
Long-Term Outcome of Patients with Stage II and III Muscle-Invasive Urothelial Bladder Cancer after Multimodality Approach. Which Is the Best Option?
 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection Criteria
2.2. Treatment
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saginala, K.; Barsouk, A.; Aluru, J.S.; Rawla, P.; Padala, S.A.; Barsouk, A. Epidemiology of Bladder Cancer. Med. Sci. 2020, 8, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, M.C.S.; Fung, F.D.H.; Leung, C.; Cheung, W.W.L.; Goggins, W.B.; Ng, C.F. The global epidemiology of bladder cancer: A joinpoint regression analysis of its incidence and mortality trends and projection. Sci. Rep. 2018, 8, 1129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freedman, N.D. Association between smoking and risk of bladder cancer among men and women. JAMA 2011, 306, 737. [Google Scholar] [CrossRef]
- Mushtaq, J.; Thurairaja, R.; Nair, R. Bladder Cancer. Surg. Oxf. Int. Ed. 2019, 37, 529–537. [Google Scholar] [CrossRef]
- Mostafa, M.H.; Sheweita, S.A.; O’Connor, P.J. Relationship between schistosomiasis and bladder cancer. Clin. Microbiol. Rev. 1999, 12, 97–111. [Google Scholar] [CrossRef] [Green Version]
- Zaghloul, M.S. Bladder cancer and schistosomiasis. J. Egypt. Natl. Cancer Inst. 2012, 24, 151–159. [Google Scholar] [CrossRef] [Green Version]
- Hein, D.W. Molecular genetics and function of NAT1 and NAT2: Role in aromatic amine metabolism and carcinogenesis. Mutat. Res. Fundam. Mol. Mech. Mutagen. 2002, 506–507, 65–77. [Google Scholar] [CrossRef] [Green Version]
- García-Closas, M.; Malats, N.; Silverman, D.; Dosemeci, M.; Kogevinas, M.; Hein, D.W.; Tardón, A.; Serra, C.; Carrato, A.; García-Closas, R.; et al. NAT2 slow acetylation, GSTM1 null genotype, and risk of bladder cancer: Results from the spanish bladder cancer study and meta-analyses. Lancet 2005, 366, 649–659. [Google Scholar] [CrossRef] [Green Version]
- Gu, J.; Liang, D.; Wang, Y.; Lu, C.; Wu, X. Effects of N-acetyl transferase 1 and 2 polymorphisms on bladder cancer risk in caucasians. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2005, 581, 97–104. [Google Scholar] [CrossRef]
- Rothman, N.; Garcia-Closas, M.; Chatterjee, N.; Malats, N.; Wu, X.; Figueroa, J.D.; Real, F.X.; Van Den Berg, D.; Matullo, G.; Baris, D.; et al. A multi-stage genome-wide association study of bladder cancer identifies multiple susceptibility loci. Nat. Genet. 2010, 42, 978–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riegert-Johnson, D.L.; Gleeson, F.C.; Roberts, M.; Tholen, K.; Youngborg, L.; Bullock, M.; Boardman, L.A. RCesaeanrccher and lhermitte-duclos disease are common in cowden syndrome patients. Hered. Cancer Clin. Pract. 