
Basic Operative Tactics for Pulmonary Echinococcosis in the Era of Endostaplers and Energy Devices
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentations
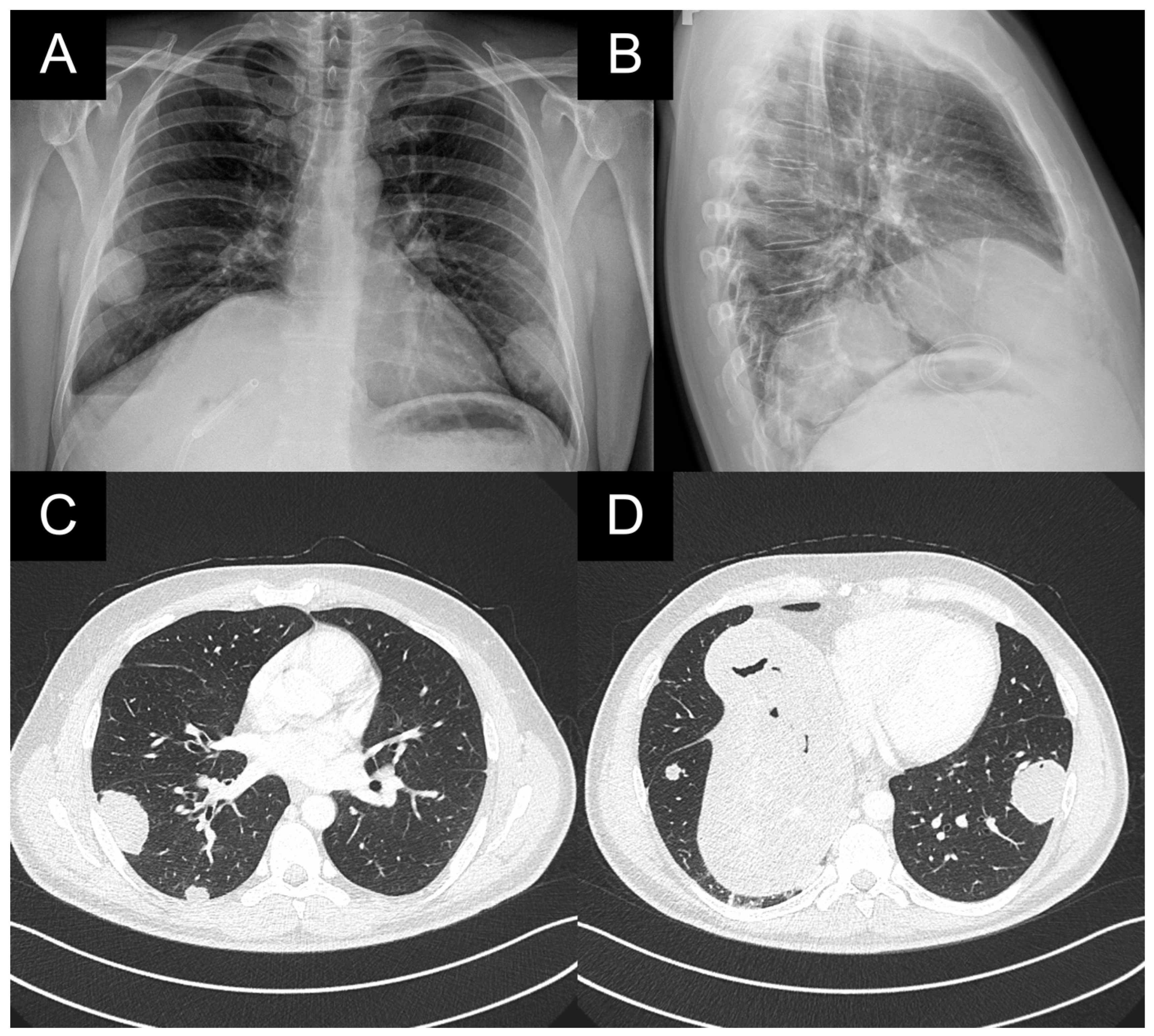
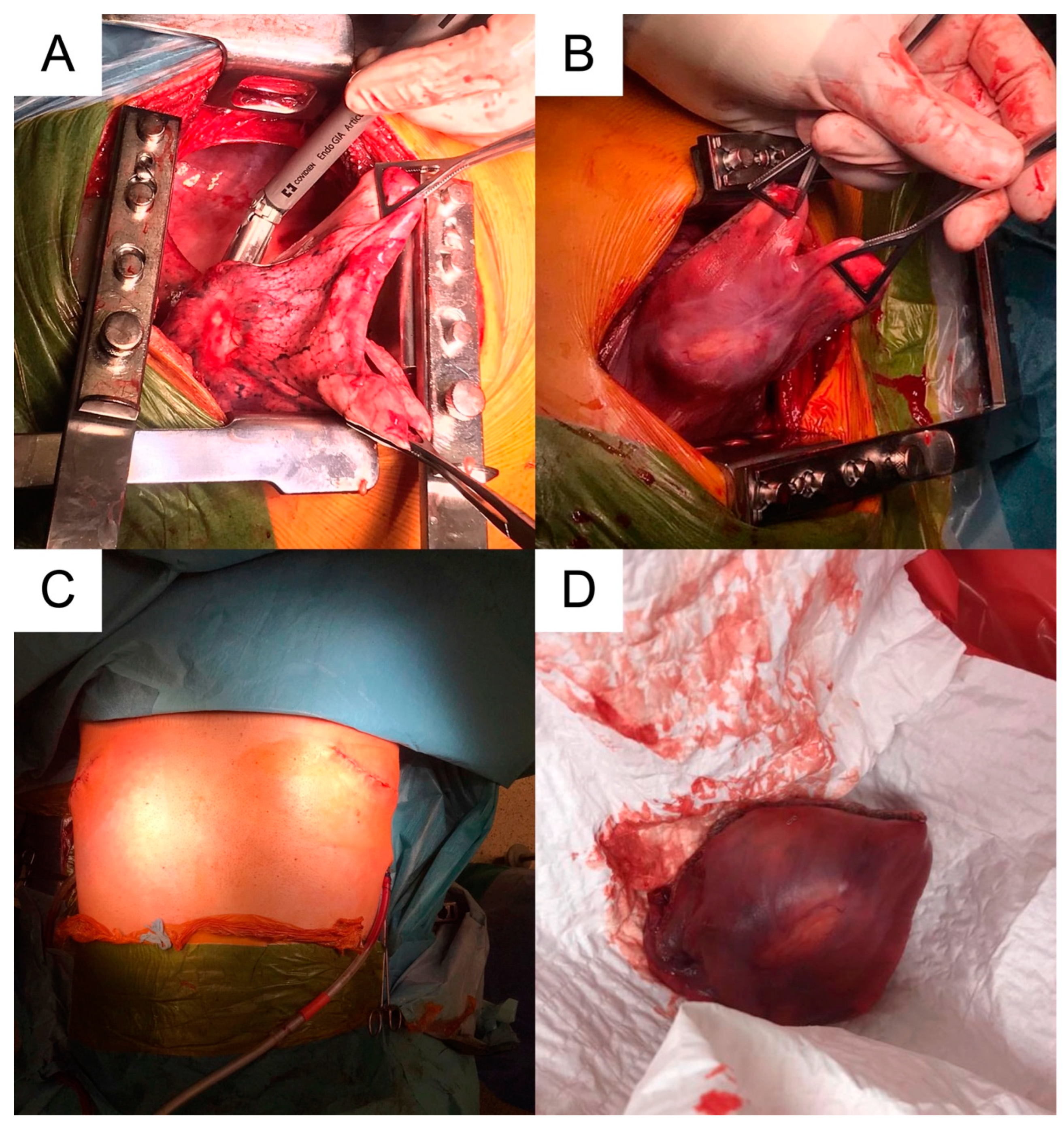
2.1. Case 1
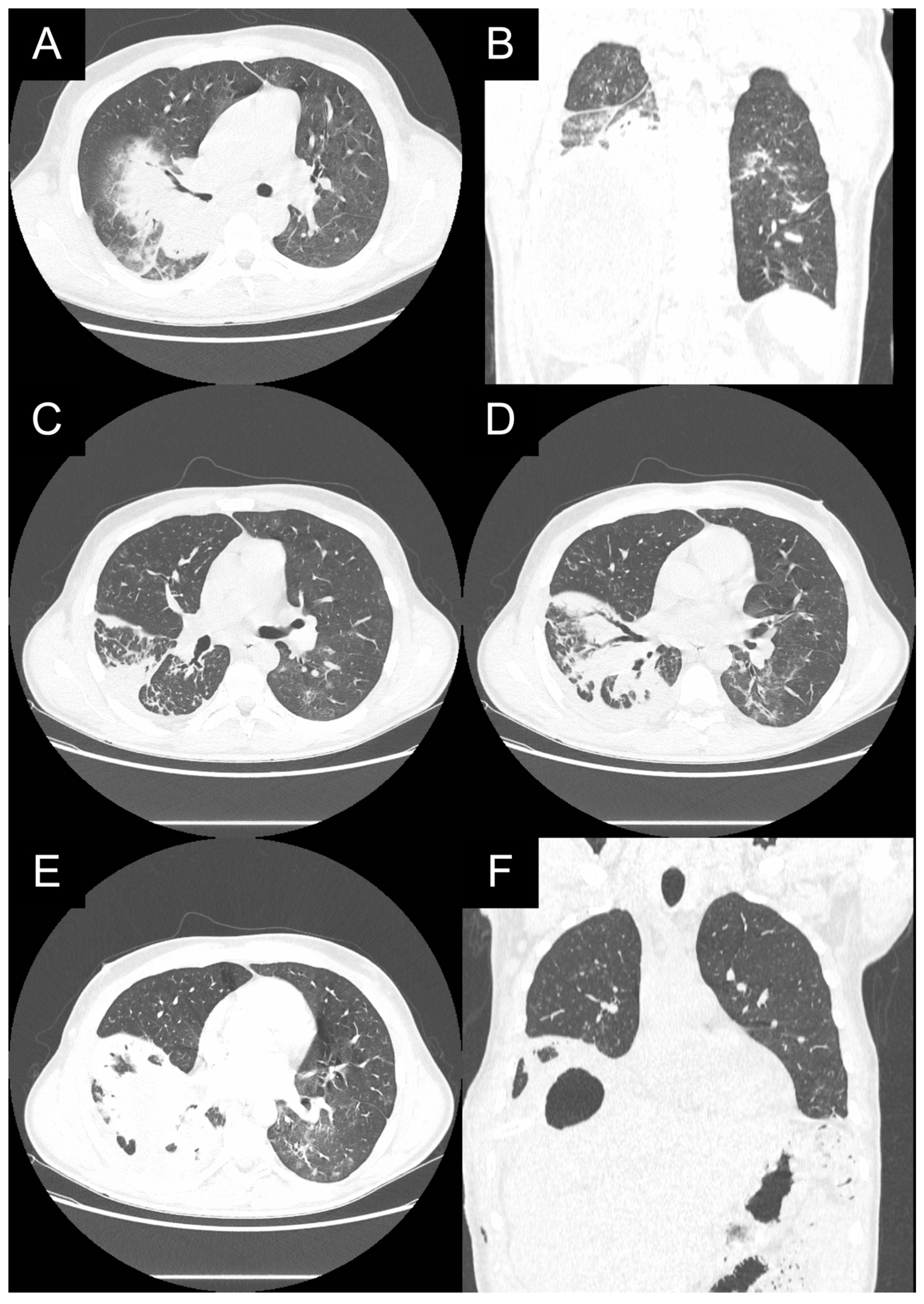
2.2. Case 2
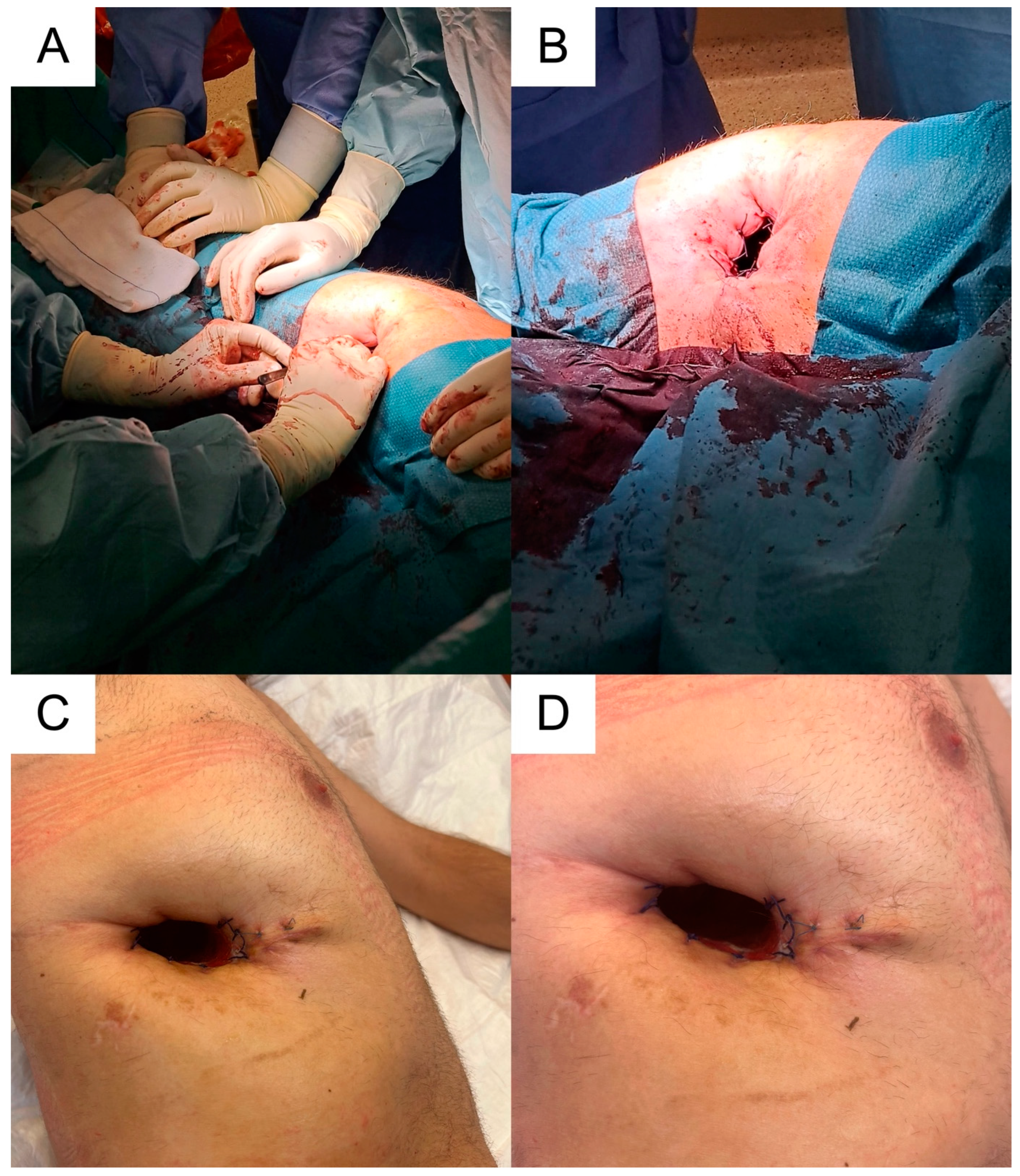
2.3. Case 3
3. Discussion
3.1. Characteristics of Echinococcus granulosus and Echinococcus multilocularis
3.1.1. Echinococcus granulosus
3.1.2. Echinococcus multilocularis
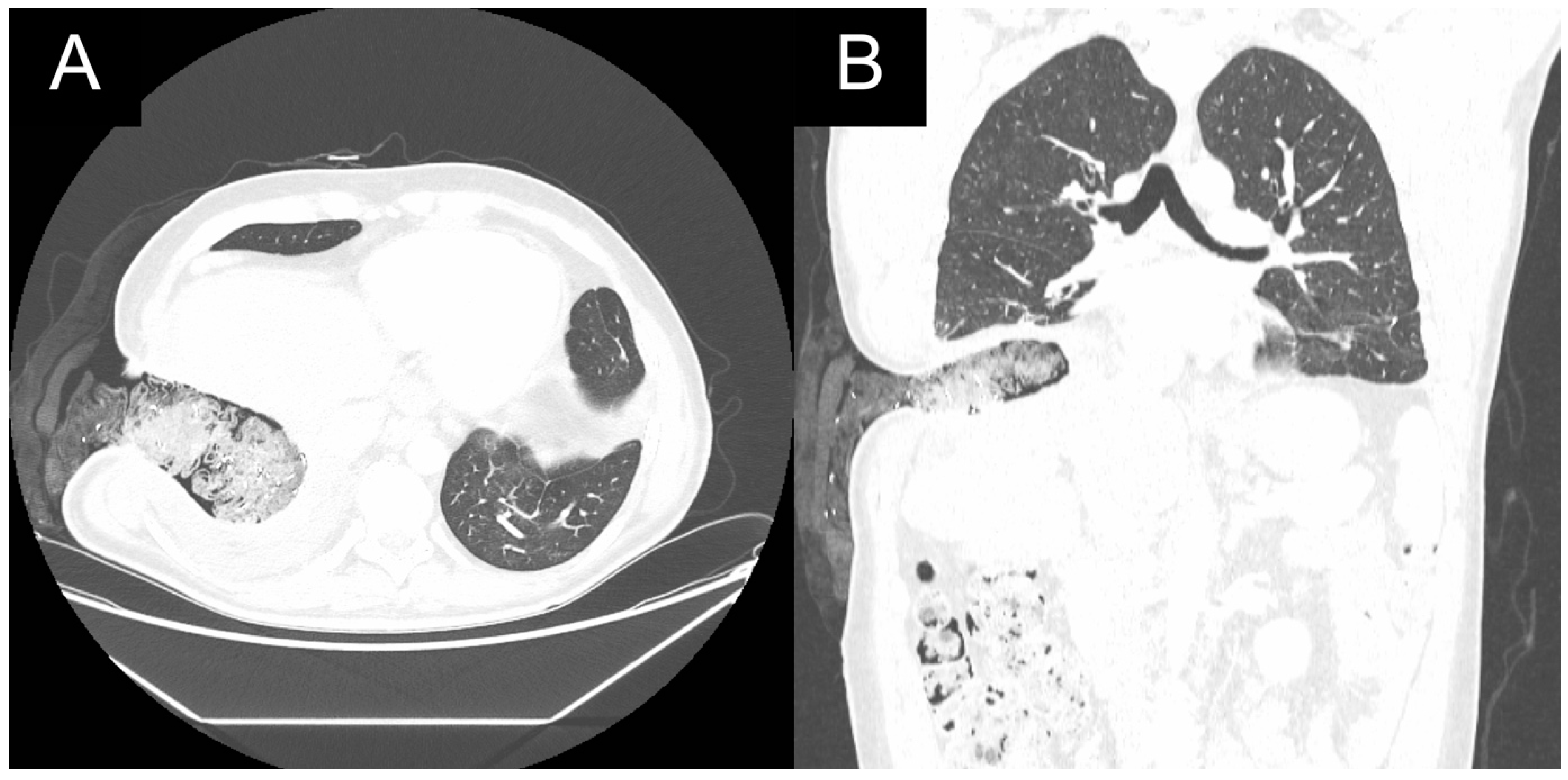
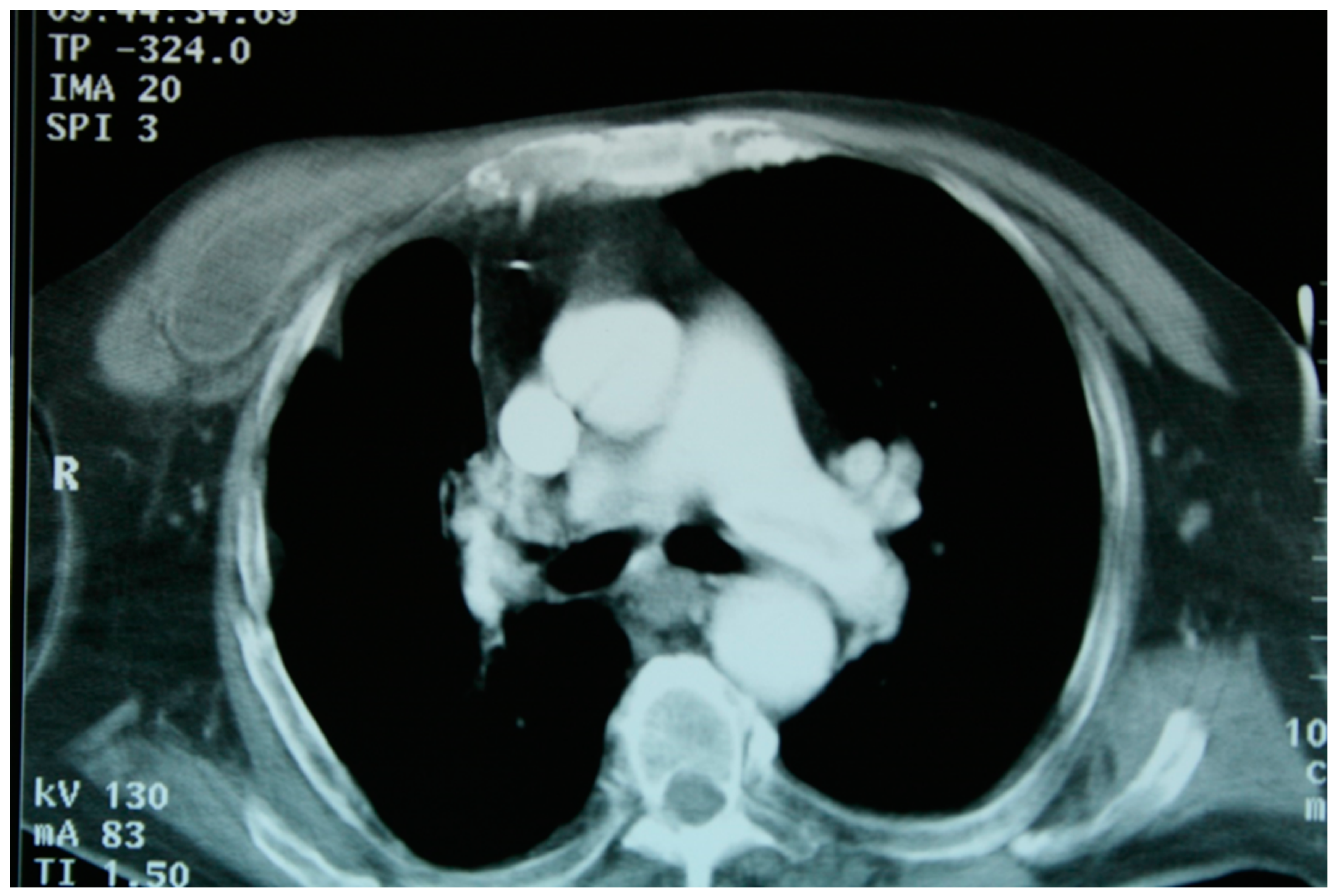
3.2. Radiological Imaging
3.3. Other Diagnosis Procedures
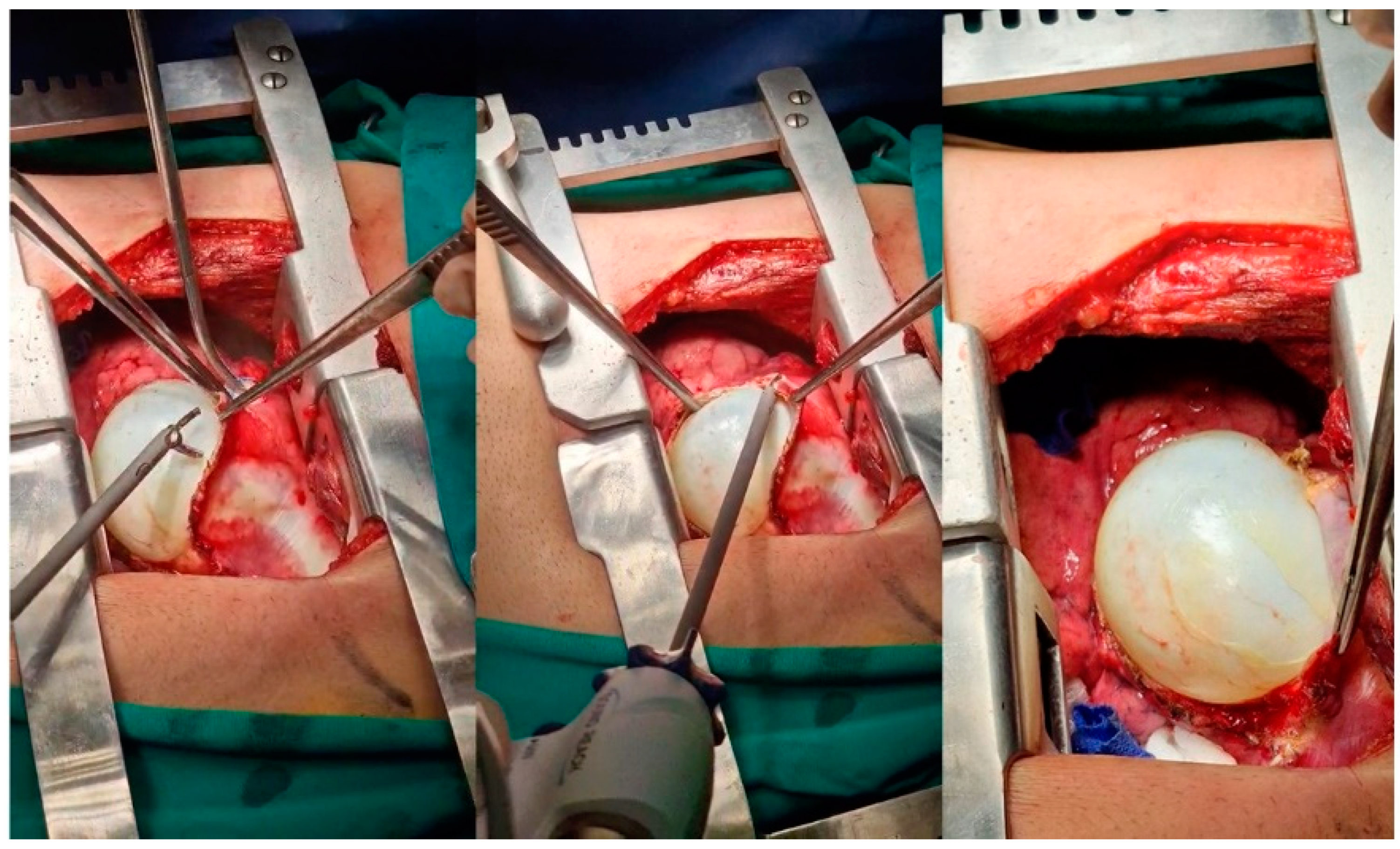
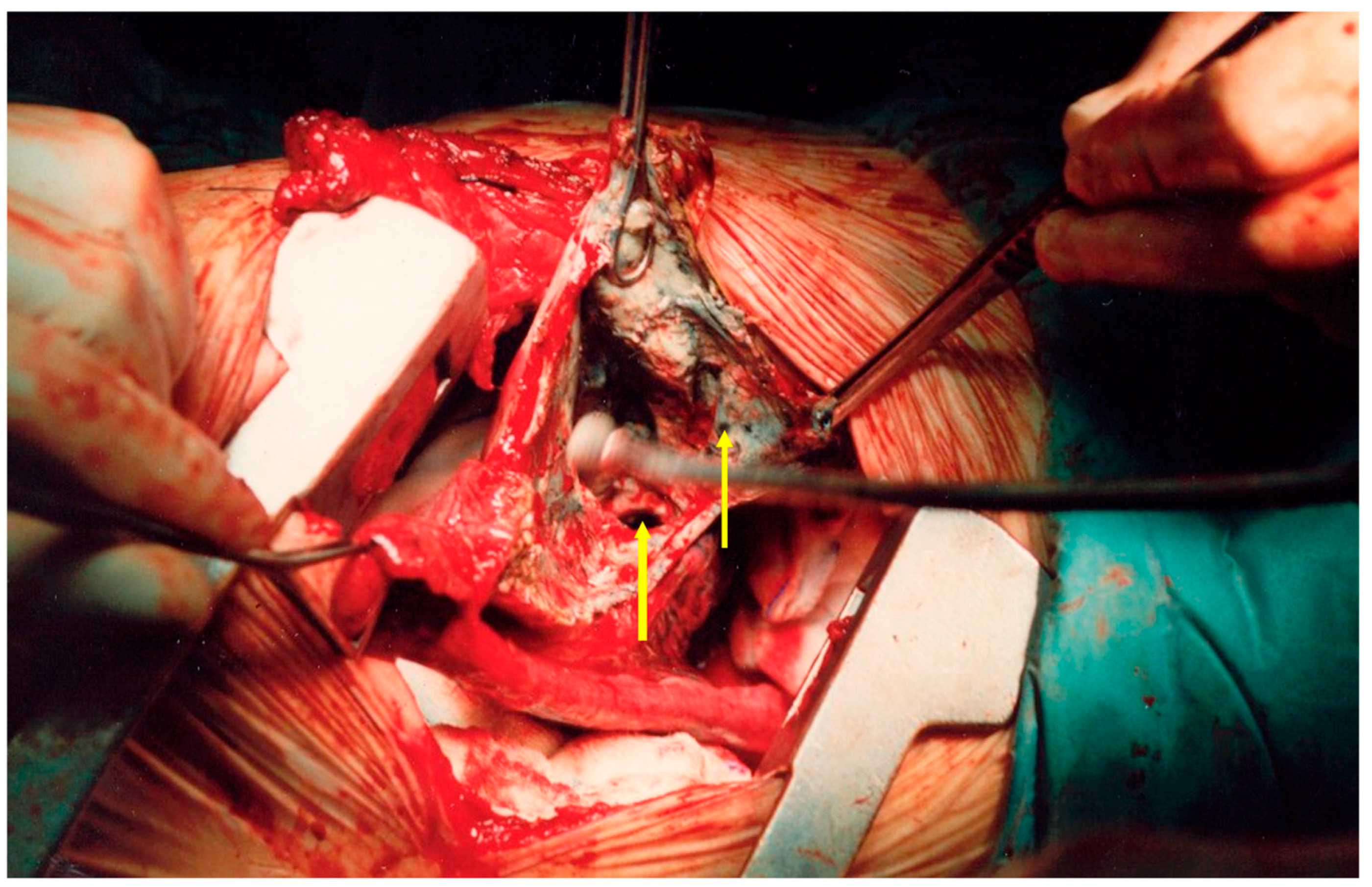
3.4. Treatment
3.5. Differential Diagnosis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Romig, T. Epidemiology of Echinococcosis. Langenbeck’s Arch. Surg. 2003, 388, 209–217. [Google Scholar] [CrossRef]
- Kundu, R.; Punia, R.; Dalal, U.; Handa, U.; Mohan, H. Pulmonary Hydatidosis in a Tertiary Care Hospital. Lung India 2015, 32, 246. [Google Scholar] [CrossRef]
- Santivanez, S.; Garcia, H.H. Pulmonary Cystic Echinococcosis. Curr. Opin. Pulm. Med. 2010, 1, 257–261. [Google Scholar] [CrossRef]
- Gottstein, B.; Reichen, J. Hydatid Lung Disease (Echinococcosis/Hydatidosis). Clin. Chest Med. 2002, 23, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Agudelo Higuita, N.I.; Brunetti, E.; McCloskey, C. Cystic Echinococcosis. J. Clin. Microbiol. 2016, 54, 518–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkar, M.; Pathania, R.; Jhobta, A.; Thakur, B.; Chopra, R. Cystic Pulmonary Hydatidosis. Lung India 2016, 33, 179. [Google Scholar] [CrossRef]
- Khan, H.; Casulli, A.; Harandi, M.F.; Afzal, M.S.; Saqib, M.A.N.; Ahmed, H. A Retrospective Cohort Study on Human Cystic Echinococcosis in Khyber Pakhtunkhwa Province (Pakistan) Based on 16 Years of Hospital Discharge Records. Pathogens 2022, 11, 194. [Google Scholar] [CrossRef] [PubMed]
