

Evaluation of Hematological, Biochemical Profiles and Molecular Detection of Envelope Gene (gp-41) in Human Immunodeficiency Virus (HIV) among Newly Diagnosed Patients
 ,
,  , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Consideration
2.2. Consent Development
2.3. Samples Collection
2.3.1. Inclusion Criteria for HIV Patients
2.3.2. Exclusion Criteria for HIV Patients
2.4. Hematological and Biochemical Analysis
2.5. Serological Screening
2.5.1. Alere Determine Rapid Device
2.5.2. Chemiluminescent Microparticle Immuno-Assay (CMIA) for HIV-1/2
2.5.3. CMIA for HBsAg
2.5.4. CMIA for Anti-HCV
2.6. Molecular Identification
2.6.1. RNA Extraction
2.6.2. cDNA Synthesis
- First, thawed, mixed, and briefly centrifuged the components of the kit and stored them on ice.
- Then RNA template (10 µL), primer (1 µL), and nuclease-free water (1 µL) was added into a sterile, nuclease-free tube on ice.
- The template RNA (2 µL), reverse primer (1 µL), and nuclease free water (13 µL) were added in a screw cap Eppendorf and were gently mixed, briefly centrifuged, and kept at 65 °C for 5 min. Cooled down over ice, spun down, and then re-chilled the vial.
- Then, 10× Reaction Buffer (2 µL), RiboLock RNase Inhibitor (0.5 µL), 10 mM dNTP Mix (1 µL), and FIREScript RT (0.5 µL) were added, gently mixed and centrifuged.
- Incubated for 5 min at 25 °C, 30 min at 60 °C.
- Terminated the reaction by heating at 85 °C for 5 min.
- The whole process was carried out in a Multigene Optimax thermal cycler (Labnet, Iselin, NJ, USA). After performing the cDNA synthesis protocol cDNA was used immediately for amplification of the desired gene or stored at −20 °C.
2.6.3. Polymerase Chain Reaction
2.6.4. Conditions for Polymerase Chain Reaction
2.6.5. Gel Electrophoresis
2.7. Statistical Analysis
3. Results
3.1. Study Design
3.2. Demographic Charateristics of Studied Patients
3.3. Comparison of CBC of HIV-Positive Patients and Healthy Controls
3.4. Prevalence of LFTs and RFTs in HIV Patients and Healthy Controls
3.5. Prevalence of Anemia in HIV Patients and Healthy Controls
3.6. Prevalence of HBV and HCV Co-infection in HIV Patients and Controls
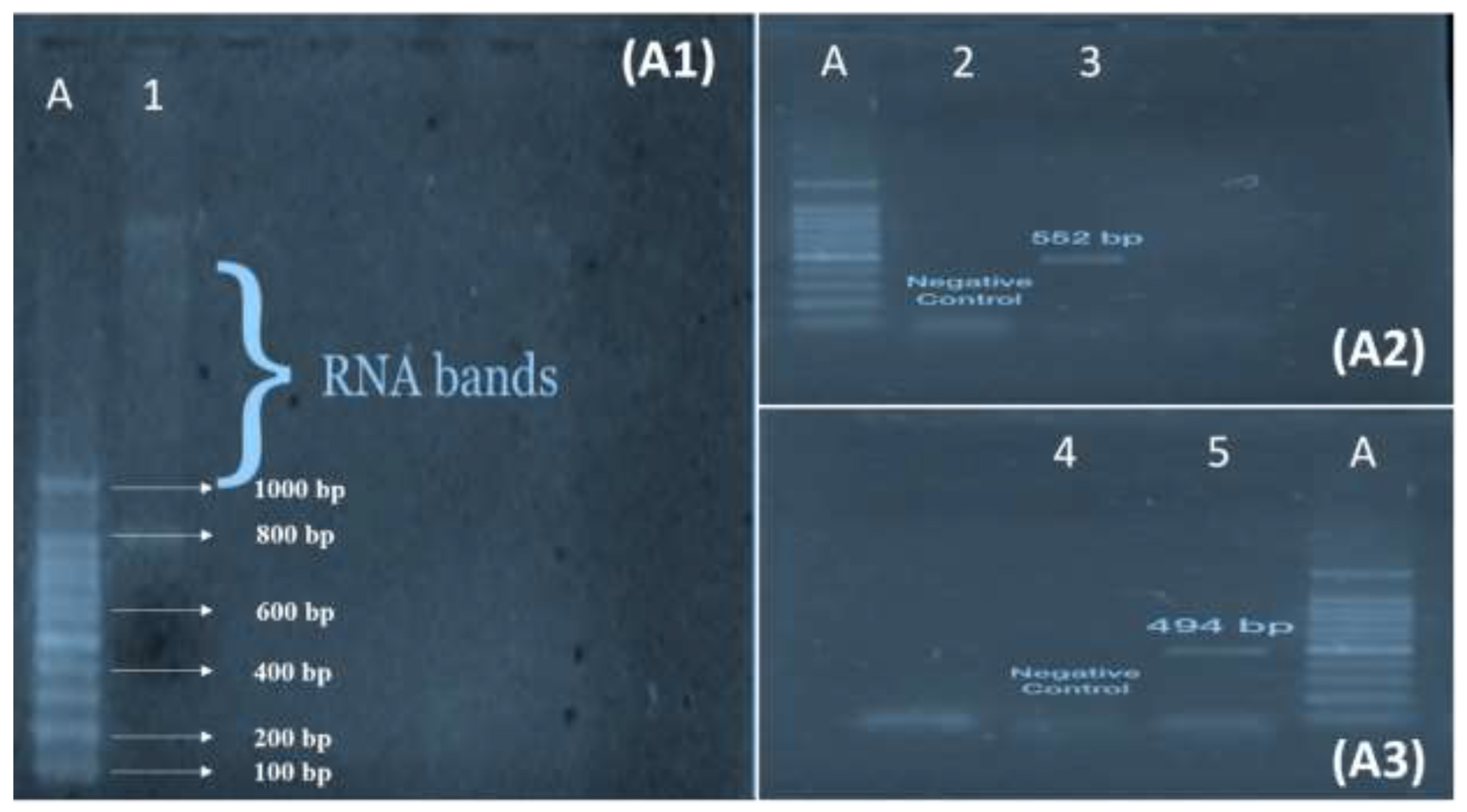
