
The Association between Brain-Derived Neurotrophic Factor (BDNF) Protein Level and Body Mass Index

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Recruitment
2.1.1. Body Mass Index (BMI) as a Measurement of Obesity
2.1.2. Serum BDNF Protein Measurement
2.2. Statistical Analysis
3. Results
3.1. Subject Characteristics
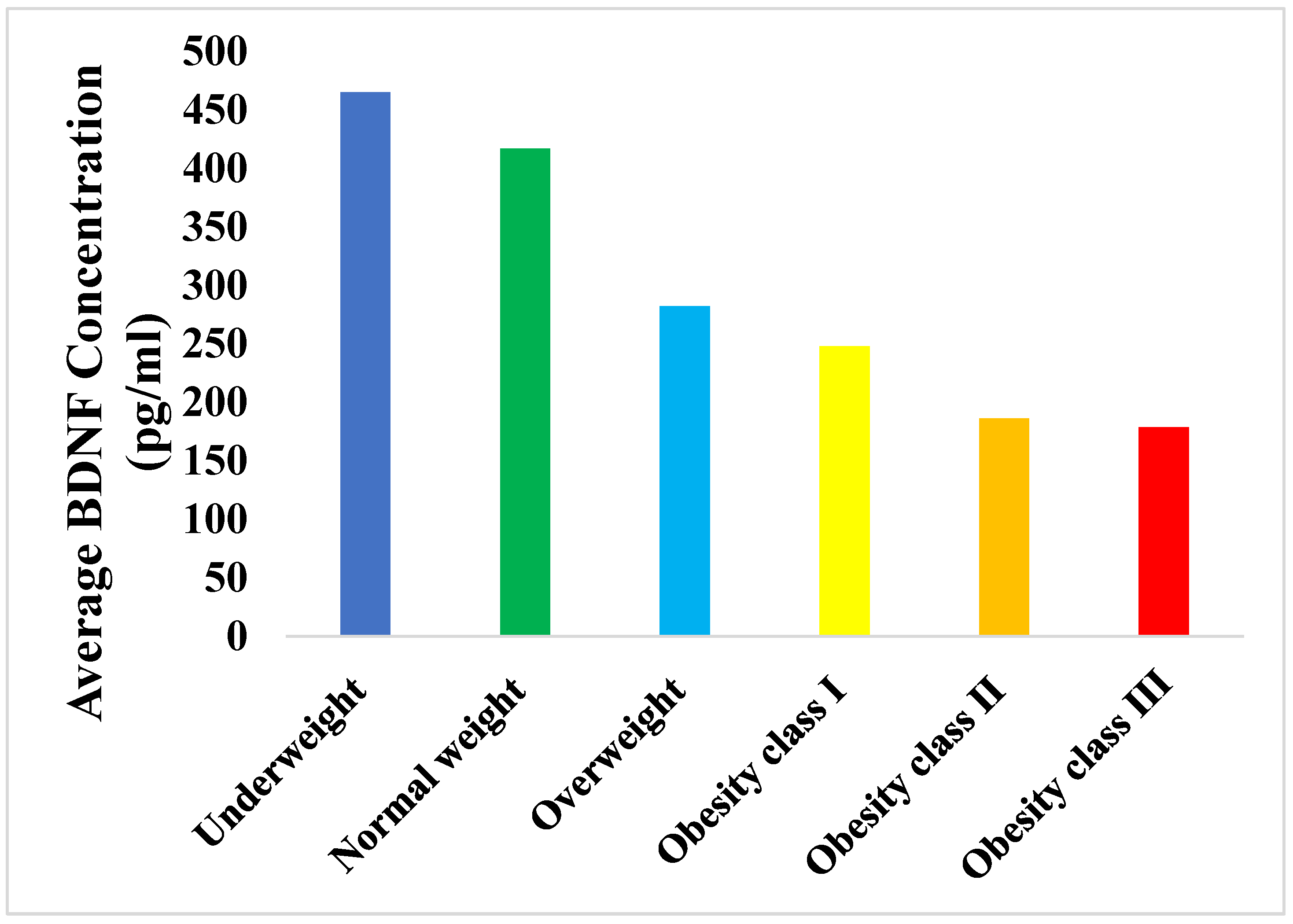
3.2. Relationship of the BDNF Serum Levels with the BMI of the Different Categories
3.3. Correlation between BDNF Concentrations and the BMI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, Y.; Beydoun, M.A.; Min, J.; Xue, H.; Kaminsky, L.A.; Cheskin, L.J. Has the prevalence of overweight, obesity and central obesity levelled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int. J. Epidemiol. 2020, 49, 810–823. [Google Scholar] [CrossRef]
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 16 November 2021).
