
Satisfactory In Vitro Activity of Ceftolozane–Tazobactam against Carbapenem-Resistant Pseudomonas aeruginosa But Not against Klebsiella pneumoniae Isolates

{kind=link}
Abstract
:1. Introduction
2. Results
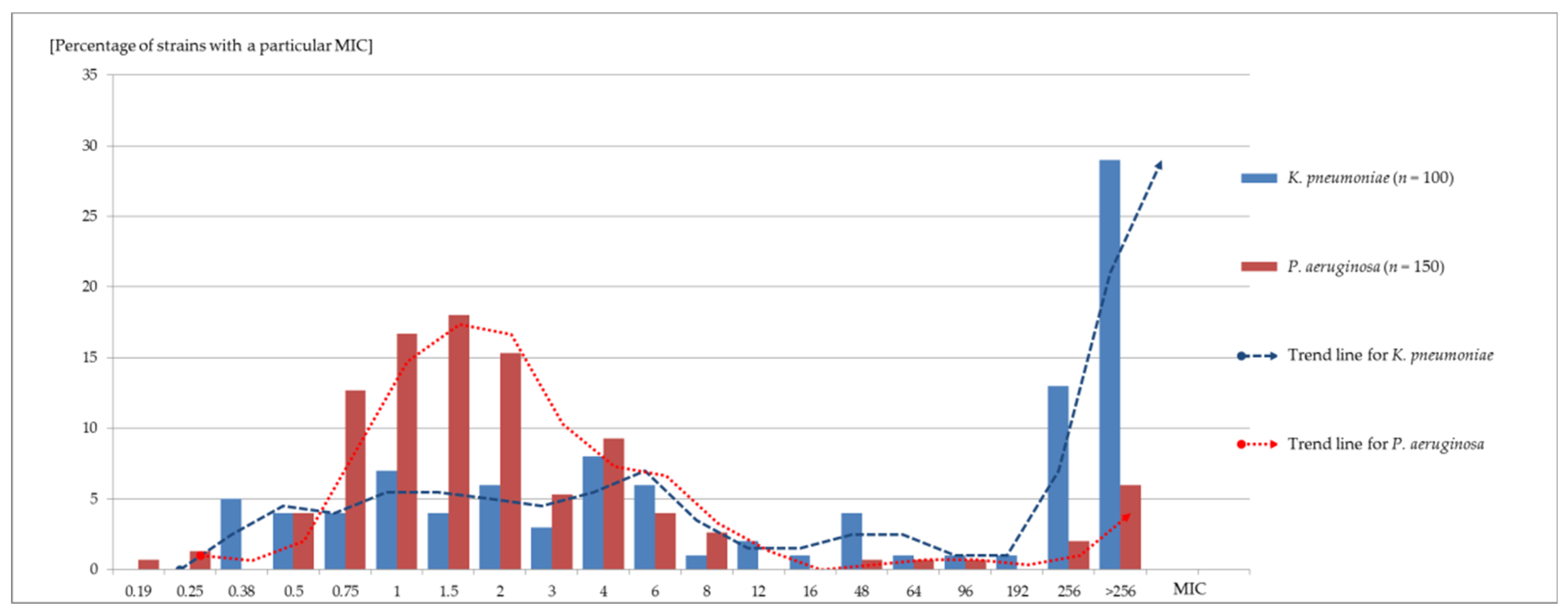
Results of Ceftolozane–Tazobactam Susceptibility Tests
3. Discussion
4. Materials and Methods
4.1. Bacterial Isolates and Their Origin
4.2. Carbapenems Susceptibility Testing and Quality Control
4.3. Carbapenemase Activity Exclusion
4.4. Extended-Spectrum Beta-Lactamase Detection
4.5. Ceftolozane–Tazobactam Sensitivity Testing
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hart, D.E.; Gallagher, J.C.; Puzniak, L.A.; Hirsch, E.B.; C/T Alliance to Deliver Real-World Evidence (CARE). A Multicenter Evaluation of Ceftolozane/Tazobactam Treatment Outcomes in Immunocompromised Patients With Multidrug-Resistant Pseudomonas aeruginosa Infections. Open Forum Infect. Dis. 2021, 8, ofab089. [Google Scholar] [CrossRef] [PubMed]
- Amanati, A.; Sajedianfard, S.; Khajeh, S.; Ghasempour, S.; Mehrangiz, S.; Nematolahi, S.; Shahhosein, Z. Bloodstream Infections in Adult Patients with Malignancy, Epidemiology, Microbiology, and Risk Factors Associated with Mortality and Multi-Drug Resistance. BMC Infect. Dis. 2021, 21, 636. [Google Scholar] [CrossRef] [PubMed]
- Han, R.; Teng, M.; Zhang, Y.; Zhang, T.; Wang, T.; Chen, J.; Li, S.; Yang, B.; Shi, Y.; Dong, Y.; et al. Choosing Optimal Antibiotics for the Treatment of Patients Infected With Enterobacteriaceae: A Network Meta-Analysis and Cost-Effectiveness Analysis. Front. Pharmacol. 2021, 12, 656790. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Shortridge, D.; Sader, H.S.; Flamm, R.K.; Castanheira, M. Ceftolozane-Tazobactam Activity against Drug-Resistant Enterobacteriaceae and Pseudomonas aeruginosa Causing Healthcare-Associated Infections in Australia and New Zealand: Report from an Antimicrobial Surveillance Program (2013–2015). J. Glob. Antimicrob. Resist. 2017, 10, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Lister, P.D.; Wolter, D.J.; Hanson, N.D. Antibacterial-Resistant Pseudomonas aeruginosa: Clinical Impact and Complex Regulation of Chromosomally Encoded Resistance Mechanisms. Clin. Microbiol. Rev. 2009, 22, 582–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tilahun, M.; Kassa, Y.; Gedefie, A.; Ashagire, M. Emerging Carbapenem-Resistant Enterobacteriaceae Infection, Its Epidemiology and Novel Treatment Options: A Review. Infect. Drug Resist. 2021, 14, 4363–4374. [Google Scholar] [CrossRef]
