
The Future of Cardiothoracic Surgical Critical Care Medicine as a Medical Science: A Call to Action
 , , ,
, , ,
Abstract
:1. Introduction
2. Part 1—The Current State of Cardiothoracic Surgical Critical Care Medicine as a Medical Science
- Cardiothoracic Surgical Critical Care Medicine is a discrete subspeciality of a medical science.
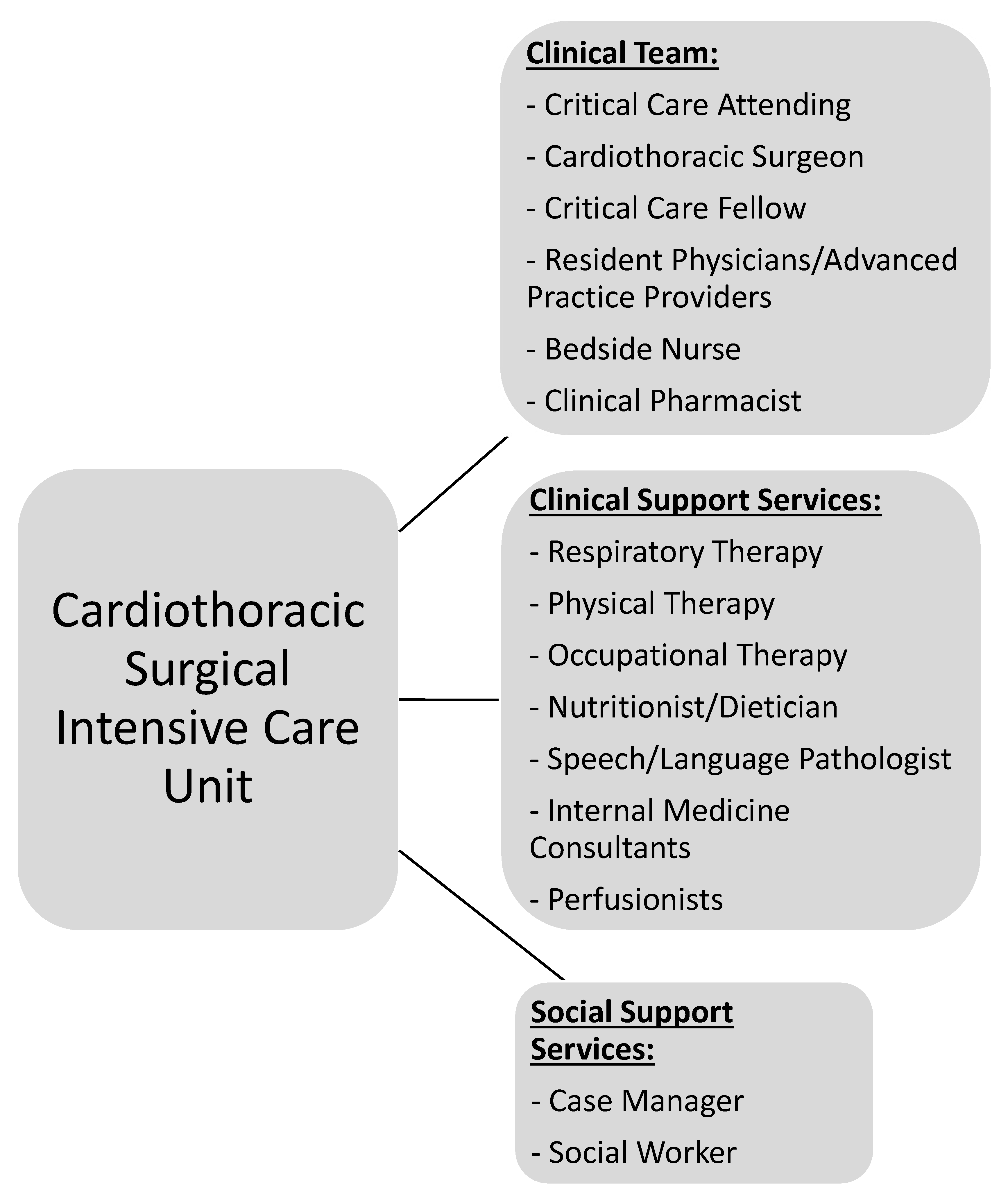
- CT-ICU patient populations are diverse and medically unique.
- Distinct investigations enlisting CT-ICU cohorts are required to answer basic scientific or clinical questions relating to these populations.
- Data acquired from general medical or surgical ICU studies may not provide evidence easily translatable to CT-CCM. Application of such information should be done with caution.
- Wide knowledge gaps exist in many areas of CT-CCM.
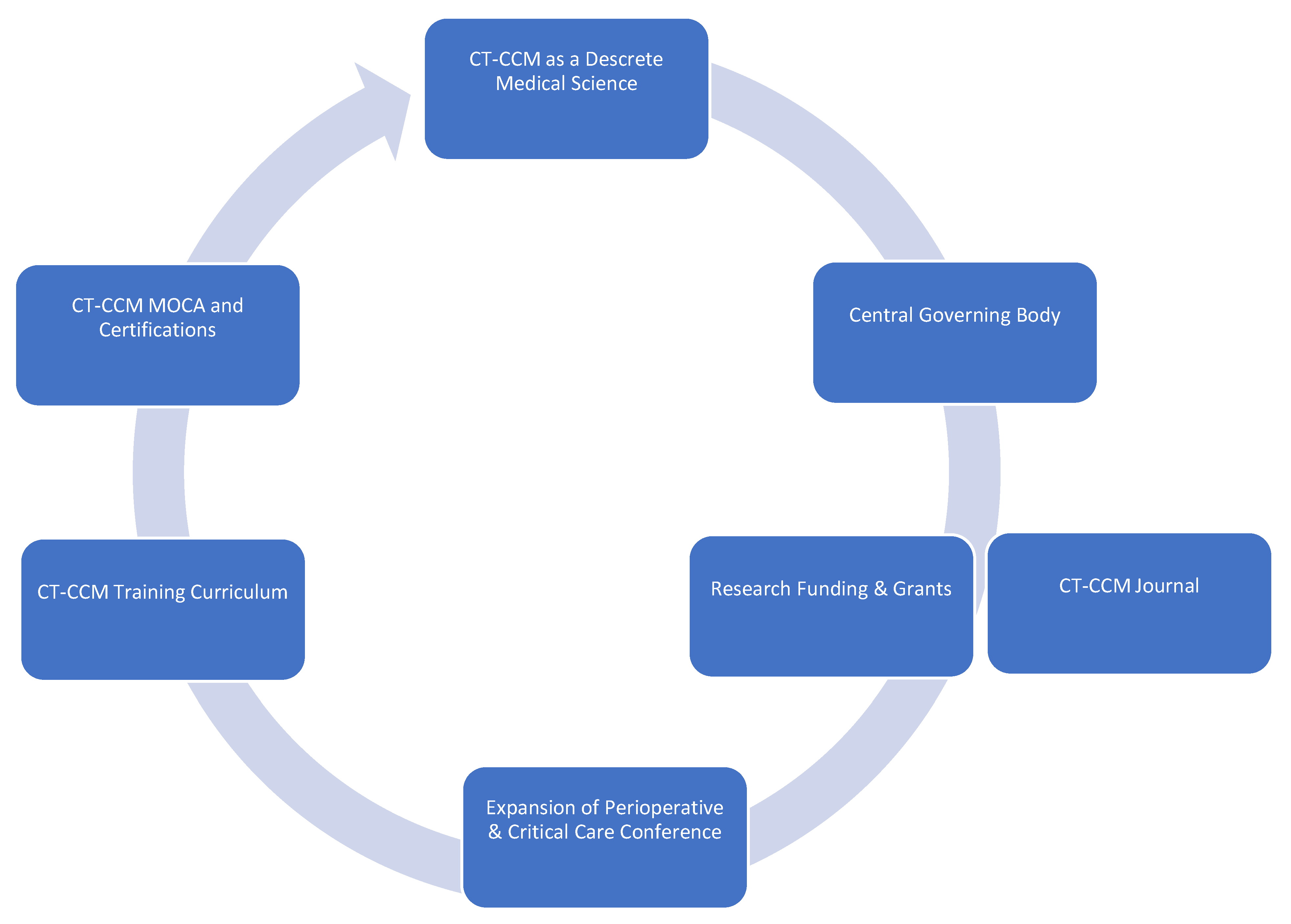
- Formation of a goal setting, centralized governing body, such as CT-CCM specific society.
- Establishment of a scientific journal centered on CT-CCM inquiry.
- Securement of funding and development of grant programs specifically geared towards CT-CCM research.
- Expansion of the Perioperative and Critical Care Conference co-sponsored by the Society of Thoracic Surgeons and the Society of Cardiovascular Anesthesiologists to include other stakeholders, such as Society of Critical Care Medicine, the American Association for Thoracic Surgery, the Society of Critical Care Anesthesiologists, and the American Academy of Cardiovascular Perfusion, and more.
- Establishment of a standardized CT-CCM training curriculum, continuing education, and certification.
3. Part 2 – Selected Gaps in Knowledge and Future Direction of Research
3.1. General Framework and Summary of Important Publications
3.2. Disorder-Specific Considerations
3.2.1. Cardiac Surgery-Associated Acute Kidney Injury (CSA-AKI)
3.2.2. Delirium
3.2.3. Pharmacotherapy
- -
- Therapy for vasoplegia after CBP;
- -
- Vasopressor of choice for hypotension;
- -
- Inotrope of choice based on pathology;
- -
- Utility of a calcium sensitizer;
- -
- Antibiotic therapy duration for hospital-acquired infections in cardiogenic shock;
- -
- Pathology and mechanical support specific anticoagulation regimens and reversal agents;
- -
- Nalaxone and spinal cord protection;
- -
- Multimodal analgesics.
3.2.4. Transfusion and Blood Conservation
3.2.5. Paralysis after Aortic Aneurysm Surgery
- (1)
- What is the ideal small or large animal model for open and endovascular repair of aortic aneurysms, given the variety of anatomical blood supply to the spinal cord across species?
- (2)
- Given the neuro-radiological-anatomical functional paradox, therapeutic treatment for both disease paradigms is different and there is a need for more preclinical trials targeting the specific mechanism behind the grey- and white-matter lesions.
- (3)
- There is a need for randomized controlled trials testing the efficacy of spinal cord drains perioperatively to prevent paralysis.
