
The Role of Lifestyle Interventions in the Prevention and Treatment of Gestational Diabetes Mellitus
 , ,
, ,  , ,
, ,  , , and
, , and
Abstract
:1. Introduction
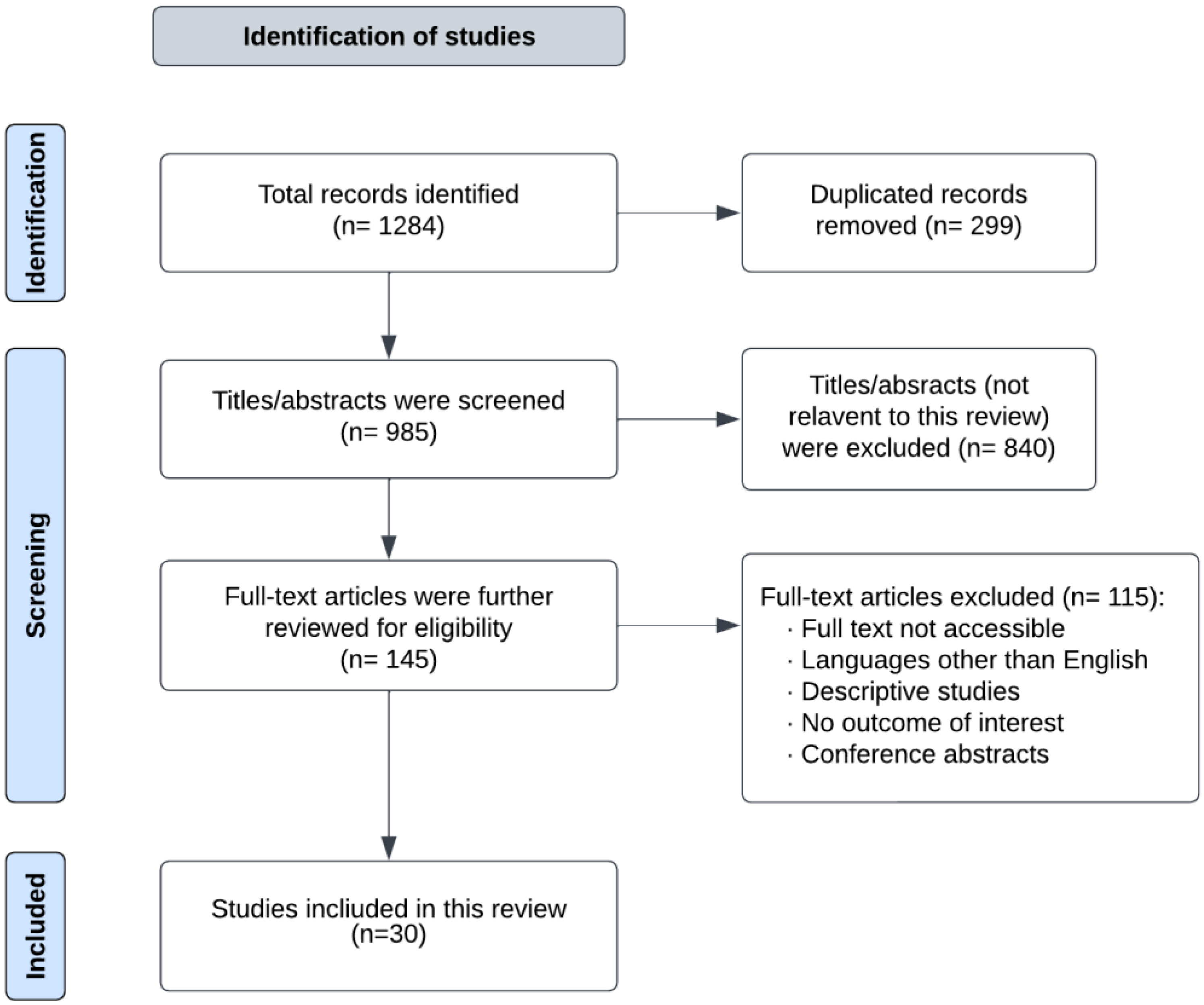
2. Methodology
3. Current Physical Activity Recommendations in GDM Treatment
4. Effect of Physical Activity on Prevention of GDM
5. Current Nutrition Therapy for GDM
6. Effect of Dietary Interventions on the Prevention of GDM
7. Effect of Combined Interventions (Physical Activity and Dietary Interventions) on the Risk of GDM
8. The Effect of Dietary Supplements on the Risk of GDM
8.1. Vitamin D
8.2. Myo-Inositol
9. Effect of Combined Interventions (Physical Activity and Dietary Interventions) on Outcomes in Patients with GDM
9.1. Glycemic Control
9.2. Weight Gain during Pregnancy
9.3. Postnatal Depression
10. Future Directions
11. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McIntyre, H.D.; Catalano, P.; Zhang, C.; Desoye, G.; Mathiesen, E.R.; Damm, P. Gestational diabetes mellitus. Nat. Rev. Dis. Prim. 2019, 5, 47. [Google Scholar] [CrossRef]
- Kim, C.; Newton, K.M.; Knopp, R.H. Gestational diabetes and the incidence of type 2 diabetes: A systematic review. Diabetes Care 2002, 25, 1862–1868. [Google Scholar] [CrossRef]
- Fraser, A.; Nelson, S.M.; Macdonald-Wallis, C.; Cherry, L.; Butler, E.; Sattar, N.; Lawlor, D.A. Associations of Pregnancy Complications With Calculated Cardiovascular Disease Risk and Cardiovascular Risk Factors in Middle Age. Circulation 2012, 125, 1367–1380. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Shen, S.; Sun, L.; Yang, H.; Jin, B.; Cao, X. Metabolic Syndrome Risk after Gestational Diabetes: A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e87863. [Google Scholar] [CrossRef] [PubMed]
- Hakkarainen, H.; Huopio, H.; Cederberg, H.; Pääkkönen, M.; Voutilainen, R.; Heinonen, S. The risk of metabolic syndrome in women with previous GDM in a long-term follow-up. Gynecol. Endocrinol. 2016, 32, 920–925. [Google Scholar] [CrossRef]
- Hakkarainen, H.; Huopio, H.; Cederberg, H.; Voutilainen, R.; Heinonen, S. Future risk of metabolic syndrome in women with a previous LGA delivery stratified by gestational glucose tolerance: A prospective cohort study. BMC Pregnancy Childbirth 2018, 18, 326. [Google Scholar] [CrossRef]
- Chandler-Laney, P.C.; Bush, N.C.; Granger, W.M.; Rouse, D.J.; Mancuso, M.S.; Gower, B.A. Overweight status and intrauterine exposure to gestational diabetes are associated with children’s metabolic health. Pediatr. Obes. 2012, 7, 44–52. [Google Scholar] [CrossRef]
- Onaade, O.; Maples, J.M.; Rand, B.; Fortner, K.B.; Zite, N.B.; Ehrlich, S.F. Physical activity for blood glucose control in gestational diabetes mellitus: Rationale and recommendations for translational behavioral interventions. Clin. Diabetes Endocrinol. 2021, 7, 7. [Google Scholar] [CrossRef]
- Farahvar, S.; Walfisch, A.; Sheiner, E. Gestational diabetes risk factors and long-term consequences for both mother and offspring: A literature review. Expert Rev. Endocrinol. Metab. 2019, 14, 63–74. [Google Scholar] [CrossRef]
- Sparks, J.R.; Ghildayal, N.; Hivert, M.-F.; Redman, L.M. Lifestyle interventions in pregnancy targeting GDM prevention: Looking ahead to precision medicine. Diabetologia 2022, 65, 1814–1824. [Google Scholar] [CrossRef]
