
Accuracy Validation of the Elecsys HBsAg II Quant Assay and Its Utility in Resolving Equivocal Qualitative HBsAg Results
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
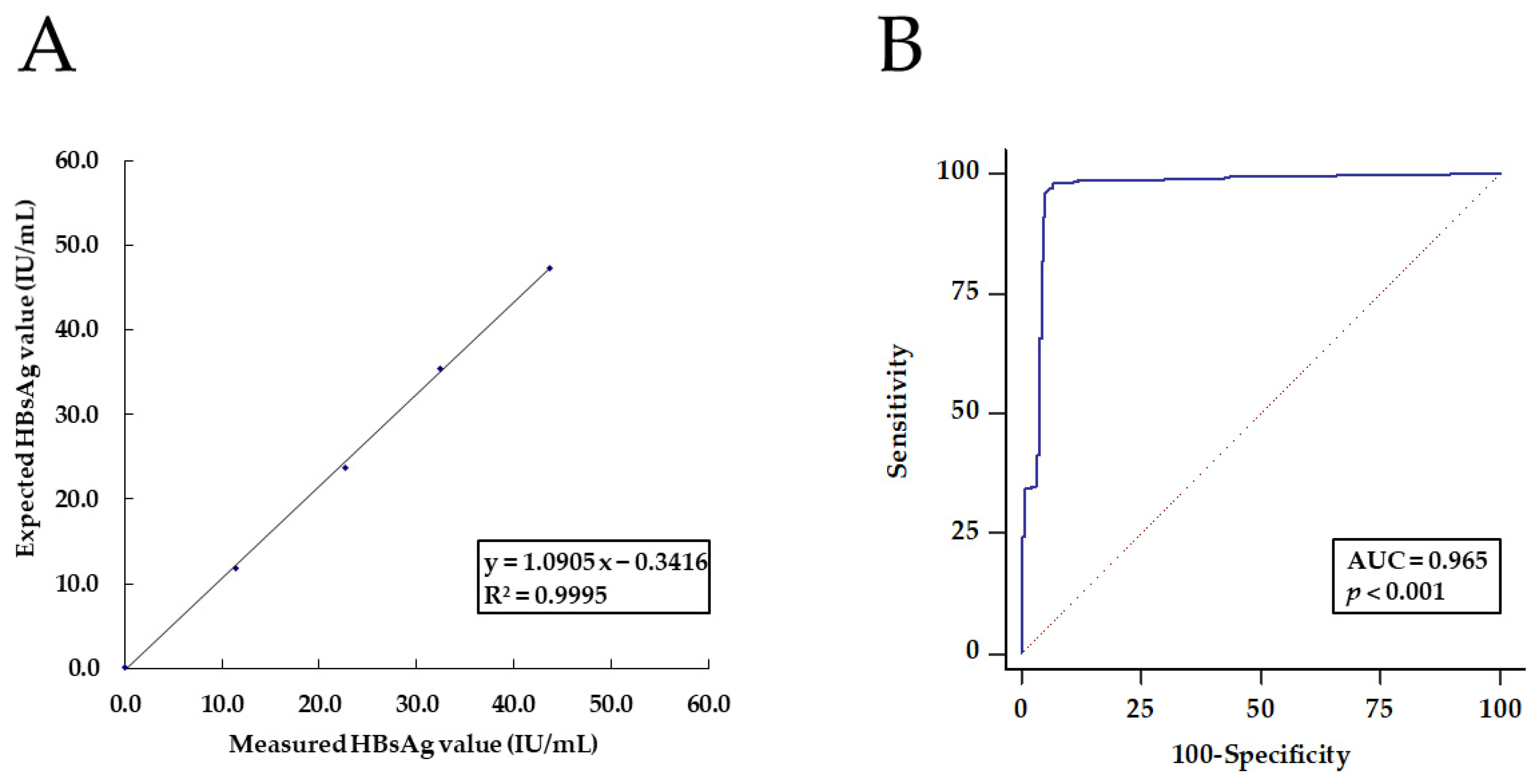
2.1. Validation of the Analytical Accuracy
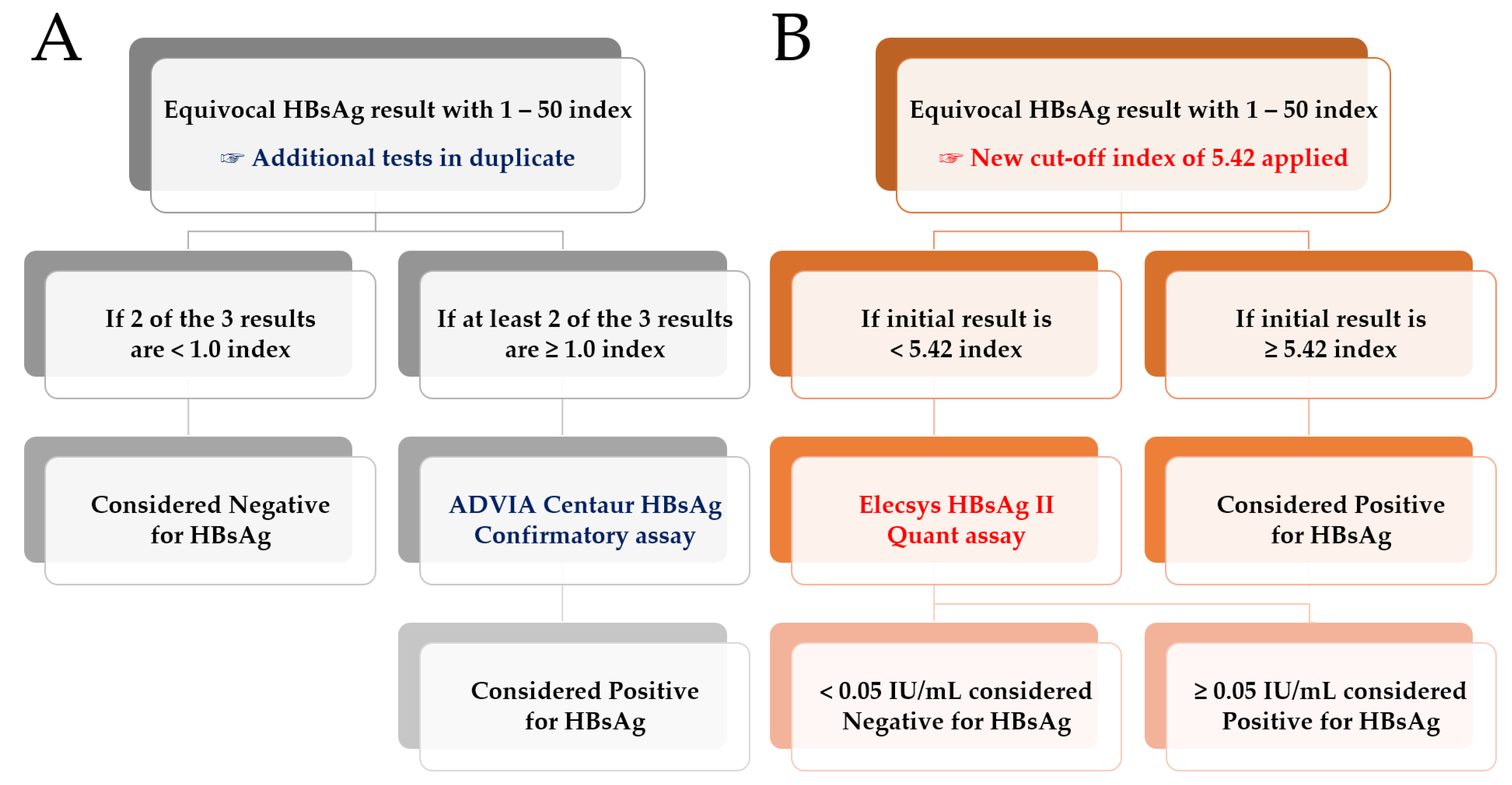
2.2. Comparative Evaluation of Elecsys HBsAg II Quant and ADVIA Centaur HBsAg II Assays
2.3. Statistical Analysis
3. Results
3.1. Analytical Accuracy of the Elecsys HBsAg II Quant Assay
3.2. Comparative Evaluation for Resolving the Equivocal Qualitative HBsAg Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, J.M.; Ahn, S.H. Quantification of HBsAg: Basic virology for clinical practice. World J. Gastroenterol. 2011, 17, 283–289. [Google Scholar] [CrossRef]
- Martinot-Peignoux, M.; Lapalus, M.; Asselah, T.; Marcellin, P. The role of HBsAg quantification for monitoring natural history and treatment outcome. Liver Int. 2013, 33 (Suppl. S1), 125–132. [Google Scholar] [CrossRef]
- Wang, C.-C.; Tseng, T.-C.; Wang, P.-C.; Lin, H.H.; Kao, J.-H. Baseline hepatitis B surface antigen quantitation can predict virologic response in entecavir-treated chronic hepatitis B patients. J. Formos. Med. Assoc. 2014, 113, 786–793. [Google Scholar] [CrossRef] [Green Version]
- Sonneveld, M.J.; Hansen, B.E.; Piratvisuth, T.; Jia, J.-D.; Zeuzem, S.; Gane, E.; Liaw, Y.-F.; Xie, Q.; Heathcote, E.J.; Chan, H.L.; et al. Response-guided peginterferon therapy in hepatitis B e antigen-positive chronic hepatitis B using serum hepatitis B surface antigen levels. Hepatology 2013, 58, 872–880. [Google Scholar] [CrossRef]
- Tseng, T.-C.; Kao, J.-H. Clinical utility of quantitative HBsAg in natural history and nucleos(t)ide analogue treatment of chronic hepatitis B: New trick of old dog. J. Gastroenterol. 2013, 48, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Tuaillon, E.; Mondain, A.-M.; Nagot, N.; Ottomani, L.; Kania, D.; Nogué, E.; Rubbo, P.-A.; Pageaux, G.-P.; Van De Perre, P.; Ducos, J. Comparison of Serum HBsAg Quantitation by Four Immunoassays, and Relationships of HBsAg Level with HBV Replication and HBV Genotypes. PLoS ONE 2012, 7, e32143. [Google Scholar] [CrossRef] [Green Version]