2010, 8, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Post, R.S.; Kiemeney, L.A.; Ligtenberg, M.J.L.; Witjes, J.A.; Hulsbergen-van de Kaa, C.A.; Bodmer, D.; Schaap, L.; Kets, C.M.; van Krieken, J.H.J.M.; Hoogerbrugge, N. Risk of urothelial bladder cancer in lynch syndrome is increased, in particular among MSH2 mutation carriers. J. Med. Genet. 2010, 47, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Phelan, A.; Lopez-Beltran, A.; Montironi, R.; Zhang, S.; Raspollini, M.R.; Cheng, M.; Kaimakliotis, H.Z.; Koch, M.O.; Cheng, L. Inherited forms of bladder cancer: A review of lynch syndrome and other inherited conditions. Future Oncol. 2018, 14, 277–290. [Google Scholar] [CrossRef]
- Cumberbatch, M.G.K.; Jubber, I.; Black, P.C.; Esperto, F.; Figueroa, J.D.; Kamat, A.M.; Kiemeney, L.; Lotan, Y.; Pang, K.; Silverman, D.T.; et al. Epidemiology of bladder cancer: A systematic review and contemporary update of risk factors in 2018. Eur. Urol. 2018, 74, 784–795. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.S.; Boorjian, S.A.; Chou, R.; Clark, P.E.; Daneshmand, S.; Konety, B.R.; Pruthi, R.; Quale, D.Z.; Ritch, C.R.; Seigne, J.D.; et al. Diagnosis and treatment of non-muscle invasive bladder cancer: AUA/SUO guideline. J. Urol. 2016, 196, 1021–1029. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, Y.; Weng, H.; Wang, D.; Han, F.; Huang, Q.; Deng, T.; Wang, X.; Jin, Y. Management of non-muscle-invasive bladder cancer: Quality of clinical practice guidelines and variations in recommendations. BMC Cancer 2019, 19, 1054. [Google Scholar] [CrossRef] [Green Version]
- Metts, M.C.; Metts, J.C.; Milito, S.J.; Thomas, C.R. Bladder cancer: A review of diagnosis and management. J. Natl. Med. Assoc. 2000, 92, 285–294. [Google Scholar]
- Sanli, O.; Dobruch, J.; Knowles, M.A.; Burger, M.; Alemozaffar, M.; Nielsen, M.E.; Lotan, Y. Bladder cancer. Nat. Rev. Dis. Prim. 2017, 3, 17022. [Google Scholar] [CrossRef] [Green Version]
- Alfred Witjes, J.; Lebret, T.; Compérat, E.M.; Cowan, N.C.; De Santis, M.; Bruins, H.M.; Hernández, V.; Espinós, E.L.; Dunn, J.; Rouanne, M.; et al. Updated 2016 EAU guidelines on muscle-invasive and metastatic bladder cancer. Eur. Urol. 2017, 71, 462–475. [Google Scholar] [CrossRef]
- Stein, J.P.; Lieskovsky, G.; Cote, R.; Groshen, S.; Feng, A.-C.; Boyd, S.; Skinner, E.; Bochner, B.; Thangathurai, D.; Mikhail, M.; et al. Radical cystectomy in the treatment of invasive bladder cancer: Long-term results in 1054 patients. JCO 2001, 19, 666–675. [Google Scholar] [CrossRef] [PubMed]
