
The Effect of Dentine Desensitizing Agents on the Retention of Cemented Fixed Dental Prostheses: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Permission and Registration
2.2. Search Criteria
2.3. Screening, Selection of Studies, and Data Extraction
2.4. Quality Assessment of the Included Studies
3. Results
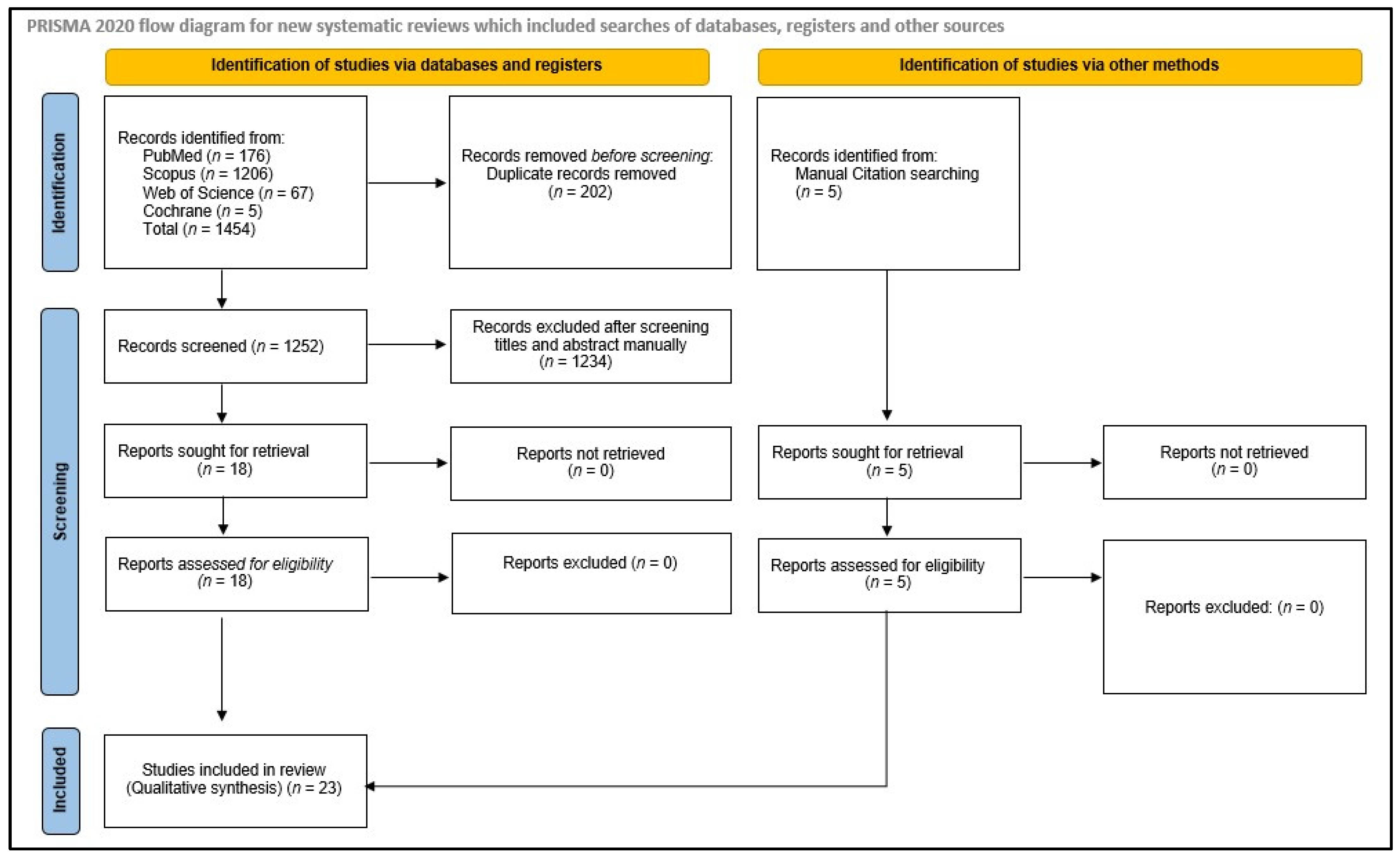
3.1. Identification and Screening
3.2. Characteristics of the Selected Studies
3.3. Findings of Quality Analysis
3.4. Results of Individual Studies
4. Discussion
5. Conclusions
- The type of dentine desensitizing agent and luting agent used affect the retention values of the cemented FDPs.
- In general, the retention values of FDPs cemented using zinc phosphate cement are reduced with most of the DAs, whereas retention values increase when GIC, resin-modified GIC, and resin cements are used with the majority of DAs.
- Blinding protocols should be followed in future in vitro studies to avoid bias.
- Dentists should have knowledge regarding the compatibility of DAs and luting cements in order to provide the best treatment to their patients.
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shillingburg, H.T.; Hobo, S.; Whit, L.D. Fundamentals of Fixed Prosthodontics, 2nd ed.; Quintessence: Chicago, IL, USA, 1981. [Google Scholar]
- Krauser, J.T. Hypersensitive teeth. Part I: Etiology. J. Prosthet. Dent. 1986, 56, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Richardson, D.; Tao, L.; Pashley, D.H. Dentin permeability: Effects of crown preparation. Int. J. Prosthodont. 1991, 4, 219–225. [Google Scholar] [PubMed]
- Watson, T.F.; Flanagan, D.; Stone, D.G. High and low torque handpieces: Cutting dynamics, enamel cracking and tooth temperature. Br. Dent. J. 2000, 188, 680–686. [Google Scholar] [CrossRef] [PubMed]
- Outhwaite, W.C.; Livingston, M.; Pashiey, D.H. Effects of changes in surface area, thickness, temperature and postextraction tirne on human dentin permeability. Arch. Oral Biol. 1976, 21, 599–603. [Google Scholar] [CrossRef]
- Reeder, O.W.; Walton, R.E.; Livingston, M.J.; Pashley, D.H. Dentin permeability: Determinants ot hydraulic conductance. J. Dent. Res. 1978, 57, 187–193. [Google Scholar] [CrossRef]
- Fogei, H.M.; Marshall, F.; Pashley, D.H. Effects of distance from the pulp and thiciiness on the permeability of human radicular dentin. J. Dent. Res. 1991, 67, 1381. [Google Scholar]
- Chandavarkar, S.M.; Ram, S.M. A comparative evaluation of the effect of dentin desensitizers on the retention of complete cast metal crowns. Contemp. Clin. Dent. 2015, 6 (Suppl. 1), S45–S50. [Google Scholar] [CrossRef]
- Garberoglio, R.; Brännström, M. Scanning electron microscopic investigation of human dentinal tubules. Arch. Oral Biol. 1976, 21, 355–3562. [Google Scholar] [CrossRef]
- Pilo, R.; Harel, N.; Nissan, J.; Levartovsky, S. The retentive strength of cemented zirconium oxide crowns after dentin pretreatment with desensitizing paste containing 8% arginine and calcium carbonate. Int. J. Mol. Sci. 2016, 17, 426. [Google Scholar] [CrossRef] [Green Version]
- Mapkar, M.A.; Jagtap, A.; Asadullah, S.R.S. Effect of two desensitizing agents on crown retention using zinc phosphate cement. Int. J. Oral Care Res. 2018, 6, 64–68. [Google Scholar]
- Wolfart, S.; Linnemann, J.; Kern, M. Crown retention with use of different sealing systems on prepared dentine. J. Oral Rehabil. 2003, 30, 1053–1061. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.C.; Ruse, N.D. Acidity of glass ionomer cements during cementation and its relation to pulp sensitivity. JADA 1986, 112, 654–657. [Google Scholar]
- Watanabe, T.; Sano, M.; Itoh, K.; Wakumoto, S. The effects of primers on the sensitivity of dentin. Dent. Mater. 1991, 7, 148–150. [Google Scholar] [CrossRef] [PubMed]
- Dhondi dall’Orologio, G.; Malferrari, S. Desensitizing effects of Gluma and Gluma 2000 on hypersensitive dentin. Am. J. Dent. 1993, 6, 283–286. [Google Scholar]
- Felton, D.A.; Bergenholtz, G.; Kanoy, B.E. Evaluation of the desensitizing effect of Gluma dentin bond on teeth prepared for complete-coverage restorations. Int. J. Prosthodont. 1991, 4, 292–298. [Google Scholar]
- Bergenholtz, G.; Jontell, M.; Tuttle, A.; Knutsson, G. Inhibition of serum albumin flux across exposed dentine following conditioning with GLUMA primer, glutaraldehyde or potassium oxalates. J. Dent. 1993, 21, 220–227. [Google Scholar] [CrossRef]
- Jalandar, S.S.; Pandharinath, D.S.; Arun, K.; Smita, V. Comparison of effect of desensitizing agents on the retention of crowns cemented with luting agents: An in vitro study. J. Adv. Prosthodont. 2012, 4, 127–133. [Google Scholar] [CrossRef] [Green Version]
- Stawarczyk, B.; Hartmann, L.; Hartmann, R.; Roos, M.; Ender, A.; Özcan, M.; Sailer, I.; Hämmerle, C.H.F. Impact of Gluma Desensitizer on the tensile strength of zirconia crowns bonded to dentin: An in vitro study. Clin. Oral Investig. 2012, 16, 201–213. [Google Scholar] [CrossRef] [Green Version]
- Patel, P.; Thummar, M.; Shah, D.; Pitti, V. Comparing the effect of a resin based sealer on crown retention for three types of cements: An in vitro study. J. Indian Prosthodont. Soc. 2013, 13, 308–314. [Google Scholar] [CrossRef]
- Fambrini, E.; Miceli, M.; Pasini, M.; Giuca, M.R. Clinical evaluation of the use of desensitizing agents in the management of dentinal hypersensitivity. Appl. Sci. 2022, 12, 11238. [Google Scholar] [CrossRef]
- Najibfard, K.; Ramalingam, K.; Chedjieu, I.; Amaechi, B.T. Remineralization of early caries by a nano-hydroxyapatite dentifrice. J. Clin. Dent. 2011, 22, 139–143. [Google Scholar]