- (4)
- There is a need for a repository containing the biological fluids of non-paralyzed patients as well as patients who develop paralysis after aortic interventions to gain mechanistic insight which will guide pharmaceutical discovery in this field.
3.2.6. Cardiac Surgical Unit—Advanced Life Support
4. Special Populations
4.1. Extracorporeal Membrane Oxygenation for Respiratory Failure
4.2. Extracorporeal Cardiopulmonary Resuscitation (E-CPR)
4.3. Enhanced Recovery after Surgery (ERAS)
4.4. Lung Transplantation
5. Ethical Considerations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P. Global burden of cardiovascular diseases and risk factors, 1990–2019: Update from the GBD 2019 study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Trogdon, J.G.; Khavjou, O.A.; Butler, J.; Dracup, K.; Ezekowitz, M.D.; Finkelstein, E.A.; Hong, Y.; Johnston, S.C.; Khera, A. Forecasting the future of cardiovascular disease in the United States: A policy statement from the American Heart Association. Circulation 2011, 123, 933–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moffatt-Bruce, S.; Crestanello, J.; Way, D.P.; Williams, T.E., Jr. Providing cardiothoracic services in 2035: Signs of trouble ahead. J. Thorac. Cardiovasc. Surg. 2018, 155, 824–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- John, A.S.; Jackson, J.L.; Moons, P.; Uzark, K.; Mackie, A.S.; Timmins, S.; Lopez, K.N.; Kovacs, A.H.; Gurvitz, M.; American Heart Association Adults With congenital Heart Disease Committee of the Council on Lifelong congenital Heart, D; et al. Advances in Managing Transition to Adulthood for Adolescents With Congenital Heart Disease: A Practical Approach to Transition Program Design: A Scientific Statement From the American Heart Association. J. Am. Heart Assoc. 2022, 11, e025278. [Google Scholar] [CrossRef]
- Kilic, A. The future of left ventricular assist devices. J. Thorac. Dis. 2015, 7, 2188–2193. [Google Scholar] [CrossRef]
- Nguyen, T.C.; Tang, G.H.L.; Nguyen, S.; Forcillo, J.; George, I.; Kaneko, T.; Thourani, V.H.; Bavaria, J.E.; Cheung, A.W.; Reardon, M.J.; et al. The train has left: Can surgeons still get a ticket to treat structural heart disease? J. Thorac. Cardiovasc. Surg. 2019, 157, 2369–2376 e2362. [Google Scholar] [CrossRef] [Green Version]
- Welt, F.G.P. CABG versus PCI-End of the Debate? N. Engl. J. Med. 2022, 386, 185–187. [Google Scholar] [CrossRef]
- Khakban, A.; Sin, D.D.; FitzGerald, J.M.; McManus, B.M.; Ng, R.; Hollander, Z.; Sadatsafavi, M. The projected epidemic of chronic obstructive pulmonary disease hospitalizations over the next 15 years. A population-based perspective. Am. J. Respir. Crit. Care Med. 2017, 195, 287–291. [Google Scholar] [CrossRef]
- Sauleda, J.; Núñez, B.; Sala, E.; Soriano, J.B. Idiopathic pulmonary fibrosis: Epidemiology, natural history, phenotypes. Med. Sci. 2018, 6, 110. [Google Scholar] [CrossRef] [Green Version]
- Nathan, S.D. The future of lung transplantation. Chest 2015, 147, 309–316. [Google Scholar] [CrossRef]
- Azzi, M.; Aboab, J.; Alviset, S.; Ushmorova, D.; Ferreira, L.; Ioos, V.; Memain, N.; Issoufaly, T.; Lermuzeaux, M.; Laine, L.; et al. Extracorporeal CO2 removal in acute exacerbation of COPD unresponsive to non-invasive ventilation. BMJ Open Respir. Res. 2021, 8, e001089. [Google Scholar] [CrossRef] [PubMed]
- Sauer, C.M.; Yuh, D.D.; Bonde, P. Extracorporeal membrane oxygenation use has increased by 433% in adults in the United States from 2006 to 2011. ASAIO J. 2015, 61, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Tollefson, J. Why deforestation and extinctions make pandemics more likely. Nature 2020, 584, 175–177. [Google Scholar] [CrossRef] [PubMed]
- Sleepwalking into the next pandemic. Nat. Med. 2022, 28, 1325. [CrossRef]
- Vetter, T.R. The Next Viral Pandemic: Not a Question of If, But When and How. Anesthesia Analg. 2022, 135, 900–902. [Google Scholar] [CrossRef]
- Katz, N.M. The emerging specialty of cardiothoracic surgical critical care: The leadership role of cardiothoracic surgeons on the multidisciplinary team. J. Thorac. Cardiovasc. Surg. 2007, 134, 1109–1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchman, T.G. A Celebration of the Society of Critical Care Medicine at the Half-Century Mark. Crit. Care Med. 2021, 49, 167–168. [Google Scholar] [CrossRef]
- Bion, J.; Brown, C.; Gomersall, C.; Boulanger, C.; Isherwood, P.; Schulman, D. Society of Critical Care Medicine 50th Anniversary Review Series: Critical Care Education. Crit. Care Med. 2021, 49, 1241–1253. [Google Scholar] [CrossRef]
- Shankar-Hari, M.; Wunsch, H.; Rowan, K.; Singer, M.; Rubenfeld, G.D.; Angus, D.C. Reflections on critical care’s past, present, and future. Crit. Care Med. 2021, 49, 1855–1865. [Google Scholar] [CrossRef]
- Biban, P.; Marlow, N.; Te Pas, A.B.; Fanaroff, A.A.; Jobe, A.H. Advances in Neonatal Critical Care: Pushing at the Boundaries and Connecting to Long-Term Outcomes. Crit. Care Med. 2021, 49, 2003–2016. [Google Scholar] [CrossRef]
- Chang, C.W.; Provencio, J.J.; Shah, S. Neurological Critical Care: The Evolution of Cerebrovascular Critical Care. Crit. Care Med. 2021, 49, 881–900. [Google Scholar] [CrossRef] [PubMed]
- Checchia, P.A.; Brown, K.L.; Wernovsky, G.; Penny, D.J.; Bronicki, R.A. The evolution of pediatric cardiac critical care. Crit. Care Med. 2021, 49, 545–557. [Google Scholar] [CrossRef] [PubMed]
- Pro, C.I.; Yealy, D.M.; Kellum, J.A.; Huang, D.T.; Barnato, A.E.; Weissfeld, L.A.; Pike, F.; Terndrup, T.; Wang, H.E.; Hou, P.C.; et al. A randomized trial of protocol-based care for early septic shock. N. Engl. J. Med. 2014, 370, 1683–1693. [Google Scholar] [CrossRef] [Green Version]
- Mouncey, P.R.; Osborn, T.M.; Power, G.S.; Harrison, D.A.; Sadique, M.Z.; Grieve, R.D.; Jahan, R.; Tan, J.C.; Harvey, S.E.; Bell, D.; et al. Protocolised Management In Sepsis (ProMISe): A multicentre randomised controlled trial of the clinical effectiveness and cost-effectiveness of early, goal-directed, protocolised resuscitation for emerging septic shock. Health Technol. Assess 2015, 19, 1–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandharipande, P.P.; Pun, B.T.; Herr, D.L.; Maze, M.; Girard, T.D.; Miller, R.R.; Shintani, A.K.; Thompson, J.L.; Jackson, J.C.; Deppen, S.A.; et al. Effect of sedation with dexmedetomidine vs lorazepam on acute brain dysfunction in mechanically ventilated patients: The MENDS randomized controlled trial. JAMA 2007, 298, 2644–2653. [Google Scholar] [CrossRef] [Green Version]
- Moss, M.; Ulysse, C.A.; Angus, D.C.; National Heart, L.; Blood Institute, P.C.T.N. Early Neuromuscular Blockade in the Acute Respiratory Distress Syndrome. Reply. N. Engl. J. Med. 2019, 381, 787–788. [Google Scholar] [CrossRef]
- Finfer, S.; Micallef, S.; Hammond, N.; Navarra, L.; Bellomo, R.; Billot, L.; Delaney, A.; Gallagher, M.; Gattas, D.; Li, Q.; et al. Balanced Multielectrolyte Solution versus Saline in Critically Ill Adults. N. Engl. J Med 2022, 386, 815–826. [Google Scholar] [CrossRef]
- Chastre, J.; Wolff, M.; Fagon, J.Y.; Chevret, S.; Thomas, F.; Wermert, D.; Clementi, E.; Gonzalez, J.; Jusserand, D.; Asfar, P.; et al. Comparison of 8 vs 15 days of antibiotic therapy for ventilator-associated pneumonia in adults: A randomized trial. JAMA 2003, 290, 2588–2598. [Google Scholar] [CrossRef]
- Veiga, R.P.; Paiva, J.-A. Pharmacokinetics–pharmacodynamics issues relevant for the clinical use of beta-lactam antibiotics in critically ill patients. Crit. Care 2018, 22, 1–34. [Google Scholar] [CrossRef] [Green Version]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef]
- Raffaeli, G.; Pokorna, P.; Allegaert, K.; Mosca, F.; Cavallaro, G.; Wildschut, E.D.; Tibboel, D. Drug disposition and pharmacotherapy in neonatal ECMO: From fragmented data to integrated knowledge. Front. Pediatr. 2019, 7, 360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, J.A.; Bellomo, R.; Cotta, M.O.; Koch, B.C.; Lyster, H.; Ostermann, M.; Roger, C.; Shekar, K.; Watt, K.; Abdul-Aziz, M.H. Machines that help machines to help patients: Optimising antimicrobial dosing in patients receiving extracorporeal membrane oxygenation and renal replacement therapy using dosing software. Intensive Care Med. 2022, 48, 1338–1351. [Google Scholar] [CrossRef] [PubMed]
- Ha, M.A.; Sieg, A.C. Evaluation of altered drug pharmacokinetics in critically ill adults receiving extracorporeal membrane oxygenation. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2017, 37, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Stöhr, E.J.; McDonnell, B.J. The unique physiology of left ventricular assist device patients–keep your finger on the pulse! Exp. Physiol. 2020, 105, 747–748. [Google Scholar] [CrossRef]
- Hall, S.F.; Athans, V.; Wanek, M.R.; Wang, L.; Estep, J.D.; Williams, B. Evaluation of a hospital-wide vancomycin-dosing nomogram in patients with continuous-flow left ventricular assist devices. Int. J. Artif. Organs 2021, 44, 411–417. [Google Scholar] [CrossRef]
- Jennings, D.L.; Makowski, C.T.; Chambers, R.M.; Lanfear, D.E. Dosing of vancomycin in patients with continuous-flow left ventricular assist devices: A clinical pharmacokinetic analysis. Int. J. Artif. Organs. 2014, 37, 270–274. [Google Scholar] [CrossRef]