- Gakis, G.; Efstathiou, J.; Lerner, S.P.; Cookson, M.S.; Keegan, K.A.; Guru, K.A.; Shipley, W.U.; Heidenreich, A.; Schoenberg, M.P.; Sagaloswky, A.I.; et al. ICUD-EAU international consultation on bladder cancer 2012: Radical cystectomy and bladder preservation for muscle-invasive urothelial carcinoma of the bladder. Eur. Urol. 2013, 63, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Vashistha, V.; Wang, H.; Mazzone, A.; Liss, M.A.; Svatek, R.S.; Schleicher, M.; Kaushik, D. Radical cystectomy compared to combined modality treatment for muscle-invasive bladder cancer: A systematic review and meta-analysis. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 1002–1020. [Google Scholar] [CrossRef] [PubMed]
- Sherif, A.; Holmberg, L.; Rintala, E.; Mestad, O.; Nilsson, J.; Nilsson, S.; Malmström, P.-U. Neoadjuvant cisplatinum based combination chemotherapy in patients with invasive bladder cancer: A combined analysis of two nordic studies. Eur. Urol. 2004, 45, 297–303. [Google Scholar] [CrossRef]
- Winquist, E.; Kirchner, T.S.; Segal, R.; Chin, J.; Lukka, H.; on behalf of the Genitourinary Cancer Disease Site Group of Cancer Care Ontario Program in Evidence-Based Care Practice Guidelines Initiative. Neoadjuvant Chemotherapy for transitional cell carcinoma of the bladder: A systematic review and meta-analysis. J. Urol. 2004, 171, 561–569. [Google Scholar] [CrossRef]
- Vale, C.L. Neoadjuvant chemotherapy in invasive bladder cancer: Update of a systematic review and meta-analysis of individual patient data. Eur. Urol. 2005, 48, 202–206. [Google Scholar] [CrossRef]
- Powles, T.; Bellmunt, J.; Comperat, E.; De Santis, M.; Huddart, R.; Loriot, Y.; Necchi, A.; Valderrama, B.P.; Ravaud, A.; Shariat, S.F.; et al. Bladder cancer: Esmo clinical practice guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2021, 33, S0923753421048274. [Google Scholar] [CrossRef]
- Kim, H.S.; Jeong, C.W.; Kwak, C.; Kim, H.H.; Ku, J.H. Adjuvant chemotherapy for muscle-invasive bladder cancer: A systematic review and network meta-analysis of randomized clinical trials. Oncotarget 2017, 8, 81204–81214. [Google Scholar] [CrossRef] [Green Version]
- Witjes, J.A.; Compérat, E.; Cowan, N.C.; De Santis, M.; Gakis, G.; Lebret, T.; Ribal, M.J.; Van der Heijden, A.G.; Sherif, A. EAU guidelines on muscle-invasive and metastatic bladder cancer: Summary of the 2013 guidelines. Eur. Urol. 2014, 65, 778–792. [Google Scholar] [CrossRef]
- Meeks, J.J.; Bellmunt, J.; Bochner, B.H.; Clarke, N.W.; Daneshmand, S.; Galsky, M.D.; Hahn, N.M.; Lerner, S.P.; Mason, M.; Powles, T.; et al. A systematic review of neoadjuvant and adjuvant chemotherapy for muscle-invasive bladder cancer. Eur. Urol. 2012, 62, 523–533. [Google Scholar] [CrossRef]