- Joanny, G.; Cappai, M.G.; Nonnis, F.; Tamponi, C.; Dessì, G.; Mehmood, N.; Dahdah, J.; Hosri, C.; Scala, A.; Varcasia, A. Human Cystic Echinococcosis in Lebanon: A Retrospective Study and Molecular Epidemiology. Acta Parasitol. 2021, 67, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Dogan, R.; Yuksel, M.; Cetin, G.; Suzer, K.; Alp, M.; Kaya, S.; Unlu, M.; Moldibi, B. Surgical Treatment of Hydatid Cysts of the Lung: Report on 1055 Patients. Thorax 1989, 44, 192–199. [Google Scholar] [CrossRef] [Green Version]
- Duran, R.; Pehlivan, B. Factors increasing mortality in Echinococcosis patients treated percutaneously or surgically. A review of 1143 patients: A retrospective single center study. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 493–500. [Google Scholar] [CrossRef]
- Dupont, C.; Grenouillet, F.; Mabrut, J.-Y.; Gay, F.; Persat, F.; Wallon, M.; Mornex, J.-F.; Philit, F.; Dupont, D. Fast-Growing Alveolar Echinococcosis Following Lung Transplantation. Pathogens 2020, 9, 756. [Google Scholar] [CrossRef] [PubMed]
- Geyer, M.; Wilpert, J.; Wiech, T.; Theilacker, C.; Stubanus, M.; Kramer-Zucker, A.; Fischer, K.-G.; Drognitz, O.; Frydrychowicz, A.; Kern, W.; et al. Rapidly Progressive Hepatic Alveolar Echinococcosis in an ABO-Incompatible Renal Transplant Recipient. Transpl. Infect. Dis. 2010, 13, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Brunetti, E.; Kern, P.; Vuitton, D.A. Expert Consensus for the Diagnosis and Treatment of Cystic and Alveolar Echinococcosis in Humans. Acta Trop. 2010, 114, 1–16. [Google Scholar] [CrossRef]
- Aydin, Y.; Ogul, H.; Topdagi, O.; Ulas, A.B.; Sade, R.; Ozturk, G.; Korkut, E.; Aksungur, N.; Sener, E.; Kesmez Can, F.; et al. Relevance of Pulmonary Alveolar Echinococcosis. Arch. Bronconeumol. 2020, 56, 779–783. [Google Scholar] [CrossRef] [PubMed]
- Kern, P.; Wen, H.; Sato, N.; Vuitton, D.A.; Gruener, B.; Shao, Y.; Delabrousse, E.; Kratzer, W.; Bresson-Hadni, S. WHO Classification of Alveolar Echinococcosis: Principles and Application. Parasitol. Int. 2006, 55, S283–S287. [Google Scholar] [CrossRef] [PubMed]