- de Melo Alencar, C.; de Paula, B.L.F.; Guanipa Ortiz, M.I.; Barauna Magno, M.; Martins Silva, C.; Cople Maia, L. Clinical efficacy of nano-hydroxyapatite in dentin hypersensitivity: A systematic review and meta-analysis. J. Dent. 2019, 82, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Tolentino, A.B.; Zeola, L.F.; Fernandes, M.R.U.; Pannuti, C.M.; Soares, P.V.; Aranha, A.C.C. Photobiomodulation therapy and 3% potassium nitrate gel as treatment of cervical dentin hypersensitivity: A randomized clinical trial. Clin. Oral. Investig. 2022, 26, 6985–6993. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kwon, H.; Kim, B. Effect of dentinal tubule occlusion by dentifrice containing nano-carbonate apatite. J. Oral Rehabil. 2008, 35, 847–853. [Google Scholar] [CrossRef]
- Matsuura, T.; Mae, M.; Ohira, M.; Mihara, Y.; Yamashita, Y.; Sugimoto, K.; Yamada, S.; Yoshimura, A. The efficacy of a novel zinc-containing desensitizer CAREDYNE Shield for cervical dentin hypersensitivity: A pilot randomized controlled trial. BMC Oral Health 2022, 22, 294. [Google Scholar] [CrossRef] [PubMed]
- Shillinberg, H.T., Jr.; Sumiya, H.; Whitsett, L.D.; Richard, J.; Brackette, S.E. Fundamentals of Fixed Prosthodontics, 3rd ed.; Quintessence: Chicago, IL, USA, 1997; pp. 119–128. [Google Scholar]
- Rosenstiel, S.F.; Land, M.F.; Fujimoto, J. Contemporary Fixed Prosthodontics, 4th ed.; Mosby Inc.: St. Louis, MI, USA, 2006; pp. 226–243. [Google Scholar]
- Tyllman, S.D.; Malone, W.F.; Koth, D.L.; Edmund, C., Jr.; Kaiser, D.A.; Margano, S.M. Theory and Practice of Fixed Prosthodontics, 8th ed.; Medico Dental Media International Inc.: New York, NY, USA, 2001; pp. 113–135. [Google Scholar]
- Ayad, M.F.; Johnston, W.M.; Rosenstiel, S.F. Influence of tooth preparation taper and cement type on recementation strength of complete metal crowns. J. Prosthet. Dent. 2009, 102, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Lawaf, S.; Jalalian, E.; Roshan, R.; Azizi, A. Effect of GLUMA desensitizer on the retention of full metal crowns cemented with Rely X U200 self-adhesive cement. J. Adv. Prosthodont. 2016, 8, 404–410. [Google Scholar] [CrossRef] [Green Version]
- Al-Omari, W.M.; Al-Wahadni, A.M. Convergence Angle, Occlusal Reduction, and Finish Line Depth of Full-Crown Preparations Made by Dental Students; Quintessence: Chicago, IL, USA, 2004; Volume 35, pp. 287–293. [Google Scholar]
- Zidan, O.; Ferguson, G.C. The retention of complete crowns prepared with three different tapers and luted with four different cements. J. Prosthet. Dent. 2003, 89, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Johnson, G.H.; Lepe, X.; Bales, D.J. Crown retention with use of a 5% glutaraldehyde sealer on prepared dentin. J. Prosthet. Dent. 1998, 79, 671–676. [Google Scholar] [CrossRef] [PubMed]
- Himashilpa, G.V.R.; Ravishankar, Y.; Srinivas, K.; Harikrishna, M.; Shameen Kumar, P.; Satyendra, T. Influence of desensitizing agents on the retention quality of Complete cast crowns cemented with various luting agents—An in-vitro study. J. Sci. Res. 2019, 8, 1–4. [Google Scholar]
- Swift, E.J., Jr.; Lloyd, A.H.; Felton, D.A. The effect of resin desensitizing agents on crown retention. JADA 1997, 128, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Yim, N.H.; Rueggeberg, F.A.; Caughman, W.F.; Gardner, F.M.; Pashley, D.H. Effect of dentin desensitizers and cementing agents on retention of full crowns using standardized crown preparations. J. Prosthet. Dent. 2000, 83, 459–465. [Google Scholar] [CrossRef]
- Sipahi, C.; Cehreli, M.; Ozen, J.; Dalkiz, M. Effects of precementation desensitizing laser treatment and conventional desensitizing agents on crown retention. Int. J. Prosthodont. 2007, 20, 289–292. [Google Scholar] [PubMed]
- Pilo, R.; Agar-Zoizner, S.; Gelbard, S.; Levartovsky, S. The retentive strength of laser-sintered cobalt-chromium-based crowns after pretreatment with a desensitizing paste containing 8% arginine and calcium carbonate. Int. J. Mol. Sci. 2018, 19, 4082. [Google Scholar] [CrossRef] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mausner, I.K.; Goldstein, G.R.; Georgescu, M. Effect of two dentinal desensitizing agents on retention of complete cast coping using four cements. J. Prosthet. Dent. 1996, 75, 129–134. [Google Scholar] [CrossRef]
- Johnson, G.H.; Hazelton, L.R.; Bales, D.J.; Lepe, X. The effect of a resin-based sealer on crown retention for three types of cement. J. Prosthet. Dent. 2004, 91, 428–435. [Google Scholar] [CrossRef]
- Chandrasekaran, A.P.; Deepan, N.; Rao, B.K.; Pai, S.; Sonthalia, A.; Bettanpalya, S.V. Evaluation of the effect of desensitizing agents on the retention of complete cast crowns: An in vitro study. SRM J. Res. Dent. Sci. 2014, 5, 174. [Google Scholar] [CrossRef]
- Kumar, S.; Rupesh, P.L.; Kalekar, S.G.A.; Ghunawat, D.B.; Siddiqui, S. Effect of desensitising laser treatment on the bond strength of full metal crowns: An in vitro comparative study. J. Int. Oral Health 2015, 7, 36–41. [Google Scholar]
- Janapala, S.D.R.; Reddy, P.S.; Jain, A.R.; Pradeep, R. The effect of three dentinal sealers on retention of crowns cemented with resin-modified glass ionomer cement: An in vitro study. March World J. Dent. 2015, 6, 10–15. [Google Scholar]
- Syed Asadullah, S.R.; Rakhewar, P.; Mapkar, M.A. Comparison of effect of desensitizing agents on the retention of crowns cemented with resinomer cement: An in vitro study. Int. J. Prev. Clin. Dent. Res. 2018, 5, 5–9. [Google Scholar]