- Purohit, S.N.; Cornwell III, W.K.; Pal, J.D.; Lindenfeld, J.; Ambardekar, A.V. Living without a pulse: The vascular implications of continuous-flow left ventricular assist devices. Circ. Heart Fail. 2018, 11, e004670. [Google Scholar] [CrossRef] [PubMed]
- Weiss, S.J. Pro: Cardiothoracic anesthesiologists should run postcardiac surgical intensive care units. J. Cardiothorac. Vasc. Anesth. 2004, 18, 521–524. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, J. Con: Cardiothoracic anesthesiologists should not run postcardiac surgical intensive care units. J. Cardiothorac. Vasc. Anesth. 2004, 18, 525–526. [Google Scholar] [CrossRef]
- Katz, N.M. The evolution of cardiothoracic critical care. J. Thorac. Cardiovasc. Surg. 2011, 141, 3–6. [Google Scholar] [CrossRef]
- Whitson, B.A.; D’Cunha, J. The thoracic surgical intensivist: The best critical care doctor for our thoracic surgical patients. In Seminars in Thoracic and Cardiovascular Surgery; WB Saunders: Philadelphia, PA, USA, 2011; pp. 12–13. [Google Scholar]
- Sherif, H.M. Cardiothoracic surgical critical care: Principles, goals and direction. Int. J. Surg. 2012, 3, 111–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherif, H.M. Developing a curriculum for cardiothoracic surgical critical care: Impetus and goals. J. Thorac. Cardiovasc. Surg. 2012, 143, 804–808. [Google Scholar] [CrossRef] [Green Version]
- Katz, N.M. It is time for certification in cardiothoracic critical care. J. Thorac. Cardiovasc. Surg. 2013, 145, 1446–1447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calhoon, J.H.; Shemin, R.J.; Allen, M.S.; Baumgartner, W.A. The American board of thoracic surgery: Update. Ann. Thorac. Surg. 2013, 95, 1517–1519. [Google Scholar] [CrossRef]
- Baumgartner, W.A.; Calhoon, J.H.; Shemin, R.J.; Allen, M.S. Critical care: American Board of Thoracic Surgery update. J. Thorac. Cardiovasc. Surg. 2013, 145, 1448–1449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherif, H.M.; Cohn, L.H. Certification in cardiothoracic surgical critical care. J. Thorac. Cardiovasc. Surg. 2014, 147, 1454–1455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, N.M. Meeting the expanded challenges of the cardiothoracic intensive care unit. J. Thorac. Cardiovasc. Surg. 2015, 150, 777–778. [Google Scholar] [CrossRef] [Green Version]
- Mehta, Y. Is cardiac anaesthesiologist the best person to look after cardiac critical care? Ann. Card. Anaesth. 2015, 18, 4. [Google Scholar] [CrossRef]
- Sherif, H.M. Cardiothoracic surgical critical care certification: A future of distinction. J. Thorac. Cardiovasc. Surg. 2016, 152, 34–36. [Google Scholar] [CrossRef] [Green Version]
- Sherif, H.M. Cardiothoracic surgical critical care surgeons: Many of the few. J. Thorac. Cardiovasc. Surg. 2016, 152, 642–643. [Google Scholar] [CrossRef]
- Andersen, N.D. Certification in cardiothoracic surgical critical care: A distinction for some or for all? J Thorac Cardiovasc Surg 2016, 152, 37–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitson, B.A. Cardiothoracic surgical critical care is critical to cardiothoracic surgery. J. Thorac. Cardiovasc. Surg. 2016, 152, 938–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, E.G.; D’Cunha, J. Redefining our cardiothoracic surgical intensive care units: Change is good. J. Thorac. Cardiovasc. Surg. 2016, 152, 643–644. [Google Scholar] [CrossRef] [PubMed]
- Andrews, M.C.; Ivascu, N.S.; Pearl, R.G. Cardiothoracic Critical Care: A New Specialty. ASA Monit. 2017, 81, 28–30. [Google Scholar]
- Bartels, K.; Dieleman, S.J. Cardiothoracic Anesthesia and Critical Care: An Ever-Changing (and Evolving) Field. Anesthesiol. Clin. 2019, 37, xv–xvii. [Google Scholar] [CrossRef] [Green Version]
- Shelton, K.T.; Wiener-Kronish, J.P. Evolving role of anesthesiology intensivists in cardiothoracic critical care. Anesthesiology 2020, 133, 1120–1126. [Google Scholar] [CrossRef]
- Savino, J.S.; Hanson, C.W., 3rd; Gardner, T.J. Cardiothoracic intensive care: Operation and administration. Semin. Thorac. Cardiovasc. Surg. 2000, 12, 362–370. [Google Scholar] [CrossRef]
- Stamou, S.C.; Camp, S.L.; Stiegel, R.M.; Reames, M.K.; Skipper, E.; Watts, L.T.; Nussbaum, M.; Robicsek, F.; Lobdell, K.W. Quality improvement program decreases mortality after cardiac surgery. J. Thorac. Cardiovasc. Surg. 2008, 136, 494–499 e498. [Google Scholar] [CrossRef] [Green Version]
- Stamou, S.C.; Camp, S.L.; Reames, M.K.; Skipper, E.; Stiegel, R.M.; Nussbaum, M.; Geller, R.; Robicsek, F.; Lobdell, K.W. Continuous quality improvement program and major morbidity after cardiac surgery. Am. J. Cardiol. 2008, 102, 772–777. [Google Scholar] [CrossRef]
- Camp, S.L.; Stamou, S.C.; Stiegel, R.M.; Reames, M.K.; Skipper, E.R.; Madjarov, J.; Velardo, B.; Geller, H.; Nussbaum, M.; Geller, R.; et al. Quality improvement program increases early tracheal extubation rate and decreases pulmonary complications and resource utilization after cardiac surgery. J. Card. Surg. 2009, 24, 414–423. [Google Scholar] [CrossRef]
- Whitman, G.J.; Haddad, M.; Hirose, H.; Allen, J.G.; Lusardi, M.; Murphy, M.A. Cardiothoracic surgeon management of postoperative cardiac critical care. Arch. Surg. 2011, 146, 1253–1260. [Google Scholar] [CrossRef] [PubMed]
- Kumar, K.; Singal, R.; Manji, R.A.; Zarychanski, R.; Bell, D.D.; Freed, D.H.; Arora, R.C.; Group, C.H.R.i.M.I. The benefits of 24/7 in-house intensivist coverage for prolonged-stay cardiac surgery patients. J. Thorac. Cardiovasc. Surg. 2014, 148, 290–297. e296. [Google Scholar] [CrossRef] [Green Version]
- Benoit, M.A.; Bagshaw, S.M.; Norris, C.M.; Zibdawi, M.; Chin, W.D.; Ross, D.B.; van Diepen, S. Postoperative Complications and Outcomes Associated With a Transition to 24/7 Intensivist Management of Cardiac Surgery Patients. Crit. Care Med. 2017, 45, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Huard, P.; Kalavrouziotis, D.; Lipes, J.; Simon, M.; Tardif, M.-A.; Blackburn, S.; Langevin, S.; Sia, Y.T.; Mohammadi, S. Does the full-time presence of an intensivist lead to better outcomes in the cardiac surgical intensive care unit? J. Thorac. Cardiovasc. Surg. 2020, 159, 1363–1375. e1367. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.Y.; Kang, P.J.; Kim, J.B.; Jung, S.H.; Choo, S.J.; Chung, C.H.; Lee, J.W. Influence of a high-intensity staffing model in a cardiac surgery intensive care unit on postoperative clinical outcomes. J. Thorac. Cardiovasc. Surg. 2020, 159, 1382–1389. [Google Scholar] [CrossRef]
- Arora, R.C.; Chatterjee, S.; Shake, J.G.; Hirose, H.; Engelman, D.T.; Rabin, J.; Firstenberg, M.; Moosdorf, R.G.; Geller, C.M.; Hiebert, B. Survey of contemporary cardiac surgery intensive care unit models in the United States. Ann. Thorac. Surg. 2020, 109, 702–710. [Google Scholar] [CrossRef]
- Lee, L.S.; Clark, A.J.; Namburi, N.; Naum, C.C.; Timsina, L.R.; Corvera, J.S.; Beckman, D.J.; Everett, J.E.; Hess, P.J. The presence of a dedicated cardiac surgical intensive care service impacts clinical outcomes in adult cardiac surgery patients. J. Card. Surg. 2020, 35, 787–793. [Google Scholar] [CrossRef]
- Kennedy-Metz, L.R.; Barbeito, A.; Dias, R.D.; Zenati, M.A. Importance of high-performing teams in the cardiovascular intensive care unit. J. Thorac. Cardiovasc. Surg. 2022, 163, 1096–1104. [Google Scholar] [CrossRef]
- Shaefi, S.; Pannu, A.; Mueller, A.L.; Flynn, B.; Evans, A.; Jabaley, C.S.; Mladinov, D.; Wall, M.; Siddiqui, S.; Douin, D.J. Nationwide Clinical Practice Patterns of Anesthesiology Critical Care Physicians—A Survey to Members of the Society of Critical Care Anesthesiologists. Anesth. Analg. 2022, 10-1213. [Google Scholar] [CrossRef]
- Tung, A. Critical care of the cardiac patient. Anesth. Clin 2013, 31, 421–432. [Google Scholar] [CrossRef]
- Lobdell, K.W.; Haden, D.W.; Mistry, K.P. Cardiothoracic Critical Care. Surg. Clin. N. Am. 2017, 97, 811–834. [Google Scholar] [CrossRef] [PubMed]
- Aneman, A.; Brechot, N.; Brodie, D.; Colreavy, F.; Fraser, J.; Gomersall, C.; McCanny, P.; Moller-Sorensen, P.H.; Takala, J.; Valchanov, K.; et al. Advances in critical care management of patients undergoing cardiac surgery. Intensiv. Care Med. 2018, 44, 799–810. [Google Scholar] [CrossRef] [PubMed]
- Birriel, B.; D’Angelo, K. End-of-Life Care in Cardiothoracic Surgery. Crit. Care Nurs. Clin. N. Am. 2019, 31, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Heiden, B.T.; Tetteh, E.; Robbins, K.J.; Tabak, R.G.; Nava, R.G.; Marklin, G.F.; Kreisel, D.; Meyers, B.F.; Kozower, B.D.; McKay, V.R.; et al. Dissemination and Implementation Science in Cardiothoracic Surgery: A Review and Case Study. Ann. Thorac. Surg. 2022, 114, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Bellomo, R. Cardiac surgery-associated acute kidney injury: Risk factors, pathophysiology and treatment. Nat. Rev. Nephrol. 2017, 13, 697–711. [Google Scholar] [CrossRef]
- Hobson, C.E.; Yavas, S.; Segal, M.S.; Schold, J.D.; Tribble, C.G.; Layon, A.J.; Bihorac, A. Acute kidney injury is associated with increased long-term mortality after cardiothoracic surgery. Circulation 2009, 119, 2444–2453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albright, R.C. Acute kidney injury (AKI) in cardiac surgery. In Cardiopulmonary Bypass, 2nd ed.; Perrino, J.A.C., Falter, F., Ghosh, S., Eds.; Cambridge University Press: Cambridge, UK, 2015; pp. 203–213. [Google Scholar]