- Fronhoffs, F.; Dold, L.; Parčina, M.; Schneidewind, A.; Willis, M.; Barth, T.F.E.; Weismüller, T.J.; Zhou, T.; Lutz, P.; Luetkens, J.A.; et al. Alveolar Echinococcosis in a Patient with Presumed Autoimmune Hepatitis and Primary Sclerosing Cholangitis: An Unexpected Finding after Liver Transplantation. Pathogens 2023, 12, 73. [Google Scholar] [CrossRef] [PubMed]
- Ammann, R.W.; Eckert, J. Cestodes. Echinococcus. Gastroenterol. Clin. N. Am. 1996, 25, 655–689. [Google Scholar] [CrossRef]
- Torgerson, P.R.; Schweiger, A.; Deplazes, P.; Pohar, M.; Reichen, J.; Ammann, R.W.; Tarr, P.E.; Halkik, N.; Müllhaupt, B. Alveolar Echinococcosis: From a Deadly Disease to a Well-Controlled Infection. Relative Survival and Economic Analysis in Switzerland over the Last 35 Years. J. Hepatol. 2008, 49, 72–77. [Google Scholar] [CrossRef]
- Wu, L.; Pema; Mu, L.; Si, M.; Xu, J.; Ciren, G.; Cai, L. Application of Multi-Slice Computed Tomography for the Preoperative Diagnosis and Classification of Pulmonary Cystic Echinococcosis. Pathogens 2021, 10, 353. [Google Scholar] [CrossRef]
- Guo, H.; Liu, W.; Wang, J.; Xing, Y. Extrahepatic Alveolar Echinococcus on Multi-Slice Computed Tomography and Magnetic Resonance Imaging. Sci. Rep. 2021, 11, 9409. [Google Scholar] [CrossRef]
- Choh, N.A.; Parry, A.H.; Wani, A.H.; Feroz, I.; Bhat, M.H.; Shaheen, F.A. The Spectrum of Imaging Findings in Pulmonary Hydatid Disease and the Additive Value of T2-Weighted Magnetic Resonance Imaging in Its Diagnosis. Pol. J. Radiol. 2021, 86, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Savu, C.; Melinte, A.; Grigorie, V.; Iliescu, L.; Diaconu, C.; Dimitriu, M.; Socea, B.; Stiru, O.; Varlas, V.; Savu, C.; et al. Primary Pleural Hydatidosis—A Rare Occurrence: A Case Report and Literature Review. Medicina 2020, 56, 567. [Google Scholar] [CrossRef]
- Aydin, Y.; Ogul, H.; Bayraktutan, U.; Ulas, A.B.; Eroglu, A. Miliary Lung Metastases in Echinococcus Multilocularis Infection. Ann. Thorac. Surg. 2019, 108, e47. [Google Scholar] [CrossRef] [PubMed]
- Manzano-Román, R.; Sánchez-Ovejero, C.; Hernández-González, A.; Casulli, A.; Siles-Lucas, M. Serological Diagnosis and Follow-Up of Human Cystic Echinococcosis: A New Hope for the Future? BioMed Res. Int. 2015, 2015, 428205. [Google Scholar] [CrossRef] [Green Version]
