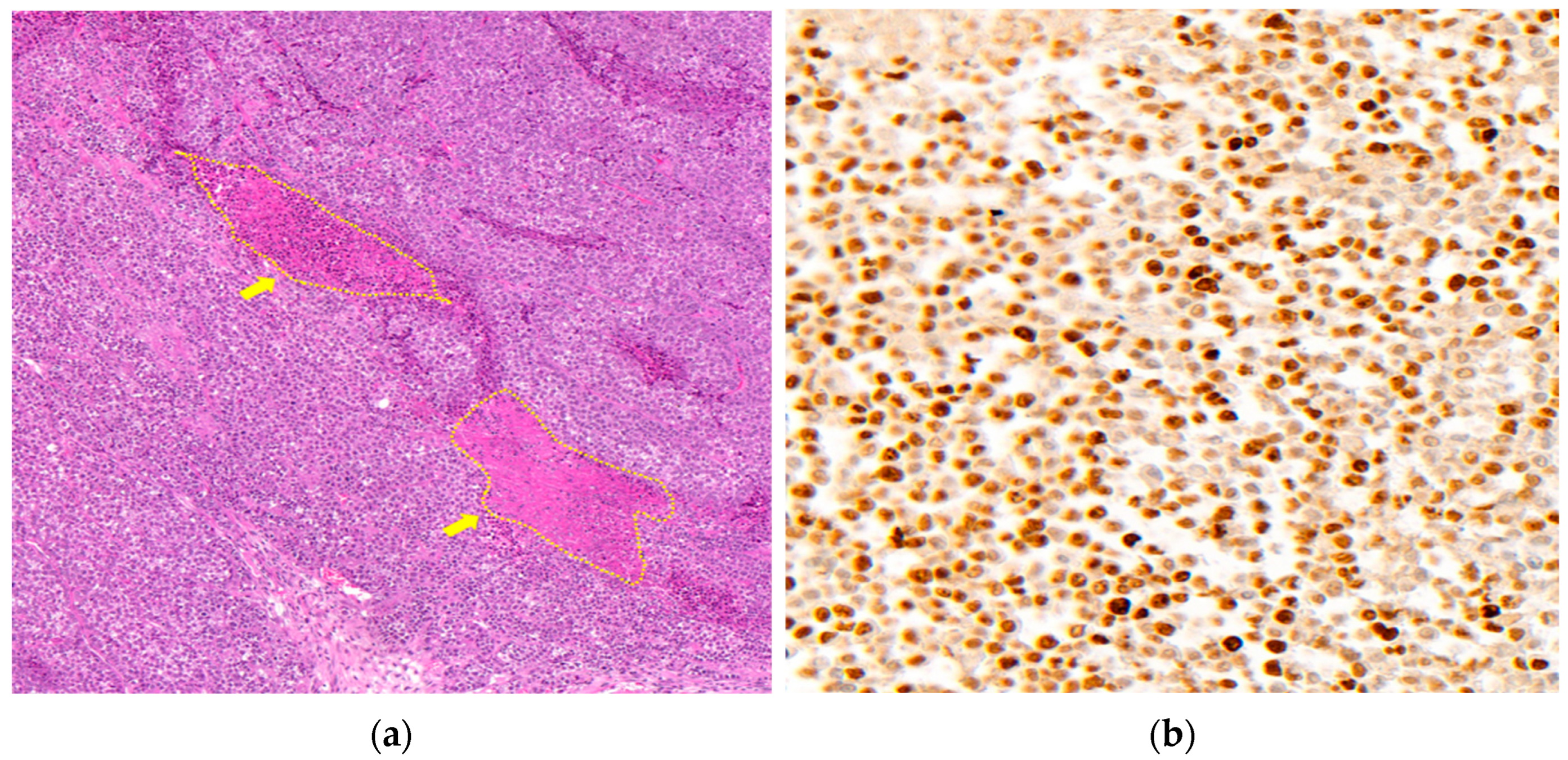
3.3. The Pathological Experiments with Resected Tumor
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hong, S.; Won, Y.J.; Lee, J.J.; Jung, K.W.; Kong, H.J.; Im, J.S.; Seo, H.G. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2018. Cancer Res. Treat. 2021, 53, 301–315. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.W.; Won, Y.J.; Kong, H.J.; Lee, E.S. Prediction of cancer incidence and mortality in Korea, 2019. Cancer Res. Treat. 2019, 51, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Gadgeel, S.M.; Ramalingam, S.S.; Kalemkerian, G.P. Treatment of Lung Cancer. Radiol. Clin. N. Am. 2012, 50, 961–974. [Google Scholar] [CrossRef] [PubMed]
- Baltayiannis, N.; Chandrinos, M.; Anagnostopoulos, D.; Zarogoulidis, P.; Tsakiridis, K.; Mpakas, A.; Machairiotis, N.; Katsikogiannis, N.; Kougioumtzi, I.; Courcoutsakis, N.; et al. Lung cancer surgery: An up to date. J. Thorac. Dis. 2013, 5, S425–S439. [Google Scholar] [CrossRef] [PubMed]
- Roth, K.; Nilsen, T.I.; Hatlen, E.; Sørensen, K.S.; Hole, T.; Haaverstad, R. Predictors of long time survival after lung cancer surgery: A retrospective cohort study. BMC Pulm. Med. 2008, 8, 22. [Google Scholar] [CrossRef] [Green Version]
- Gottschalk, A.; Sharma, S.; Ford, J.; Durieux, M.E.; Tiouririne, M. Review article: The role of the perioperative period in recurrence after cancer surgery. Anesth. Analg. 2010, 110, 1636–1643. [Google Scholar] [CrossRef]
- Dubowitz, J.A.; Sloan, E.K.; Riedel, B.J. Implicating anaesthesia and the perioperative period in cancer recurrence and metastasis. Clin. Exp. Metastasis 2018, 35, 347–358. [Google Scholar] [CrossRef]
- Mao, L.; Lin, S.; Lin, J. The effects of anesthetics on tumor progression. Int. J. Physiol. Pathophysiol. Pharmacol. 2013, 5, 1–10. [Google Scholar] [PubMed]
- Kelbel, I.; Weiss, M. Anaesthetics and immune function. Curr. Opin. Anaesthesiol. 2001, 14, 685–691. [Google Scholar] [CrossRef]
- Wang, J.; Cheng, C.S.; Lu, Y.; Sun, S.; Huang, S. Volatile Anesthetics Regulate Anti-Cancer Relevant Signaling. Front. Oncol. 2021, 11, 610514. [Google Scholar] [CrossRef]
- Zhang, C.; Wang, B.; Wang, X.; Sheng, X.; Cui, Y. Sevoflurane inhibits the progression of ovarian cancer through down-regulating stanniocalcin 1 (STC1). Cancer Cell Int. 2019, 19, 339. [Google Scholar] [CrossRef] [Green Version]