3.7. Polymerase Chain Reaction of GP41 Fragment 1 and 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zaheer, M.; Malik, S.S.; Javed, H.; Waheed, F.; Ahsan, M.; Irfan, M.; Fatima, W. CD4 count and Gender based hematological profile of HIV patients, in Punjab Pakistan. Pak. BioMed. J. 2022, 5, 115–119. [Google Scholar] [CrossRef]
- Melhuish, A.; Lewthwaite, P. Natural history of HIV and AIDS. Medicine 2018, 46, 356–361. [Google Scholar] [CrossRef]
- Sullivan, P.S.; Johnson, A.S.; Pembleton, E.S.; Stephenson, R.; Justice, A.C.; Althoff, K.N.; Bradley, H.; Castel, A.D.; Oster, A.M.; Rosenberg, E.S. Epidemiology of HIV in the USA: Epidemic burden, inequities, contexts, and responses. Lancet 2021, 397, 1095–1106. [Google Scholar] [CrossRef] [PubMed]
- Rabold, E.M.; Ali, H.; Fernandez, D.; Knuth, M.; Schenkel, K.; Asghar, R.J.; Baig, M.A.; Shaikh, S.; Morgan, O. Systematic review of reported HIV outbreaks, Pakistan, 2000–2019. Emerg. Infect. Dis. 2021, 27, 1039. [Google Scholar] [CrossRef]
- Carvalho, A.R.; Pinto, C.; Baleanu, D. HIV/HCV coinfection model: A fractional-order perspective for the effect of the HIV viral load. Adv. Differ. Equ. 2018, 2018, 2. [Google Scholar] [CrossRef]
- Wali, A.; Khan, D.; Safdar, N.; Shawani, Z.; Fatima, R.; Yaqoob, A.; Qadir, A.; Ahmed, S.; Rashid, H.; Ahmed, B. Prevalence of tuberculosis, HIV/AIDS, and hepatitis; in a prison of Balochistan: A cross-sectional survey. BMC Public Health 2019, 19, 1631. [Google Scholar] [CrossRef] [PubMed]
- Lodhi, A.; Sajjad, A.; Mehmood, K.; Lodhi, A.; Rizwan, S.; Ubaid, A.; Baloch, K.; Ahmed, S.; Mehmood, Z. Profile and predictors of hepatitis and HIV infection in patients on hemodialysis of Quetta, Pakistan. Drug Discov. Ther. 2019, 13, 274–279. [Google Scholar] [CrossRef] [Green Version]
- Afari, S.; Blay, E. Prevalence of haematological and serum biochemical abnormalities in hiv infected patients in Ghana, before and after antiretroviral therapy. Int. J. Virol. AIDS 2018, 5, 039. [Google Scholar]
- Chang, C.C.; Crane, M.; Zhou, J.; Mina, M.; Post, J.J.; Cameron, B.A.; Lloyd, A.R.; Jaworowski, A.; French, M.A.; Lewin, S.R. HIV and co-infections. Immunol. Rev. 2013, 254, 114–142. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, A.; Hashmi, F.K.; Khan, G.M. HIV outbreaks in Pakistan. Lancet HIV 2019, 6, e418. [Google Scholar] [CrossRef] [Green Version]