- Sadjjadi, S.M.; Sedaghat, F.; Hosseini, S.V.; Sarkari, B. Serum Antigen and Antibody Detection in Echinococcosis: Application in Serodiagnosis of Human Hydatidosis. Korean J. Parasitol. 2009, 47, 153. [Google Scholar] [CrossRef] [Green Version]
- Shahabinejad, P.; Shahriarirad, R.; Omidian, M.; Ghorbani, F.; Barazesh, A.; Sarkari, B. Diagnostic Performance of Echinococcus Granulosus Protoscolices Antigens in the Serodiagnosis of Human Cystic Echinococcosis. J. Immunoass. Immunochem. 2020, 41, 833–840. [Google Scholar] [CrossRef]
- Carmena, D.; Benito, A.; Eraso, E. The Immunodiagnosis of Echinococcus Multilocularis Infection. Clin. Microbiol. Infect. 2007, 13, 460–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barth, T.F.E.; Casulli, A. Morphological Characteristics of Alveolar and Cystic Echinococcosis Lesions in Human Liver and Bone. Pathogens 2021, 10, 1326. [Google Scholar] [CrossRef] [PubMed]
- Barth, T.F.E.; Herrmann, T.S.; Tappe, D.; Stark, L.; Grüner, B.; Buttenschoen, K.; Hillenbrand, A.; Juchems, M.; Henne-Bruns, D.; Kern, P.; et al. Sensitive and Specific Immunohistochemical Diagnosis of Human Alveolar Echinococcosis with the Monoclonal Antibody Em2G11. PLoS Negl. Trop. Dis. 2012, 6, e1877. [Google Scholar] [CrossRef]
- Joliat, G.-R.; Martins-Filho, S.N.; Haefliger, S.; Demartines, N.; Halkic, N.; Labgaa, I.; Sempoux, C. PD-L1 Is a Determinant of Recurrence in Alveolar Echinococcosis. Int. J. Infect. Dis. 2023; in press. [Google Scholar] [CrossRef]
- Bellanger, A.; Wang, J.; Gbaguidi-Haore, H.; Barrera, C.; Bresson-Hadni, S.; Zlobec, I.; Lachenmayer, A.; Richou, C.; Turco, C.; Gottstein, B.; et al. Investigating New Serological and Tissue Markers for the Follow-up of Patients Operated for Alveolar Echinococcosis. Parasite Immunol. 2021, 43, e12827. [Google Scholar] [CrossRef]