- Kottem, S.; Dileep, N.V.; Divi, V.V.V.K.; Srinivas, R.P. Evaluation of freshly prepared “arginine-calcium carbonate-fluoride” and “casein phosphopeptide-amorphous calcium phosphate-fluoride” desensitizing agents on crown retention: An in vitro study. World J. Dent. 2020, 11, 355–360. [Google Scholar]
- Seba, H.; Ebtisam, L. The influence of systemp desensitizer on the retention quality of Complete cast crowns cemented by glass ionomer and resin modified glass Ionomer cements (in-vitro study). Int. J. Recent Sci. Res. 2021, 12, 41662–41669. [Google Scholar]
- Dewan, H.; Sayed, M.E.; Alqahtani, N.M.; Alnajai, T.; Qasir, A.; Chohan, H. The effect of commercially available desensitizers on bond strength following cementation of zirconia crowns using self-adhesive resin cement—An in vitro study. Materials 2022, 15, 514. [Google Scholar] [CrossRef] [PubMed]
- Faggion, C.M., Jr. Guidelines for reporting pre-clinical in vitro studies on dental materials. J. Evid. Based Dent. Pract. 2012, 12, 182–189. [Google Scholar] [CrossRef]
- Krithikadatta, J.; Datta, M.; Gopikrishna, V. CRIS guidelines (checklist for reporting in-vitro studies): A concept note on the need for standardized guidelines for improving quality and transparency in reporting in-vitro studies in experimental dental research. J. Conserv. Dent. 2014, 17, 301–304. [Google Scholar] [CrossRef] [Green Version]
- Johnson, G.H.; Powell, L.V.; DeRouen, T.A. Evaluation and control of post-cementation pulpal sensitivity: Zinc phosphate and glass ionomer luting cements. J. Am. Dent. Assoc. 1993, 124, 38–46. [Google Scholar] [CrossRef]
- Jackson, C.R.; Skidmore, A.E.; Rice, R.T. Pulpal evaluation of teeth restored with fixedprostheses. J. Prosthet. Dent. 1992, 67, 323–325. [Google Scholar] [CrossRef]
- Brannstrom, M.; Linden, L.A.; Astrom, A. The hydrodynamics of the dental tubule and ofpulp fluid. Caries Res. 1967, 1, 310–317. [Google Scholar] [CrossRef]
- Nicholson, J.W.; Croll, T.P. Glass-ionomer cements in restorative dentistry. Quintessence 1997, 28, 705–714. [Google Scholar]
- Pace, L.L.; Hummel, S.K.; Marker, V.A.; Bolouri, A. Comparison of the flexural strength of five adhesive resin cements. J. Prosthodont. 2007, 16, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Arrais, C.A.; Chan, D.C.; Giannini, M. Effects of desensitizing agents on dentinal tubule occlusion. J. Appl. Oral Sci. 2004, 12, 144–148. [Google Scholar] [CrossRef]
- Ceballo, L.; Toledano, M.; Osorio, R.; Tay, F.R.; Marshall, G.W. Bonding to Er-YAG-laser-treated dentin. J. Dent. Res. 2002, 81, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Munksgaard, E.C.; Asmussen, E. Bond strength between dentin and restorative resins mediated by mixtures of HEMA and glutaraldehyde. J. Dent. Res. 1984, 63, 1087–1089. [Google Scholar] [CrossRef]
- Qin, C.; Xu, J.; Zhang, Y. Spectroscopic investigation of the function of aqueous 2-hydroxyethylmethacrylate/glutaraldehyde solution as a dentin desensitizer. Eur. J. Oral Sci. 2006, 114, 354–359. [Google Scholar] [CrossRef]
- Acar, O.; Tuncer, D.; Yuzugullu, B.; Celik, C. The effect of dentin desensitizers and Nd: YAG laser pre-treatment on microtensile bond strength of self-adhesive resin cement to dentin. J. Adv. Prosthodont. 2014, 6, 88–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalil, A.; Khalid, A.; Ziad, N.A.-D.; Hani, A.; Abdulrhman, A.; Abdulaziz, A.; Edward, L. Retention of zirconium oxide copings using different types of luting agents. J. Dent. Sci. 2013, 8, 392–398. [Google Scholar]
- Monticelli, F.; Osorio, R.; Mazzitelli, C.; Ferrari, M.; Toledano, M. Limited decalcification/diffusion of self-adhesive cements into dentin. J. Dent. Res. 2008, 87, 974–979. [Google Scholar] [CrossRef]
- Pathak, S.; Shashibhushan, K.K.; Poornima, P.; Reddy, V.V.S. In Vitro evaluation of stainless steel crowns cemented with resin-modified glass Ionomer and two new self-adhesive resin cements. Int. J. Clin. Pediatr. Dent. 2016, 9, 197–200. [Google Scholar] [CrossRef]
- Sabatini, C.; Patel, M.; D’Silva, E. In Vitro shear bond strength of three self adhesive resin cements and a resin-modified glass ionomer cement to various prosthodontic substrates. Oper. Dent. 2013, 38, 186–196. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Author, Year and Country | Study Design | Sample Size | Abutment Type | Specimen Fabrication Technique | Type of FDP (Single Crown, 3 Unit FPD) and Fabrication Technique | Control | Intervention | Name of DA (Manufacturer) | Main Chemical Composition | Type of Cement, Trade Name and Manufacturer | Test and Machine Used | Mean TBS (N)/ Retentive Strength (MPa) | Primary Outcomes | Secondary Outcomes | Authors’ Suggestions/Conclusions/ Inferences |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mausner et al., 1996, USA [41] | In vitro | n = 96 (16 per group) | Human Third molars | Finish line: rounded shoulder/bevel Axial height: 5 mm Taper: 6–10° Spacer: 3 coats Ageing: No | Full metal silver–palladium alloy copings (Ceradela 2, Metalor, Neuchatel, Switzerland) Fabrication technique: lost wax casting | No DA applied | Application of DA before final cementation | (A) Imperva bonding agent (IBA) (Shofu Dental Corp., Menlo Park, CA, USA) (B) All-Bond (AB) desensitizing agent (Bisco Inc., Itasca, IL, USA) | (A) HEMA & UDMA & TEGMA (B) NTG-GMA & BPDM | (i) ZPC (Flecks Mizzy, Mizzy, Inc., Cherry Hill, NJ, USA) (ii) PCC (Duralon, Espe-Premier, Norristown, PA, USA), (iii) GIC (Ketec Cem Maxicaps, Espe-Premier, St. Paul, MN, USA), (iv) RC (NM) | Retention values, UTM | Retention values (N) (A) ZPC: 383.28 ± 62.17 (B) ZPC + IBA DA: 354.89 ± 84.06 (C) ZPC + AB DA: 187.48 ± 50.18 (D) PCC: 335.97 ± 54.29 (E) PCC + IBA DA: 388.26 ± 34.53 (F) PCC + AB DA: 42.85 ± 14.24 (G) GIC: 234.74 ± 64.70 (H) GIC+ IBA DA: 135.73 ± 41.39 (I) GIC + AB DA: 211.37 ± 39.43 (J) RC: 289.25 ± 116.10 (K) RC + IBA DA: 485.05 ± 117.21 (L) RC + AB DA: 406.06 ± 132.61 | Retention values: RC + IBA DA > RC + AB DA > PCC + IBA DA > ZPC > ZPC + IBA DA > PCC > RC > GIC > GIC + AB DA > ZPC + AB DA > GIC+ IBA DA > PCC + AB DA | Retention values: ZPC > PCC > RC > GIC | In general, application of DA reduced the retention in most of the tested specimens when cemented with ZPC, PCC or GIC, whereas retention increased when RC was used. |