- Ampofo, A.G.; Boateng, E.B. Beyond 2020: Modelling obesity and diabetes prevalence. Diabetes Res. Clin. Pract. 2020, 167, 108362. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, A.K.; Dubey, P.; Cistola, D.P.; Reddy, S.Y. Association Between Obesity and Cardiovascular Outcomes: Updated Evidence from Meta-analysis Studies. Curr. Cardiol. Rep. 2020, 22, 25. [Google Scholar] [CrossRef]
- Katta, N.; Loethen, T.; Lavie, C.J.; Alpert, M.A. Obesity and Coronary Heart Disease: Epidemiology, Pathology, and Coronary Artery Imaging. Curr. Probl. Cardiol. 2021, 46, 100655. [Google Scholar] [CrossRef] [PubMed]
- Okunogbe, A.; Nugent, R.; Spencer, G.; Ralston, J.; Wilding, J. Economic impacts of overweight and obesity: Current and future estimates for eight countries. BMJ Glob. Health 2021, 6, e006351. [Google Scholar] [CrossRef] [PubMed]
- Ahirwar, R.; Mondal, P.R. Prevalence of obesity in India: A systematic review. Diabetes Metab. Syndr. 2019, 13, 318–321. [Google Scholar] [CrossRef]
- Twig, G.; Reichman, B.; Afek, A.; Derazne, E.; Hamiel, U.; Furer, A.; Gershovitz, L.; Bader, T.; Cukierman-Yaffe, T.; Kark, J.D.; et al. Severe obesity and cardio-metabolic comorbidities: A nationwide study of 2.8 million adolescents. Int. J. Obes. 2019, 43, 1391–1399. [Google Scholar] [CrossRef]
- Althumiri, N.A.; Basyouni, M.H.; AlMousa, N.; AlJuwaysim, M.F.; Almubark, R.A.; BinDhim, N.F.; Alkhamaali, Z.; Alqahtani, S.A. Obesity in Saudi Arabia in 2020: Prevalence, Distribution, and Its Current Association with Various Health Conditions. Healthcare 2021, 9, 311. [Google Scholar] [CrossRef]
- Alghadir, A.H.; Iqbal, Z.A.; Gabr, S.A. Differences among Saudi and Expatriate Students: Body Composition Indices, Sitting Time Associated with Media Use and Physical Activity Pattern. Int. J. Environ. Res. Public Health 2020, 17, 832. [Google Scholar] [CrossRef] [Green Version]
- Al-Qahtani, A.M. Prevalence and Predictors of Obesity and Overweight among Adults Visiting Primary Care Settings in the Southwestern Region, Saudi Arabia. Biomed. Res. Int. 2019, 2019, 8073057. [Google Scholar] [CrossRef]
- Al-Nozha, M.M.; Al-Mazrou, Y.Y.; Al-Maatouq, M.A.; Arafah, M.R.; Khalil, M.Z.; Khan, N.B.; Al-Marzouki, K.; Abdullah, M.A.; Al-Khadra, A.H.; Al-Harthi, S.S.; et al. Obesity in Saudi Arabia. Saudi Med. J. 2005, 26, 824–829. [Google Scholar]
- Fruh, S.M. Obesity: Risk factors, complications, and strategies for sustainable long-term weight management. J. Am. Assoc. Nurse Pract. 2017, 29, S3–S14. [Google Scholar] [CrossRef]
- Sarma, S.; Sockalingam, S.; Dash, S. Obesity as a multisystem disease: Trends in obesity rates and obesity-related complications. Diabetes Obes. Metab. 2021, 23 (Suppl. S1), 3–16. [Google Scholar] [CrossRef]
- Kinlen, D.; Cody, D.; O’Shea, D. Complications of obesity. QJM 2018, 111, 437–443. [Google Scholar] [CrossRef] [Green Version]
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef] [Green Version]