- Knapp, J.; Lallemand, S.; Monnien, F.; Felix, S.; Valmary-Degano, S.; Courquet, S.; Demonmerot, F.; Heyd, B.; Turco, C.; Doussot, A.; et al. Molecular Diagnosis of Alveolar Echinococcosis in Patients Based on Frozen and Formalin-Fixed Paraffin-Embedded Tissue Samples. Parasite 2022, 29, 4. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Ma, Y.; Wang, W.; Dai, Y.; Sun, H.; Li, J.; Wang, S.; Li, F. Status and Prospect of Novel Treatment Options toward Alveolar and Cystic Echinococcosis. Acta Trop. 2022, 226, 106252. [Google Scholar] [CrossRef]
- Velasco-Tirado, V.; Alonso-Sardón, M.; Lopez-Bernus, A.; Romero-Alegría, Á.; Burguillo, F.J.; Muro, A.; Carpio-Pérez, A.; Muñoz Bellido, J.L.; Pardo-Lledias, J.; Cordero, M.; et al. Medical Treatment of Cystic Echinococcosis: Systematic Review and Meta-Analysis. BMC Infect. Dis. 2018, 18, 306. [Google Scholar] [CrossRef]
- Stamatakos, M.; Sargedi, C.; Stefanaki, C.; Safioleas, C.; Matthaiopoulou, I.; Safioleas, M. Anthelminthic Treatment: An Adjuvant Therapeutic Strategy against Echinococcus Granulosus. Parasitol. Int. 2009, 58, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Polat, C.; Dervisoglu, A.; Hokelek, M.; Yetim, I.; Buyukkarabacak, Y.; Ozkutuk, Y.; Erzurumlu, K. Dual Treatment of Albendazole in Hepatic Hydatidosis: New Therapeutic Modality in 52 Cases. J. Gastroenterol. Hepatol. 2005, 20, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Fattahi Masoom, S.H.; Lari, S.M.; Fattahi, A.S.; Ahmadnia, N.; Rajabi, M.; NaderiKalat, M. Albendazole Therapy in Human Lung and Liver Hydatid Cysts: A 13-Year Experience. Clin. Res. J. 2017, 12, 1076–1083. [Google Scholar] [CrossRef]
- Sozuer, E.; Akyuz, M.; Akbulut, S. Open Surgery for Hepatic Hydatid Disease. Int. Surg. 2014, 99, 764–769. [Google Scholar] [CrossRef] [Green Version]
- Mönnink, G.L.E.; Stijnis, C.; van Delden, O.M.; Spijker, R.; Grobusch, M.P. Percutaneous Versus Surgical Interventions for Hepatic Cystic Echinococcosis: A Systematic Review and Meta-Analysis. CardioVasc. Intervent. Radiol. 2021, 44, 1689–1696. [Google Scholar] [CrossRef]