| Swift et al., 1997, USA [36] | In vitro | n = 30 (10 per group) | Human molars | Finish line: NM Axial height: 4 mm Taper: 2.4° per wall Spacer: NM Ageing: No | Full metal silver–palladium copings (Ney-Oro 76, Ney Dental International) Fabrication technique: lost wax casting | No DA applied | Application of DA before final cementation | (A) One step (Bisco Dental Products, Schaumburg, IL, USA) (B) Gluma (Heraeus Kulzer, South Bend, IN, USA) | (A) phosphoric acid with Benzalkonium Chloride (B) glutaraldehyde and HEMA | (i) ZPC (Hy-Bond, Shofu Inc., Koyoto, Japan) (ii) GIC ((Fuji I, GC America Inc., Alsip, IL, USA) (iii) RMGIC (Vitremer Luting Cement, 3M Dental Products Division, St. Paul, MN, USA) | Mean force for removing crown, UTM | Mean force for removing crown (N) (A) ZPC: 587 ± 400 (B) ZPC + One step DA: 479 ± 215 (C) ZPC + Gluma DA: 449 ± 277 (D) GIC: 788 ± 401 (E) GIC + One Step DA: 872 ± 342 (F) GIC + Gluma DA: 653 ± 234 (G) RMGIC: 685 ± 156 (H) RMGIC + One Step DA: 713 ± 191 (I) RMGIC + Gluma DA: 748 ± 306 | Mean force for removing crown GIC + One Step DA > GIC > RMGIC + RMGIC + Gluma DA + One Step DA > RMGIC > GIC + Gluma DA > ZPC > ZPC + One step DA > ZPC + Gluma DA | Retention GIC > RMGIC > ZPC | Use of DA does not affect the retentive properties of the three tested luting cements. |
| Johnson et al., 1998, USA [34] | In vitro | n = 60 (10 per group) | Human molars | Finish line: chamfer Axial height: 4 mm Taper: 20° Spacer: 3 coats Ageing: No | Full base metal alloy copings (Olympia porcelain metal alloy, Jelenko Dental Products, Armonk, NY, USA) Fabrication technique: lost wax casting | No DA applied | Application of DA before final cementation | Gluma Desensitizer sealer (Heraeus/Kulzer, Dental Products Division, South Bend, IN, USA) | 5% glutaraldehyde + HEMA | (i) ZPC (Fleck’s, Mizzy Inc., Cherry Hill, NJ, USA) (ii) GIC (Ketac-Cem Maxicap, ESPE Gmbh, Seefeld, Germany) (iii) Modified RC (Resinomer, Bisco, Inc., Schaumburg, IL, USA) | Failure stress, UTM | Failure stress (MPa) (A) ZPC: 6.3 (B) ZPC + Gluma DA: 6.4 (C) GIC:9.1 (D) GIC + Gluma DA:10.1 (E) Modified RC: 12.1 (F) Modified RC + Gluma DA: 12.6 | Failure stress: RC + DA > RC > GIC + DA > GIC > ZPC + DA > ZPC | RC > GIC > ZPC | Application of Gluma DA for desensitizing treatment does not affect retention of crowns cemented with the tested luting agents. |
| Yim et al., 2000, Georgia [37] | In vitro | n = 144 (12 per group) | Human molars | Finish line: Chamfer Axial height: 4 mm Taper: 26° Spacer: 2 coats Ageing: No | Full metal Ni-Cr crown Fabrication technique: lost wax casting | No DA | Application of DA before final cementation | (A) PD (All-Bond 2, BISCO Dental Products, Schaumburg, IL, USA) (B) NPD (Gluma Desensitizer, Heraeus Kulzer, South Bend, IN, USA) | (A) Photopolymerizable, resin-based DA (B) Nonpolymerizing, protein-precipitating, resin-based DA | (i) ZPC (Fleck’s Cement, Mizzy Inc., Cherry Hill, NJ, USA) (ii) GIC (Ketac Cem, ESPE GmbH, Seefeld, Germany) (iii) RMGIC (Fuji Plus, GC Corporation, Tokyo, Japan) (iv) RC (Panavia 21, J. Morita, Tustin, CA, USA) | Debond Stress; UTM | Debond Stress (MPa): (A) ZPC + PD DA: 0.67 ± 0.14 (B) ZPC + NPD DA: 0.81 ± 0.11 C) ZPC: 1.68 ± 0.08 (D) GIC + PD DA: 2.23 ± 0.20 (E) GIC + NPD DA: 1.98 ± 0.23 F) GIC: 2.36 ± 0.20 (G) RMGIC + PD DA: 3.46 ± 0.26 (H) RMGIC + NPD DA: 2.81 ± 0.15 (I) RMGIC: 2.96 ± 0.18 (J) RC + PD DA: 5.68 ± 0.70 (K) RC + NPD DA: 4.12 ± 0.37 (L) RC: 4.67 ± 0.48 | Debond Stress RC + PD DA > RC > RC + NPD DA > RMGIC + PD DA > RMGIC > RMGIC + NPD DA > GIC + PD DA > GIC > GIC + NPD DA > ZPC > ZPC + NPD DA > ZPC + PD DA | Debond Stress RC > RMGIC > GIC > ZPC | Application of NPD DA significantly decreased the retention strength when RC, GIC and ZPC were used. Application of PD DA significantly increased retention strength when RC and RMGIC was used. DA when used with ZPC significantly decreased retention strength. |
| Wolfart et al., 2003, Germany [12] | In vitro | n = 80 (10 per group) | Human premolars | Finish line: Chamfer Axial height: 4 mm Taper: 11° Spacer: yes Ageing: 3 days and 150 days (37,500 cycles) | Full metal nickel chromium alloy (Wiron 99, Bego, Germany) copings Fabrication technique: lost wax casting | Calcium Hydroxide DA applied | Application of DA before final cementation | (A) Gluma (Heraeus Kulzer) (B) Prompt L-Pop (3M-Espe, Seefeld, Germany) (C) Optibond FL (Kerr, Orange County, CA, USA) (D) Calcium hydroxide suspension (Merck, Darmstadt, Germany) | (A) 5% Glutaraldehyde and HEMA (B) Low filled resin sealer (C) Highly filled resin sealer | GIC (Ketac-Cem Maxicup,3M-Espe, Seefield, Germany) | Failure Stress, UTM | Failure Stress (MPa) After 3 days aging: ## (A) GIC + Calcium hydroxide:6.92 (B) GIC + Gluma: 6.20 (C) GIC + Prompt L-Pop: 6.62 (D) GIC + Optibond: 4.91 After 150 days aging: ## (A) GIC + Calcium hydroxide: 6.02 (B) GIC + Gluma: 5.60 (C) GIC + Prompt L-Pop: 6.9 (D) GIC + Optibond:5.01 | Failure stress After 3 days ageing: GIC + Calcium hydroxide > GIC + Prompt L-Pop > GIC + Gluma > GIC + Optibond After 150 days ageing: GIC + Prompt L-Pop > GIC + Calcium hydroxide > GIC + Gluma > GIC + Optibond | - | Gluma and Prompt L-Pop DA does not affect the retention of crowns cemented with GIC when compared to calcium hydroxide application. |