- Cultrera, R.; Libanore, M.; Barozzi, A.; d’Anchera, E.; Romanini, L.; Fabbian, F.; De Motoli, F.; Quarta, B.; Stefanati, A.; Bolognesi, N.; et al. Ceftolozane/Tazobactam and Ceftazidime/Avibactam for Multidrug-Resistant Gram-Negative Infections in Immunocompetent Patients: A Single-Center Retrospective Study. Antibiotics 2020, 9, E640. [Google Scholar] [CrossRef]
- Fiore, M.; Corrente, A.; Pace, M.C.; Alfieri, A.; Simeon, V.; Ippolito, M.; Giarratano, A.; Cortegiani, A. Ceftolozane-Tazobactam Combination Therapy Compared to Ceftolozane-Tazobactam Monotherapy for the Treatment of Severe Infections: A Systematic Review and Meta-Analysis. Antibiotics 2021, 10, 79. [Google Scholar] [CrossRef]
- Han, R.; Sun, D.; Li, S.; Chen, J.; Teng, M.; Yang, B.; Dong, Y.; Wang, T. Pharmacokinetic/Pharmacodynamic Adequacy of Novel β-Lactam/β-Lactamase Inhibitors against Gram-Negative Bacterial in Critically Ill Patients. Antibiotics 2021, 10, 993. [Google Scholar] [CrossRef]
- Lin, W.-T.; Lai, C.-C.; Cheong, C.-U. Novel β-Lactam/β-Lactamase Combination Versus Meropenem for Treating Nosocomial Pneumonia. Antibiotics 2019, 8, 219. [Google Scholar] [CrossRef] [Green Version]
- Caffrey, A.R.; Appaneal, H.J.; Liao, J.X.; Piehl, E.C.; Lopes, V.; Dillon, R.J.; Puzniak, L.A.; LaPlante, K.L. The Comparative Effectiveness of Ceftolozane/Tazobactam versus Aminoglycoside- or Polymyxin-Based Regimens in Multi-Drug-Resistant Pseudomonas aeruginosa Infections. Antibiotics 2022, 11, 626. [Google Scholar] [CrossRef]
- Nasomsong, W.; Nulsopapon, P.; Changpradub, D.; Pungcharoenkijkul, S.; Hanyanunt, P.; Chatreewattanakul, T.; Santimaleeworagun, W. Optimizing Doses of Ceftolozane/Tazobactam as Monotherapy or in Combination with Amikacin to Treat Carbapenem-Resistant Pseudomonas aeruginosa. Antibiotics 2022, 11, 517. [Google Scholar] [CrossRef]
- Shortridge, D.; Castanheira, M.; Pfaller, M.A.; Flamm, R.K. Ceftolozane-Tazobactam Activity against Pseudomonas aeruginosa Clinical Isolates from U.S. Hospitals: Report from the PACTS Antimicrobial Surveillance Program, 2012 to 2015. Antimicrob. Agents Chemother. 2017, 61, e00465-17. [Google Scholar] [CrossRef] [Green Version]
- Mazer, D.M.; Young, C.; Kalikin, L.M.; Spilker, T.; LiPuma, J.J. In Vitro Activity of Ceftolozane-Tazobactam and Other Antimicrobial Agents against Burkholderia cepacia Complex and Burkholderia gladioli. Antimicrob. Agents Chemother. 2017, 61, e00766-17. [Google Scholar] [CrossRef] [Green Version]