- Sternberg, C.N.; Yagoda, A.; Scher, H.I.; Watson, R.C.; Geller, N.; Herr, H.W.; Morse, M.J.; Sogani, P.C.; Vaughan, E.D.; Bander, N. Methotrexate, vinblastine, doxorubicin, and cisplatin for advanced transitional cell carcinoma of the urothelium. Efficacy and patterns of response and relapse. Cancer 1989, 64, 2448–2458. [Google Scholar] [CrossRef] [PubMed]
- Loehrer, P.J.; Einhorn, L.H.; Elson, P.J.; Crawford, E.D.; Kuebler, P.; Tannock, I.; Raghavan, D.; Stuart-Harris, R.; Sarosdy, M.F.; Lowe, B.A. A Randomized comparison of cisplatin alone or in combination with methotrexate, vinblastine, and doxorubicin in patients with metastatic urothelial carcinoma: A cooperative group study. J. Clin. Oncol. 1992, 10, 1066–1073. [Google Scholar] [CrossRef] [PubMed]
- Logothetis, C.J.; Dexeus, F.H.; Finn, L.; Sella, A.; Amato, R.J.; Ayala, A.G.; Kilbourn, R.G. A prospective randomized trial comparing MVAC and CISCA chemotherapy for patients with metastatic urothelial tumors. J. Clin. Oncol. 1990, 8, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Nadal, R.; Bellmunt, J. Management of metastatic bladder cancer. Cancer Treat. Rev. 2019, 76, 10–21. [Google Scholar] [CrossRef]
- von der Maase, H.; Andersen, L.; Crinò, L.; Weinknecht, S.; Dogliotti, L. Weekly gemcitabine and cisplatin combination therapy in patients with transitional cell carcinoma of the urothelium: A phase II clinical trial. Ann. Oncol. 1999, 10, 1461–1466. [Google Scholar] [CrossRef]
- Moore, M.J.; Winquist, E.W.; Murray, N.; Tannock, I.F.; Huan, S.; Bennett, K.; Walsh, W.; Seymour, L. Gemcitabine plus cisplatin, an active regimen in advanced urothelial cancer: A phase II trial of the National Cancer Institute of Canada Clinical Trials Group. JCO 1999, 17, 2876–2881. [Google Scholar] [CrossRef]
- Kaufman, D.; Raghavan, D.; Carducci, M.; Levine, E.G.; Murphy, B.; Aisner, J.; Kuzel, T.; Nicol, S.; Oh, W.; Stadler, W. Phase II trial of gemcitabine plus cisplatin in patients with metastatic urothelial cancer. JCO 2000, 18, 1921–1927. [Google Scholar] [CrossRef]
- von der Maase, H.; Hansen, S.W.; Roberts, J.T.; Dogliotti, L.; Oliver, T.; Moore, M.J.; Bodrogi, I.; Albers, P.; Knuth, A.; Lippert, C.M.; et al. Gemcitabine and cisplatin versus methotrexate, vinblastine, doxorubicin, and cisplatin in advanced or metastatic bladder cancer: Results of a large, randomized, multinational, multicenter, phase III study. JCO 2000, 18, 3068–3077. [Google Scholar] [CrossRef]
- Von der Maase, H.; Sengelov, L.; Roberts, J.T.; Ricci, S.; Dogliotti, L.; Oliver, T.; Moore, M.J.; Zimmermann, A.; Arning, M. Long-term survival results of a randomized trial comparing gemcitabine plus cisplatin, with methotrexate, vinblastine, doxorubicin, plus cisplatin in patients with bladder cancer. JCO 2005, 23, 4602–4608. [Google Scholar] [CrossRef]