- Fu, J.; Retnakaran, R. The life course perspective of gestational diabetes: An opportunity for the prevention of diabetes and heart disease in women. EClinicalMedicine 2022, 45, 101294. [Google Scholar] [CrossRef]
- Lin, J.; Liu, H.; Wu, D.-D.; Hu, H.-T.; Wang, H.-H.; Zhou, C.-L.; Liu, X.-M.; Chen, X.-J.; Sheng, J.-Z.; Huang, H.-F. Long interpregnancy interval and adverse perinatal outcomes: A retrospective cohort study. Sci. China Life Sci. 2020, 63, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Yong, H.Y.; Mohd Shariff, Z.; Mohd Yusof, B.N.; Rejali, Z.; Tee, Y.Y.S.; Bindels, J.; Van Der Beek, E.M. Independent and combined effects of age, body mass index and gestational weight gain on the risk of gestational diabetes mellitus. Sci. Rep. 2020, 10, 8486. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, L.; Gross, J.; Lanzi, S.; Quansah, D.Y.; Puder, J.; Horsch, A. How diet, physical activity and psychosocial well-being interact in women with gestational diabetes mellitus: An integrative review. BMC Pregnancy Childbirth 2019, 19, 60. [Google Scholar] [CrossRef] [PubMed]
- Mamun, A.A.; Callaway, L.K.; O’Callaghan, M.J.; Williams, G.M.; Najman, J.M.; Alati, R.; Clavarino, A.; Lawlor, D.A. Associations of maternal pre-pregnancy obesity and excess pregnancy weight gains with adverse pregnancy outcomes and length of hospital stay. BMC Pregnancy Childbirth 2011, 11, 62. [Google Scholar] [CrossRef] [PubMed]
- Tzanetakou, I.P. Nutrition During Pregnancy and the Effect of Carbohydrates on the Offspring’s Metabolic Profile: In Search of the “Perfect Maternal Diet”. Open Cardiovasc. Med. J. 2011, 5, 103–109. [Google Scholar] [CrossRef]
- Rose, A.J.; Richter, E.A. Skeletal muscle glucose uptake during exercise: How is it regulated? Physiology 2005, 20, 260–270. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.L.; Shields, N.; Taylor, N.F.; Frawley, H.C. Exercise improves glycaemic control in women diagnosed with gestational diabetes mellitus: A systematic review. J. Physiother. 2016, 62, 188–196. [Google Scholar] [CrossRef]
- Laredo-Aguilera, J.A.; Gallardo-Bravo, M.; Rabanales-Sotos, J.A.; Cobo-Cuenca, A.I.; Carmona-Torres, J.M. Physical Activity Programs during Pregnancy Are Effective for the Control of Gestational Diabetes Mellitus. Int. J. Environ. Res. Public Health 2020, 17, 6151. [Google Scholar] [CrossRef]
- Management of Diabetes in Pregnancy: Standards of Medical Care in Diabetes—2022. Diabetes Care 2022, 45, S232–S243. [CrossRef]
- Savvaki, D.; Taousani, E.; Goulis, D.G.; Tsirou, E.; Voziki, E.; Douda, H.; Nikolettos, N.; Tokmakidis, S.P. Guidelines for exercise during normal pregnancy and gestational diabetes: A review of international recommendations. Hormones 2018, 17, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Sen, A.; Henriksen, T.; Saugstad, O.D.; Tonstad, S. Physical activity and the risk of gestational diabetes mellitus: A systematic review and dose–response meta-analysis of epidemiological studies. Eur. J. Epidemiol. 2016, 31, 967–997. [Google Scholar] [CrossRef]
- da Silva, S.G.; Ricardo, L.I.; Evenson, K.R.; Hallal, P.C. Leisure-time physical activity in pregnancy and maternal-child health: A systematic review and meta-analysis of randomized controlled trials and cohort studies. Sports Med. 2017, 47, 295–317. [Google Scholar] [CrossRef]