- Castón, J.J.; De la Torre, Á.; Ruiz-Camps, I.; Sorlí, M.L.; Torres, V.; Torre-Cisneros, J. Salvage Therapy with Ceftolozane-Tazobactam for Multidrug-Resistant Pseudomonas aeruginosa Infections. Antimicrob. Agents Chemother. 2017, 61, e02136-16. [Google Scholar] [CrossRef] [Green Version]
- Criscuolo, M.; Trecarichi, E.M. Ceftazidime/Avibactam and Ceftolozane/Tazobactam for Multidrug-Resistant Gram Negatives in Patients with Hematological Malignancies: Current Experiences. Antibiotics 2020, 9, E58. [Google Scholar] [CrossRef] [Green Version]
- Livermore, D.M.; Mushtaq, S.; Meunier, D.; Hopkins, K.L.; Hill, R.; Adkin, R.; Chaudhry, A.; Pike, R.; Staves, P.; Woodford, N.; et al. Activity of Ceftolozane/Tazobactam against Surveillance and “problem” Enterobacteriaceae, Pseudomonas aeruginosa and Non-Fermenters from the British Isles. J. Antimicrob. Chemother. 2017, 72, 2278–2289. [Google Scholar] [CrossRef] [Green Version]
- Solomkin, J.; Hershberger, E.; Miller, B.; Popejoy, M.; Friedland, I.; Steenbergen, J.; Yoon, M.; Collins, S.; Yuan, G.; Barie, P.S.; et al. Ceftolozane/Tazobactam Plus Metronidazole for Complicated Intra-Abdominal Infections in an Era of Multidrug Resistance: Results From a Randomized, Double-Blind, Phase 3 Trial (ASPECT-CIAI). Clin. Infect. Dis. 2015, 60, 1462–1471. [Google Scholar] [CrossRef] [Green Version]
- Stokem, K.; Zuckerman, J.B.; Nicolau, D.P.; Wungwattana, M.; Sears, E.H. Use of Ceftolozane-Tazobactam in a Cystic Fibrosis Patient with Multidrug-Resistant Pseudomonas Infection and Renal Insufficiency. Respir. Med. Case Rep. 2018, 23, 8–9. [Google Scholar] [CrossRef]
- Del Barrio-Tofiño, E.; López-Causapé, C.; Cabot, G.; Rivera, A.; Benito, N.; Segura, C.; Montero, M.M.; Sorlí, L.; Tubau, F.; Gómez-Zorrilla, S.; et al. Genomics and Susceptibility Profiles of Extensively Drug-Resistant Pseudomonas aeruginosa Isolates from Spain. Antimicrob. Agents Chemother. 2017, 61, e01589-17. [Google Scholar] [CrossRef] [Green Version]
- Skalweit, M.J. Profile of Ceftolozane/Tazobactam and Its Potential in the Treatment of Complicated Intra-Abdominal Infections. Drug Des. Dev. Ther. 2015, 9, 2919–2925. [Google Scholar] [CrossRef] [Green Version]
- Eucast: Clinical Breakpoints and Dosing of Antibiotics. Available online: https://www.eucast.org/clinical_breakpoints (accessed on 9 October 2022).