| Johnson et al., 2004; USA [42] | In vitro | n = 55 (11 per group) | Human molars | Finish line:—NA Axial height: 4 mm Taper: 20° Spacer: 1 layer Ageing: 2500 cycles | Full ceramometal high noble alloy (Olympia) copings Fabrication technique: lost wax casting | No DA applied | Application of DA before final cementation | (A) One step (Bisco Dental Products, Schaumburg, IL, USA) | Phosphoric acid with Benzalkonium Chloride | (A) ZPC (Fleck’s, Keystone Industries GmbH, Singen, Germany), (B) GIC (Ketac-Cem, ESPE Gmbh, Seefeld, Germany) (C) Modified-RC (Resinomer, Schaum-burg, IL, USA) | Dislodgment stresses, UTM | Mean dislodgment stress (MPa) (A) ZPC: 3.7 ±1.0 (B) ZPC + One step DA:2.2 ± 0.8 (C) GIC: 2.7 ± 1.2 (D) GIC + One step DA: 4.2 ± 0.9 (E) Modified-RC: 6.4 ± 1.7 | Mean dislodgment stress Modified RC > GIC + One step > ZPC > GIC > ZPC + One step | dislodgment stress: Modified RC > ZPC > GIC | Resin sealers reduced retention when used with ZPC and increased retention when used with GIC. |
| Sipahi et al., 2007, Turkey [38] | In vitro | n = 50 (10 per group) | Human molars | - | Full metal base metal alloy copings Fabrication technique: lost wax casting | No DA applied | Application of DA before final cementation | (A) Laser group (LAS), (B) sodium fluoride group (C) Oxagel oxalate group (D) Gluma primer group | - | GIC | TS, UTM | TS (N) (A) GIC: 261 (B) GIC + Laser DA: 223 (C) GIC + sodium fluoride DA: 208 (D) GIC + Oxagel DA: 147 (E) GIC + Gluma DA: 161 | Ts: GIC > GIC + Laser > GIC + sodium fluoride > GIC + Gluma > GIC + Oxagel | - | Lee negative effect of laser treatment on retention for crowns cemented with GIC, as compared to other DA. |
| Jalandar et al., 2012, India [18] | In vitro | n = 90 (10 per group) | Human molars | Finish line: Chamfer Axial height: 4 mm Taper: 6° Spacer: 35–40 µ Ageing: No | Full metal Ni-Cr crown Fabrication technique: lost wax casting | No DA | Application of DA before final cementation | (A) GC Tooth Mousse (GC International, Itabashiku, Tokyo, Japan) (B) GLUMA desensitizer (Heraeus Kulzer, Hanau, Germany). | (A) CPP-ACP-based (B) GLU-based | (i) ZPC (Harvard cement Quick setting, Harvard Dental International GmbH, Hoppegarten, Germany) (ii) GIC (GC Fuji 1Tokyo, Japan) (iii) RMGIC (RelyXTM Luting, 3M ESPE, St. Paul, MN, USA) | TBS; UTM | TBS (kg) (A) ZPC + TM DA: 25.27 ± 4.60 (B) ZPC + GLUMA DA: 27.92 ± 3.20 (C) ZPC:27.69 ± 3.39 (D) GIC + TM DA: 40.32 ± 3.89 (E) GIC + GLUMA DA: 41.14 ± 2.42 (F) GIC: 39.09 ± 2.80 (G) RMGIC + TM DA: 48.34 ± 2.94 (H) RMGIC + GLUMA DA: 49.02 ± 3.32 (I) RMGIC: 48.61 ± 3.54 | TBS: RMGIC + GLUMA DA > RMGIC > RMGIC + TM DA > GIC + GLUMA DA > GIC + TM DA > GIC > ZPC + GLUMA DA > ZPC > ZPC + TM DA | TBS: RMGIC > GIC > ZPC | GLUMA DA improves retention of cast crowns with ZPC, GIC, RMGIC. Tooth Mousse DA improves retention of cast crowns with GIC, RMGIC and reduces retention for ZPC. |
| Stawarczyk et al., 2012, Switzerland [19] | In vitro | n = 144 (12 per group) | Human molars | Finish line: Shoulder Axial height: 3 mm Taper: 10° Spacer: 35–40 µ Ageing: half specimens were aged—chewing machine, 6000 cycles | Zirconia crowns Fabrication technique: CAD/CAM milled | No DA | Application of DA before final cementation | Gluma Desensitizer (Haereus Kulzer, Hanau, Germany) | HEMA, glutaraldehyde | (i) Panavia 21 (Kuraray Dental Co. Ltd., Osaka, Japan) (ii) RelyX Unicem (3M ESPE, Seefeld, Germany) (iii) G-Cem (GC, Leuven, Belgium) | TS; UTM | Tensile strength (MPa) Initial (A) Panavia 21 + Gluma DA: 2.6 ± 1.4 (B) Panavia 21: 14.1 ± 3.5 (C) RelyX Unicem + Gluma DA: 13.1 ± 2.9 (D) RelyX Unicem: 12.8 ± 2.9 (E) G-Cem + Gluma DA: 13.7 ± 4.2 (F) G-Cem: 10.7 ± 2.9 After Ageing (A) Panavia 21 + Gluma DA: 0.9 ± 0.6 (B) Panavia 21: 7.3 ± 1.7 (C) RelyX Unicem + Gluma DA: 12.8 ± 4.3 (D) RelyX Unicem: 9.1 ± 3 (E) G-Cem + Gluma DA: 13.4 ± 6.2 (F) G-Cem: 8.6 ± 2.2 | Tensile strength Initial: Panavia 21 > G-Cem + Gluma DA > RelyX Unicem + Gluma DA > RelyX Unicem > G-Cem > Panavia 21 + Gluma DA After Ageing G-Cem + Gluma DA > RelyX Unicem + Gluma DA > RelyX Unicem > G-Cem > Panavia 21 > Panavia 21 + Gluma DA | TS: Panavia 21 > RelyX Unicem > G-Cem | RelyX Unicem & G-Cem (self-adhesive Resins) when used with Gluma DA displayed better long-term stability. |
| Patel et al., 2013, India [20] | In vitro | n = 55 (11 per group) | Human molars | Finish line: Chamfer Axial height: 4 mm Taper: 20° Spacer: 3 layer Ageing: 2500 cycles | base metal porcelain metal alloy (Wirobond 280, BEGO, Fabrication technique: lost wax casting | No DA applied | Application of DA before final cementation | One-Step—Resinomer, (Bisco) | phosphoric acid with Benzalkonium Chloride | (A) ZPC: (Harvard; Harvard Dental International GmbH, Hoppegarten, Germany) (B) GIC: (Vivaglass; Ivoclar vivadent Inc.,Buffalo, NY, USA) (C) Modified RC (Resinomer, Bisco Inc., Schaum-burg, IL, USA) | Removal stress, UTM | Removal stress (MPa) (A) ZPC: 3.5682 ± 0.2135 (B) ZPC + DA: 1.9209 ± 0.152 (C) GIC: 2.4082 ± 0.2581 (D) GIC + DA: 4.2609 ± 0.1963 (E) Modified RC: 6.9591 ± 0.5883 | Removal stress: Modified RC > GIC + DA > GIC > ZPC > ZPC + DA | Removal stress: RC > GIC > ZPC | DA reduces retention with ZPC and increases retention with GIC. |