- Arif, F. HIV crisis in Sindh, Pakistan: The tip of the iceberg. Lancet Infect. Dis. 2019, 19, 695–696. [Google Scholar] [CrossRef] [PubMed]
- Awan, S.; Zia, N.; Sharif, F.; Shah, S.A.; Jamil, B. Types and risk factors of violence experienced by people living with HIV, Pakistan: A cross-sectional study. East. Mediterr. Health J. 2020, 26, 1200. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.D.; Wali, A.; Fatima, R.; Yaqoob, A.; Aziz, S. Prevalence and associated risk factors of HIV in prisons in Balochistan, Pakistan: A cross-sectional study. F1000Research 2018, 7, 1821. [Google Scholar] [CrossRef]
- Zahra, A.; Saleem, M.A.; Javed, H.; Khan, M.A.U. Prevalence of HCV-HIV Co-Infection with Intravenous Drug Users in Central Punjab, Pakistan. Pak. J. Zool. 2021, 54, 2003–2500. [Google Scholar] [CrossRef]
- Mir, F.; Mahmood, F.; Siddiqui, A.R.; Baqi, S.; Abidi, S.H.; Kazi, A.M.; Nathwani, A.A.; Ladhani, A.; Qamar, F.N.; Soofi, S.B. HIV infection predominantly affecting children in Sindh, Pakistan, 2019: A cross-sectional study of an outbreak. Lancet Infect. Dis. 2020, 20, 362–370. [Google Scholar] [CrossRef] [PubMed]
- D’arc, M.; Ayouba, A.; Esteban, A.; Learn, G.H.; Boué, V.; Liegeois, F.; Etienne, L.; Tagg, N.; Leendertz, F.H.; Boesch, C. Origin of the HIV-1 group O epidemic in western lowland gorillas. Proc. Natl. Acad. Sci. USA 2015, 112, E1343–E1352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wondimeneh, Y.; Alem, M.; Asfaw, F.; Belyhun, Y. HBV and HCV seroprevalence and their correlation with CD4 cells and liver enzymes among HIV positive individuals at University of Gondar Teaching Hospital, Northwest Ethiopia. Virol. J. 2013, 10, 171. [Google Scholar] [CrossRef] [Green Version]
- Platt, L.; French, C.E.; McGowan, C.R.; Sabin, K.; Gower, E.; Trickey, A.; McDonald, B.; Ong, J.; Stone, J.; Easterbrook, P. Prevalence and burden of HBV co-infection among people living with HIV: A global systematic review and meta-analysis. J. Viral Hepat. 2020, 27, 294–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrier, M.; Castain, L.; Regad, L.; Todesco, E.; Landman, R.; Visseaux, B.; Yazdanpanah, Y.; Rodriguez, C.; Joly, V.; Calvez, V. HIV-1 protease, Gag and gp41 baseline substitutions associated with virological response to a PI-based regimen. J. Antimicrob. Chemother. 2019, 74, 1679–1692. [Google Scholar] [CrossRef]