- Deguchi, M.; Kagita, M.; Yoshioka, N.; Tsukamoto, H.; Takao, M.; Tahara, K.; Maeda, I.; Hidaka, Y.; Yamauchi, S.; Kaneko, A.; et al. Evaluation of the highly sensitive chemiluminescent enzyme immunoassay “Lumipulse HBsAg-HQ” for hepatitis B virus screening. J. Clin. Lab. Anal. 2018, 32, e22334. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Bae, T.; Cho, Y.; Kim, D.; Lee, J. Analytical Performance of the Sysmex HISCL HBsAg Assay and Comparison with the Roche Elecsys HBsAg II Quant Assay in the Quantification of Hepatitis B Surface Antigen. Medicina 2021, 57, 1307. [Google Scholar] [CrossRef]
- Maylin, S.; Boyd, A.; Delaugerre, C.; Zoulim, F.; Lavocat, F.; Simon, F.; Girard, P.-M.; Lacombe, K. Comparison between Elecsys HBsAg II and Architect HBsAg QT Assays for Quantification of Hepatitis B Surface Antigen among Patients Coinfected with HIV and Hepatitis B Virus. Clin. Vaccine Immunol. 2012, 19, 242–248. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.; Hu, Y.; Yang, Y.; Hu, T.; Wang, X. Comparison of two immunoassays for quantification of hepatitis B surface antigen in Chinese patients with concomitant hepatitis B surface antigen and hepatitis B surface antibodies. Arch. Virol. 2015, 160, 191–198. [Google Scholar] [CrossRef]
- Xu, L.; Wang, X.; Ma, R.; Zeng, X.; Wu, B.; Hu, L.; Li, Y. False decrease of HBsAg S/CO values in serum with high-concentration rheumatoid factors. Clin. Biochem. 2013, 46, 799–804. [Google Scholar] [CrossRef]
- Wiwanitkit, V. Influenza vaccine and false-positive HBsAg results. Transfus. Apher. Sci. 2014, 50, 309. [Google Scholar] [CrossRef]
- Gencay, M.; Vermeulen, M.; Neofytos, D.; Westergaard, G.; Pabinger, S.; Kriegner, A.; Seffner, A.; Gohl, P.; Huebner, K.; Nauck, M.; et al. Substantial variation in the hepatitis B surface antigen (HBsAg) in hepatitis B virus (HBV)-positive patients from South Africa: Reliable detection of HBV by the Elecsys HBsAg II assay. J. Clin. Virol. 2018, 101, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.-Y.; Groboske, S.E.; Baldwin, A.D.; Yeo, K.J.; Van Wijk, X.M.R. False-Positive Hepatitis B Surface Antibody Results: An Example of Reagent Carryover. J. Appl. Lab. Med. 2020, 5, 429–431. [Google Scholar] [CrossRef]
