

Effect of Peptides from Plasma of Patients with Coronary Artery Disease on the Vascular Endothelial Cells
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Groups
2.2. Blood Sampling and Plasma Preparation
2.3. Plasma Peptide Pool Isolation
2.4. Human Endothelial Progenitor Cell (HEPC) Culture
2.5. Enzyme-Linked Immunosorbent Assay (ELISA)
2.6. Statistical Analysis
3. Results
3.1. Peptide Concentrations in Plasma of Patients with CAD and Healthy Subjects
3.2. The Levels of Some Soluble Anticoagulant As Well As Procoagulant Mediators Synthetized by Endothelial Cells Treated with Peptides Isolated from Plasma of Patients with CAD and Control Subjects
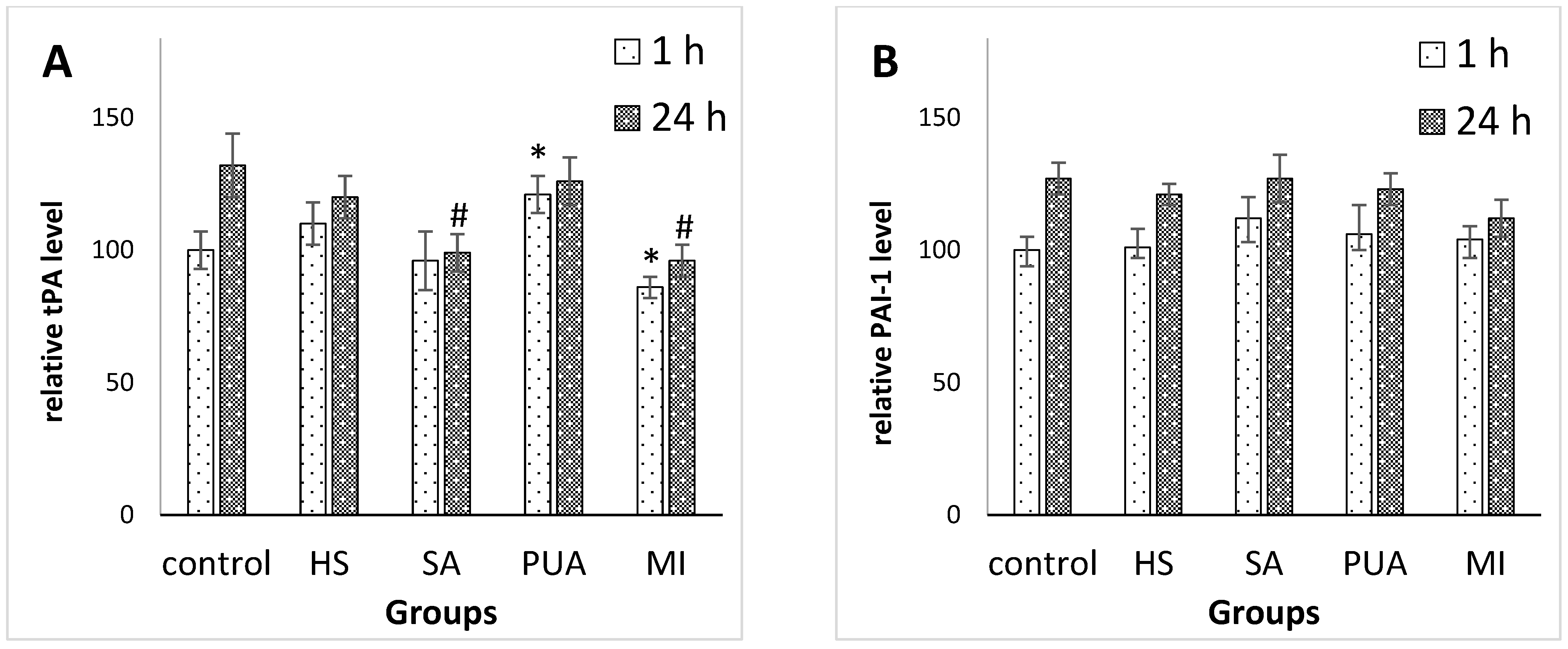
3.2.1. The Levels of Tissue Plasminogen Activator and Plasminogen Activator Inhibitor-1 Synthetized by Endothelial Cells Treated with Peptides Isolated from Plasma of Patients with CAD and Control Subjects
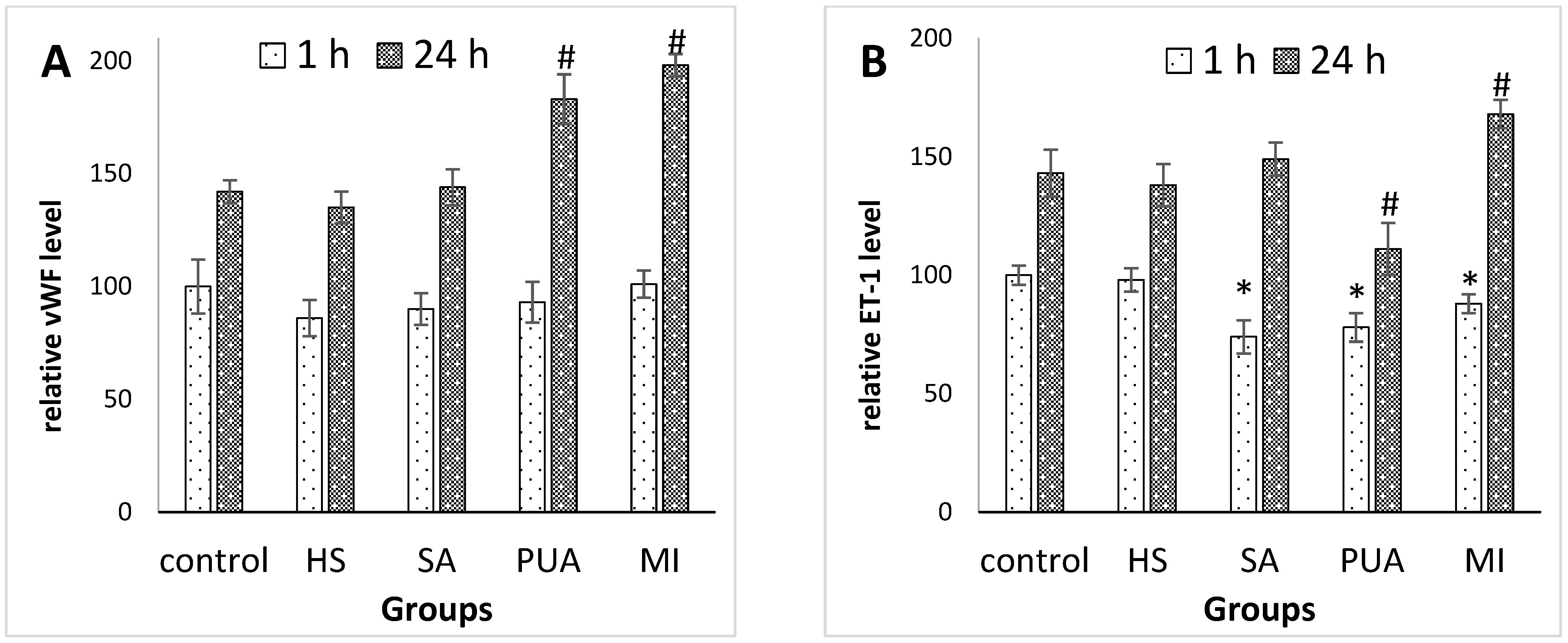
3.2.2. The Levels of von Willebrand factor and Endothelin-1 Synthetized by Endothelial Cells Treated with Peptides Isolated from Plasma of Patients with CAD and Control Subjects
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malakar, A.K.; Choudhury, D.; Halder, B.; Paul, P.; Uddin, A.; Chakraborty, S. A review on coronary artery disease, its risk factors, and therapeutics. J. Cell Physiol. 2019, 234, 16812–16823. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.; Fernando, S.; Schwarz, N.; Tan, J.; Bursill, C.; Psaltis, P. Inflammation as a Therapeutic Target in Atherosclerosis. J. Clin. Med. 2019, 8, 1109. [Google Scholar] [CrossRef] [Green Version]
- Zmysłowski, A.; Szterk, A. Current knowledge on the mechanism of atherosclerosis and pro-atherosclerotic properties of oxysterols. Lipids Health Dis. 2017, 16, 188. [Google Scholar] [CrossRef] [Green Version]
- Alfarisi, H.A.H.; Mohamed, Z.B.H.; Ibrahim, M.B. Basic pathogenic mechanisms of atherosclerosis. Egypt. J. Basic Appl. Sci. 2020, 7, 116–125. [Google Scholar] [CrossRef]
- Gutierrez, E.; Flammer, A.J.; Lerman, L.O.; Elizaga, J.; Lerman, A.; Fernandez-Aviles, F. Endothelial dysfunction over the course of coronary artery disease. Eur. Heart J. 2013, 34, 3175–3181. [Google Scholar] [CrossRef] [Green Version]