- Sternberg, C.N.; de Mulder, P.; Schornagel, J.H.; Theodore, C.; Fossa, S.D.; van Oosterom, A.T.; Witjes, J.A.; Spina, M.; van Groeningen, C.J.; Duclos, B.; et al. Seven year update of an EORTC phase III trial of high-dose intensity M-VAC chemotherapy and G-CSF versus classic M-VAC in advanced urothelial tract tumours. Eur. J. Cancer 2006, 42, 50–54. [Google Scholar] [CrossRef]
- Bamias, A.; Dafni, U.; Karadimou, A.; Timotheadou, E.; Aravantinos, G.; Psyrri, A.; Xanthakis, I.; Tsiatas, M.; Koutoulidis, V.; Constantinidis, C.; et al. Prospective, open-label, randomized, phase III study of two dose-dense regimens MVAC versus gemcitabine/cisplatin in patients with inoperable, metastatic or relapsed urothelial cancer: A Hellenic cooperative oncology group study (HE 16/03). Ann. Oncol. 2013, 24, 1011–1017. [Google Scholar] [CrossRef] [PubMed]
- Koie, T.; Hatakeyama, S.; Yoneyama, T.; Hashimoto, Y.; Kamimura, N.; Ohyama, C. Uterus-, fallopian tube-, ovary-, and vagina-sparing cystectomy followed by u-shaped ileal neobladder construction for female bladder cancer patients: Oncological and functional outcomes. Urology 2010, 75, 1499–1503. [Google Scholar] [CrossRef] [PubMed]
- Parekh, D.J.; Reis, I.M.; Castle, E.P.; Gonzalgo, M.L.; Woods, M.E.; Svatek, R.S.; Weizer, A.Z.; Konety, B.R.; Tollefson, M.; Krupski, T.L.; et al. Robot-assisted radical cystectomy versus open radical cystectomy in patients with bladder cancer (RAZOR): An open-label, randomised, phase 3, non-inferiority trial. Lancet 2018, 391, 2525–2536. [Google Scholar] [CrossRef] [PubMed]
- Hussain, M.H.A.; Wood, D.P.; Bajorin, D.F.; Bochner, B.H.; Dreicer, R.; Lamm, D.L.; O’Donnell, M.A.; Siefker-Radtke, A.O.; Theodorescu, D.; Dinney, C.P. Bladder cancer: Narrowing the gap between evidence and practice. JCO 2009, 27, 5680–5684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laslo, C.; Stoian, A.; Socea, B.; Paduraru, D.; Bodean, O.; Socea, L.; Neagu, T.; Stanescu, A.; Marcu, D.; Diaconu, C. New oral anticoagulants and their reversal agents. JMMS 2018, 5, 195–201. [Google Scholar] [CrossRef]
- Zheng, Y.; Ye, Y.; Chen, J.; Wei, Z.; Liu, Z.; Yu, K.; Zhang, X. Prevalence and outcomes of transurethral resection versus radical cystectomy for muscle-infiltrating bladder cancer in the United States: A population-based cohort study. Int. J. Surg. 2022, 103, 106693. [Google Scholar] [CrossRef]
- Grossman, H.B.; Natale, R.B.; Tangen, C.M.; Speights, V.O.; Vogelzang, N.J.; Trump, D.L.; deVere White, R.W.; Sarosdy, M.F.; Wood, D.P.; Raghavan, D.; et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N. Engl. J. Med. 2003, 349, 859–866. [Google Scholar] [CrossRef]