- Khuroo, M.S.; Wani, N.A.; Javid, G.; Khan, B.A.; Yattoo, G.N.; Shah, A.H.; Jeelani, S.G. Percutaneous Drainage Compared with Surgery for Hepatic Hydatid Cysts. N. Engl. J. Med. 1997, 337, 881–887. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jebbawi, F.; Bellanger, A.-P.; Beldi, G.; Millon, L.; Gottstein, B. Immunotherapy of Alveolar Echinococcosis via PD-1/PD-L1 Immune Checkpoint Blockade in Mice. Parasite Immunol. 2018, 40, e12596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kavukcu, S.; Kilic, D.; Tokat, A.O.; Kutlay, H.; Cangir, A.K.; Enon, S.; Okten, I.; Ozdemir, N.; Gungor, A.; Akal, M.; et al. Parenchyma-Preserving Surgery in the Management of Pulmonary Hydatid Cysts. J. Investig. Surg. 2006, 19, 61–68. [Google Scholar] [CrossRef]
- Aydin, Y.; Ulas, A.B.; Ince, I.; Kalin, A.; Can, F.K.; Gundogdu, B.; Kasali, K.; Kerget, B.; Ogul, Y.; Eroglu, A. Evaluation of Albendazole Efficiency and Complications in Patients with Pulmonary Hydatid Cyst. Interact. CardioVasc. Thorac. Surg. 2021, 34, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Cai, B.; Li, C.; Luo, Z.; Ciren, D.; Guo, W.; Huang, J.; Dawa, Q. Efficacy and Safety of Video-Assisted Thoracoscopic Surgery and Thoracotomy in the Treatment of Pulmonary Hydatid Disease in the Tibetan Plateau: A Retrospective Study. J. Thorac. Dis. 2022, 14, 2247–2253. [Google Scholar] [CrossRef] [PubMed]
- Abbas, N.; Zaher Addeen, S.; Abbas, F.; Al Saadi, T.; Hanafi, I.; Alkhatib, M.; Turk, T.; Al Khaddour, A. Video-Assisted Thoracoscopic Surgery (VATS) with Mini-Thoracotomy for the Management of Pulmonary Hydatid Cysts. J. Cardiothorac. Surg. 2018, 13, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aydın, Y. Pulmonary Metastasectomy with Laparotomy in Alveolar Echinococcosis. Turk. J. Thorac. Cardiovasc. Surg. 2019, 27, 593–596. [Google Scholar] [CrossRef]
- Chen, L.; Cheng, Z.; Xian, S.; Zhan, B.; Xu, Z.; Yan, Y.; Chen, J.; Wang, Y.; Zhao, L. Immunization with EmCRT-Induced Protective Immunity against Echinococcus Multilocularis Infection in BALB/c Mice. Trop. Med. Infect. Dis. 2022, 7, 279. [Google Scholar] [CrossRef]
- Zhou, P.; Zhou, Z.; Huayu, M.; Wang, L.; Feng, L.; Xiao, Y.; Dai, Y.; Xin, M.; Tang, F.; Li, R. A Multi-Epitope Vaccine GILE against Echinococcus Multilocularis Infection in Mice. Front. Immunol. 2023, 13, 1091004. [Google Scholar] [CrossRef] [PubMed]