- Sarin, S.K.; Kumar, M.; Lau, G.K.; Abbas, Z.; Chan, H.L.; Chen, C.J.; Chen, D.S.; Chen, H.L.; Chen, P.J.; Chien, R.N.; et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol. Int. 2016, 10, 1–98. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.L.; Thompson, A.; Martinot-Peignoux, M.; Piratvisuth, T.; Cornberg, M.; Brunetto, M.R.; Tillmann, H.L.; Kao, J.-H.; Jia, J.-D.; Wedemeyer, H.; et al. Hepatitis B surface antigen quantification: Why and how to use it in 2011—A core group report. J. Hepatol. 2011, 55, 1121–1131. [Google Scholar] [CrossRef]
- Sonneveld, M.J.; Rijckborst, V.; Boucher, C.A.; Zwang, L.; Beersma, M.F.; Hansen, B.E.; Janssen, H.L. A comparison of two assays for quantification of Hepatitis B surface Antigen in patients with chronic hepatitis B. J. Clin. Virol. 2011, 51, 175–178. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.-J.; Kim, S.Y.; Lee, S.M.; Heo, J.; Kim, H.H.; Chang, C.L.; Lee, E.Y.; Son, H.C. Elecsys Hepatitis B Surface Antigen Quantitative Assay: Performance Evaluation and Correlation with Hepatitis B Virus DNA during 96 Weeks of Follow-up in Chronic Hepatitis B Patients. Ann. Lab. Med. 2012, 32, 420–425. [Google Scholar] [CrossRef] [Green Version]
- Thompson, A.J.; Nguyen, T.; Iser, D.; Ayres, A.; Jackson, K.; Littlejohn, M.; Slavin, J.; Bowden, S.; Gane, E.J.; Abbott, W.; et al. Serum hepatitis B surface antigen and hepatitis B e antigen titers: Disease phase influences correlation with viral load and intrahepatic hepatitis B virus markers. Hepatology 2010, 51, 1933–1944. [Google Scholar] [CrossRef]
- Grimes, D.A.; Schulz, K.F. Uses and abuses of screening tests. Lancet 2002, 359, 881–884. [Google Scholar] [CrossRef]
- Tenny, S.; Hoffman, M.R. Prevalence. In StatPearls; StatPearls Publishing Copyright© 2022; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Yim, S.Y.; Kim, J.H. The epidemiology of hepatitis B virus infection in Korea. Korean J. Intern. Med. 2019, 34, 945–953. [Google Scholar] [CrossRef]
- Kim, B.H.; Park, J.-W. Epidemiology of liver cancer in South Korea. Clin. Mol. Hepatol. 2018, 24, 1–9. [Google Scholar] [CrossRef]