- Mukaida, H.; Matsushita, S.; Yamamoto, T.; Minami, Y.; Sato, G.; Asai, T.; Amano, A. Oxygen delivery-guided perfusion for the prevention of acute kidney injury: A randomized controlled trial. J. Thorac. Cardiovasc. Surg. 2021. [Google Scholar] [CrossRef]
- Ranucci, M.; Johnson, I.; Willcox, T.; Baker, R.A.; Boer, C.; Baumann, A.; Justison, G.A.; De Somer, F.; Exton, P.; Agarwal, S. Goal-directed perfusion to reduce acute kidney injury: A randomized trial. J. Thorac. Cardiovasc. Surg. 2018, 156, 1918–1927.e1912. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, S.R.; Kandler, K.; Nielsen, R.V.; Cornelius Jakobsen, P.; Knudsen, N.N.; Ranucci, M.; Christian Nilsson, J.; Ravn, H.B. Duration of critically low oxygen delivery is associated with acute kidney injury after cardiac surgery. Acta Anaesthesiol. Scand. 2019, 63, 1290–1297. [Google Scholar] [CrossRef]
- Carrasco-Serrano, E.; Jorge-Monjas, P.; Muñoz-Moreno, M.F.; Gómez-Sánchez, E.; Priede-Vimbela, J.M.; Bardají-Carrillo, M.; Cubero-Gallego, H.; Tamayo, E.; Ortega-Loubon, C. Impact of Oxygen Delivery on the Development of Acute Kidney Injury in Patients Undergoing Valve Heart Surgery. J. Clin. Med. 2022, 11, 3046. [Google Scholar] [CrossRef]
- Oshita, T.; Hiraoka, A.; Nakajima, K.; Muraki, R.; Arimichi, M.; Chikazawa, G.; Yoshitaka, H.; Sakaguchi, T. A better predictor of acute kidney injury after cardiac surgery: The largest area under the curve below the oxygen delivery threshold during cardiopulmonary bypass. J. Am. Heart Assoc. 2020, 9, e015566. [Google Scholar] [CrossRef] [PubMed]
- Broadwin, M.; Palmeri, M.; Kelting, T.; Groom, R.; Robich, M.; Lucas, F.L.; Kramer, R. Goal Directed Perfusion Is Not Associated with a Decrease in Acute Kidney Injury in Patients Predicted to Be at High Risk for Acute Renal Failure after Cardiac Surgery. J. Extra-Corpor. Technol. 2022, 54, 128–134. [Google Scholar] [PubMed]
- Menting, T.P.; Wever, K.E.; Ozdemir-van Brunschot, D.M.; Van der Vliet, D.J.; Rovers, M.M.; Warle, M.C. Ischaemic preconditioning for the reduction of renal ischaemia reperfusion injury. Cochrane Database Syst. Rev. 2017, 3, Cd010777. [Google Scholar] [CrossRef]
- Krajewski, M.; Raghunathan, K.; Paluszkiewicz, S.; Schermer, C.; Shaw, A. Meta-analysis of high-versus low-chloride content in perioperative and critical care fluid resuscitation. J. Br. Surg. 2015, 102, 24–36. [Google Scholar] [CrossRef] [Green Version]
- Zayed, Y.Z.; Aburahma, A.M.; Barbarawi, M.O.; Hamid, K.; Banifadel, M.; Rashdan, L.; Bachuwa, G.I. Balanced crystalloids versus isotonic saline in critically ill patients: Systematic review and meta-analysis. J. Intensiv. Care 2018, 6, 1–7. [Google Scholar] [CrossRef]
- Otero, T.M.; Aljure, O.D.; Yu, S. Postoperative resuscitation with hypertonic saline or hyperoncotic albumin in patients following cardiac surgery: A review of the literature. J. Card. Surg. 2021, 36, 1040–1049. [Google Scholar] [CrossRef] [PubMed]
- Meersch, M.; Schmidt, C.; Hoffmeier, A.; Van Aken, H.; Wempe, C.; Gerss, J.; Zarbock, A. Prevention of cardiac surgery-associated AKI by implementing the KDIGO guidelines in high risk patients identified by biomarkers: The PrevAKI randomized controlled trial. Intensive Care Med. 2017, 43, 1551–1561. [Google Scholar] [CrossRef] [Green Version]
- Zarbock, A.; Küllmar, M.; Ostermann, M.; Lucchese, G.; Baig, K.; Cennamo, A.; Rajani, R.; McCorkell, S.; Arndt, C.; Wulf, H. Prevention of Cardiac Surgery–Associated Acute Kidney Injury by Implementing the KDIGO Guidelines in High-Risk Patients Identified by Biomarkers: The PrevAKI-Multicenter Randomized Controlled Trial. Anesth. Analg. 2021, 133, 292–302. [Google Scholar] [CrossRef]
- Zarbock, A.; Kellum, J.A.; Schmidt, C.; Van Aken, H.; Wempe, C.; Pavenstädt, H.; Boanta, A.; Gerß, J.; Meersch, M. Effect of early vs delayed initiation of renal replacement therapy on mortality in critically ill patients with acute kidney injury: The ELAIN randomized clinical trial. JAMA 2016, 315, 2190–2199. [Google Scholar] [CrossRef] [Green Version]
- McPherson, J.A.; Wagner, C.E.; Boehm, L.M.; Hall, J.D.; Johnson, D.C.; Miller, L.R.; Burns, K.M.; Thompson, J.L.; Shintani, A.K.; Ely, E.W. Delirium in the cardiovascular intensive care unit: Exploring modifiable risk factors. Crit. Care Med. 2013, 41, 405. [Google Scholar] [CrossRef] [Green Version]
- Sanson, G.; Khlopenyuk, Y.; Milocco, S.; Sartori, M.; Dreas, L.; Fabiani, A. Delirium after cardiac surgery. Incidence, phenotypes, predisposing and precipitating risk factors, and effects. Heart Lung 2018, 47, 408–417. [Google Scholar] [CrossRef] [PubMed]
- Turan, A.; Duncan, A.; Leung, S.; Karimi, N.; Fang, J.; Mao, G.; Hargrave, J.; Gillinov, M.; Trombetta, C.; Ayad, S. Dexmedetomidine for reduction of atrial fibrillation and delirium after cardiac surgery (DECADE): A randomised placebo-controlled trial. Lancet 2020, 396, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, J.R. Acute brain failure: Pathophysiology, diagnosis, management, and sequelae of delirium. Crit. Care Clin. 2017, 33, 461–519. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.E.; Mart, M.F.; Cunningham, C.; Shehabi, Y.; Girard, T.D.; MacLullich, A.M.; Slooter, A.J.; Ely, E. Delirium. Nat. Rev. Dis. Prim. 2020, 6, 1–26. [Google Scholar] [CrossRef]
- Greaves, D.; Psaltis, P.J.; Ross, T.J.; Davis, D.; Smith, A.E.; Boord, M.S.; Keage, H.A. Cognitive outcomes following coronary artery bypass grafting: A systematic review and meta-analysis of 91,829 patients. Int. J. Cardiol. 2019, 289, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Cook, D.J.; Bruggink, S.M. Cerebral morbidity in adult cardiac surgery. In Cardiopulmonary Bypass, 2nd ed.; Perrino, J.A.C., Falter, F., Ghosh, S., Eds.; Cambridge University Press: Cambridge, UK, 2015; pp. 186–202. [Google Scholar]
- Greaves, D.; Psaltis, P.J.; Davis, D.H.; Ross, T.J.; Ghezzi, E.S.; Lampit, A.; Smith, A.E.; Keage, H.A. Risk factors for delirium and cognitive decline following coronary artery bypass grafting surgery: A systematic review and meta-analysis. J. Am. Heart Assoc. 2020, 9, e017275. [Google Scholar] [CrossRef]
- Maldonado, J.R. Delirium pathophysiology: An updated hypothesis of the etiology of acute brain failure. Int. J. Geriatr. Psychiatry 2018, 33, 1428–1457. [Google Scholar] [CrossRef]
- Migirov, A.; Chahar, P.; Maheshwari, K. Postoperative delirium and neurocognitive disorders. Curr. Opin. Crit. Care 2021, 27, 686–693. [Google Scholar] [CrossRef]
- Oh, E.S.; Akeju, O.; Avidan, M.S.; Cunningham, C.; Hayden, K.M.; Jones, R.N.; Khachaturian, A.S.; Khan, B.A.; Marcantonio, E.R.; Needham, D.M.; et al. A roadmap to advance delirium research: Recommendations from the NIDUS Scientific Think Tank. Alzheimers Dement 2020, 16, 726–733. [Google Scholar] [CrossRef]
- Humeidan, M.L.; Reyes, J.-P.C.; Mavarez-Martinez, A.; Roeth, C.; Nguyen, C.M.; Sheridan, E.; Zuleta-Alarcon, A.; Otey, A.; Abdel-Rasoul, M.; Bergese, S.D. Effect of cognitive prehabilitation on the incidence of postoperative delirium among older adults undergoing major noncardiac surgery: The neurobics randomized clinical trial. JAMA Surg. 2021, 156, 148–156. [Google Scholar] [CrossRef]
- O’Gara, B.P.; Mueller, A.; Gasangwa, D.V.I.; Patxot, M.; Shaefi, S.; Khabbaz, K.; Banner-Goodspeed, V.; Pascal-Leone, A.; Marcantonio, E.R.; Subramaniam, B. Prevention of early postoperative decline: A randomized, controlled feasibility trial of perioperative cognitive training. Anesth. Analg. 2020, 130, 586. [Google Scholar] [CrossRef] [PubMed]
- Kelava, M.; Alfirevic, A.; Bustamante, S.; Hargrave, J.; Marciniak, D. Regional anesthesia in cardiac surgery: An overview of fascial plane chest wall blocks. Anesth. Analg. 2020, 131, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, P.; Labaste, F.; Gobin, J.; Marcheix, B.; Minville, V. Bilateral Parasternal Block and Bilateral Erector Spinae Plane Block Reduce Opioid Consumption in During Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2021, 35, 1249–1250. [Google Scholar] [CrossRef]
- Hughes, C.G.; Mailloux, P.T.; Devlin, J.W.; Swan, J.T.; Sanders, R.D.; Anzueto, A.; Jackson, J.C.; Hoskins, A.S.; Pun, B.T.; Orun, O.M. Dexmedetomidine or propofol for sedation in mechanically ventilated adults with sepsis. N. Engl. J. Med. 2021, 384, 1424–1436. [Google Scholar] [CrossRef]
- Smith, W.; Whitlock, E.L. Cardiac surgery, ICU sedation, and delirium: Is dexmedetomidine the silver bullet. Curr. Opin. Anesthsiol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Farrell, R.; Oomen, G.; Carey, P. A technical review of the history, development and performance of the anaesthetic conserving device “AnaConDa” for delivering volatile anaesthetic in intensive and post-operative critical care. J. Clin. Monit. Comput. 2018, 32, 595–604. [Google Scholar] [CrossRef] [Green Version]
- Beitler, J. Efficacy and Safety of Inhaled Isoflurane Delivered Via the Sedaconda ACD-S Compared to Intravenous Propofol for Sedation of Mechanically Ventilated Intensive Care Unit Adult Patients (INSPiRE-ICU2) (INSPiRE-ICU2). Available online: https://clinicaltrials.gov/ct2/show/study/NCT05327296 (accessed on 21 September 2022).