- Junaid, K.; Ali, H.; Khan, A.A.; Khan, T.A.; Khan, A.M.; Khan, A.; Nazim, R.; Tahira, K. Prevalence and associated factors of depression among patients with HIV/AIDS in Lahore, Pakistan: Cross-sectional study. Psychol. Res. Behav. Manag. 2021, 14, 77. [Google Scholar] [CrossRef] [PubMed]
- Chaganti, J.; Marripudi, K.; Staub, L.P.; Rae, C.D.; Gates, T.M.; Moffat, K.J.; Brew, B.J. Imaging correlates of the blood–brain barrier disruption in HIV-associated neurocognitive disorder and therapeutic implications. Aids 2019, 33, 1843–1852. [Google Scholar] [CrossRef] [PubMed]
- Roychoudhury, S.; Das, A.; Sengupta, P.; Dutta, S.; Roychoudhury, S.; Choudhury, A.P.; Ahmed, A.F.; Bhattacharjee, S.; Slama, P. Viral pandemics of the last four decades: Pathophysiology, health impacts and perspectives. Int. J. Environ. Res. Public Health 2020, 17, 9411. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, A.; Sen, J.; Rong, L.; Caffrey, M. Alanine scanning mutants of the HIV gp41 loop. J. Biol. Chem. 2005, 280, 27284–27288. [Google Scholar] [CrossRef] [Green Version]
- Kalinina, O.V.; Pfeifer, N.; Lengauer, T. Modelling binding between CCR5 and CXCR4 receptors and their ligands suggests the surface electrostatic potential of the co-receptor to be a key player in the HIV-1 tropism. Retrovirology 2013, 10, 130. [Google Scholar] [CrossRef] [Green Version]
- Batra, S.; Memon, Z.A.; Ochani, R.K.; Awan, S.; Bhimani, S.; Siddiqui, Y.; Mohiuddin, A.; Farooqi, H.A. Knowledge, attitude and practice of medical students towards HIV patients in their pre-clinical and post-clinical years in Karachi, Pakistan: A dual-center cross-sectional study. Infez. Med. 2020, 28, 231–237. [Google Scholar] [PubMed]
- Bbosa, N.; Kaleebu, P.; Ssemwanga, D. HIV subtype diversity worldwide. Curr. Opin. HIV AIDS 2019, 14, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Lau, K.A.; Wong, J.J. Current trends of HIV recombination worldwide. Infect. Dis. Rep. 2013, 5, 15–20. [Google Scholar] [CrossRef] [Green Version]
- Van Dyck, E.; Meheus, A.; Piot, P. Laboratory Diagnosis of Sexually Transmitted Diseases; World Health Organization: Geneva, Switzerland, 1999.