- Saran, O.; Sulik-Tyszka, B.; Basak, G.W.; Wróblewska, M.M. Activity of Ceftolozane/Tazobactam Against Gram-Negative Rods of the Family Enterobacteriaceae and Pseudomonas spp. Isolated from Onco-Hematological Patients Hospitalized in a Clinical Hospital in Poland. Med. Sci. Monit. 2019, 25, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Shortridge, D.; Streit, J.; Pfaller, M.; Tulloch, M.; Chen, W.-T.; Castanheira, M. Activity of Ceftolozane-Tazobactam Against Gram-Negative Isolates from Australia and New Zealand as Part of the PACTS Surveillance 2016–2018. J. Glob. Antimicrob. Resist. 2022, 31, 98–103. [Google Scholar] [CrossRef] [PubMed]
- García-Betancur, J.C.; De La Cadena, E.; Mojica, M.F.; Hernández-Gómez, C.; Correa, A.; Radice, M.A.; Castañeda-Méndez, P.; Jaime-Villalon, D.A.; Gales, A.C.; Munita, J.M.; et al. Comparative In Vitro Activity of Ceftolozane/Tazobactam against Clinical Isolates of Pseudomonas aeruginosa and Enterobacterales from Five Latin American Countries. Antibiotics 2022, 11, 1101. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, C.A.; Nicolau, D.P. Potency of Parenteral Antimicrobials Including Ceftolozane/Tazobactam against Nosocomial Respiratory Tract Pathogens: Considerations for Empiric and Directed Therapy. J. Thorac. Dis. 2017, 9, 214–221. [Google Scholar] [CrossRef] [Green Version]
- Tantisiriwat, W.; Buppanharun, J.; Ekpanyaskul, C.; Onruang, K.; Yungyuen, T.; Kiratisin, P.; Santiwatanakul, S. In Vitro Activity of Ceftolozane-Tazobactam and Other Antibiotics against Pseudomonas aeruginosa Infection-Isolates from an Academic Medical Center in Thailand. Antibiotics 2022, 11, 732. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, M.D.; McMullen, A.R.; Wallace, M.A.; Crotty, M.P.; Ritchie, D.J.; Burnham, C.A.D. Susceptibility of Ceftolozane-Tazobactam and Ceftazidime-Avibactam Against a Collection of β-Lactam-Resistant Gram-Negative Bacteria. Ann. Lab. Med. 2017, 37, 174–176. [Google Scholar] [CrossRef]
- Grupper, M.; Sutherland, C.; Nicolau, D.P. Multicenter Evaluation of Ceftazidime-Avibactam and Ceftolozane-Tazobactam Inhibitory Activity against Meropenem-Nonsusceptible Pseudomonas aeruginosa from Blood, Respiratory Tract, and Wounds. Antimicrob. Agents Chemother. 2017, 61, e00875-17. [Google Scholar] [CrossRef] [Green Version]
- Klinker, K.P.; Hidayat, L.K.; Wenzler, E.; Balada-Llasat, J.-M.; Motyl, M.; DeRyke, C.A.; Bauer, K.A. Use of Novel Antibiograms to Determine the Need for Earlier Susceptibility Testing and Administration for New β-Lactam/β-Lactamase Inhibitors in the United States. Antibiotics 2022, 11, 660. [Google Scholar] [CrossRef]
- Sader, H.S.; Carvalhaes, C.G.; Duncan, L.R.; Flamm, R.K.; Shortridge, D. Susceptibility Trends of Ceftolozane/Tazobactam and Comparators When Tested against European Gram-Negative Bacterial Surveillance Isolates Collected during 2012–18. J. Antimicrob. Chemother. 2020, 75, 2907–2913. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Shortridge, D.; Sader, H.S.; Gales, A.; Castanheira, M.; Flamm, R.K. Ceftolozane-Tazobactam Activity against Drug-Resistant Enterobacteriaceae and Pseudomonas aeruginosa Causing Healthcare-Associated Infections in Latin America: Report from an Antimicrobial Surveillance Program (2013–2015). Braz. J. Infect. Dis. 2017, 21, 627–637. [Google Scholar] [CrossRef]