- Lv, Y.; Chang, L.; Yang, J.; Wen, J.; Zhao, Y.; Zhu, M.; Wu, C.; Zhao, W. Immunogenicity of Peptide-based Vaccine Composed of Epitopes from Echinococcus Granulosus rEg.P29. FASEB J. 2023, 37, e22819. [Google Scholar] [CrossRef]
- Dakak, M.; Caylak, H.; Kavakli, K.; Gozubuyuk, A.; Yucel, O.; Gurkok, S.; Sapmaz, E.; Genc, O.; Cubukcu, S.; Tanyuksel, M. Parenchyma-Saving Surgical Treatment of Giant Pulmonary Hydatid Cysts. Thorac. Cardiovasc. Surg. 2009, 57, 165–168. [Google Scholar] [CrossRef]
- Toktogaziev, B.; Omorov, K.; Aitbaev, S.; Artisbekov, B.; Omorov, R.; Vityala, Y.; Tagaev, T. A Rare Case of Concurrent Pulmonary and Hepatic Hydatid Cysts Treated by Single-stage Surgical Management. Clin. Case Rep. 2022, 10, e05897. [Google Scholar] [CrossRef]
- Essa, R.A.; Ahmed, S.K.; Mohamed, M.G. Pulmonary Hydatid Cyst Mimicking Lung Tumor in a Heavy Smoker Patient—Uniportal VATS Management. Int. J. Surg. Case Rep. 2022, 95, 107138. [Google Scholar] [CrossRef]
- Ozkok, A.; Gul, E.; Okumus, G.; Yekeler, E.; Gulluoglu, M.G.; Kiyan, E.; Arseven, O. Disseminated Alveolar Echinococcosis Mimicking a Metastatic Malignancy. Int. Med. 2008, 47, 1495–1497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karamustafaoglu, Y.A.; Yoruk, Y.; Mamedov, R.; Yavasman, I. Pulmonary Echinococcosis Mimicking Pancoast Tumor. J. Thorac. Cardiovasc. Surg. 2010, 139, e57–e58. [Google Scholar] [CrossRef] [Green Version]
- Darwish, B.; Alsabek, M.B.; Kakaje, A. A Complicated Pulmonary Hydatid Cyst Resembling a Tumour in an Adult on PET Scan: A Case Report. J. Surg. Case Rep. 2020, 2020, rjaa448. [Google Scholar] [CrossRef]
- Kurt, Y.; Sücüllü, İ.; Filiz, A.İ.; Urhan, M.; Akın, M.L. Pulmonary Echinococcosis Mimicking Multipl Lung Metastasis of Breast Cancer: The Role of Fluoro-Deoxy-Glucose Positron Emission Tomography. World J. Surg. Oncol. 2008, 6, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wojtyś, M.E.; Kacalska-Janssen, O.; Ptaszyński, K.; Lisowski, P.; Kunc, M.; Wójcik, J.; Grodzki, T. Benign Metastasizing Leiomyoma of the Lung: Diagnostic Process and Treatment Based on Three Case Reports and a Review of the Literature. Biomedicines 2022, 10, 2465. [Google Scholar] [CrossRef] [PubMed]