- Meiser, A.; Volk, T.; Wallenborn, J.; Guenther, U.; Becher, T.; Bracht, H.; Schwarzkopf, K.; Knafelj, R.; Faltlhauser, A.; Thal, S.C. Inhaled isoflurane via the anaesthetic conserving device versus propofol for sedation of invasively ventilated patients in intensive care units in Germany and Slovenia: An open-label, phase 3, randomised controlled, non-inferiority trial. Lancet Respir. Med. 2021, 9, 1231–1240. [Google Scholar] [CrossRef] [PubMed]
- Muller, M.; Lefebvre, F.; Harlay, M.-L.; Glady, L.; Becker, G.; Muller, C.; Aberkane, O.; Tawk, M.; Julians, M.; Romoli, A. Impact of intravenous lidocaine on clinical outcomes of patients with ARDS during COVID-19 pandemia (LidoCovid): A structured summary of a study protocol for a randomised controlled trial. Trials 2021, 22, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Gaudino, M.; Benedetto, U.; Fremes, S.; Biondi-Zoccai, G.; Sedrakyan, A.; Puskas, J.D.; Angelini, G.D.; Buxton, B.; Frati, G.; Hare, D.L. Radial-artery or saphenous-vein grafts in coronary-artery bypass surgery. N. Engl. J. Med. 2018, 378, 2069–2077. [Google Scholar] [CrossRef] [Green Version]
- Verma, S.; Szmitko, P.E.; Weisel, R.D.; Bonneau, D.; Latter, D.; Errett, L.; LeClerc, Y.; Fremes, S.E. Should radial arteries be used routinely for coronary artery bypass grafting? Circulation 2004, 110, e40–e46. [Google Scholar] [CrossRef]
- Schwann, T.A.; Gaudino, M.; Baldawi, M.; Tranbaugh, R.; Schwann, A.N.; Habib, R.H. Optimal management of radial artery grafts in CABG: Patient and target vessel selection and anti-spasm therapy. J. Card. Surg. 2018, 33, 205–212. [Google Scholar] [CrossRef]
- Gaudino, M.; Luciani, N.; Nasso, G.; Salica, A.; Canosa, C.; Possati, G. Is postoperative calcium channel blocker therapy needed in patients with radial artery grafts? J. Thorac. Cardiovasc. Surg. 2005, 129, 532–535. [Google Scholar] [CrossRef] [Green Version]
- Bratzler, D.W.; Dellinger, E.P.; Olsen, K.M.; Perl, T.M.; Auwaerter, P.G.; Bolon, M.K.; Fish, D.N.; Napolitano, L.M.; Sawyer, R.G.; Slain, D. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Surg. Infect. 2013, 14, 73–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engelman, R.; Shahian, D.; Shemin, R.; Guy, T.S.; Bratzler, D.; Edwards, F.; Jacobs, M.; Fernando, H.; Bridges, C. The Society of Thoracic Surgeons practice guideline series: Antibiotic prophylaxis in cardiac surgery, part II: Antibiotic choice. Ann. Thorac. Surg. 2007, 83, 1569–1576. [Google Scholar] [CrossRef]
- Silvetti, S.; Landoni, G.; Castagnola, E.; Nuri, H.; Pomé, G.; Moscatelli, A. Antibiotic management for delayed sternal closure following pediatric cardiac surgery: A systematic review of recent literature. J. Cardiothorac. Vasc. Anesth. 2020, 34, 1333–1340. [Google Scholar] [CrossRef] [PubMed]
- Eckardt, J.L.; Wanek, M.R.; Udeh, C.I.; Neuner, E.A.; Fraser, T.G.; Attia, T.; Roselli, E.E. Evaluation of prophylactic antibiotic use for delayed sternal closure after cardiothoracic operation. Ann. Thorac. Surg. 2018, 105, 1365–1369. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Mazzeffi, M.A.; Gammie, J.S.; Banoub, M.; Pazhani, Y.; Herr, D.; Madathil, R.; Pousatis, S.; Bathula, A. Characterization of postoperative infection risk in cardiac surgery patients with delayed sternal closure. J. Cardiothorac. Vasc. Anesth. 2020, 34, 1238–1243. [Google Scholar] [CrossRef] [PubMed]
- Burcham, P.K.; Rozycki, A.J.; Abel, E.E. Considerations for analgosedation and antithrombotic management during extracorporeal life support. Ann. Transl. Med. 2017, 5, 69. [Google Scholar] [CrossRef] [Green Version]
- Shekar, K.; Roberts, J.A.; Mcdonald, C.I.; Fisquet, S.; Barnett, A.G.; Mullany, D.V.; Ghassabian, S.; Wallis, S.C.; Fung, Y.L.; Smith, M.T. Sequestration of drugs in the circuit may lead to therapeutic failure during extracorporeal membrane oxygenation. Crit. Care 2012, 16, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shekar, K.; Roberts, J.A.; Mcdonald, C.I.; Ghassabian, S.; Anstey, C.; Wallis, S.C.; Mullany, D.V.; Fung, Y.L.; Fraser, J.F. Protein-bound drugs are prone to sequestration in the extracorporeal membrane oxygenation circuit: Results from an ex vivo study. Crit. Care 2015, 19, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Kühn, D.; Metz, C.; Seiler, F.; Wehrfritz, H.; Roth, S.; Alqudrah, M.; Becker, A.; Bracht, H.; Wagenpfeil, S.; Hoffmann, M. Antibiotic therapeutic drug monitoring in intensive care patients treated with different modalities of extracorporeal membrane oxygenation (ECMO) and renal replacement therapy: A prospective, observational single-center study. Crit. Care 2020, 24, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; McIntyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit. Care Med. 2021, 49, e1063–e1143. [Google Scholar] [CrossRef] [PubMed]
- Apostolidou, E.; Kolte, D.; Kennedy, K.F.; Beale, C.E.; Abbott, J.D.; Ehsan, A.; Gurm, H.S.; Carson, J.L.; Mamdani, S.; Aronow, H.D. Institutional Red Blood Cell Transfusion Rates Are Correlated Following Endovascular and Surgical Cardiovascular Procedures: Evidence That Local Culture Influences Transfusion Decisions. J. Am. Heart Assoc. 2020, 9, e016232. [Google Scholar] [CrossRef] [PubMed]
- Mazer, C.D.; Whitlock, R.P.; Fergusson, D.A.; Hall, J.; Belley-Cote, E.; Connolly, K.; Khanykin, B.; Gregory, A.J.; de Médicis, É.; McGuinness, S.; et al. Restrictive or Liberal Red-Cell Transfusion for Cardiac Surgery. N. Engl. J. Med. 2017, 377, 2133–2144. [Google Scholar] [CrossRef]
- Mazer, C.D.; Whitlock, R.P.; Fergusson, D.A.; Belley-Cote, E.; Connolly, K.; Khanykin, B.; Gregory, A.J.; de Médicis, É.; Carrier, F.M.; McGuinness, S.; et al. Six-Month Outcomes after Restrictive or Liberal Transfusion for Cardiac Surgery. N. Engl. J. Med. 2018, 379, 1224–1233. [Google Scholar] [CrossRef]
- Ducrocq, G.; Gonzalez-Juanatey, J.R.; Puymirat, E.; Lemesle, G.; Cachanado, M.; Durand-Zaleski, I.; Arnaiz, J.A.; Martínez-Sellés, M.; Silvain, J.; Ariza-Solé, A.; et al. Effect of a Restrictive vs Liberal Blood Transfusion Strategy on Major Cardiovascular Events Among Patients With Acute Myocardial Infarction and Anemia: The REALITY Randomized Clinical Trial. JAMA 2021, 325, 552–560. [Google Scholar] [CrossRef]
- Carson, J.L.; Brooks, M.M.; Abbott, J.D.; Chaitman, B.; Kelsey, S.F.; Triulzi, D.J.; Srinivas, V.; Menegus, M.A.; Marroquin, O.C.; Rao, S.V.; et al. Liberal versus restrictive transfusion thresholds for patients with symptomatic coronary artery disease. Am. Heart J. 2013, 165, 964–971.e961. [Google Scholar] [CrossRef] [Green Version]
- Raphael, J.; Mazer, C.D.; Subramani, S.; Schroeder, A.; Abdalla, M.; Ferreira, R.; Roman, P.E.; Patel, N.; Welsby, I.; Greilich, P.E.; et al. Society of Cardiovascular Anesthesiologists Clinical Practice Improvement Advisory for Management of Perioperative Bleeding and Hemostasis in Cardiac Surgery Patients. Anesth. Analg. 2019, 129, 1209–1221. [Google Scholar] [CrossRef]
- Tanaka, K.A.; Egan, K.; Szlam, F.; Ogawa, S.; Roback, J.D.; Sreeram, G.; Guyton, R.A.; Chen, E.P. Transfusion and hematologic variables after fibrinogen or platelet transfusion in valve replacement surgery: Preliminary data of purified lyophilized human fibrinogen concentrate versus conventional transfusion. Transfusion 2014, 54, 109–118. [Google Scholar] [CrossRef]
- Rahe-Meyer, N.; Solomon, C.; Hanke, A.; Schmidt, D.S.; Knoerzer, D.; Hochleitner, G.; Sørensen, B.; Hagl, C.; Pichlmaier, M. Effects of fibrinogen concentrate as first-line therapy during major aortic replacement surgery: A randomized, placebo-controlled trial. Anesthesiology 2013, 118, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Krachey, E.; Viele, K.; Spinella, P.C.; Steiner, M.E.; Zantek, N.D.; Lewis, R.J. The design of an adaptive clinical trial to evaluate the efficacy of platelets stored at low temperature in surgical patients. J. Trauma Acute Care Surg. 2018, 84, S41–S46. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Zhang, C.; Wang, Y.; Yu, L.; Yan, M. Preoperative Acute Normovolemic Hemodilution for Minimizing Allogeneic Blood Transfusion: A Meta-Analysis. Anesth. Analg. 2015, 121, 1443–1455. [Google Scholar] [CrossRef] [PubMed]