- Davenport, M.H.; Ruchat, S.-M.; Poitras, V.J.; Garcia, A.J.; Gray, C.E.; Barrowman, N.; Skow, R.J.; Meah, V.L.; Riske, L.; Sobierajski, F. Prenatal exercise for the prevention of gestational diabetes mellitus and hypertensive disorders of pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1367–1375. [Google Scholar] [CrossRef]
- Mijatovic-Vukas, J.; Capling, L.; Cheng, S.; Stamatakis, E.; Louie, J.; Cheung, N.W.; Markovic, T.; Ross, G.; Senior, A.; Brand-Miller, J.C. Associations of diet and physical activity with risk for gestational diabetes mellitus: A systematic review and meta-analysis. Nutrients 2018, 10, 698. [Google Scholar] [CrossRef] [PubMed]
- Ming, W.-K.; Ding, W.; Zhang, C.J.; Zhong, L.; Long, Y.; Li, Z.; Sun, C.; Wu, Y.; Chen, H.; Chen, H. The effect of exercise during pregnancy on gestational diabetes mellitus in normal-weight women: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2018, 18, 440. [Google Scholar] [CrossRef] [PubMed]
- Nasiri-Amiri, F.; Sepidarkish, M.; Shirvani, M.A.; Habibipour, P.; Tabari, N.S.M. The effect of exercise on the prevention of gestational diabetes in obese and overweight pregnant women: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2019, 11, 72. [Google Scholar] [CrossRef]
- Russo, L.M.; Nobles, C.; Ertel, K.A.; Chasan-Taber, L.; Whitcomb, B.W. Physical activity interventions in pregnancy and risk of gestational diabetes mellitus: A systematic review and meta-analysis. Obstet. Gynecol. 2015, 125, 576–582. [Google Scholar] [CrossRef]
- Yu, Y.; Xie, R.; Shen, C.; Shu, L. Effect of exercise during pregnancy to prevent gestational diabetes mellitus: A systematic review and meta-analysis. J. Matern. Fetal Neonatal Med. 2018, 31, 1632–1637. [Google Scholar] [CrossRef]
- Zheng, J.; Wang, H.; Ren, M. Influence of exercise intervention on gestational diabetes mellitus: A systematic review and meta-analysis. J. Endocrinol. Investig. 2017, 40, 1027–1033. [Google Scholar] [CrossRef]
- Madhuvrata, P.; Govinden, G.; Bustani, R.; Song, S.; Farrell, T. Prevention of gestational diabetes in pregnant women with risk factors for gestational diabetes: A systematic review and meta-analysis of randomised trials. Obstet. Med. 2015, 8, 68–85. [Google Scholar] [CrossRef] [PubMed]
- DiPietro, L.; Evenson, K.R.; Bloodgood, B.; Sprow, K.; Troiano, R.P.; Piercy, K.L.; Vaux-Bjerke, A.; Powell, K.E. Benefits of physical activity during pregnancy and postpartum: An umbrella review. Med. Sci. Sports Exerc. 2019, 51, 1292. [Google Scholar] [CrossRef] [PubMed]
- Mitanchez, D.; Ciangura, C.; Jacqueminet, S. How can maternal lifestyle interventions modify the effects of gestational diabetes in the neonate and the offspring? A systematic review of meta-analyses. Nutrients 2020, 12, 353. [Google Scholar] [CrossRef] [PubMed]
- Doi, S.A.; Furuya-Kanamori, L.; Toft, E.; Musa, O.A.; Mohamed, A.M.; Clark, J.; Thalib, L. Physical activity in pregnancy prevents gestational diabetes: A meta-analysis. Diabetes Res. Clin. Pract. 2020, 168, 108371. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.; Ceysens, G.; Boulvain, M. Exercise for pregnant women with gestational diabetes for improving maternal and fetal outcomes. Cochrane Database Syst. Rev. 2017, 6, CD012202. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.Y.; Shu, J.; Fu, X.H.; Chen, X.P.; Zhang, L.; Ji, M.X.; Liu, X.M.; Yu, T.T.; Sheng, J.Z.; Huang, H.F. Improving the effectiveness of lifestyle interventions for gestational diabetes prevention: A meta-analysis and meta-regression. Bjog 2019, 126, 311–320. [Google Scholar] [CrossRef]