- Dengel, D.R.; Bronas, U.G. The Role of Endothelial Dysfunction on Development and Progression of Atherosclerosis and Methods to Assess Vascular Function and Structure. Am. J. Lifestyle Med. 2010, 4, 445–456. [Google Scholar] [CrossRef]
- Galley, H.F.; Webster, N.R. Physiology of the endothelium. Br. J. Anaesth. 2004, 93, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Sandoo, A.; Veldhuijzen van Zanten, J.J.C.; Metsios, G.S.; Carroll, D.; Kitas, G.D. The Endothelium and Its Role in Regulating Vascular Tone. Open Cardiovasc. Med. J. 2010, 4, 302–312. [Google Scholar] [CrossRef] [Green Version]
- Félétou, M.; Köhler, R.; Vanhoutte, P.M. Endothelium-derived Vasoactive Factors and Hypertension: Possible Roles in Pathogenesis and as Treatment Targets. Curr. Hypertens. Rep. 2010, 12, 267–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radder, C.M.; Beekhuizen, H.; Kanhai, H.; Brand, A. Effect of maternal anti-HPA-1a antibodies and polyclonal IVIG on the activation status of vascular endothelial cells. Clin. Exp. Immunol. 2004, 137, 216–222. [Google Scholar] [CrossRef]
- Chuhray, S.M.; Lavrynenko, V.E.; Kaminsky, R.F.; Dzevulska, I.V.; Malikov, O.V.; Matkivska, R.M.; Shobat, L.B.; Kovalchuk, O.I.; Sokurenko, L.M. Morphofunctional status of cardio-vascular system of rats with arterial hypertension. Wiad. Lek. 2020, 73, 355–359. [Google Scholar] [CrossRef] [PubMed]
- Chuhray, S.M.; Lavrynenko, V.E.; Kaminsky, R.F.; Dzevulska, I.V.; Malikov, O.V.; Kovalchuk, O.I.; Sokurenko, L.M. Morphofunctional status of cardio-vascular system of rats with congenital hypothyreosis. Wiad. Lek. 2019, 72, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Katrii, T.; Raksha, N.; Halenova, T.; Vovk, T.; Savchuk, O.; Ostapchenko, L.; Tomchuk, V.; Melnyk, V. Influence of peptide pools from the plasma of ischemic stroke patients on hemostasis. Curr. Top. Pept. Protein Res. 2020, 21, 21–29. [Google Scholar]
- Ostapchenko, L.; Savchuk, O.; Burlova-Vasilieva, N. Enzyme electrophoresis method in analysis of active components of haemostasis system. Adv. Biosci. Biotechnol. 2011, 2, 20–26. [Google Scholar] [CrossRef] [Green Version]