- Barile, L.; Fominskiy, E.; Di Tomasso, N.; Alpìzar Castro, L.E.; Landoni, G.; De Luca, M.; Bignami, E.; Sala, A.; Zangrillo, A.; Monaco, F. Acute Normovolemic Hemodilution Reduces Allogeneic Red Blood Cell Transfusion in Cardiac Surgery: A Systematic Review and Meta-analysis of Randomized Trials. Anesth. Analg. 2017, 124, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Callum, J.; Farkouh, M.E.; Scales, D.C.; Heddle, N.M.; Crowther, M.; Rao, V.; Hucke, H.P.; Carroll, J.; Grewal, D.; Brar, S.; et al. Effect of Fibrinogen Concentrate vs Cryoprecipitate on Blood Component Transfusion After Cardiac Surgery: The FIBRES Randomized Clinical Trial. JAMA 2019, 322, 1966–1976. [Google Scholar] [CrossRef] [PubMed]
- Karkouti, K.; Bartoszko, J.; Grewal, D.; Bingley, C.; Armali, C.; Carroll, J.; Hucke, H.P.; Kron, A.; McCluskey, S.A.; Rao, V.; et al. Comparison of 4-Factor Prothrombin Complex Concentrate With Frozen Plasma for Management of Hemorrhage During and After Cardiac Surgery: A Randomized Pilot Trial. JAMA Netw. Open 2021, 4, e213936. [Google Scholar] [CrossRef] [PubMed]
- Avidan, M.S.; Alcock, E.L.; Da Fonseca, J.; Ponte, J.; Desai, J.B.; Despotis, G.J.; Hunt, B.J. Comparison of structured use of routine laboratory tests or near-patient assessment with clinical judgement in the management of bleeding after cardiac surgery. Br. J. Anaesth. 2004, 92, 178–186. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, E.; Moore, E.E.; Moore, H.B.; Chapman, M.P.; Chin, T.L.; Ghasabyan, A.; Wohlauer, M.V.; Barnett, C.C.; Bensard, D.D.; Biffl, W.L.; et al. Goal-directed Hemostatic Resuscitation of Trauma-induced Coagulopathy: A Pragmatic Randomized Clinical Trial Comparing a Viscoelastic Assay to Conventional Coagulation Assays. Ann Surg. 2016, 263, 1051–1059. [Google Scholar] [CrossRef]
- Baksaas-Aasen, K.; Gall, L.S.; Stensballe, J.; Juffermans, N.P.; Curry, N.; Maegele, M.; Brooks, A.; Rourke, C.; Gillespie, S.; Murphy, J.; et al. Viscoelastic haemostatic assay augmented protocols for major trauma haemorrhage (ITACTIC): A randomized, controlled trial. Intensive Care Med. 2021, 47, 49–59. [Google Scholar] [CrossRef]
- Chowdhury, M.; Shore-Lesserson, L.; Mais, A.M.; Leyvi, G. Thromboelastograph with Platelet Mapping(TM) predicts postoperative chest tube drainage in patients undergoing coronary artery bypass grafting. J. Cardiothorac. Vasc. Anesth. 2014, 28, 217–223. [Google Scholar] [CrossRef]
- de Siqueira, G.M.V.; Pereira-Dos-Santos, F.M.; Silva-Rocha, R.; Guazzaroni, M.E. Nanopore Sequencing Provides Rapid and Reliable Insight Into Microbial Profiles of Intensive Care Units. Front. Public Health 2021, 9, 710985. [Google Scholar] [CrossRef]
- Baccarelli, A.A.; Byun, H.M. Platelet mitochondrial DNA methylation: A potential new marker of cardiovascular disease. Clin. Epigenet. 2015, 7, 44. [Google Scholar] [CrossRef] [PubMed]
- Awad, H.; Tili, E.; Nuovo, G.; Kelani, H.; Ramadan, M.E.; Williams, J.; Binzel, K.; Rajan, J.; Mast, D.; Efanov, A.A.; et al. Endovascular repair and open repair surgery of thoraco-abdominal aortic aneurysms cause drastically different types of spinal cord injury. Sci. Rep. 2021, 11, 7834. [Google Scholar] [CrossRef] [PubMed]
- Aldskogius, H. Animal Models of Spinal Cord Repair; Springer: Berlin/Heidelberg, Germany, 2013; 1 online resource (XII, 336 p. 349 illus., 336 illus. in color). [Google Scholar]
- Fouad, K.; Popovich, P.G.; Kopp, M.A.; Schwab, J.M. The neuroanatomical-functional paradox in spinal cord injury. Nat. Rev. Neurol. 2021, 17, 53–62. [Google Scholar] [CrossRef]
- Dunning, J.; Levine, A.; Ley, J.; Strang, T.; Lizotte Jr, D.E.; Lamarche, Y.; Bartley, T.; Zellinger, M.; Katz, N.; Arora, R.C. The society of thoracic surgeons expert consensus for the resuscitation of patients who arrest after cardiac surgery. Ann. Thorac. Surg. 2017, 103, 1005–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohrer, H.; Gust, R.; Bottiger, B.W. Cardiopulmonary resuscitation after cardiac surgery. J. Cardiothorac. Vasc. Anesth. 1995, 9, 352. [Google Scholar] [CrossRef]
- Kempen, P.M.; Allgood, R. Right ventricular rupture during closed-chest cardiopulmonary resuscitation after pneumonectomy with pericardiotomy: A case report. Crit. Care Med. 1999, 27, 1378–1379. [Google Scholar] [CrossRef]
- Combes, A.; Peek, G.J.; Hajage, D.; Hardy, P.; Abrams, D.; Schmidt, M.; Dechartres, A.; Elbourne, D. ECMO for severe ARDS: Systematic review and individual patient data meta-analysis. Intensiv. Care Med. 2020, 46, 2048–2057. [Google Scholar] [CrossRef]
- Shrestha, D.B.; Sedhai, Y.R.; Budhathoki, P.; Gaire, S.; Subedi, P.; Maharjan, S.; Yuan, M.; Asija, A.; Memon, W. Extracorporeal Membrane Oxygenation (ECMO) Dependent Acute Respiratory Distress Syndrome (ARDS): A Systematic Review and Meta-Analysis. Cureus 2022, 14, e25696. [Google Scholar] [CrossRef]
- Urner, M.; Barnett, A.G.; Bassi, G.L.; Brodie, D.; Dalton, H.J.; Ferguson, N.D.; Heinsar, S.; Hodgson, C.L.; Peek, G.; Shekar, K.; et al. Venovenous extracorporeal membrane oxygenation in patients with acute covid-19 associated respiratory failure: Comparative effectiveness study. BMJ 2022, 377, e068723. [Google Scholar] [CrossRef]
- Akoumianaki, E.; Jonkman, A.; Sklar, M.C.; Georgopoulos, D.; Brochard, L. A rational approach on the use of extracorporeal membrane oxygenation in severe hypoxemia: Advanced technology is not a panacea. Ann. Intensive Care 2021, 11, 107. [Google Scholar] [CrossRef] [PubMed]
- Tonna, J.E.; Abrams, D.; Brodie, D.; Greenwood, J.C.; RUBIO Mateo-Sidron, J.A.; Usman, A.; Fan, E. Management of Adult Patients Supported with Venovenous Extracorporeal Membrane Oxygenation (VV ECMO): Guideline from the Extracorporeal Life Support Organization (ELSO). ASAIO J. 2021, 67, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoué, S.; Guervilly, C.; Da Silva, D.; Zafrani, L.; Tirot, P.; Veber, B.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2018, 378, 1965–1975. [Google Scholar] [CrossRef]
- Schmidt, M.; Bailey, M.; Sheldrake, J.; Hodgson, C.; Aubron, C.; Rycus, P.T.; Scheinkestel, C.; Cooper, D.J.; Brodie, D.; Pellegrino, V.; et al. Predicting survival after extracorporeal membrane oxygenation for severe acute respiratory failure. The Respiratory Extracorporeal Membrane Oxygenation Survival Prediction (RESP) score. Am. J. Respir. Crit. Care Med. 2014, 189, 1374–1382. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.F.; Matthay, M.A.; Luce, J.M.; Flick, M.R. An expanded definition of the adult respiratory distress syndrome. Am. Rev. Respir. Dis. 1988, 138, 720–723. [Google Scholar] [CrossRef]
- Zochios, V.; Parhar, K.; Tunnicliffe, W.; Roscoe, A.; Gao, F. The Right Ventricle in ARDS. Chest 2017, 152, 181–193. [Google Scholar] [CrossRef]
- Amato, M.B.; Meade, M.O.; Slutsky, A.S.; Brochard, L.; Costa, E.L.; Schoenfeld, D.A.; Stewart, T.E.; Briel, M.; Talmor, D.; Mercat, A.; et al. Driving pressure and survival in the acute respiratory distress syndrome. N. Engl. J. Med. 2015, 372, 747–755. [Google Scholar] [CrossRef] [Green Version]
- Bartlett, R.H. Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome: EOLIA and Beyond. Crit. Care Med. 2019, 47, 114–117. [Google Scholar] [CrossRef]
- Steimer, D.A.; Hernandez, O.; Mason, D.P.; Schwartz, G.S. Timing of ECMO Initiation Impacts Survival in Influenza-Associated ARDS. Thorac. Cardiovasc. Surg. 2019, 67, 212–215. [Google Scholar] [CrossRef]
- Olivier, P.-Y.; Ottavy, G.; Hoff, J.; Auchabie, J.; Darreau, C.; Pierrot, M. Prolonged time from intubation to cannulation in VV-ECMO for COVID-19: Does it really matter? Crit. Care 2021, 25, 385. [Google Scholar] [CrossRef]