- Han, S.; Middleton, P.; Shepherd, E.; Van Ryswyk, E.; Crowther, C.A. Different types of dietary advice for women with gestational diabetes mellitus. Cochrane Database Syst. Rev. 2017, 2, CD009275. [Google Scholar] [CrossRef]
- Martis, R.; Crowther, C.A.; Shepherd, E.; Alsweiler, J.; Downie, M.R.; Brown, J. Treatments for women with gestational diabetes mellitus: An overview of Cochrane systematic reviews. Cochrane Database Syst. Rev. 2018, 2018, CD012327. [Google Scholar] [CrossRef]
- Farrar, D.; Simmonds, M.; Bryant, M.; Sheldon, T.A.; Tuffnell, D.; Golder, S.; Lawlor, D.A. Treatments for gestational diabetes: A systematic review and meta-analysis. BMJ Open 2017, 7, e015557. [Google Scholar] [CrossRef]
- Duarte-Gardea, M.O.; Gonzales-Pacheco, D.M.; Reader, D.M.; Thomas, A.M.; Wang, S.R.; Gregory, R.P.; Piemonte, T.A.; Thompson, K.L.; Moloney, L. Academy of nutrition and dietetics gestational diabetes evidence-based nutrition practice guideline. J. Acad. Nutr. Diet. 2018, 118, 1719–1742. [Google Scholar] [CrossRef]
- Kintiraki, E.; Goulis, D.G. Gestational diabetes mellitus: Multi-disciplinary treatment approaches. Metabolism 2018, 86, 91–101. [Google Scholar] [CrossRef]
- Knopp, R.H.; Magee, M.S.; Raisys, V.; Benedetti, T.; Bonet, B. Hypocaloric diets and ketogenesis in the management of obese gestational diabetic women. J. Am. Coll. Nutr. 1991, 10, 649–667. [Google Scholar] [CrossRef]
- Pang, G.; Xie, J.; Chen, Q.; Hu, Z. Energy intake, metabolic homeostasis, and human health. Food Sci. Hum. Wellness 2014, 3, 89–103. [Google Scholar] [CrossRef]
- De Ridder, D.; Kroese, F.; Evers, C.; Adriaanse, M.; Gillebaart, M. Healthy diet: Health impact, prevalence, correlates, and interventions. Psychol. Amp. Health 2017, 32, 907–941. [Google Scholar] [CrossRef] [PubMed]
- Saisho, Y. β-cell dysfunction: Its critical role in prevention and management of type 2 diabetes. World J. Diabetes 2015, 6, 109. [Google Scholar] [CrossRef] [PubMed]
- Xiao, R.S.; Simas, T.A.M.; Person, S.D.; Goldberg, R.J.; Waring, M.E. Peer Reviewed: Diet Quality and History of Gestational Diabetes Mellitus Among Childbearing Women, United States, 2007–2010. Prev. Chronic Dis. 2015, 12, E25. [Google Scholar] [CrossRef] [PubMed]
- Rogozińska, E.; Chamillard, M.; Hitman, G.A.; Khan, K.S.; Thangaratinam, S. Nutritional Manipulation for the Primary Prevention of Gestational Diabetes Mellitus: A Meta-Analysis of Randomised Studies. PLoS ONE 2015, 10, e0115526. [Google Scholar] [CrossRef]
- Bennett, C.J.; Walker, R.E.; Blumfield, M.L.; Gwini, S.-M.; Ma, J.; Wang, F.; Wan, Y.; Dickinson, H.; Truby, H. Interventions designed to reduce excessive gestational weight gain can reduce the incidence of gestational diabetes mellitus: A systematic review and meta-analysis of randomised controlled trials. Diabetes Res. Clin. Pract. 2018, 141, 69–79. [Google Scholar] [CrossRef]
- Tobias, D.K.; Zhang, C.; Chavarro, J.; Bowers, K.; Rich-Edwards, J.; Rosner, B.; Mozaffarian, D.; Hu, F.B. Prepregnancy adherence to dietary patterns and lower risk of gestational diabetes mellitus. Am. J. Clin. Nutr. 2012, 96, 289–295. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhang, C. Prevalence of gestational diabetes and risk of progression to type 2 diabetes: A global perspective. Curr. Diabetes Rep. 2016, 16, 7. [Google Scholar] [CrossRef]