- Yin, M.; Joshi, M.; Meijer, R.P.; Glantz, M.; Holder, S.; Harvey, H.A.; Kaag, M.; Fransen van de Putte, E.E.; Horenblas, S.; Drabick, J.J. Neoadjuvant chemotherapy for muscle-invasive bladder cancer: A systematic review and two-step meta-analysis. Oncologist 2016, 21, 708–715. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Yao, Y.; Guan, F.; Sun, L.; Zhang, G. Neoadjuvant chemotherapy for different stages of muscle-invasive bladder cancer: A systematic review and meta-analysis. Dis. Markers 2022, 2022, 8493519. [Google Scholar] [CrossRef]
- Hanna, N.; Trinh, Q.-D.; Seisen, T.; Vetterlein, M.W.; Sammon, J.; Preston, M.A.; Lipsitz, S.R.; Bellmunt, J.; Menon, M.; Choueiri, T.K.; et al. Effectiveness of neoadjuvant chemotherapy for muscle-invasive bladder cancer in the current real world setting in the USA. Eur. Urol. Oncol. 2018, 1, 83–90. [Google Scholar] [CrossRef]
- Grossmann, N.C.; Pradere, B.; D’Andrea, D.; Schuettfort, V.M.; Mori, K.; Rajwa, P.; Quhal, F.; Laukhtina, E.; Katayama, S.; Fankhauser, C.D.; et al. Neoadjuvant chemotherapy in elderly patients with upper tract urothelial cancer: Oncologic outcomes from a multicenter study. Clin. Genitourin. Cancer 2022, 20, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Pfister, C.; Gravis, G.; Fléchon, A.; Soulié, M.; Guy, L.; Laguerre, B.; Mottet, N.; Joly, F.; Allory, Y.; Harter, V.; et al. Randomized phase III trial of dose-dense methotrexate, vinblastine, doxorubicin, and cisplatin, or gemcitabine and cisplatin as perioperative chemotherapy for patients with muscle-invasive bladder cancer. Analysis of the GETUG/AFU V05 VESPER trial secondary endpoints: Chemotherapy toxicity and pathological responses. Eur. Urol. 2021, 79, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Gómez Caamaño, A.; García Vicente, A.M.; Maroto, P.; Rodríguez Antolín, A.; Sanz, J.; Vera González, M.A.; Climent, M.Á.; on behalf of the Spanish Oncology Genitourinary (SOGUG) Multisiciplinary Working Group. Management of localized muscle-invasive bladder cancer from a multidisciplinary perspective: Current position of the Spanish Oncology Genitourinary (SOGUG) Working Group. Curr. Oncol. 2021, 28, 5084–5100. [Google Scholar] [CrossRef]
- Ritch, C.R.; Balise, R.; Prakash, N.S.; Alonzo, D.; Almengo, K.; Alameddine, M.; Venkatramani, V.; Punnen, S.; Parekh, D.J.; Gonzalgo, M.L. Propensity matched comparative analysis of survival following chemoradiation or radical cystectomy for muscle-invasive bladder cancer. BJU Int. 2018, 121, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Cahn, D.B.; Handorf, E.A.; Ghiraldi, E.M.; Ristau, B.T.; Geynisman, D.M.; Churilla, T.M.; Horwitz, E.M.; Sobczak, M.L.; Chen, D.Y.T.; Viterbo, R.; et al. Contemporary use trends and survival outcomes in patients undergoing radical cystectomy or bladder-preservation therapy for muscle-invasive bladder cancer: RC versus BPT in the NCDB. Cancer 2017, 123, 4337–4345. [Google Scholar] [CrossRef] [Green Version]