- Homs, C.; Berruezo, P.; Según, G.; Estrada, L.; de Bont, J.; Riera-Romaní, J.; Carrillo-Álvarez, E.; Schröder, H.; Milà, R.; Gómez, S.F. Family-based intervention to prevent childhood obesity among school-age children of low socioeconomic status: Study protocol of the FIVALIN project. BMC Pediatr. 2021, 21, 246. [Google Scholar] [CrossRef]
- Marcos-Pasero, H.; Aguilar-Aguilar, E.; Ikonomopoulou, M.P.; Loria-Kohen, V. BDNF Gene as a Precision Skill of Obesity Management. Adv. Exp. Med. Biol. 2021, 1331, 233–248. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.S.; He, Y.; Xu, L.; Jin, Y.; Zhang, W.S.; Jiang, C.Q.; Cheng, K.K.; Lam, T.H. Brain-derived neurotrophic factor gene variants and obesity in former smokers. BMC Genom. 2021, 22, 668. [Google Scholar] [CrossRef] [PubMed]
- Piotrowicz, Z.; Chalimoniuk, M.; Czuba, M.; Langfort, J. Rola neurotroficznego czynnika pochodzenia mózgowego w kontroli łaknienia [Role of brain-derived neurotrophic factor in appetite control]. Postepy Biochem. 2020, 66, 205–212. [Google Scholar] [CrossRef] [PubMed]
- da Fonseca, A.C.P.; Abreu, G.M.; Palhinha, L.; Zembrzuski, V.M.; Campos Junior, M.; Carneiro, J.R.I.; Neto, J.F.N.; Magno, F.C.C.M.; Rosado, E.L.; Monteiro, C.M.M.; et al. A Rare Potential Pathogenic Variant in the BDNF Gene is Found in a Brazilian Patient with Severe Childhood-Onset Obesity. Diabetes Metab. Syndr. Obes. 2021, 14, 11–22. [Google Scholar] [CrossRef]
- Katuri, R.B.; Gaur, G.S.; Sahoo, J.P.; Bobby, Z.; Shanmugavel, K. Association of Circulating Brain-Derived Neurotrophic Factor with Cognition among Adult Obese Population. J. Obes. Metab. Syndr. 2021, 30, 163–172. [Google Scholar] [CrossRef]
- Huang, C.J.; Mari, D.C.; Whitehurst, M.; Slusher, A.; Wilson, A.; Shibata, Y. Brain-derived neurotrophic factor expression ex vivo in obesity. Physiol. Behav. 2014, 123, 76–79. [Google Scholar] [CrossRef]
- Bumb, J.M.; Bach, P.; Grosshans, M.; Wagner, X.; Koopmann, A.; Vollstädt-Klein, S.; Schuster, R.; Wiedemann, K.; Kiefer, F. BDNF influences neural cue-reactivity to food stimuli and food craving in obesity. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 963–974. [Google Scholar] [CrossRef] [PubMed]
- Glud, M.; Christiansen, T.; Larsen, L.H.; Richelsen, B.; Bruun, J.M. Changes in Circulating BDNF in relation to Sex, Diet, and Exercise: A 12-Week Randomized Controlled Study in Overweight and Obese Participants. J Obes. 2019, 2019, 4537274. [Google Scholar] [CrossRef] [PubMed]
- Lharbi, N.S.; Almutari, R.; Jones, S.; Al-Daghri, N.; Khunti, K.; de Lusignan, S. Trends in the prevalence of type 2 diabetes mellitus and obesity in the Arabian Gulf States: Systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2014, 106, e30–e33. [Google Scholar] [CrossRef] [Green Version]
- Han, J.C.; Liu, Q.R.; Jones, M.; Levinn, R.L.; Menzie, C.M.; Jefferson-George, K.S.; Adler-Wailes, D.C.; Sanford, E.L.; Lacbawan, F.L.; Uhl, G.R.; et al. Brain-derived neurotrophic factor and obesity in the WAGR syndrome. N. Engl. J. Med. 2008, 359, 918–927. [Google Scholar] [CrossRef] [Green Version]