- Parry, J.V.; Easterbrook, P.; Sands, A.R. One or two serological assay testing strategy for diagnosis of HBV and HCV infection? The use of predictive modelling. BMC Infect. Dis. 2017, 17, 705. [Google Scholar] [CrossRef] [Green Version]
- Tseng, T.; Liu, C.; Su, T.; Wang, C.; Chen, C.; Chen, P.; Chen, D.; Kao, J. Serum Hepatitis B Surface Antigen Levels Predict Surface Antigen Loss in Hepatitis B e Antigen Seroconverters. Gastroenterology 2011, 141, 517–525, 525.e511–512. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.M.; Lee, S.G. Clinical features of HBsAg seroclearance in hepatitis B virus carriers in South Korea: A retrospective longitudinal study. World J. Gastroenterol. 2016, 22, 9836–9843. [Google Scholar] [CrossRef]
- Kim, S.-K.; Huh, J.; Jeong, T.-D. Proposal of Efficient Workflows for Confirmatory Neutralization Test for Initial Hepatitis B Surface Antigen Positive Samples. Clin. Lab. 2019, 65, 1971–1974. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Performance Characteristics | Elecsys HBsAg II Quant Assay | ADVIA Centaur HBsAg II Assay |
|---|---|---|
| Manufacturer | Roche Diagnostics | Siemens Healthcare Diagnostics |
| Principle of operation | ECLIA | CLIA |
| Measurement/Unit | Quantitative/IU/mL | Qualitative/index |
| Capture antibody | Biotinylated monoclonal (mouse) | Biotinylated monoclonal (mouse) |
| Conjugate antibody | Ruthenium complex polyclonal (sheep) | Acridinium-ester-labeled monoclonal (mouse) |
| Duration of the assay (min) | 18 | 23 |
| Sample volume (μL) | 50 | 100 |
| Limit of quantitation (IU/mL) | ≥0.05 | 0.040 at the 1.0 index cutoff |
| Precision | CV <3.2% in Cobas e601/e602 | CV <3.6% in ADVIA Centaur XP |
| Analytical measuring range (theoretical) | 0.05–130 IU/mL (pre-dilution applied) * | 0.1–1000 index |
| Traceability of the value assigned to the calibrator | WHO International Reference Standard, 00/588 | WHO International Reference Standard, 00/588 |
| Sample ID | HBsAg Qual 1st | HBsAg Qual 2nd | HBsAg Qual 3rd | Qual Result | Quant Result | Anti-HBs | HBeAg | Anti-HBe | Anti-HBc IgG | Anti-HBc IgM | HBV DNA | Diagnosis |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 271 | 1.19 | 0.11 | 0.24 | Neg | 0.05 | Pos | Neg | Neg | Pos | Neg | ND | CHB |
| 285 | 1.05 | <0.1 | <0.1 | Neg | 116.04 | Pos | Pos | Neg | Pos | Neg | na | CHB |