- Marini, J.J.; Gattinoni, L. Management of COVID-19 Respiratory Distress. JAMA 2020, 323, 2329–2330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrams, D.; Schmidt, M.; Pham, T.; Beitler, J.R.; Fan, E.; Goligher, E.C.; McNamee, J.J.; Patroniti, N.; Wilcox, M.E.; Combes, A.; et al. Mechanical Ventilation for Acute Respiratory Distress Syndrome during Extracorporeal Life Support. Research and Practice. Am. J. Respir. Crit. Care Med. 2020, 201, 514–525. [Google Scholar] [CrossRef] [PubMed]
- Chiu, L.C.; Kao, K.C. Mechanical Ventilation during Extracorporeal Membrane Oxygenation in Acute Respiratory Distress Syndrome: A Narrative Review. J. Clin. Med. 2021, 10, 4953. [Google Scholar] [CrossRef]
- Liu, L.; Liu, F.; Tan, J.; Zhao, L. Bivalirudin versus heparin in adult and pediatric patients with extracorporeal membrane oxygenation therapy: A systematic review and meta-analysis. Pharm. Res 2022, 177, 106089. [Google Scholar] [CrossRef] [PubMed]
- Abruzzo, A.; Gorantla, V.; Thomas, S.E. Venous thromboembolic events in the setting of extracorporeal membrane oxygenation support in adults: A systematic review. Thromb. Res. 2022, 212, 58–71. [Google Scholar] [CrossRef] [PubMed]
- Kalbhenn, J.; Zieger, B. Bleeding During Veno-Venous ECMO: Prevention and Treatment. Front. Med. 2022, 9, 879579. [Google Scholar] [CrossRef]
- McMichael, A.B.V.; Ryerson, L.M.; Ratano, D.; Fan, E.; Faraoni, D.; Annich, G.M. 2021 ELSO Adult and Pediatric Anticoagulation Guidelines. ASAIO J. 2022, 68, 303–310. [Google Scholar] [CrossRef]
- Fina, D.; Matteucci, M.; Jiritano, F.; Meani, P.; Kowalewski, M.; Ballotta, A.; Ranucci, M.; Lorusso, R. Extracorporeal membrane oxygenation without systemic anticoagulation: A case-series in challenging conditions. J. Thorac. Dis. 2020, 12, 2113–2119. [Google Scholar] [CrossRef]
- Pavlushkov, E.; Berman, M.; Valchanov, K. Cannulation techniques for extracorporeal life support. Ann. Transl. Med. 2017, 5, 70. [Google Scholar] [CrossRef] [Green Version]
- Shah, A.; Dave, S.; Goerlich, C.E.; Kaczorowski, D.J. Hybrid and parallel extracorporeal membrane oxygenation circuits. JTCVS Tech. 2021, 8, 77–85. [Google Scholar] [CrossRef]
- Bartlett, R.H. ECMO: The next ten years. Egypt. J. Crit. Care Med. 2016, 4, 7–10. [Google Scholar] [CrossRef] [Green Version]
- Giraud, R.; Banfi, C.; Assouline, B.; De Charrière, A.; Cecconi, M.; Bendjelid, K. The use of extracorporeal CO2 removal in acute respiratory failure. Ann. Intensiv. Care 2021, 11, 43. [Google Scholar] [CrossRef]
- Chen, H.; Yu, R.G.; Yin, N.N.; Zhou, J.X. Combination of extracorporeal membrane oxygenation and continuous renal replacement therapy in critically ill patients: A systematic review. Crit. Care 2014, 18, 675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, M.; Franchineau, G.; Combes, A. Recent advances in venovenous extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. Curr. Opin. Crit. Care 2019, 25, 71–76. [Google Scholar] [CrossRef]
- Smith, A.; Morgan, C.; Ledot, S.; Doyle, J.; Xu, T.; Shedden, L.; Passariello, M.; Patel, B.; Doyle, A.M.; Price, S.; et al. Veno-venous extracorporeal membrane oxygenation for the acute respiratory distress syndrome: A bridge too far? Acta Cardiol. 2021, 76, 455–458. [Google Scholar] [CrossRef]
- Dennis, M.; Lal, S.; Forrest, P.; Nichol, A.; Lamhaut, L.; Totaro, R.J.; Burns, B.; Sandroni, C. In-Depth Extracorporeal Cardiopulmonary Resuscitation in Adult Out-of-Hospital Cardiac Arrest. J. Am. Heart Assoc. 2020, 9, e016521. [Google Scholar] [CrossRef]
- Richardson, A.S.C.; Tonna, J.E.; Nanjayya, V.; Nixon, P.; Abrams, D.C.; Raman, L.; Bernard, S.; Finney, S.J.; Grunau, B.; Youngquist, S.T.; et al. Extracorporeal Cardiopulmonary Resuscitation in Adults. Interim Guideline Consensus Statement From the Extracorporeal Life Support Organization. ASAIO J. 2021, 67, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Belohlavek, J.; Smalcova, J.; Rob, D.; Franek, O.; Smid, O.; Pokorna, M.; Horák, J.; Mrazek, V.; Kovarnik, T.; Zemanek, D.; et al. Effect of Intra-arrest Transport, Extracorporeal Cardiopulmonary Resuscitation, and Immediate Invasive Assessment and Treatment on Functional Neurologic Outcome in Refractory Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA 2022, 327, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Massion, P.B.; Joachim, S.; Morimont, P.; Dulière, G.L.; Betz, R.; Benoit, A.; Amabili, P.; Lagny, M.; Lizin, J.; Massaro, A.; et al. Feasibility of extracorporeal membrane oxygenation cardiopulmonary resuscitation by low volume centers in Belgium. J. Am. Coll. Emerg. Physicians Open 2021, 2, e12484. [Google Scholar] [CrossRef]
- Addison, D.; Cheng, E.; Forrest, P.; Livingstone, A.; Morton, R.L.; Dennis, M. Cost-effectiveness of extracorporeal cardiopulmonary resuscitation for adult out-of-hospital cardiac arrest: A systematic review. Resuscitation 2022, 178, 19–25. [Google Scholar] [CrossRef]
- Yannopoulos, D.; Bartos, J.; Raveendran, G.; Walser, E.; Connett, J.; Murray, T.A.; Collins, G.; Zhang, L.; Kalra, R.; Kosmopoulos, M.; et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): A phase 2, single centre, open-label, randomised controlled trial. Lancet 2020, 396, 1807–1816. [Google Scholar] [CrossRef]
- Ruggeri, L.; Franco, A.; Alba, A.C.; Lembo, R.; Frassoni, S.; Scandroglio, A.M.; Calabrò, M.G.; Zangrillo, A.; Pappalardo, F. Coagulation Derangements in Patients With Refractory Cardiac Arrest Treated With Extracorporeal Cardiopulmonary Resuscitation. J. Cardiothorac. Vasc. Anesth. 2019, 33, 1877–1882. [Google Scholar] [CrossRef] [PubMed]
- Mene-Afejuku, T.O.; Moisa, E.-A.; Akinlonu, A.; Dumancas, C.; Veranyan, S.; Perez, J.A.; Salazar, P.; Chaudhari, S.; Pekler, G.; Mushiyev, S. The relevance of serum albumin among elderly patients with acute decompensated heart failure. J. Geriatr. Cardiol. 2019, 16, 522. [Google Scholar]
- Gebauer, A.; Petersen, J.; Konertz, J.; Brickwedel, J.; Schulte-Uentrop, L.; Reichenspurner, H.; Girdauskas, E. Enhanced Recovery After Cardiac Surgery: Where Do We Stand? Curr. Anesthesiol. Rep. 2021, 11, 501–506. [Google Scholar] [CrossRef]
- Engelman, D.T.; Ali, W.B.; Williams, J.B.; Perrault, L.P.; Reddy, V.S.; Arora, R.C.; Roselli, E.E.; Khoynezhad, A.; Gerdisch, M.; Levy, J.H. Guidelines for perioperative care in cardiac surgery: Enhanced recovery after surgery society recommendations. JAMA Surg. 2019, 154, 755–766. [Google Scholar] [CrossRef]
- Acinapura, A.; Jacobowitz, I.; Kramer, M.; Adkins, M.; Zisbrod, Z.; Cunningham Jr, J. Demographic changes in coronary artery bypass surgery and its effect on mortality and morbidity. Eur. J. Cardio-Thorac. Surg. 1990, 4, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Chandramouli, C.; Allocco, B.; Gong, E.; Lam, C.S.; Yan, L.L. Women’s participation in cardiovascular clinical trials from 2010 to 2017. Circulation 2020, 141, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Coelho, P.N.; Miranda, L.M.; Barros, P.M.; Fragata, J.I. Quality of life after elective cardiac surgery in elderly patients. Interact. CardioVascular Thorac. Surg. 2019, 28, 199–205. [Google Scholar] [CrossRef] [Green Version]
- Kudsk, K.A.; Tolley, E.A.; DeWitt, R.C.; Janu, P.G.; Blackwell, A.P.; Yeary, S.; King, B.K. Preoperative albumin and surgical site identify surgical risk for major postoperative complications. J. Parenter. Enter. Nutr. 2003, 27, 1–9. [Google Scholar] [CrossRef]
- Lee, E.H.; Kim, W.J.; Kim, J.Y.; Chin, J.H.; Choi, D.K.; Sim, J.Y.; Choo, S.J.; Chung, C.H.; Lee, J.W.; Choi, I.C. Effect of exogenous albumin on the incidence of postoperative acute kidney injury in patients undergoing off-pump coronary artery bypass surgery with a preoperative albumin level of less than 4.0 g/dl. Anesthesiology 2016, 124, 1001–1011. [Google Scholar] [CrossRef]