- Gubar, O.S.; Rodnichenko, A.E.; Zlatska, O.V.; Zubov, D.O.; Litvinova, L.S.; Shupletsova, V.V.; Vasyliev, R.G. Isolation and Large Scale Expansion of Human Endothelial Progenitor Cells from Peripheral Blood. Probl. Cryobiol. Cryomedicine 2018, 28, 29–33. [Google Scholar] [CrossRef] [Green Version]
- Sillen, M.; Declerck, P.J. A Narrative Review on Plasminogen Activator Inhibitor-1 and Its (Patho)Physiological Role: To Target or Not to Target? Int. J. Mol. Sci. 2021, 22, 2721. [Google Scholar] [CrossRef]
- Jung, R.G.; Motazedian, P.; Ramirez, F.D.; Simard, T.; Di Santo, P.; Visintini, S.; Faraz, M.A.; Labinaz, A.; Jung, Y.; Hibbert, B. Association between plasminogen activator inhibitor-1 and cardiovascular events: A systematic review and meta-analysis. Thromb. J. 2018, 16, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rayner, S.G.; Scholl, Z.; Mandrycky, C.J.; Chen, J.; LaValley, K.N.; Leary, P.J.; Altemeier, W.A.; Liles, W.C.; Chung, D.W.; López, J.A.; et al. Endothelial-derived von Willebrand factor accelerates fibrin clotting within engineered microvessels. J. Thromb. Haemost. 2022, 20, 1627–1637. [Google Scholar] [CrossRef]
- Marchi, R.; Rojas, H. Effect of von Willebrand factor on clot structure and lysis. Blood Coagul. Fibrinolysis 2015, 26, 533–536. [Google Scholar] [CrossRef] [PubMed]
- Marasciulo, F.L.; Montagnani, M.; Potenza, M.A. Endothelin-1: The yin and yang on vascular function. Curr. Med. Chem. 2006, 13, 1655–1665. [Google Scholar] [CrossRef] [PubMed]
- Sanders, E.J.; Harvey, S. Peptide hormones as developmental growth and differentiation factors. Dev. Dyn. 2008, 237, 1537–1552. [Google Scholar] [CrossRef]
- Fosgerau, K.; Hoffmann, T. Peptide therapeutics: Current status and future directions. Drug Discov. Today 2015, 20, 122–128. [Google Scholar] [CrossRef] [Green Version]
- Fricker, L.D. Neuropeptide-processing enzymes: Applications for drug discovery. AAPS J. 2005, 7, E449–E455. [Google Scholar] [CrossRef] [PubMed]
- Glickman, M.H.; Ciechanover, A. The Ubiquitin-Proteasome Proteolytic Pathway: Destruction for the Sake of Construction. Physiol. Rev. 2002, 82, 373–428. [Google Scholar] [CrossRef] [PubMed]