- Alimi, F.; El Hadj Sidi, C.; Ghannouchi, C. Cystic Benign Metastasizing Leiomyoma of the Lung Mimicking Hydatid Cyst. Lung 2016, 194, 1029–1030. [Google Scholar] [CrossRef]
- Aala, F.; Badali, H.; Hashemi Fesharaki, S.; Boroumand, M.; Sotoudeh Anvari, M.; Davari, H.; Agha Kuchak Afshari, S.; Khodavaisy, S. Coexistence of Aspergilloma and Pulmonary Hydatid Cyst in an Immunocompetent Individual. J. Mycolog. Méd. 2017, 27, 396–399. [Google Scholar] [CrossRef]
- Haif, A.; Achouri, D.; Bougharnout, H.; Chahmana, A.; Bouchareb, F.; Bendecheche, B.; Soualili, Z. Coexistence of Pulmonary Hydatid Cyst and Tuberculosis in a Child: A Case Report. Ann. Pediatr. Surg. 2022, 18, 60. [Google Scholar] [CrossRef]
- Mahmood, N.; Azam, H.; Ali, M.I.; Khan, M.A. Pulmonary Hydatid Cyst with Complicating Aspergillus Infection Presenting as a Refractory Lung Abscess. Clin. Med. Insights Case Rep. 2011, 4, 63–68. [Google Scholar] [CrossRef]











Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakinowska, E.; Kostopanagiotou, K.; Wojtyś, M.E.; Kiełbowski, K.; Ptaszyński, K.; Gajić, D.; Ruszel, N.; Wójcik, J.; Grodzki, T.; Tomos, P. Basic Operative Tactics for Pulmonary Echinococcosis in the Era of Endostaplers and Energy Devices. Medicina 2023, 59, 543. https://doi.org/10.3390/medicina59030543
Bakinowska E, Kostopanagiotou K, Wojtyś ME, Kiełbowski K, Ptaszyński K, Gajić D, Ruszel N, Wójcik J, Grodzki T, Tomos P. Basic Operative Tactics for Pulmonary Echinococcosis in the Era of Endostaplers and Energy Devices. Medicina. 2023; 59(3):543. https://doi.org/10.3390/medicina59030543
Chicago/Turabian StyleBakinowska, Estera, Konstantinos Kostopanagiotou, Małgorzata Edyta Wojtyś, Kajetan Kiełbowski, Konrad Ptaszyński, Darko Gajić, Nikola Ruszel, Janusz Wójcik, Tomasz Grodzki, and Periklis Tomos. 2023. "Basic Operative Tactics for Pulmonary Echinococcosis in the Era of Endostaplers and Energy Devices" Medicina 59, no. 3: 543. https://doi.org/10.3390/medicina59030543