- Liang, H.; Gu, M.; Yang, C.; Wang, H.; Wen, X.; Zhou, Q. Sevoflurane inhibits invasion and migration of lung cancer cells by inactivating the p38 MAPK signaling pathway. J. Anesth. 2012, 26, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Jiang, W.; Xie, S.; Xue, F.; Zhu, X. The Role of Inhaled Anesthetics in Tumorigenesis and Tumor Immunity. Cancer Manag. Res. 2020, 12, 1601–1609. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Yun, S.; Shin, K.A.; Chung, W.; Ko, Y.; Kim, Y.H.; Lim, C. Effects of Sevoflurane on Lewis Lung Carcinoma Cell Proliferation In Vivo and In Vitro. Medicina 2021, 57, 45. [Google Scholar] [CrossRef]
- Tomayko, M.M.; Reynolds, C.P. Determination of subcutaneous tumor size in athymic (nude) mice. Cancer Chemother. Pharmacol. 1989, 24, 148–154. [Google Scholar] [CrossRef]
- Elmore, S.A.; Dixon, D.; Hailey, J.R.; Harada, T.; Herbert, R.A.; Maronpot, R.R.; Nolte, T.; Rehg, J.E.; Rittinghausen, S.; Rosol, T.J.; et al. Recommendations from the INHAND Apoptosis/Necrosis Working Group. Toxicol. Pathol. 2016, 44, 173–188. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Hu, R.; Yan, J.; Chen, Z.; Lu, Y.; Jiang, J.; Jiang, H. Sevoflurane inhibits the malignant potential of head and neck squamous cell carcinoma via activating the hypoxia-inducible factor-1α signaling pathway in vitro. Int. J. Mol. Med. 2018, 41, 995–1002. [Google Scholar] [CrossRef] [Green Version]
- Kazzaz, J.A.; Xu, J.; Palaia, T.A.; Mantell, L.; Fein, A.M.; Horowitz, S. Cellular oxygen toxicity. Oxidant injury without apoptosis. J. Biol. Chem. 1996, 271, 15182–15186. [Google Scholar] [CrossRef] [Green Version]
- Housset, B.; Hurbain, I.; Masliah, J.; Laghsal, A.; Chaumette-Demaugre, M.T.; Karam, H.; Derenne, J. Toxic effects of oxygen on cultured alveolar epithelial cells, lung fibroblasts and alveolar macrophages. Eur. Respir. J. 1991, 4, 1066–1075. [Google Scholar] [CrossRef] [PubMed]
- Ecimovic, P.; McHugh, B.; Murray, D.; Doran, P.; Buggy, D.J. Effects of sevoflurane on breast cancer cell function in vitro. Anticancer Res. 2013, 33, 4255–4260. [Google Scholar] [PubMed]
- Shi, Q.Y.; Zhang, S.J.; Liu, L.; Chen, Q.S.; Yu, L.N.; Zhang, F.J.; Yan, M. Sevoflurane promotes the expansion of glioma stem cells through activation of hypoxia-inducible factors in vitro. Br. J. Anaesth. 2015, 114, 825–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Wang, T.; Gu, J.Q.; Su, H.B. Volatile anesthetic sevoflurane suppresses lung cancer cells and miRNA interference in lung cancer cells. Onco. Targets Ther. 2018, 11, 5689–5693. [Google Scholar] [CrossRef] [Green Version]