- Liao, G.Y.; Kinney, C.E.; An, J.J.; Xu, B. TrkB-expressing neurons in the dorsomedial hypothalamus are necessary and sufficient to suppress homeostatic feeding. Proc. Natl. Acad. Sci. USA 2019, 116, 3256–3261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonoyama, T.; Stadler, L.K.J.; Zhu, M.; Keogh, J.M.; Henning, E.; Hisama, F.; Kirwan, P.; Jura, M.; Blaszczyk, B.K.; DeWitt, D.C.; et al. Human BDNF/TrkB variants impair hippocampal synaptogenesis and associate with neurobehavioural abnormalities. Sci. Rep. 2020, 10, 9028. [Google Scholar] [CrossRef]
- Sandrini, L.; Di Minno, A.; Amadio, P.; Ieraci, A.; Tremoli, E.; Barbieri, S.S. Association between Obesity and Circulating Brain-Derived Neurotrophic Factor (BDNF) Levels: Systematic Review of Literature and Meta-Analysis. Int. J. Mol. Sci. 2018, 19, 2281. [Google Scholar] [CrossRef] [Green Version]
- Gray, J.; Yeo, G.S.; Cox, J.J.; Morton, J.; Adlam, A.L.; Keogh, J.M.; Yanovski, J.A.; El Gharbawy, A.; Han, J.C.; Tung, Y.L.; et al. Hyperphagia, severe obesity, impaired cognitive function, and hyperactivity associated with functional loss of one copy of the brain-derived neurotrophic factor (BDNF) gene. Diabetes 2006, 55, 3366–3371. [Google Scholar] [CrossRef] [Green Version]
- Strawbridge, W.J.; Wallhagen, M.I.; Shema, S.J. New NHLBI clinical guidelines for obesity and overweight: Will they promote health? Am. J. Public Health 2000, 90, 340–343. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Prevalence of overweight and obesity among adults with diagnosed diabetes—United States, 1988–1994 and 1999–2002. MMWR Morb. Mortal. Wkly Rep. 2004, 53, 1066–1068. [Google Scholar]
- Global BMI Mortality Collaboration; Di Angelantonio, E.; Bhupathiraju, S.N.; Wormser, D.; Gao, P.; Kaptoge, S.; de Gonzalez, A.B.; Cairns, B.J.; Huxley, R.; Jackson, C.L.; et al. Body-mass index and all-cause mortality: Individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet 2016, 388, 776–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celik Guzel, E.; Bakkal, E.; Guzel, S.; Eroglu, H.E.; Acar, A.; Topcu, B.; Kuçukyalcin, V. Can low brain-derived neurotrophic factor levels be a marker of the presence of depression in obese women? Neuropsychiatr. Dis. Treat. 2014, 10, 2079–2086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alomari, M.A.; Khabour, O.F.; Alawneh, K.; Alzoubi, K.H.; Maikano, A.B. The importance of physical fitness for the relationship of BDNF with obesity measures in young normal-weight adults. Heliyon 2020, 6, e03490. [Google Scholar] [CrossRef]
- El-Gharbawy, A.H.; Adler-Wailes, D.C.; Mirch, M.C.; Theim, K.R.; Ranzenhofer, L.; Tanofsky-Kraff, M.; Yanovski, J. Serum brain-derived neurotrophic factor concentrations in lean and overweight children and adolescents. J. Clin. Endocrinol. Metab. 2006, 91, 3548–3552. [Google Scholar] [CrossRef]