| 299 | 1.02 | 0.80 | 0.87 | Neg | 0.80 | Pos | Neg | Pos | Pos | Neg | ND | CHB |
| 28 | 1.08 | 0.78 | 1.02 | Pos | <0.05 | Neg | Neg | Neg | Neg | Neg | ND | AHC |
| 257 | 1.50 | 1.02 | 1.01 | Pos | <0.05 | Pos | Neg | Pos | Pos | Neg | ND | NVH |
| 309 | 3.34 | 3.59 | 3.24 | Pos | <0.05 | Neg | Neg | Neg | Neg | Neg | ND | NVH |
| 362 | 3.52 | 3.63 | 3.38 | Pos | <0.05 | Neg | Neg | Neg | Neg | Neg | ND | NVH |
| Statistics | Elecsys HBsAg II Quant Assay | ADVIA Centaur HBsAg II Assay |
|---|---|---|
| Kappa agreement | Almost perfect (Kappa, 0.9669; 95% CI, 0.9426 to 0.9912) | |
| Concordance rate (%) | 100 | 98.44 |
| True positive (n) | 170 | 167 |
| True negative (n) | 279 | 275 |
| False positive (n) | 0 | 4 |
| False negative (n) | 0 | 3 |
| Sensitivity (%) | 100 (95% CI, 97.87 to 100) | 98.24 (95% CI, 94.93 to 99.63) |
| Specificity (%) | 100 (95% CI, 98.68 to 100) | 98.57 (95% CI, 96.37 to 99.61) |
| Positive likelihood ratio | Not available | 68.52 (95% CI, 25.89 to 181.32) |
| Negative likelihood ratio | 0 (95% CI, not available) | 0.02 (95% CI, 0.01 to 0.05) |
| Positive predictive value * (%) | 100 (95% CI, not available) | 79.18 (95% CI, 58.98 to 90.96) |
| Negative predictive value * (%) | 100 (95% CI, not available) | 99.90 (95% CI, 99.70 to 99.97) |
| Accuracy * (%) | 100 (95% CI, 99.18 to 100) | 98.55 (95% CI, 96.96 to 99.44) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Lee, S.Y.; Cho, Y.G.; Kim, D.S.; Park, J. Accuracy Validation of the Elecsys HBsAg II Quant Assay and Its Utility in Resolving Equivocal Qualitative HBsAg Results. Medicina 2023, 59, 443. https://doi.org/10.3390/medicina59030443
Lee J, Lee SY, Cho YG, Kim DS, Park J. Accuracy Validation of the Elecsys HBsAg II Quant Assay and Its Utility in Resolving Equivocal Qualitative HBsAg Results. Medicina. 2023; 59(3):443. https://doi.org/10.3390/medicina59030443
Chicago/Turabian StyleLee, Jaehyeon, Seung Yeob Lee, Yong Gon Cho, Dal Sik Kim, and Joonhong Park. 2023. "Accuracy Validation of the Elecsys HBsAg II Quant Assay and Its Utility in Resolving Equivocal Qualitative HBsAg Results" Medicina 59, no. 3: 443. https://doi.org/10.3390/medicina59030443