- Wei, G.H.; Zhang, J.; Liao, D.Q.; Li, Z.; Yang, J.; Luo, N.F.; Gu, Y. The common anesthetic, sevoflurane, induces apoptosis in A549 lung alveolar epithelial cells. Mol. Med. Rep. 2014, 9, 197–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, H.; Yang, C.X.; Zhang, B.; Wang, H.B.; Liu, H.Z.; Lai, X.H.; Liao, M.J.; Zhang, T. Sevoflurane suppresses hypoxia-induced growth and metastasis of lung cancer cells via inhibiting hypoxia-inducible factor-1α. J. Anesth. 2015, 29, 821–830. [Google Scholar] [CrossRef]
- Kang, K.; Wang, Y. Sevoflurane Inhibits Proliferation and Invasion of Human Ovarian Cancer Cells by Regulating JNK and p38 MAPK Signaling Pathway. Drug Des. Devel. Ther. 2019, 13, 4451–4460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, Y.; Guo, L.; Liu, Y.; Zhao, T.; Liu, X.; Zhang, Y. Sevoflurane Limits Glioma Progression by Regulating Cell Proliferation, Apoptosis, Migration, and Invasion via miR-218-5p/DEK/β-Catenin Axis in Glioma. Cancer Manag. Res. 2021, 13, 2057–2069. [Google Scholar] [CrossRef]
- Lai, R.C.; Shan, W.R.; Zhou, D.; Zeng, X.Q.; Zuo, K.; Pan, D.F.; Zeng, W.A.; Zuo, Z.Y. Sevoflurane promotes migration, invasion, and colony-forming ability of human glioblastoma cells possibly via increasing the expression of cell surface protein 44. Acta Pharmacol. Sin. 2019, 40, 1424–1435. [Google Scholar] [CrossRef]
- Silliman, C.C.; Wang, M. The merits of in vitro versus in vivo modeling in investigation of the immune system. Environ. Toxicol. Pharmacol. 2006, 21, 123–134. [Google Scholar] [CrossRef]
- Liu, Z.G.; Jiao, D. Necroptosis, tumor necrosis and tumorigenesis. Cell Stress 2019, 4, 1–8. [Google Scholar] [CrossRef]
- Sun, X.; Kaufman, P.D. Ki-67: More than a proliferation marker. Chromosoma 2018, 127, 175–186. [Google Scholar] [CrossRef]
- Tabata, K.; Tanaka, T.; Hayashi, T.; Hori, T.; Nunomura, S.; Yonezawa, S.; Fukuoka, J. Ki-67 is a strong prognostic marker of non-small cell lung cancer when tissue heterogeneity is considered. BMC Clin. Pathol. 2014, 14, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.T.; Jiang, G.; Chen, Q.; Zheng, J.N. Ki67 is a promising molecular target in the diagnosis of cancer (review). Mol. Med. Rep. 2015, 11, 1566–1572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamiloglu, S.; Sari, G.; Ozdal, T.; Capanoglu, E. Guidelines for cell viability assays. Food Front. 2020, 1, 332–349. [Google Scholar] [CrossRef]