- Silveira, P.; Gil, J.; Casis, L.; Irazusta, J. Peptide Metabolism and the Control of Body Fluid Homeostasis. Curr. Med. Chem. Hematol. Agents 2004, 2, 219–238. [Google Scholar] [CrossRef]
- Miller, G.D. Appetite Regulation: Hormones, Peptides, and Neurotransmitters and Their Role in Obesity. Am. J. Lifestyle Med. 2019, 13, 586–601. [Google Scholar] [CrossRef] [PubMed]
- Raksha, N.; Halenova, T.; Vovk, T.; Kharchenko, O.; Savchuk, O.; Samborska, I.; Zaichko, N.; Ostapchenko, L.; Maievskyi, O. Protein-peptide composition in the lungs of rats with hyperhomocysteinemia. Boll. Soc. Ital. Biol. Sper. 2021, 94, 67–71. [Google Scholar] [CrossRef]
- De Araujo, C.B.; Heimann, A.S.; Remer, R.A.; Russo, L.C.; Colquhoun, A.; Forti, F.L.; Ferro, E.S. Intracellular Peptides in Cell Biology and Pharmacology. Biomolecules 2019, 9, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiryaev, S.A.; Cieplak, P.; Aleshin, A.E.; Sun, Q.; Zhu, W.; Motamedchaboki, K.; Sloutsky, A.; Strongin, A.Y. Matrix metalloproteinase proteolysis of the mycobacterial HSP65 protein as a potential source of immunogenic peptides in human tuberculosis. FEBS J. 2011, 278, 3277–3286. [Google Scholar] [CrossRef]
- Apostolopoulos, V.; Bojarska, J.; Chai, T.-T.; Elnagdy, S.; Kaczmarek, K.; Matsoukas, J.; New, R.; Parang, K.; Lopez, O.P.; Parhiz, H.; et al. A Global Review on Short Peptides: Frontiers and Perspectives. Molecules 2021, 26, 430. [Google Scholar] [CrossRef]
- Tammen, H.; Schulte, I.; Hess, R.; Menzel, C.; Kellmann, M.; Mohring, T.; Schulz-Knappe, P. Peptidomic analysis of human blood specimens: Comparison between plasma specimens and serum by differential peptide display. Proteomics 2005, 5, 3414–3422. [Google Scholar] [CrossRef]
- Li, Y.; Li, S.; Wu, H. Ubiquitination-proteasome system (UPS) and autophagy two main protein degradation machineries in response to cell stress. Cells 2022, 11, 851. [Google Scholar] [CrossRef] [PubMed]
- Apcher, S.; Millot, G.; Daskalogianni, C.; Scherl, A.; Manoury, B.; Fåhraeus, R. Translation of pre-spliced RNAs in the nuclear compartment generates peptides for the MHC class I pathway. Proc. Natl. Acad. Sci. USA 2013, 110, 17951–17956. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Healthy Subjects (n = 20) | Patients with Stable Angina (n = 25) | Patients with Progressive Unstable Angina (n = 28) | Patients with Myocardial Infarction (n = 17) | |