| Chandrasekaran et al., 2014, India [43] | In vitro | n = 81 (9 per group) | Human maxillary first premolars | Finish line: Chamfer Axial height: 4 mm Taper: 6–10° Spacer: NM Ageing: No | Full metal Ni-Cr crown Fabrication technique: lost wax casting | No DA | (A) & (B) Application of DA before final cementation | (A) Seal and protect (dentsply) (B) Tooth Mousse (GC) | (A) D-TMR & PENTA (B) CPP-ACP | (i) ZPC (Harvard cement, Harvard Dental International GmbH, Hoppegarten, Germany) (ii) GIC (GC Fuji 1, Tokyo, Japan) (iii) RMGIC (GC Fuji Plus, GC Corporation, Tokyo, Japan) | Bond strength; UTM | Mean Bond strength (MPa) (A) ZPC + SP DA: 249.25 ± 65.65 (B) ZPC + TM DA: 219 ± 49.30 (C) ZPC:295.12 ± 31.16 (D) GIC + SP DA: 345.49 ± 109.86 (E) GIC + TM DA: 421.46 ± 96.52 (F) GIC: 416.21 ± 113.10 (G) RMGIC + SP DA: 379.26 ± 114.59 (H) RMGIC + TM DA: 528.5 ± 67.65 (I) RMGIC: 537.2 ± 73.83 | Mean Bond strength: RMGIC > RMGIC + TM DA > GIC + TM DA > GIC > RMGIC + SP DA > GIC + SP DA > ZPC > ZPC + SP DA > ZPC + TM DA | Mean Bond strength: RMGIC > GIC > ZPC | Retentive strength: RMGIC: Control > TM > SP GIC: TM > Control > SP ZPC: Control > SP > TM TM & SP Can be used before crown cementation using GIC or RMGIC, but not with ZPC. |
| Kumar et al., 2015, India [44] | In vitro | n = 48 (12 per group) | Human maxillary first premolars | NM | Full metal Ni-Cr crown Fabrication technique: lost wax casting | No DA | laser treatment Er, Cr: YSGG laser at 0.5 W potency for 15 s | Desensitising Laser: Er, Cr: YSGG laser (NM) | NA | (i) GIC (ii) self-adhesive RC | TBS; UTM | TBS (N): GIC: 170 ± 7.519 GIC + DA:119.08 ± 5.350 RC: 244.33 ± 11.865 RC + DA: 269.16 ± 5.184 | TBS: RC + DA > RC > GIC > GIC_DA | TBS: RC > GIC | The luting agent of choice for laser DA treated dentine: self-adhesive RC. |
| Chandavarkar et al., 2015 India [8] | In vitro | n = 50 (10 per group) | human premolars | Finish line: Chamfer Axial height: 4 mm Taper: 20° Spacer: 25 µ Ageing: No | Full metal Ni-Cr crown Fabrication technique: lost wax casting | No DA | (A), (B), (D): Application of DA before final cementation (C) laser treatment Er, Cr: YSGG laser at 0.5 W potency for 45 s | (A) Gluma Desensitizer, (Haereus Kulzer, Hanau, Germany) (B) GC Tooth Mousse, Recaldent Tooth Mousse, GC Corporation, Tokyo, Ja-pan)). (C) Waterlase MD Turbo, Biolase Inc, Foothill Ranch, CA, USA) (D) Colgate Sensitive Pro-Relief in-office polishing paste, New York, NY, USA) | (A) GLU-based (B) CPP-ACP-based (C) Er, Cr: YSGG laser (D) Pro-Argin | GIC | Tensile stress; UTM | Tensile stress (MPa); (A) GLU DA + GIC: 3.87 (B) CPP-ACP DA + GIC: 4.01 (C) Laser DA + GIC:3.37 (D) Pro-Argin DA + GIC: 4.10 (E) GIC: 3.65 | Tensile stress: Pro-Argin DA + GIC > CPP-ACP DA + GIC > GLU DA + GIC > GIC > Laser DA + GIC | - | Pro-Argin and CPP-ACP-based DA can be used safely without compromising the retention of cast crowns cemented with GIC. Laser as DA reduces the tensile stress when used with GIC. |
| Janapala et al., 2015, India [45] | In vitro | n = 40 (10 per group) | Human maxillary first premolars | Finish line: NM Axial height: 4 mm Taper: 20° Spacer: NM Ageing: No | Full metal nickel chromium alloy copings (Bellabond, BEGO) Fabrication technique: lost wax casting | No DA applied | Application of DA before final cementation | (A) Cavity varnish (Namuvar, Deepti Dental Products, Maharashtra, India) (B), Glutaraldehyde (Gluma-Heraeus Kulzer, Hanau, Germany), (C) Resin (AdheSE bond, Ivoclar Vivadent, Buffalo, NY, USA) | (A) Dissolved solids (B) 5% Glutaraldehyde & HEMA (C) HEMA, dimethacrylate, silicon dioxide | RMGIC (FujiCEM, GC Corporation, Tokyo, Japan) | TS, UTM | Tensile strength (N) (A) RMGIC: 2.627 ± 1.1887 (B) RMGIC + Varnish: 1.968 ± 0.751 (C) RMGIC + GLUMA: 3.304 ± 0.762 (D) RMGIC + AdheSE: 4.042 ± 0.742 | Tensile strength RMGIC + AdheSE > RMGIC + GLUMA > RMGIC > RMGIC + Varnish | - | Recommends use of resin-based and glutaraldehyde-based sealers with RMGIC before crown cementation. |
| Lawaf et al., 2016, Iran [31] | In vitro | n = 20 (10 per group) | Human premolars | Finish line: Deep chamfer Axial height: 4 mm Taper: 6° Spacer: 3 coats Ageing: No | Full base metal alloy copings Fabrication technique: lost wax casting | No DA applied | Application of DA before final cementation | GLUMA (Heraeus-Kulzer, Hanau, Germany ) | 5% Glutaraldehyde & HEMA | Self-adhesive RC (RelyX U200, 3M ESPE, St. Paul, MN, USA) | TBS; UTM | Tensile Bond Strength (N) (A) RC: 164.45 ± 39.3 (B) RC + GLUMA DA: 230.63 ± 63.8 | TBS RC + GLUMA DA > RC | - | Application of GLUMA DA on Hypersensitive prepared teeth before final cementation using self-adhesive RC. |
| Pilo et al., 2016, Israel [10] | In vitro | n = 40 (10 per group) | Human Mandibular molars | Finish line: Chamfer Axial height: 5 mm Taper: 10° Spacer: 50 µ Ageing: 10,000 cycles | Zirconia crowns copings (Lava frame Y-TZP blocks, 3M ESPE, Seefeld, Germany) Fabrication technique: CAD/CAM milling | No DA applied | Application of DA before final cementation | Colgate Sensitive Pro-Relief Desensitizing Paste (Colgate -Palmolive Company, New York, NY, USA) | 8% arginine and calcium carbonate | (i) RMGIC (RelyX Luting 2, 3M ESPE) (ii) Self Adhesive RC (RelyX U-200, 3M ESPE) | Retentive strength, UTM | Retentive strength (MPa) (A) RMGIC + DA: 2.92 ± 0.84 (B) RMGIC: 3.16 ± 0.73 (C) Self Adhesive RC + DA: 2.27 ± 0.64 (D) Self Adhesive RC: 2.29 ± 0.55 | Retentive strength RMGIC > RMGIC + DA > RC > RC + DA | Retentive strength RMGIC > RC | Retentive strengths of zirconia crowns cemented by either RMGIC or RC remain unaltered when 8% A-C-C is used as DA. |