- Sid Ahmed, M.A.; Khan, F.A.; Hadi, H.A.; Skariah, S.; Sultan, A.A.; Salam, A.; Al Khal, A.L.; Söderquist, B.; Ibrahim, E.B.; Omrani, A.S.; et al. Association of BlaVIM-2, BlaPDC-35, BlaOXA-10, BlaOXA-488 and BlaVEB-9 β-Lactamase Genes with Resistance to Ceftazidime–Avibactam and Ceftolozane–Tazobactam in Multidrug-Resistant Pseudomonas Aeruginosa. Antibiotics 2022, 11, 130. [Google Scholar] [CrossRef]
- Sader, H.S.; Mendes, R.E.; Streit, J.M.; Carvalhaes, C.G.; Castanheira, M. Antimicrobial Susceptibility of Gram-Negative Bacteria from Intensive Care Unit and Non-Intensive Care Unit Patients from United States Hospitals (2018–2020). Diagn. Microbiol. Infect. Dis. 2022, 102, 115557. [Google Scholar] [CrossRef]
- Gallagher, J.C.; Satlin, M.J.; Elabor, A.; Saraiya, N.; McCreary, E.K.; Molnar, E.; El-Beyrouty, C.; Jones, B.M.; Dixit, D.; Heil, E.L.; et al. Ceftolozane-Tazobactam for the Treatment of Multidrug-Resistant Pseudomonas aeruginosa Infections: A Multicenter Study. Open Forum Infect. Dis. 2018, 5, ofy280. [Google Scholar] [CrossRef]
- Goodlet, K.J.; Nicolau, D.P.; Nailor, M.D. Ceftolozane/Tazobactam and Ceftazidime/Avibactam for the Treatment of Complicated Intra-Abdominal Infections. Ther. Clin. Risk Manag. 2016, 12, 1811–1826. [Google Scholar] [CrossRef] [Green Version]
- European Antimicrobial Resistance Surveillance Network (EARS-Net). Available online: https://www.ecdc.europa.eu/en/about-us/partnerships-and-networks/disease-and-laboratory-networks/ears-net (accessed on 9 October 2022).
- Bianco, G.; Lombardo, D.; Ricciardelli, G.; Boattini, M.; Comini, S.; Cavallo, R.; Costa, C.; Ambretti, S. Multicentre Evaluation of the EUCAST Rapid Antimicrobial Susceptibility Testing (RAST) Extending Analysis to 16–20 Hours Reading Time. Antibiotics 2022, 11, 1404. [Google Scholar] [CrossRef]
- Lee, K.; Lim, Y.S.; Yong, D.; Yum, J.H.; Chong, Y. Evaluation of the Hodge Test and the Imipenem-EDTA Double-Disk Synergy Test for Differentiating Metallo-β-Lactamase-Producing Isolates of Pseudomonas Spp. and Acinetobacter spp. J. Clin. Microbiol. 2003, 41, 4623–4629. [Google Scholar] [CrossRef] [Green Version]
- Yong, D.; Lee, K.; Yum, J.H.; Shin, H.B.; Rossolini, G.M.; Chong, Y. Imipenem-EDTA Disk Method for Differentiation of Metallo-β-Lactamase-Producing Clinical Isolates of Pseudomonas spp. and Acinetobacter spp. J. Clin. Microbiol. 2002, 40, 3798–3801. [Google Scholar] [CrossRef] [Green Version]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sękowska, A.; Grabowska, M.; Bogiel, T. Satisfactory In Vitro Activity of Ceftolozane–Tazobactam against Carbapenem-Resistant Pseudomonas aeruginosa But Not against Klebsiella pneumoniae Isolates. Medicina 2023, 59, 518. https://doi.org/10.3390/medicina59030518
Sękowska A, Grabowska M, Bogiel T. Satisfactory In Vitro Activity of Ceftolozane–Tazobactam against Carbapenem-Resistant Pseudomonas aeruginosa But Not against Klebsiella pneumoniae Isolates. Medicina. 2023; 59(3):518. https://doi.org/10.3390/medicina59030518
Chicago/Turabian StyleSękowska, Alicja, Marta Grabowska, and Tomasz Bogiel. 2023. "Satisfactory In Vitro Activity of Ceftolozane–Tazobactam against Carbapenem-Resistant Pseudomonas aeruginosa But Not against Klebsiella pneumoniae Isolates" Medicina 59, no. 3: 518. https://doi.org/10.3390/medicina59030518