- Obeng, B.M.; Bonney, E.Y.; Asamoah-Akuoko, L.; Nii-Trebi, N.I.; Mawuli, G.; Abana, C.Z.-Y.; Sagoe, K.W.C. Transmitted drug resistance mutations and subtype diversity amongst HIV-1 sero-positive voluntary blood donors in Accra, Ghana. Virol. J. 2020, 17, 114. [Google Scholar] [CrossRef]
- Bayleyegn, B.; Woldu, B.; Yalew, A.; Asrie, F. Magnitude and associated factors of peripheral cytopenia among HIV-infected children attending at University of Gondar Specialized Referral Hospital, Northwest Ethiopia. PLoS ONE 2021, 16, e0247878. [Google Scholar] [CrossRef]
- Adetifa, I.; Temiye, E.; Akinsulie, A.; Ezeaka, V.; Iroha, E. Haematological abnormalities associated with paediatric HIV/AIDS in Lagos. Ann. Trop. Paediatr. 2006, 26, 121–125. [Google Scholar] [CrossRef]
- Rabold, E.M.; Shaikh, S.A.; Schenkel, K.; Baig, M.A.; Asghar, R.J.; Liban, A.; Morgan, O.; Ali, H. Notes from the Field: Pediatric HIV Outbreak in Ratodero, Pakistan—April 2019–April 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 1489. [Google Scholar] [CrossRef]
- Kaspar, M.B.; Sterling, R.K. Mechanisms of liver disease in patients infected with HIV. BMJ Open Gastroenterol. 2017, 4, e000166. [Google Scholar] [CrossRef] [Green Version]
- Platt, L.; Vickerman, P.; Collumbien, M.; Hasan, S.; Lalji, N.; Mayhew, S.; Muzaffar, R.; Andreasen, A.; Hawkes, S. Prevalence of HIV, HCV and sexually transmitted infections among injecting drug users in Rawalpindi and Abbottabad, Pakistan: Evidence for an emerging injection-related HIV epidemic. Sex. Transm. Infect. 2009, 85, ii17–ii22. [Google Scholar] [CrossRef]
- Teweldemedhin, M.; Asres, N.; Gebreyesus, H.; Asgedom, S.W. Tuberculosis-Human Immunodeficiency Virus (HIV) co-infection in Ethiopia: A systematic review and meta-analysis. BMC Infect. Dis. 2018, 18, 676. [Google Scholar] [CrossRef] [PubMed]
- French, H.; Greeff, M.; Watson, M.J.; Doak, C.M. HIV stigma and disclosure experiences of people living with HIV in an urban and a rural setting. Aids Care 2015, 27, 1042–1046. [Google Scholar] [CrossRef] [PubMed]
- French, H.; Greeff, M.; Watson, M.J. Experiences of people living with HIV and people living close to them of a comprehensive HIV stigma reduction community intervention in an urban and a rural setting. SAHARA-J J. Soc. Asp. HIV/AIDS 2014, 11, 105–115. [Google Scholar] [CrossRef] [PubMed]
- González-Ortega, E.; Ballana, E.; Badia, R.; Clotet, B.; Esté, J.A. Compensatory mutations rescue the virus replicative capacity of VIRIP-resistant HIV-1. Antivir. Res. 2011, 92, 479–483. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Name | Primer Sequence | Product Size (bp) | Annealing Temperature (°C) |
|---|---|---|---|
| TMF1 | CATGGGCCAAGTTCCGAGC | 494 | 59 |
| TMR1 | CGGACATCGGGAGGAGC | ||
| TMF2 | GGGGGGTACTAGGAACACG | 552 | 56 |
| TMR2 | CCCTCGAAGGTGGATCGAG |
| Characteristics | Frequency (n) | Percentage (%) | |
|---|---|---|---|
| Gender | Male | 24 | 64.86 |
| Female | 13 | 35.13 | |
| Age (Years) | 18–34 | 8 | 21.62 |
| 35–44 | 13 | 35.13 | |
| >45 | 16 | 43.24 | |
| Marital status | Married | 33 | 89.18 |
| Unmarried | 4 | 10.81 | |
| Employment status | Employed | 20 | 54.05 |
| Unemployed | 3 | 8.10 | |
| Self-business | 14 | 37.83 | |
| Education level | Primary school certificate | 17 | 45.94 |
| Secondary school certificate | 16 | 43.24 | |
| Bachelor’s degree | 4 | 10.81 | |
| Characteristics | Frequency (n) | Percentage (%) | |
|---|---|---|---|