- Tryggvadottir, E.A.; Medek, H.; Birgisdottir, B.E.; Geirsson, R.T.; Gunnarsdottir, I. Association between healthy maternal dietary pattern and risk for gestational diabetes mellitus. Eur. J. Clin. Nutr. 2016, 70, 237–242. [Google Scholar] [CrossRef]
- Pham, N.M.; Do, V.V.; Lee, A.H. Polyphenol-rich foods and risk of gestational diabetes: A systematic review and meta-analysis. Eur. J. Clin. Nutr. 2019, 73, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Bao, W.; Song, Y.; Bertrand, K.A.; Tobias, D.K.; Olsen, S.F.; Chavarro, J.E.; Mills, J.L.; Hu, F.B.; Zhang, C. Prepregnancy habitual intake of vitamin D from diet and supplements in relation to risk of gestational diabetes mellitus: A prospective cohort study. J. Diabetes 2018, 10, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Tieu, J.; Shepherd, E.; Middleton, P.; Crowther, C.A. Dietary advice interventions in pregnancy for preventing gestational diabetes mellitus. Cochrane Database Syst. Rev. 2017, 2017, CD006674. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, E.; Gomersall, J.C.; Tieu, J.; Han, S.; Crowther, C.A.; Middleton, P. Combined diet and exercise interventions for preventing gestational diabetes mellitus. Cochrane Database Syst. Rev. 2017, 11, Cd010443. [Google Scholar] [CrossRef]
- Harrison, C.L.; Lombard, C.B.; Strauss, B.J.; Teede, H.J. Optimizing healthy gestational weight gain in women at high risk of gestational diabetes: A randomized controlled trial. Obesity 2013, 21, 904–909. [Google Scholar] [CrossRef]
- Koivusalo, S.B.; Rönö, K.; Klemetti, M.M.; Roine, R.P.; Lindström, J.; Erkkola, M.; Kaaja, R.J.; Pöyhönen-Alho, M.; Tiitinen, A.; Huvinen, E. Gestational diabetes mellitus can be prevented by lifestyle intervention: The Finnish Gestational Diabetes Prevention Study (RADIEL) a randomized controlled trial. Diabetes Care 2016, 39, 24–30. [Google Scholar] [CrossRef]
- Simmons, D.; Devlieger, R.; Van Assche, A.; Jans, G.; Galjaard, S.; Corcoy, R.; Adelantado, J.M.; Dunne, F.; Desoye, G.; Harreiter, J.; et al. Effect of physical activity and/or healthy eating on GDM risk: The DALI Lifestyle Study. J. Clin. Endocrinol. Amp. Metab. 2016, 102, 903–913. [Google Scholar] [CrossRef]
- Dodd, J.M.; Turnbull, D.; McPhee, A.J.; Deussen, A.R.; Grivell, R.M.; Yelland, L.N.; Crowther, C.A.; Wittert, G.; Owens, J.A.; Robinson, J.S. Antenatal lifestyle advice for women who are overweight or obese: LIMIT randomised trial. BMJ 2014, 348, g1285. [Google Scholar] [CrossRef]
- Bain, E.; Crane, M.; Tieu, J.; Han, S.; Crowther, C.A.; Middleton, P. Diet and exercise interventions for preventing gestational diabetes mellitus. Cochrane Database Syst. Rev. 2015, 4, CD010443. [Google Scholar] [CrossRef]
- Song, C.; Li, J.; Leng, J.; Ma, R.C.; Yang, X. Lifestyle intervention can reduce the risk of gestational diabetes: A meta-analysis of randomized controlled trials. Obes. Rev. 2016, 17, 960–969. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.-Q.; Qi, H.-P.; Luo, Z.-C.; Fraser, W.D. Maternal vitamin D status and adverse pregnancy outcomes: A systematic review and meta-analysis. J. Matern. Fetal Neonatal Med. 2013, 26, 889–899. [Google Scholar] [CrossRef]