- Alharbi, K.K.; Richardson, T.G.; Khan, I.A.; Syed, R.; Mohammed, A.K.; Boustred, C.R.; Gaunt, T.R.; Tamimi, W.; Al-Daghri, N.M.; Day, I.N.M.; et al. Influence of adiposity-related genetic markers in a population of saudi arabians where other variables influencing obesity may be reduced. Dis. Markers 2014, 2014, 758232. [Google Scholar] [CrossRef]
- Lebrun, B.; Bariohay, B.; Moyse, E.; Jean, A. Brain-derived neurotrophic factor (BDNF) and food intake regulation: A minireview. Auton. Neurosci. 2006, 126–127, 30–38. [Google Scholar] [CrossRef]
- Kernie, S.G.; Liebl, D.J.; Parada, L.F. BDNF regulates eating behavior and locomotor activity in mice. EMBO J. 2000, 19, 1290–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lommatzsch, M.; Zingler, D.; Schuhbaeck, K.; Schloetcke, K.; Zingler, C.; Schuff-Werner, P.; Virchow, J.C. The impact of age, weight and gender on BDNF levels in human platelets and plasma. Neurobiol. Aging 2005, 26, 115–123. [Google Scholar] [CrossRef]
- Gajewska, E.; Sobieska, M.; Łojko, D.; Wieczorowska-Tobis, K.; Suwalska, A. Obesity itself does not influence BDNF serum levels in adults. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 3246–3250. [Google Scholar] [PubMed]
- Bathina, S.; Das, U.N. Brain-derived neurotrophic factor and its clinical implications. Arch. Med. Sci. 2015, 11, 1164–1178. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Age of the Participants (Year; Range) | 21–45 |
|---|---|
| Sex | |
| Female | 33 (31%) |
| Male | 75 (69%) |
| BMI Categories | N = 108 | Mean Rank BDNF Concentrations | df | X2 | p-Value |
|---|---|---|---|---|---|
| Underweight < 18.5 | 15 | 70.80 | |||
| Normal weight 18.5–24.9 | 23 | 73.74 | |||
| Overweight 25–29.9 | 22 | 53.48 | 5 | 24.201 | 0.0001 |
| Obesity class I 30–34.9 | 19 | 48.55 | |||
| Obesity class II 35–39.9 | 17 | 36.68 | |||
| Obesity class III ≥ 40 | 12 | 33.79 |
| Group vs. Group | p-Value * |
|---|---|
| Underweight vs. Obesity class III | 0.03 |
| Normal weight vs. Obesity class III | 0.005 |
| Underweight vs. Obesity class II | 0.03 |
| Normal weight vs. Obesity class II | 0.003 |
| Variable | BMI (kg/m2) |
|---|---|
| BDNF (pg/mL) | −0.478 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taha, M.A.; AL-maqati, T.N.; Alnaam, Y.A.; Alharbi, S.S.; Khaneen, R.; Almutairi, H.; AL-harbi, M. The Association between Brain-Derived Neurotrophic Factor (BDNF) Protein Level and Body Mass Index. Medicina 2023, 59, 99. https://doi.org/10.3390/medicina59010099
Taha MA, AL-maqati TN, Alnaam YA, Alharbi SS, Khaneen R, Almutairi H, AL-harbi M. The Association between Brain-Derived Neurotrophic Factor (BDNF) Protein Level and Body Mass Index. Medicina. 2023; 59(1):99. https://doi.org/10.3390/medicina59010099
Chicago/Turabian StyleTaha, Murtada A., Thekra N. AL-maqati, Yaser A. Alnaam, Sulaiman S. Alharbi, Rajaa Khaneen, Hajra Almutairi, and Mashael AL-harbi. 2023. "The Association between Brain-Derived Neurotrophic Factor (BDNF) Protein Level and Body Mass Index" Medicina 59, no. 1: 99. https://doi.org/10.3390/medicina59010099