- Liang, H.; Gu, M.N.; Yang, C.X.; Wang, H.B.; Wen, X.J.; Zhou, Q.L. Sevoflurane inhibits proliferation, induces apoptosis, and blocks cell cycle progression of lung carcinoma cells. Asian Pac. J. Cancer Prev. 2011, 12, 3415–3420. [Google Scholar] [PubMed]
- Hoffmann, B.; Lange, T.; Labitzky, V.; Riecken, K.; Wree, A.; Schumacher, U.; Wedemann, G. The initial engraftment of tumor cells is critical for the future growth pattern: A mathematical study based on simulations and animal experiments. BMC Cancer 2020, 20, 524. [Google Scholar] [CrossRef]
- Reid, M.D.; Bagci, P.; Ohike, N.; Saka, B.; Erbarut Seven, I.; Dursun, N.; Balci, S.; Gucer, H.; Jang, K.T.; Tajiri, T.; et al. Calculation of the Ki67 index in pancreatic neuroendocrine tumors: A comparative analysis of four counting methodologies. Mod. Pathol. 2015, 28, 686–694. [Google Scholar] [CrossRef] [Green Version]
- Gao, Z.; Xu, J.; Coburn, M.; Ma, D.; Wang, K. Postoperative Long-Term Outcomes and Independent Risk Factors of Non-Small-Cell Lung Cancer Patients With Propofol versus Sevoflurane Anesthesia: A Retrospective Cohort Study. Front. Pharmacol. 2022, 13, 945868. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Air Group (n = 5) | 2% Sevo Group (n = 5) | p Value | |
|---|---|---|---|
| Initial weight (g) | 25.8 ± 1.2 | 25.6 ± 1.0 | 0.763 |
| Final weight (g) | 25.9 ± 2.1 | 26.2 ± 2.0 | 0.868 |
| Weight change (g) | −0.4 ± 1.4 | 0.2 ± 1.3 | 0.528 |
| Tumor size (cm3) | 1.5 ± 0.7 | 2.4 ± 1.9 | 0.38 |
| Tumor weight (g) | 4.6 ± 0.9 | 4.6 ± 3.3 | 0.978 |
| Air Group (n = 10) | 2% Sevo Group (n = 10) | p Value | |
|---|---|---|---|
| Necrosis ratio (%) | 16.7 ± 3.2 | 16.7 ± 2.9 | 0.972 |
| Ki-67 positive index (%) | 86.8 (84.4; 88.8) | 87.6 (80.3; 88.6) | 0.925 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yun, S.; Kim, K.; Shin, K.; Park, H.; Lee, S.; Shin, Y.; Paing, A.S.; Choi, S.; Lim, C. Effect of Sevoflurane on the Proliferation of A549 Lung Cancer Cells. Medicina 2023, 59, 613. https://doi.org/10.3390/medicina59030613
Yun S, Kim K, Shin K, Park H, Lee S, Shin Y, Paing AS, Choi S, Lim C. Effect of Sevoflurane on the Proliferation of A549 Lung Cancer Cells. Medicina. 2023; 59(3):613. https://doi.org/10.3390/medicina59030613
Chicago/Turabian StyleYun, Sangwon, Kyongsik Kim, Keuna Shin, Hanmi Park, Sunyeul Lee, Yongsup Shin, Aung Soe Paing, Songyi Choi, and Chaeseong Lim. 2023. "Effect of Sevoflurane on the Proliferation of A549 Lung Cancer Cells" Medicina 59, no. 3: 613. https://doi.org/10.3390/medicina59030613