- Ojo, O.; Weldon, S.M.; Thompson, T.; Vargo, E.J. The effect of vitamin D supplementation on glycaemic control in women with gestational diabetes mellitus: A systematic review and meta-analysis of randomised controlled trials. Int. J. Environ. Res. Public Health 2019, 16, 1716. [Google Scholar] [CrossRef]
- Wilson, R.L.; Leviton, A.J.; Leemaqz, S.Y.; Anderson, P.H.; Grieger, J.A.; Grzeskowiak, L.E.; Verburg, P.E.; McCowan, L.; Dekker, G.A.; Bianco-Miotto, T. Vitamin D levels in an Australian and New Zealand cohort and the association with pregnancy outcome. BMC Pregnancy Childbirth 2018, 18, 251. [Google Scholar] [CrossRef] [PubMed]
- Yin, W.; Jin, D.; Yao, M.; Yu, W.; Zhu, P. Effect of vitamin D supplementation on gestational diabetes mellitus: A Meta-analysis. Wei Sheng Yan Jiu J. Hyg. Res. 2019, 48, 811–821. [Google Scholar]
- Jin, S.; Sha, L.; Dong, J.; Yi, J.; Liu, Y.; Guo, Z.; Hu, B. Effects of nutritional strategies on glucose homeostasis in gestational diabetes mellitus: A systematic review and network meta-analysis. J. Diabetes Res. 2020, 2020, 6062478. [Google Scholar] [CrossRef]
- Jamilian, M.; Karamali, M.; Taghizadeh, M.; Sharifi, N.; Jafari, Z.; Memarzadeh, M.R.; Mahlouji, M.; Asemi, Z. Vitamin D and evening primrose oil administration improve glycemia and lipid profiles in women with gestational diabetes. Lipids 2016, 51, 349–356. [Google Scholar] [CrossRef]
- Jamilian, M.; Mirhosseini, N.; Eslahi, M.; Bahmani, F.; Shokrpour, M.; Chamani, M.; Asemi, Z. The effects of magnesium-zinc-calcium-vitamin D co-supplementation on biomarkers of inflammation, oxidative stress and pregnancy outcomes in gestational diabetes. BMC Pregnancy Childbirth 2019, 19, 107. [Google Scholar] [CrossRef]
- D’Anna, R.; Scilipoti, A.; Giordano, D.; Caruso, C.; Cannata, M.L.; Interdonato, M.L.; Corrado, F.; Di Benedetto, A. myo-Inositol supplementation and onset of gestational diabetes mellitus in pregnant women with a family history of type 2 diabetes: A prospective, randomized, placebo-controlled study. Diabetes Care 2013, 36, 854–857. [Google Scholar] [CrossRef]
- D’Anna, R.; Di Benedetto, A.; Scilipoti, A.; Santamaria, A.; Interdonato, M.L.; Petrella, E.; Neri, I.; Pintaudi, B.; Corrado, F.; Facchinetti, F. Myo-inositol Supplementation for Prevention of Gestational Diabetes in Obese Pregnant Women: A Randomized Controlled Trial. Obs. Gynecol 2015, 126, 310–315. [Google Scholar] [CrossRef]
- Vitagliano, A.; Saccone, G.; Cosmi, E.; Visentin, S.; Dessole, F.; Ambrosini, G.; Berghella, V. Inositol for the prevention of gestational diabetes: A systematic review and meta-analysis of randomized controlled trials. Arch. Gynecol. Obstet. 2019, 299, 55–68. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.; Alwan, N.A.; West, J.; Brown, S.; McKinlay, C.J.; Farrar, D.; Crowther, C.A. Lifestyle interventions for the treatment of women with gestational diabetes. Cochrane Database Syst. Rev. 2017, 5, CD011970. [Google Scholar] [CrossRef] [PubMed]
- Landon, M.B.; Spong, C.Y.; Thom, E.; Carpenter, M.W.; Ramin, S.M.; Casey, B.; Wapner, R.J.; Varner, M.W.; Rouse, D.J.; Thorp Jr, J.M. A multicenter, randomized trial of treatment for mild gestational diabetes. N. Engl. J. Med. 2009, 361, 1339–1348. [Google Scholar] [CrossRef] [PubMed]
- Crowther, C.A.; Hiller, J.E.; Moss, J.R.; McPhee, A.J.; Jeffries, W.S.; Robinson, J.S. Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. N. Engl. J. Med. 2005, 352, 2477–2486. [Google Scholar] [CrossRef]