- Fahmy, O.; Khairul-Asri, M.G.; Schubert, T.; Renninger, M.; Malek, R.; Kübler, H.; Stenzl, A.; Gakis, G. A systematic review and meta-analysis on the oncological long-term outcomes after trimodality therapy and radical cystectomy with or without neoadjuvant chemotherapy for muscle-invasive bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2018, 36, 43–53. [Google Scholar] [CrossRef]
- Shabsigh, A.; Korets, R.; Vora, K.C.; Brooks, C.M.; Cronin, A.M.; Savage, C.; Raj, G.; Bochner, B.H.; Dalbagni, G.; Herr, H.W.; et al. Defining early morbidity of radical cystectomy for patients with bladder cancer using a standardized reporting methodology. Eur. Urol. 2009, 55, 164–176. [Google Scholar] [CrossRef]
- Necchi, A.; Marandino, L.; Raggi, D.; Bandini, M.; Gallina, A.; Moschini, M.; Briganti, A.; Montorsi, F. Is it time to consider eliminating surgery from the treatment of locally advanced bladder cancer? Eur. Urol. 2021, 79, 713–716. [Google Scholar] [CrossRef]
- The European Association of Urology-Young Academic Urologists (EAU-YAU), Urothelial Carcinoma Working Group; Afferi, L.; Zamboni, S.; Karnes, R.J.; Roghmann, F.; Sargos, P.; Montorsi, F.; Briganti, A.; Gallina, A.; Mattei, A.; et al. The impact of treatment modality on survival in patients with clinical node-positive bladder cancer: Results from a multicenter collaboration. World J. Urol. 2021, 39, 443–451. [Google Scholar] [CrossRef]
- Aapro, M.S.; Chrápavá, M.; Curca, R.-O.D.; Gales, L.; Grigorescu, A.C.; Karlínová, B.; Kellnerová, R.; Petru, E.; Pluzanski, A.; Rubach, M.; et al. Assessing the impact of antiemetic guideline compliance on prevention of chemotherapy-induced nausea and vomiting (CINV): Results of the nausea/emesis registry in oncology (NERO). JCO 2020, 38, 12083. [Google Scholar] [CrossRef]
- Aapro, M.; Caprariu, Z.; Chilingirov, P.; Chrápavá, M.; Curca, R.-O.; Gales, L.; Grigorescu, A.C.; Huszno, J.; Karlínová, B.; Kellnerová, R.; et al. Assessing the impact of antiemetic guideline compliance on prevention of chemotherapy-induced nausea and vomiting: Results of the nausea/emesis registry in oncology (NERO). Eur. J. Cancer 2022, 166, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Balar, A.V.; Milowsky, M.I.; O’Donnell, P.H.; Alva, A.S.; Kollmeier, M.; Rose, T.L.; Pitroda, S.; Kaffenberger, S.D.; Rosenberg, J.E.; Francese, K.; et al. Pembrolizumab (Pembro) in combination with gemcitabine (Gem) and concurrent hypofractionated radiation therapy (RT) as bladder sparing treatment for muscle-invasive urothelial cancer of the bladder (MIBC): A multicenter phase 2 trial. JCO 2021, 39, 4504. [Google Scholar] [CrossRef]