| Possible route of acquiring HIV infection | Sexual intercourse with men | 05 | 13.51 |
| Sexual intercourse with women (sex workers) | 16 | 43.24 | |
| Sexual intercourse with transgender | 06 | 16.21 | |
| Intravenous drug use | 06 | 16.21 | |
| Reusing of injection needle from infected person | 01 | 2.70 | |
| Parental transfer | 01 | 2.70 | |
| Sexual intercourse with spouse | 03 | 8.10 | |
| Unknown | 02 | 5.40 | |
| Stage of HIV infection | Symptomatic | 21 | 56.75 |
| Non-symptomatic | 16 | 43.24 | |
| Co-infected with tuberculosis | 04 | 10.81 | |
| Symptoms | Frequency (n) | Percentage (%) | |
|---|---|---|---|
| Psychopathological symptoms | Anxiety | 11 | 29.72 |
| Depression | 05 | 13.51 | |
| Physical symptoms | Weakness | 32 | 86.48 |
| Weight loss | 29 | 78.37 | |
| Lack of energy | 16 | 43.24 | |
| Lack of hunger | 19 | 51.35 | |
| Diarrhea | 04 | 10.81 | |
| Body pain | 27 | 72.97 | |
| Hair loss | 05 | 13.51 | |
| Dizziness | 06 | 16.21 | |
| Respiratory problems | 06 | 16.21 | |
| Difficulty in walking | 24 | 64.86 | |
| Tiredness | 30 | 81.08 | |
| Discharge from genitalia | 04 | 10.81 | |
| Parameter | Unit | Positive Patients | Normal Patients | p-Value |
|---|---|---|---|---|
| HB | g/dL | 10.01 ± 0.77 | 12.51 ± 0.60 | <0.0001 |
| TLC | 103 mm3 | 7.36 ± 1.01 | 8.22 ± 0.78 | 0.001 |
| PLT | 103 mm3 | 183.51 ± 38.13 | 301.05 ± 39.34 | <0.0001 |
| Parameter | Unit | Positive Patients | Normal Patients | p-Value |
|---|---|---|---|---|
| ALT | U/L | 45.51 ± 38.98 | 28.3 ± 3.31 | 0.0548 |
| AST | U/L | 32.35 ± 15.37714 | 28.4 ± 4.29 | 0.2669 |
| Total Bilirubin (T. Bil) | mg/dL | 0.8 ± 0.42961 | 0.71 ± 0.10 | 0.2258 |
| ALP | U/L | 97.05 ± 39.33 | 74.85 ± 8.29 | 0.0160 |
| Albumin (Alb) | g/dL | 4.3 ± 0.15 | 4.0 ± 0.14 | <0.0001 |
| Urea | mg/dL | 38.4 ± 7.13 | 30.8 ± 3.08 | <0.0001 |
| Creatinine | mg/dL | 1.0 ± 0.34 | 0.9 ± 0.14 | 0.3700 |
| Total No of HIV-Positive Patients | HIV-Positive with HB < 10.0 g/dL | HIV-Positive with Hb > 10.0 g/dL |
|---|---|---|
| 37 | 22 (59.4%) | 15 (40.6%) |
| Viral Hepatitis Co-Infection | Number (%) |
|---|---|
| Total HIV patients | 37 (100 %) |
| Overall co-infection | 4 (10.8 %) |
| HBV | 3 (8.1 %) |
| HCV | 1 (2.7 %) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anjum, A.; Rehman, A.u.; Siddique, H.; Rabaan, A.A.; Alhumaid, S.; Garout, M.; Almuthree, S.A.; Halwani, M.A.; Turkistani, S.A.; Qutob, H.; et al. Evaluation of Hematological, Biochemical Profiles and Molecular Detection of Envelope Gene (gp-41) in Human Immunodeficiency Virus (HIV) among Newly Diagnosed Patients. Medicina 2023, 59, 93. https://doi.org/10.3390/medicina59010093
Anjum A, Rehman Au, Siddique H, Rabaan AA, Alhumaid S, Garout M, Almuthree SA, Halwani MA, Turkistani SA, Qutob H, et al. Evaluation of Hematological, Biochemical Profiles and Molecular Detection of Envelope Gene (gp-41) in Human Immunodeficiency Virus (HIV) among Newly Diagnosed Patients. Medicina. 2023; 59(1):93. https://doi.org/10.3390/medicina59010093
Chicago/Turabian StyleAnjum, Asfa, Abaid ur Rehman, Hina Siddique, Ali A. Rabaan, Saad Alhumaid, Mohammed Garout, Souad A. Almuthree, Muhammad A. Halwani, Safaa A. Turkistani, Haitham Qutob, and et al. 2023. "Evaluation of Hematological, Biochemical Profiles and Molecular Detection of Envelope Gene (gp-41) in Human Immunodeficiency Virus (HIV) among Newly Diagnosed Patients" Medicina 59, no. 1: 93. https://doi.org/10.3390/medicina59010093