| Mapkar et al., 2018, India [11] | In vitro | n = 33 (11 per group) | Human maxillary first premolars | Finish line: shoulder Axial height: 4 mm Taper: 20° Spacer: 1 layer Ageing: 2500 cycles | Full metal base metal alloy copings Fabrication technique: lost wax casting | No DA applied | Application of DA before final cementation | (A) Gluma (Heraeus Kulzer, hanau, Germany) (B) Ultraseal (Ultradent, South Jordan, UT USA) | (A) 5% Glutaraldehyde & HEMA (B) Non polymerizable, high -molecular-weight resin | ZPC (MEDIcept, Middlesex, UK). | Dislodgement force, UTM | Dislodgement force (N): (A) ZPC:345.01 (B) ZPC + Gluma:556.41 ZPC + Ultraseal: 320.22 | Dislodgement force: ZPC + Gluma > ZPC > ZPC + Ultraseal | - | Significant increase in retention after application of Gluma DA, whereas non-significant decrease after Ultraseal application. |
| Pilo et al., 2018, Israel [39] | In vitro | n = 40 (10 per group) | Human Mandibular molars | Finish line: Chamfer Axial height: 5 mm Taper: 10° Spacer: 50 µ Ageing: 5000 cycles | Full metal Co-Cr alloy Fabrication technique: selective laser melting (SLM) technology | No DA applied | Application of DA before final cementation | Colgate Sensitive Pro-Relief Desensitizing Paste (Colgate-Palmolive Company, New York, NY, USA) | 8% arginine and calcium carbonate | (i) GIC (ii) ZPC | Retentive strength, UTM | Retentive strength (MPa) GIC + DA: 6.39 ± 1.06 GIC: 5.73 ± 1.10 ZPC + DA: 2.39 ± 0.99 ZPC: 3.10 ± 1.44 | Retentive strength: GIC + DA > GIC > ZPC > ZPC + DA | Retentive strength: GIC > ZPC | Application of 8% arginine and calcium carbonate can be used safely without reducing the retentive strength of crowns cemented with GIC and/or ZPC. |
| Asadullah et al., 2018, India [46] | In vitro | n = 33 (11 per group) | Human maxillary first premolars | Finish line: shoulder Axial height: 4 mm Taper: 20° Spacer: 1coat Ageing: 2500 cycles | Full base metal alloy copings Fabrication technique: lost wax casting | No DA applied | Application of DA before final cementation | (A) ULTRASEAL (Ultradent, South Jordan, UT, USA) (B) GLUMA (Heraeus-Kulzer, Hanau, Germany) | (A) non polymerizable, high -molecular-weight resin (B) 5% Glutaraldehyde & HEMA | RC (RelyX, 3M ESPE) | Dislodgement force, UTM | Dislodgement force (N) (A) RC: 228.892 ## (B) RC + Ultra seal DA: 173.353 ## (C) RC + GLUMA DA: 339.098 ## | Dislodgement force: RC + GLUMA > RC > RC + Ultra seal | - | GLUMA DA can be safely used with RC whereas, Ultraseal DA should not be used with RC. |
| Himashilpa et al., 2019, India [35] | In vitro | n = 420 (10 per group) | Human maxillary premolars | Finish line: Shoulder Axial height: 4 mm Taper: 12° Spacer: NM Ageing: No | Full metal nickel chromium alloy copings Fabrication technique: lost wax casting | No DA applied | Application of DA before final cementation | (A) Systemp (ivoclar vivadent, Liechtenstein) (B) Gluma (Heraeus Kulzer, Hanau, Germany) (C) GC tooth Mousse (GC International, Itabashiku, Tokyo, Japan) (D) Colgate Sensitive Pro-Relief Desensitizing Paste (Colgate-Palmolive Company, New York, NY, USA) (E) Sensodyne repair and protect (F) Sensodyne rapid action repair and protect | (A) Poly(ethylene glycol)dimethacrylate and glutaraldehyde (B) 5% Glutaraldehyde & HEMA (C) CPP-ACP (D) 8% arginine and calcium carbonate (E) Novamin (F) Fluoride | (A) GIC (Fuji luting GC, GC Corporation, Tokyo, Japan) (B) RMGIC: (RelyX Luting Cement 3M ESPE) (C) self-adhesive RC (Maxcem Elite, Kerr, Orange County, CA, USA) | TBS, UTM | TBS (N) Thermocycling (A) GIC: 6.79 ± 0.74 (B) GIC + Systemp: 7.75 ± 0.67 (C) GIC + Gluma: 6.89 ± 0.66 (D) GIC + Mousse: 6.88 ± 0.65 (E) GIC + Arginine: 6.40 ± 0.86 (F) GIC + Novamin: 6.39 ± 0.36 (G) GIC + Flouride: 6.59 ± 1.32 (H) RMGIC: 8.26 ± 0.64 (I) RMGIC + Systemp: 8.44 ± 0.51 (J) RMGIC + Gluma: 8.13 ± 0.49 (K) RMGIC + Mousse: 7.80 ± 0.59 (L) RMGIC + Arginine: 8.15 ± 0.96 (M) RMGIC + Novamin: 8.05 ± 0.42 (N) RMGIC + Flouride: 7.37 ± 1.10 (O) RC: 9.85 ± 0.85 (P) RC + Systemp: 10.80 ± 0.91 (Q) RC + Gluma: 10.06 ± 0.77 (R) RC + Mousse: 9.97 ± 0.82 (S) RC + Arginine: 9.63 ± 0.80 (T) RC + Novamin: 9.49 ± 0.87 (U) RC + Flouride: 9.17 ± 0.64 Non-Thermocycling (A) GIC: 5.41 ± 1.02 (B) GIC + Systemp: 6.15 ± 0.49 (C) GIC + Gluma: 5.61 ± 0.89 (D) GIC + Mousse: 6.85 ± 0.71 (E) GIC + Arginine: 6.29 ± 0.43 (F) GIC + Novamin: 5.86 ± 0.49 (G) GIC + Flouride: 6.15 ± 1.10 (H) RMGIC: 6.58 ± 1.32 (I) RMGIC + Systemp: 7.54 ± 0.77 (J) RMGIC + Gluma: 7.47 ± 0.98 (K) RMGIC + Mousse: 7.35 ± 1.10 (L) RMGIC + Arginine: 6.54 ± 0.89 (M) RMGIC + Novamin:7.54 ± 0.34 (N) RMGIC + Flouride: 6.97 ± 0.61 (O) RC: 9.17 ± 0.52 (P) RC + Systemp: 9.25 ± 0.78 (Q) RC + Gluma: 9.12 ± 0.59 (R) RC + Mousse: 8.80 ± 0.78 (S) RC + Arginine: 8.64 ± 0.60 (T) RC + Novamin:8.75 ± 0.58 (U) RC + Flouride: 8.74 ± 0.64 | TBS: Thermocycling Resin Cement: RC + Systemp > RC + Gluma > RC + Mousse > RC > RC + Arginine > RC + Novamin > RC + Flouride RMGIC: RMGIC + Systemp > RMGIC > RMGIC + Arginine > RMGIC + Gluma > RMGIC + Novamin > RMGIC + Mousse > RMGIC + Flouride GIC: GIC + Systemp > GIC + Gluma > GIC + Mousse > GIC > GIC + Flouride > GIC + Arginine > GIC + Novamin | TBS: RC > RMGIC > GIC | Highest TBS displayed by use of systemp DA, and lowest by Pro-Arginine in all groups. Thermocycling increased TBS |