- Galsky, M.D.; Daneshmand, S.; Chan, K.G.; Dorff, T.B.; Cetnar, J.P.; Neil, B.O.; D’souza, A.; Mamtani, R.; Kyriakopoulos, C.; Garcia, P.; et al. Phase 2 trial of gemcitabine, cisplatin, plus nivolumab with selective bladder sparing in patients with muscle- invasive bladder cancer (MIBC): HCRN GU 16-257. JCO 2021, 39, 4503. [Google Scholar] [CrossRef]
- Garcia del Muro, X.; Valderrama, B.P.; Medina, A.; Cuellar, M.A.; Etxaniz, O.; Gironés Sarrió, R.; Juan-Fita, M.J.; Ferrer, F.; Miras Rodríguez, I.; Lendínez-Cano, G.; et al. Phase II trial of durvalumab plus tremelimumab with concurrent radiotherapy (RT) in patients (Pts) with localized muscle invasive bladder cancer (MIBC) treated with a selective bladder preservation approach: IMMUNOPRESERVE-SOGUG trial. JCO 2021, 39, 4505. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients’ Characteristics | (n = 231) |
|---|---|
| Female/Male | 41/190 (17.75/82.25%) |
| Urban/rural area | 156/84 (65/35%) |
| Age | 65 ± 10.98 |
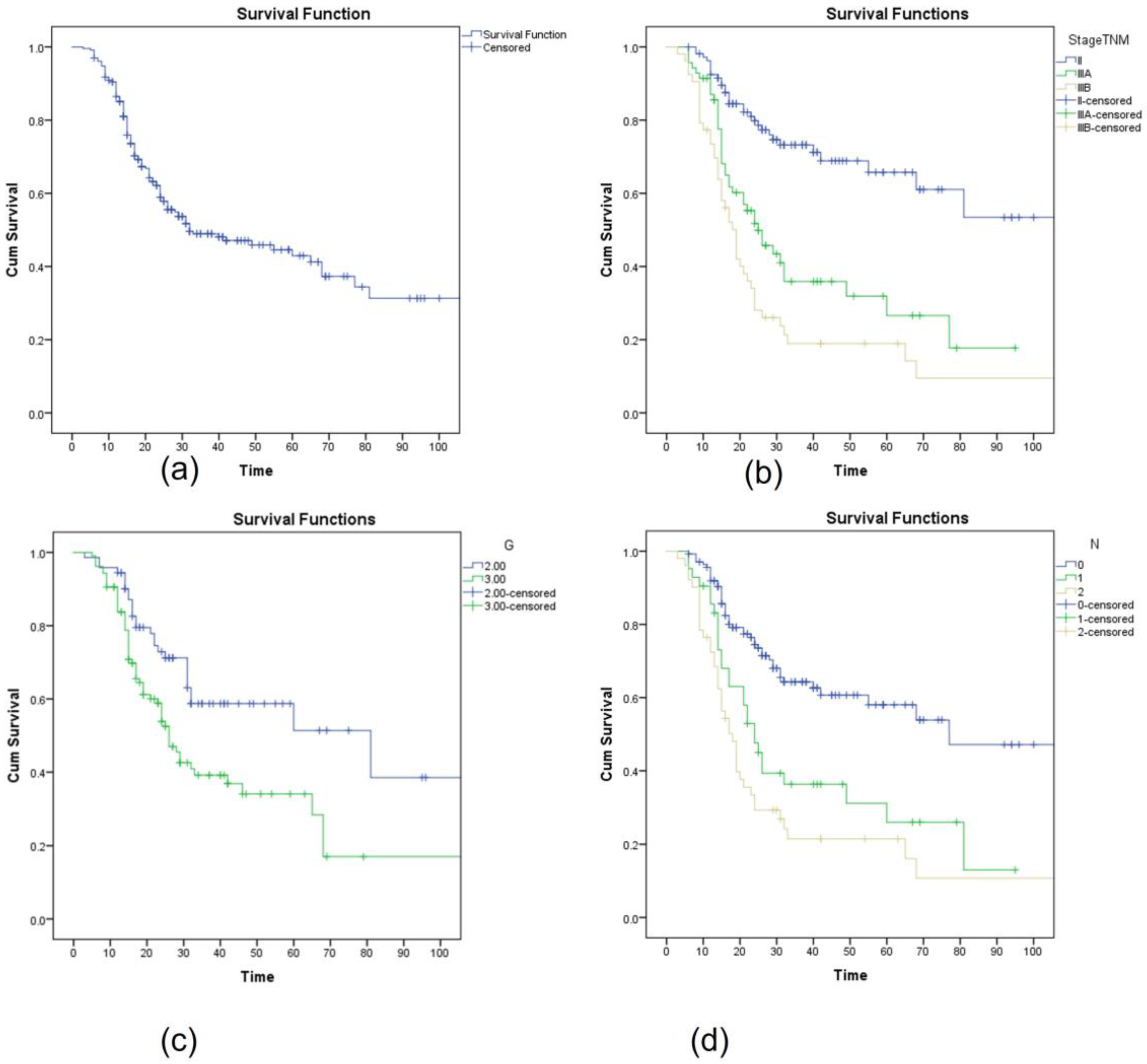
| Staging II/IIIA/IIIB | 108/70/53 (46.8%/30.3%/22.9%) |
| T2a/T2b/T3a/T4a | 25.9%/27.7%/19.5%/19.1%/7.8% |
| N0/N1/N2 | 59.8%/18.2%/22% |
| G2/G3 | 40.3%/59.7% |
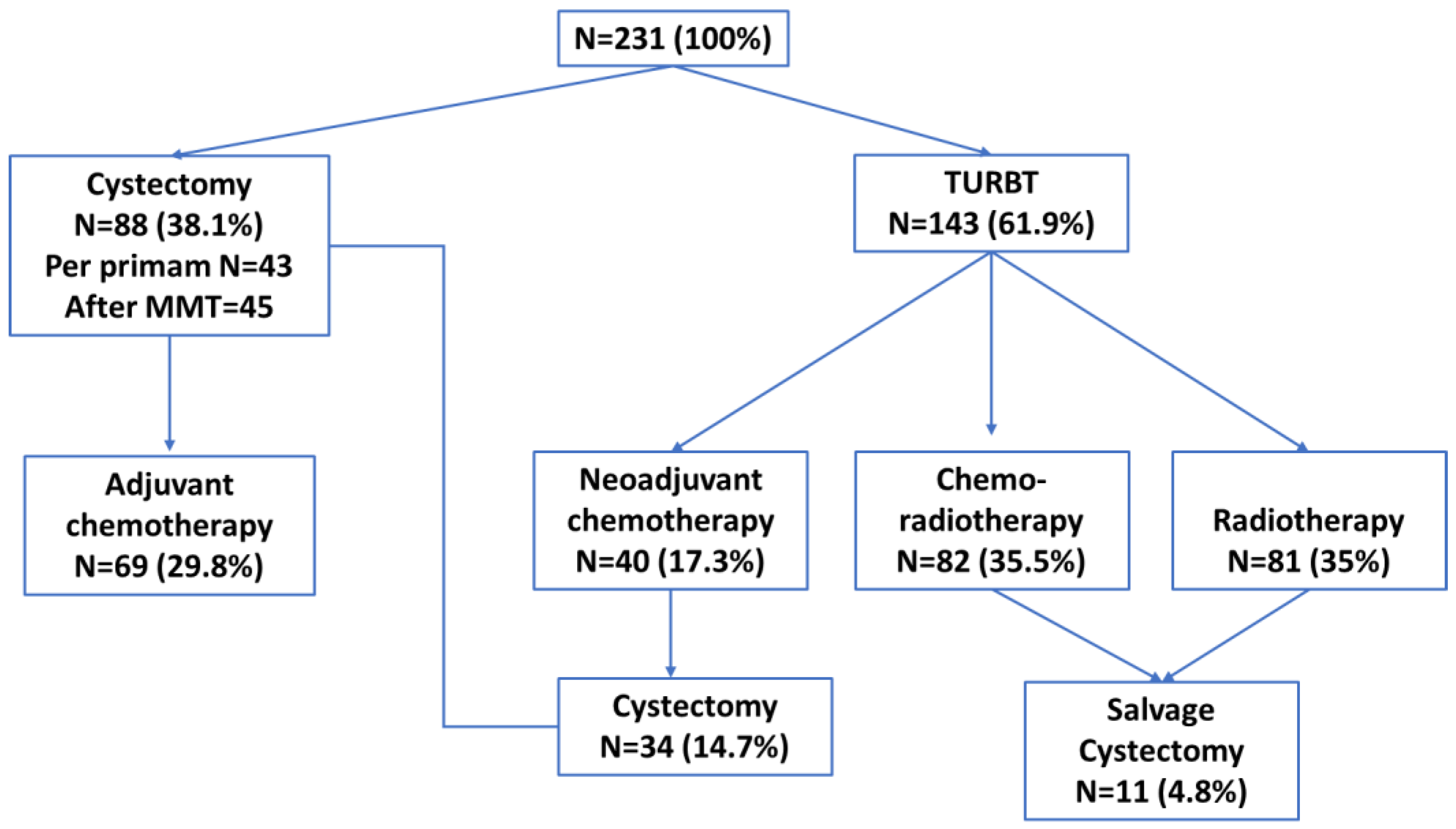
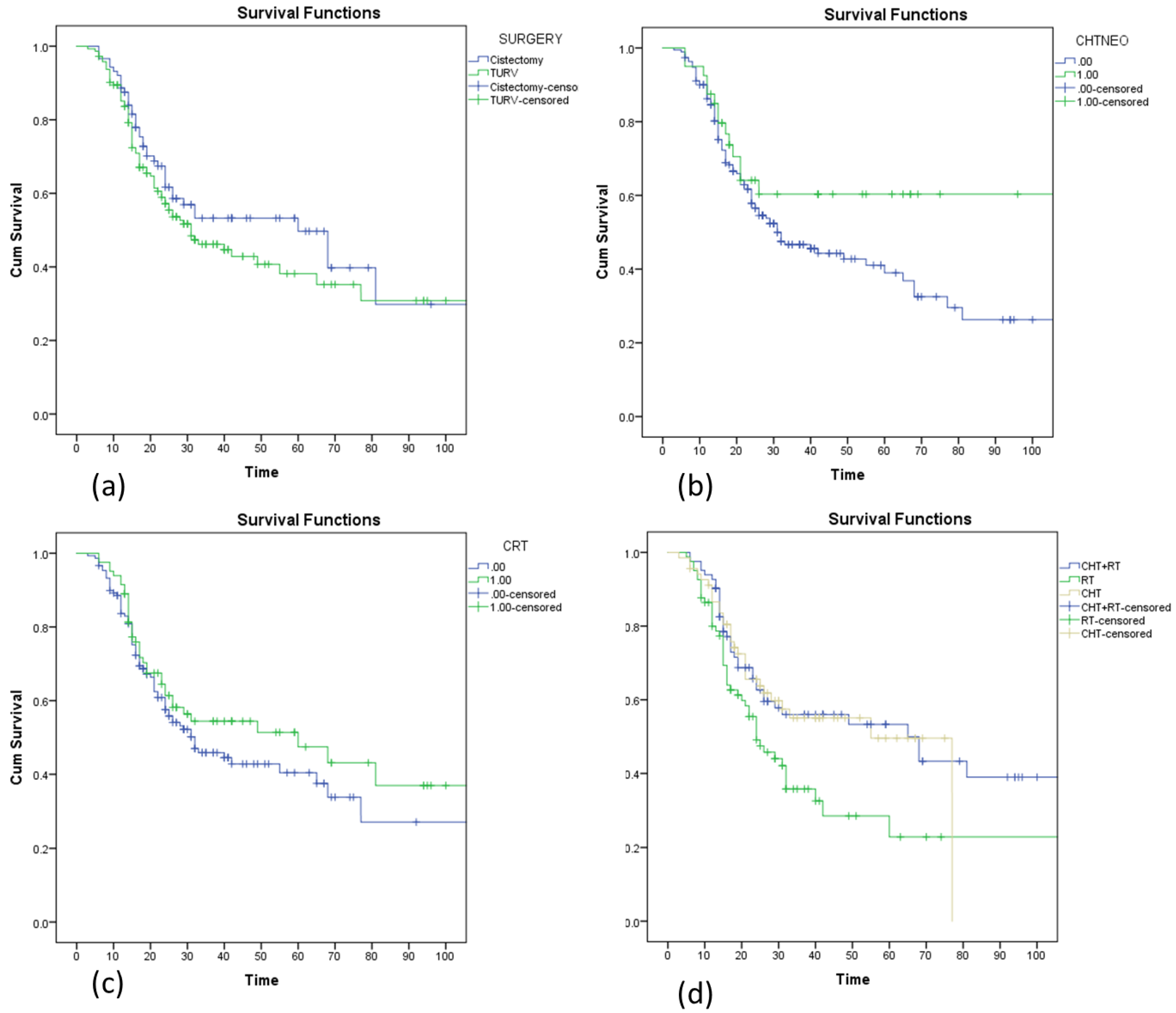
| Surgery (Cystectomy vs. TURBT) | 88/143 (38.1%/61.9%) |
| Neoadjuvant Chemotherapy | 40 (17.3%) |
| Chemotherapy adjuvant | 69 (29.8%) |
| Chemoradiotherapy | 82 (35.5%) |
| Radiotherapy | 81 (35%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trifanescu, O.G.; Gales, L.N.; Paun, M.A.; Motas, N.; Marinescu, S.A.; Virtosu, I.; Trifanescu, R.A.; Gherghe, M.; Bilteanu, L.; Diaconu, C.C.; et al. Long-Term Outcome of Patients with Stage II and III Muscle-Invasive Urothelial Bladder Cancer after Multimodality Approach. Which Is the Best Option? Medicina 2023, 59, 50. https://doi.org/10.3390/medicina59010050
Trifanescu OG, Gales LN, Paun MA, Motas N, Marinescu SA, Virtosu I, Trifanescu RA, Gherghe M, Bilteanu L, Diaconu CC, et al. Long-Term Outcome of Patients with Stage II and III Muscle-Invasive Urothelial Bladder Cancer after Multimodality Approach. Which Is the Best Option? Medicina. 2023; 59(1):50. https://doi.org/10.3390/medicina59010050
Chicago/Turabian StyleTrifanescu, Oana Gabriela, Laurentia Nicoleta Gales, Mihai Andrei Paun, Natalia Motas, Serban Andrei Marinescu, Ion Virtosu, Raluca Alexandra Trifanescu, Mirela Gherghe, Liviu Bilteanu, Camelia Cristina Diaconu, and et al. 2023. "Long-Term Outcome of Patients with Stage II and III Muscle-Invasive Urothelial Bladder Cancer after Multimodality Approach. Which Is the Best Option?" Medicina 59, no. 1: 50. https://doi.org/10.3390/medicina59010050