|---|---|---|---|---|
| Age, years | 53 ± 6 | 63 ± 8 | 67 ± 7 | 61 ± 7 |
| Sex, male, n (%) | 10 (50) | 15 (60) | 14 (50) | 11 (65) |
| Smoking, n (%) | 7 (35) | 9 (36) | 11 (39) | 6 (35) |
| BMI, kg/m2 | 27 ± 4 | 29 ± 6 | 29 ± 3 | 28 ± 6 |
| TC, mmol·L−1 | 5.14 ± 0.99 | 5.96 ± 1.64 | 6.39 ± 2.18 | 5.28 ± 0.94 |
| TG, mmol·L−1 | 1.28 ± 0.43 | 2.50 ± 0.70 | 2.21 ± 1.12 | 3.29 ± 1.17 * |
| LDL, mmol·L−1 | 2.38 ± 0.47 | 3.39 ± 1.38 | 3.75 ± 1.19 | 3.29 ± 1.17 |
| HDL, mmol·L−1 | 1.64 ± 0.45 | 1.64 ± 0.87 | 1.31 ± 0.51 | 0.85 ± 0.24 * |
| TP, g·L−1 | 13.8 ± 4.0 | 10.4 ± 5.0 § | 11.5 ± 4.6 § | 35.5 ± 11.8 * |
| hs-cTnI, pg·mL−1 | ≤5 | ≤5 | 17.6 ± 9.2 *#§ | 24.3 ± 10.2 *# |
| Groups | Peptide Concentration, μg per mL of Plasma |
|---|---|
| Healthy subjects (n = 20) | 68 ± 18 |
| Patients with stable angina (n = 25) | 336 ± 17 *§ |
| Patients with progressive unstable angina (n = 28) | 428 ± 27 *#§ |
| Patients with myocardial infarction (n = 17) | 987 ± 64 *# |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kozyk, M.; Strubchevska, K.; Marynenko, T.; Zlatska, A.; Halenova, T.; Raksha, N.; Savchuk, O.; Falalyeyeva, T.; Kovalchuk, O.; Ostapchenko, L. Effect of Peptides from Plasma of Patients with Coronary Artery Disease on the Vascular Endothelial Cells. Medicina 2023, 59, 238. https://doi.org/10.3390/medicina59020238
Kozyk M, Strubchevska K, Marynenko T, Zlatska A, Halenova T, Raksha N, Savchuk O, Falalyeyeva T, Kovalchuk O, Ostapchenko L. Effect of Peptides from Plasma of Patients with Coronary Artery Disease on the Vascular Endothelial Cells. Medicina. 2023; 59(2):238. https://doi.org/10.3390/medicina59020238
Chicago/Turabian StyleKozyk, Marko, Kateryna Strubchevska, Tetiana Marynenko, Alena Zlatska, Tetiana Halenova, Nataliia Raksha, Olexii Savchuk, Tetyana Falalyeyeva, Oleksandr Kovalchuk, and Ludmyla Ostapchenko. 2023. "Effect of Peptides from Plasma of Patients with Coronary Artery Disease on the Vascular Endothelial Cells" Medicina 59, no. 2: 238. https://doi.org/10.3390/medicina59020238