| Supraja et al., 2020, India [47] | In vitro | n = 45 (5 per group) | Human Maxillary premolars | Finish line: Chamfer Axial height: 4 mm Taper: 6° Spacer: NM Ageing: No | Full metal Co-Cr alloy Fabrication technique: additive manufacturing (direct metal laser sintering). | No DA applied | Application of DA before final cementation | (A) A-CC-F DA (custom made) (B) CPP-ACP-F DA (custom made) | (A) Arginine, Calcium Carbonate, Fluoride (B) Casein Phosphopeptide, Amorphous Calcium Phosphate, Fluoride | (i) GIC (NM) (ii) RMGIC (NM) (iii) RC (NM) | TBS; UTM | TBS (N): GIC + A-CC-F DA: 90.26 ± 10.68 GIC + CPP-ACP-F DA: 272.32 ± 30.5 GIC: 308.62 ± 58.84 RMGIC + A-CC-F DA: 85.07 ± 18.82 RMGIC + CPP-ACP-F DA: 203.47 ± 60.57 RMGIC: 176.89 ± 35.46 RC + A-CC-F DA: 236.05 ± 43.62 RC + CPP-ACP-F DA: 158.66 ± 25.32 RC+: 300.35 ± 27.9 | TBS: GIC: GIC > GIC + A-CC-F DA > GIC + CPP-ACP-F DA RMGIC: RMGIC + CPP-ACP-F DA > RMGIC > RMGIC + A-CC-F DA RC: RC > RC + A-CC-F DA > RC + CPP-ACP-F DA | TBS: RC > RMGIC > GIC | Application of both types of DA decreased TBS for GIC to dentin Application of CPP-ACP-F DA increased, while A-CC-F DA decreased the TBS for RMGIC to dentin Application of both types of DA decreased TBS for RC to dentin |
| Hanjik et al., 2021, Syria [48] | In vitro | n = 40 (10 per group) | Human Maxillary premolars | Finish line: Chamfer Axial height: 4 mm Taper: 6° Spacer: 2 layer, 1 mm above the finish line. Ageing: No | Full metal Ni-Cr crown Fabrication technique: lost wax casting | No DA applied | Application of DA before final cementation | Systemp desensitizer (ivoclar vivadent, Schaan, Liechtenstein) | Poly(ethylene glycol)dimethacrylate and glutaraldehyde in an aqueous solution | (i) GIC (Cavex, CJ Haarlem, The Netherlands) (ii) RMGIC (GC Fuji plus, Tokyo Japan) | TBS; UTM | TBS (N): RMGIC + DA: 829.95 ±104.29 RMGIC + No DA:604.03 ± 127.20 GIC + DA: 415.74 ± 139.92 GIC + No DA: 433.74 ± 177.73 | TBS: DA + RMGIC > RMGIC > GIC > DA + GIC | TBS: RMGIC > GIC | Application of DA increase TBS for RMGIC to dentin Application of DA decrease TBS for GIC to dentin |
| Dewan et al., 2022; Saudi Arabia [49] | In vitro | n = 40 (10 per group) | Human molars | Finish line: Chamfer Axial height: 4 mm Taper: 10° Spacer: NM Ageing: 3000 cycles | Zirconia copings (Ceramill ZI, Austria) Fabrication technique: CAD/CAM milling | No DA applied | Application of DA before final cementation | (A) Gluma (Heraeus Kulzer, Hanau, Germany) (B) Telio CS (Ivoclar Vivadent, Schaan, Liechtenstein) (C) Shield Force Plus (Tokuyama Dental, Encinitas, CA, USA) | (A) 5% Glutaraldehyde & HEMA (B) PEGDMA, Glutaraldehyde (C) HPDMA & PA | RC (Rely X U200, 3M ESPE, St. Paul, MN, USA ) | TS, UTM | TS (MPa) (A) RC: 0.22 ± 0.03 (B) RC + Gluma: 0.53 ± 0.08 (C) RC + Telio CS: 0.35 ± 0.10 (D) RC + Shield force: 0.36 ± 0.14 | TS: RC + Gluma > RC + Shield force > Rc + Telio CS > RC | - | Advocates using the tested DAs before cementing Zirconia crowns. |
| Item → | 1 | 2a | 2b | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Studies | |||||||||||||||
| Mausner et al., 1996 [41] | Y | Y | Y | Y | Y | N | Y | N | N | N | Y | Y | N | N | N |
| Swift et al., 1997 [36] | Y | Y | Y | Y | Y | N | Y | N | N | N | Y | Y | N | N | N |
| Johnson et al., 1998 [34] | Y | Y | Y | Y | Y | N | N | N | N | N | Y | Y | N | N | N |
| Yim et al., 2000 [37] | Y | Y | Y | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | N |
| Wolfart et al., 2003 [12] | Y | Y | Y | Y | Y | N | Y | N | N | N | Y | Y | Y | N | N |
| Johnson et al., 2004 [42] | Y | Y | Y | Y | Y | N | N | N | N | N | Y | Y | N | N | N |
| Sipahi et al., 2007 [38] | Y | Y | Y | Y | Y | N | N | N | N | N | Y | Y | N | N | N |
| Jalandar et al., 2012 [18] | Y | Y | Y | Y | Y | N | N | N | N | N | Y | Y | Y | N | N |
| Stawarczyk et al., 2012 [19] | Y | Y | Y | Y | Y | N | Y | N | N | N | Y | Y | Y | N | N |
| Patel et al., 2013 [20] | Y | Y | Y | Y | Y | N | N | N | N | N | Y | Y | Y | N | N |
| Chandrasekaran et al., 2014 [43] | Y | Y | Y | Y | Y | N | Y | Y | N | N | Y | Y | Y | N | N |
| Kumar et al., 2015 [44] | Y | Y | Y | Y | Y | N | N | N | N | N | Y | Y | N | N | N |
| Chandavarkar et al., 2015 [8] | Y | Y | Y | Y | Y | N | N | N | N | N | Y | Y | Y | Y | N |
| Janapala et al., 2015 [45] | Y | Y | Y | Y | Y | Y | N | N | N | N | Y | Y | Y | Y | N |
| Lawaf et al., 2016 [31] | Y | Y | Y | Y | Y | N | N | N | N | N | Y | Y | Y | N | N |
| Pilo et al., 2016 [10] | Y | Y | Y | Y | Y | N | N | N | N | N | Y | Y | N | N | N |
| Mapkar et al., 2018 [11] | Y | Y | Y | Y | Y | N | N | N | N | N | Y | Y | Y | Y | N |
| Pilo et al., 2018 [39] | Y | Y | Y | Y | Y | N | N | N | N | N | Y | Y | Y | Y | N |
| Asadullah et al., 2018 [46] | Y | Y | Y | Y | Y | N | N | N | N | N | Y | Y | N | Y | N |
| Himashilpa et al., 2019 [35] | Y | Y | Y | Y | Y | N | N | N | N | N | Y | Y | N | N | N |
| Supraja et al., 2020 [47] | Y | Y | Y | Y | Y | Y | N | N | N | N | Y | Y | Y | Y | N |
| Hanjik et al., 2021 [48] | Y | Y | Y | Y | Y | N | N | N | N | N | Y | Y | N | N | N |
| Dewan et al., 2022 [49] | Y | Y | Y | Y | Y | N | N | N | N | N | Y | Y | Y | Y | Y |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sayed, M.E. The Effect of Dentine Desensitizing Agents on the Retention of Cemented Fixed Dental Prostheses: A Systematic Review. Medicina 2023, 59, 515. https://doi.org/10.3390/medicina59030515
Sayed ME. The Effect of Dentine Desensitizing Agents on the Retention of Cemented Fixed Dental Prostheses: A Systematic Review. Medicina. 2023; 59(3):515. https://doi.org/10.3390/medicina59030515
Chicago/Turabian StyleSayed, Mohammed E. 2023. "The Effect of Dentine Desensitizing Agents on the Retention of Cemented Fixed Dental Prostheses: A Systematic Review" Medicina 59, no. 3: 515. https://doi.org/10.3390/medicina59030515