- Champion, M.L.; Harper, L.M. Gestational weight gain: Update on outcomes and interventions. Curr. Diabetes Rep. 2020, 20, 11. [Google Scholar] [CrossRef]


{kind=link}
| Author, Year |
Studies Included | Number of Participants | Intervention | Outcome | Effect | 95% CI | Risk Reduction | Quality of the Evidence (GRADE) |
|---|---|---|---|---|---|---|---|---|
| Ying Yu et al., 2018 [29] | 5 RCTs | 1370 | Exercise during pregnancy | A physical activity intervention might substantially reduce the incidence of gestational diabetes mellitus. | OR: 0.59 | CI = 0.39 to 0.88 | 41% | NA |
| Aune D et al., 2016 [22] | 4607 | Low vs. high-intensity physical activity before pregnancy | High-intensity training before pregnancy was more effective in reducing GDM risk | RR: 0.62 | CI = 0.41 to 0.94 | 38% | NA | |
| 3 cohorts | 3996 | Low vs. high-intensity physical activity during pregnancy | High-intensity training during pregnancy was more effective in reducing GDM risk | RR: 0.66 | CI = 0.36 to 1.21 | 34% | NA | |
| 2 cohorts | 2714 | Physical exercise in leisure time before and during pregnancy | Compared to women who were sedentary before and throughout pregnancy, women who were physically active before and during pregnancy had a 59% lower relative risk. | RR: 0.41 | CI = 0.23 to 0.73 | 59% | NA | |
| Davenport MH et al., 2018 [24] | 26 RCTs | 6934 | Prenatal exercise compared to no exercise | Exercise-only therapies decreased the likelihood of developing GDM by 38% compared to those that did not involve exercise. | OR: 0.62 | CI = 0.52 to 0.75 | 38% | Moderate |
| Da Silva SG. et al., 2017 [23] | 10 RCTs | 3790 | Leisure-Time Physical Activity | Preventive effect of leisure-time physical activity interventions on the onset of GDM | RR: 0.67 | CI = 0.49–0.92) | 33% | NA |
| 6 Cohorts | 6754 | OR: 0.75 | CI = 0.55 to 1.01 | 25% | NA | |||
| Mijatovic-Vukas. et al., 2018 [25] | 11 RCTs | 57,722 | Any type of physical activity pre-pregnancy | Pre-pregnancy physical activity reduced the risk of GDM by 30% | OR: 0.70 | CI = 0.57 to 0.85 | 30% | NA |
| 8 RCTs | 23,717 | Any type of physical activity early in pregnancy | Early in pregnancy physical activity reduced the risk of GDM by 21% | OR: 0.79 | CI = 0.64 to 0.97 | 21% | NA | |
| 6 RCTs | 45,162 | >15 MET hr./week pre-pregnancy | Reduced the risk of GDM by 48% | OR: 0.52 | CI = 0.27 to 1.00 | 48% | NA | |
| 4 RCTs | 19,730 | >90 min/week pre-pregnancy | Reduced risk of GDM by 46% | OR: 0.54 | CI = 0.34 to 0.87 | 46% | NA | |
| Russo LM. et al., 2015 [28] | 10 RCTs | 3401 | Group exercise intervention or individualized plan until GDM screening | Physical exercise during pregnancy has a minor protective impact against gestational diabetes. | RR: 0.72 | CI = 0.52–0.97 | 28% | Low |
| Ming W-K et al., 2018 [26] | 8 RCTs | 2981 | Physical activity during pregnancy | Positive effect on decreasing the incidence of GDM | Depending on different diagnostic criteria | |||
| RR: 0.58 | CI = 0.37 to 0.90 | 42% | NA | |||||
| RR: 0.60 | CI = 0.36 to 0.98 | 40% | NA | |||||
| Nasiri-Amiri F et al., 2019 [27] | 8 RCTs | 1441 | Physical activity during pregnancy | Physical activity during pregnancy, in the second trimester and 3 times/week were effective in reducing the risk of GDM by 24%, 36%, and 41% respectively. | RR: 0.76 | CI = 0.56 to 1.03 | 24% | NA |
| 4 RCTs | 1022 | Physical activity 3 times/week or less | RR: 0.59 | CI = 0.46 to 0.76 | 41% | NA | ||
| 4 RCTs | 797 | Physical activity in the second trimester | RR: 0.64 | CI = 0.40 to 1.04 | 36% | NA | ||
| Zheng J. et al., 2017 [30] | 5 RCTs | 1872 | Exercise at 10–22 weeks of gestation | An exercise intervention has been reported to significantly lower the risk of GDM when compared to a control intervention. | OR: 0.62 | CI = 0.43 to 0.89 | 38% | NA |
| Madhuvrata P. et al., 2015 [31] | 3 RCTs | 183 | Exercise during pregnancy | In terms of GDM, there was no statistical difference between the two groups. | OR: 0.77 | CI = 0.33 to 1.79 | 23% | NA |
| Doi SA et al., 2020 [34] | 11 RCTs | 1467 | Physical activity was delivered in healthcare facilities to pregnant women in high-risk pregnancies before the 20th week of gestation. | GDM risk was found to be significantly lower in pregnant women in the intervention group | RR: 0.53 | CI = 0.38 to 0.74 | 49% | NA |
| Author, Year | Studies Included | Number of Participants | Groups | Outcome | Relative Risk | Quality of the Evidence (GRADE) |
|---|---|---|---|---|---|---|
| Bain E et al., 2015 [60] | 13 RCTs | 4983 | Dietary and physical activity combination lifestyle interventions vs. standard management | There was no discernible difference in the risk of developing GDM Women who received the combined diet and activity intervention had lower GWG during pregnancy (mean difference (MD) 0.76 kg, (CI 1.55 to 0.03) | RR: 0.92, 95% (CI 0.68 to 1.23) | Moderate |
| Song et al., 2016 [61] | 29 RCTs | 11,487 | Dietary, physical activity, or combination lifestyle interventions vs. standard management | GDM risk was reduced by 18% (95 percent CI 5–30%) (p = 0.0091). Subgroup analysis revealed that such an intervention was successful among women who received it before the 15th gestational week | RR: 0.80, 95% CI 0.66–0.97). | Low to moderate |
| Shepherd et al., 2017 [55] | 23 RCTs | 8918 | Combination of dietary and physical activity interventions vs. standard management | The diet and exercise intervention group had a probable lower risk of GDM compared to the standard care group | RR: 0.85, 95% (CI 0.71 to 1.01) | Moderate |
| Guo et al., 2019 [36] | 47 RCTs | 15,745 | Dietary, physical activity, or combination lifestyle interventions vs. standard management | GDM was prevented by diet and physical activity during pregnancy | RR: 0.77, 95% (CI 0.69–0.87) | Low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zakaria, H.; Abusanana, S.; Mussa, B.M.; Al Dhaheri, A.S.; Stojanovska, L.; Mohamad, M.N.; Saleh, S.T.; Ali, H.I.; Cheikh Ismail, L. The Role of Lifestyle Interventions in the Prevention and Treatment of Gestational Diabetes Mellitus. Medicina 2023, 59, 287. https://doi.org/10.3390/medicina59020287
Zakaria H, Abusanana S, Mussa BM, Al Dhaheri AS, Stojanovska L, Mohamad MN, Saleh ST, Ali HI, Cheikh Ismail L. The Role of Lifestyle Interventions in the Prevention and Treatment of Gestational Diabetes Mellitus. Medicina. 2023; 59(2):287. https://doi.org/10.3390/medicina59020287
Chicago/Turabian StyleZakaria, Hala, Salah Abusanana, Bashair M. Mussa, Ayesha S. Al Dhaheri, Lily Stojanovska, Maysm N. Mohamad, Sheima T. Saleh, Habiba I. Ali, and Leila Cheikh Ismail. 2023. "The Role of Lifestyle Interventions in the Prevention and Treatment of Gestational Diabetes Mellitus" Medicina 59, no. 2: 287. https://doi.org/10.3390/medicina59020287