- Karas, P.L.; Goh, S.L.; Dhital, K. Is low serum albumin associated with postoperative complications in patients undergoing cardiac surgery? Interact. Cardiovasc. Thorac. Surg. 2015, 21, 777–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waitzberg, D.L.; Saito, H.; Plank, L.D.; Jamieson, G.G.; Jagannath, P.; Hwang, T.-L.; Mijares, J.M.; Bihari, D. Postsurgical infections are reduced with specialized nutrition support. World J. Surg. 2006, 30, 1592–1604. [Google Scholar] [CrossRef] [PubMed]
- Barberan-Garcia, A.; Ubré, M.; Roca, J.; Lacy, A.M.; Burgos, F.; Risco, R.; Momblán, D.; Balust, J.; Blanco, I.; Martínez-Pallí, G. Personalised prehabilitation in high-risk patients undergoing elective major abdominal surgery: A randomized blinded controlled trial. Ann. Surg. 2018, 267, 50–56. [Google Scholar] [CrossRef]
- Li, C.; Carli, F.; Lee, L.; Charlebois, P.; Stein, B.; Liberman, A.S.; Kaneva, P.; Augustin, B.; Wongyingsinn, M.; Gamsa, A. Impact of a trimodal prehabilitation program on functional recovery after colorectal cancer surgery: A pilot study. Surg. Endosc. 2013, 27, 1072–1082. [Google Scholar] [CrossRef] [PubMed]
- Gillis, C.; Li, C.; Lee, L.; Awasthi, R.; Augustin, B.; Gamsa, A.; Liberman, A.S.; Stein, B.; Charlebois, P.; Feldman, L.S. Prehabilitation versus rehabilitation: A randomized control trial in patients undergoing colorectal resection for cancer. Anesthesiology 2014, 121, 937–947. [Google Scholar] [CrossRef]
- Oravec, N.; Arora, R.C.; Bjorklund, B.; Gregora, A.; Monnin, C.; Duhamel, T.A.; Kent, D.E.; Schultz, A.S.; Chudyk, A.M. Expanding enhanced recovery protocols for cardiac surgery to include the patient voice: A scoping review protocol. Syst. Rev. 2021, 10, 1–10. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N. Heart disease and stroke statistics—2021 update: A report from the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar]
- Hessian, R.; Jabagi, H.; Ngu, J.M.; Rubens, F.D. Coronary surgery in women and the challenges we face. Can. J. Cardiol. 2018, 34, 413–421. [Google Scholar] [CrossRef]
- Cho, L.; Kibbe, M.R.; Bakaeen, F.; Aggarwal, N.R.; Davis, M.B.; Karmalou, T.; Lawton, J.S.; Ouzounian, M.; Preventza, O.; Russo, A.M. Cardiac surgery in women in the current era: What are the gaps in care? Circulation 2021, 144, 1172–1185. [Google Scholar] [CrossRef]
- Volgman, A.S.; Bairey Merz, C.N.; Aggarwal, N.T.; Bittner, V.; Bunch, T.J.; Gorelick, P.B.; Maki, P.; Patel, H.N.; Poppas, A.; Ruskin, J. Sex differences in cardiovascular disease and cognitive impairment: Another health disparity for women? J. Am. Heart Assoc. 2019, 8, e013154. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Kappetein, A.P.; Sabik, J.F.; Pocock, S.J.; Morice, M.-C.; Puskas, J.; Kandzari, D.E.; Karmpaliotis, D.; Brown III, W.M.; Lembo, N.J. Five-year outcomes after PCI or CABG for left main coronary disease. N. Engl. J. Med. 2019, 381, 1820–1830. [Google Scholar] [CrossRef] [PubMed]
- Hayanga, A.J.; Aboagye, J.K.; Hayanga, H.E.; Morrell, M.; Huffman, L.; Shigemura, N.; Bhama, J.K.; Bermudez, C.A. Contemporary analysis of early outcomes after lung transplantation in the elderly using a national registry. J. Heart Lung Transplant. 2015, 34, 182–188. [Google Scholar] [CrossRef]
- Benissan-Messan, D.Z.; Ganapathi, A.M.; Guo, M.; Henn, M.C.; Keller, B.C.; Howsare, M.; Rosenheck, J.P.; Kirkby, S.E.; Mokadam, N.A.; Nunley, D. Lung transplantation in the septuagenarian can be successfully performed though long-term results impacted by diseases of aging. Clin. Transplant. 2022, 36, e14593. [Google Scholar] [CrossRef] [PubMed]
- Hammad, S.; Ravichandran, B.; Madathil, R.; McLaughlin, P.; Cipriano, S.; Timofte, I. Outcomes Associated with Septuagenarian Lung Transplant Recipients. J. Heart Lung Transplant. 2020, 39, S320–S321. [Google Scholar] [CrossRef]
- Flume, P.A.; Egan, T.M.; Westerman, J.H.; Paradowski, L.J.; Yankaskas, J.R.; Detterbeck, F.C.; Mill, M.R. Lung transplantation for mechanically ventilated patients. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 1994, 13, 15–21; discussion 22. [Google Scholar]
- Vermeijden, J.W.; Zijlstra, J.G.; Erasmus, M.E.; van der Bij, W.; Verschuuren, E.A. Lung transplantation for ventilator-dependent respiratory failure. J. Heart Lung Transplant. 2009, 28, 347–351. [Google Scholar] [CrossRef]
- Bartz, R.R.; Love, R.B.; Leverson, G.E.; Will, L.R.; Welter, D.L.; Meyer, K.C. Pre-transplant mechanical ventilation and outcome in patients with cystic fibrosis. J. Heart Lung Transplant. 2003, 22, 433–438. [Google Scholar] [CrossRef]
- Bharat, A.; Machuca, T.N.; Querrey, M.; Kurihara, C.; Garza-Castillon Jr, R.; Kim, S.; Manerikar, A.; Pelaez, A.; Pipkin, M.; Shahmohammadi, A. Early outcomes after lung transplantation for severe COVID-19: A series of the first consecutive cases from four countries. Lancet Respir. Med. 2021, 9, 487–497. [Google Scholar] [CrossRef]
- Magnusson, J.M.; Silverborn, M.; Broome, M.; Riise, G.C.; Dellgren, G. Long-term Extracorporeal Membrane Oxygenation Bridge to Lung Transplantation After COVID-19. Ann. Thorac. Surg. 2022, 113, e5–e8. [Google Scholar] [CrossRef]
- Mohanka, M.R.; Joerns, J.; Lawrence, A.; Bollineni, S.; Kaza, V.; Cheruku, S.; Leveno, M.; Chen, C.; Terada, L.S.; Kershaw, C.D. ECMO Long Haulers: A Distinct Phenotype of COVID-19–Associated ARDS with Implications for Lung Transplant Candidacy. Transplantation 2022, 106, e202–e211. [Google Scholar] [CrossRef]
- Harano, T.; Chan, E.G.; Furukawa, M.; Dos Santos, P.R.; Morrell, M.R.; Sappington, P.L.; Sanchez, P.G. Oxygenated right ventricular assist device with a percutaneous dual-lumen cannula as a bridge to lung transplantation. J. Thorac. Dis. 2022, 14, 832–840. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.K.; D’Ovidio, F.; Garan, A.R.; Brodie, D.; Sonett, J.R.; Farr, M.A.; Arcasoy, S.M.; Takeda, K. Minimally invasive central venoarterial extracorporeal membrane oxygenation for long-term ambulatory support as a bridge to heart–lung transplant. J. Artif. Organs 2020, 23, 394–396. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.G.; Pak, C.; Oh, D.K.; Kim, H.C.; Kang, P.J.; Lee, G.D.; Choi, S.H.; Jung, S.-H.; Hong, S.-B. Right ventricular assist device with extracorporeal membrane oxygenation for bridging right ventricular heart failure to lung transplantation: A single-center case series and literature review. J. Cardiothorac. Vasc. Anesth. 2021. [Google Scholar] [CrossRef] [PubMed]
- Kinaschuk, K.; Bozso, S.J.; Halloran, K.; Kapasi, A.; Jackson, K.; Nagendran, J. Mechanical circulatory support as a bridge to lung transplantation: A single Canadian institution review. Can. Respir. J. 2017, 2017, 5947978. [Google Scholar] [CrossRef] [Green Version]
- Rana, R.; Ghandehari, S.; Falk, J.; Simsir, S.; Ghaly, A.; Cheng, W.; Cohen, J.; Peng, A.; Czer, L.; Schwarz, E. Successful combined heart-bilateral lung-kidney transplantation from a same donor to treat severe hypertrophic cardiomyopathy with secondary pulmonary hypertension and renal failure: Case report and review of the literature. Transplant. Proc. 2011, 43, 2820–2826. [Google Scholar] [CrossRef]
- Borro, J.M.; Rama, P.; Rey, T.; Fernández-Rivera, C. Long-term success of combined kidney–lung transplantation in a patient with cystic fibrosis. Arch. Bronconeumol. 2013, 49, 272–274. [Google Scholar] [CrossRef]
- Mason, D.P.; Boffa, D.J.; Murthy, S.C.; Gildea, T.R.; Budev, M.M.; Mehta, A.C.; McNeill, A.M.; Smedira, N.G.; Feng, J.; Rice, T.W. Extended use of extracorporeal membrane oxygenation after lung transplantation. J. Thorac. Cardiovasc. Surg. 2006, 132, 954–960. [Google Scholar] [CrossRef] [Green Version]
- Boffini, M.; Simonato, E.; Ricci, D.; Scalini, F.; Marro, M.; Pidello, S.; Attisani, M.; Solidoro, P.; Lausi, P.O.; Fanelli, V. Extracorporeal membrane oxygenation after lung transplantation: Risk factors and outcomes analysis. Ann. Cardiothorac. Surg. 2019, 8, 54. [Google Scholar] [CrossRef] [Green Version]
- Mason, D.P.; Solovera-Rozas, M.; Feng, J.; Rajeswaran, J.; Thuita, L.; Murthy, S.C.; Budev, M.M.; Mehta, A.C.; Haug III, M.; McNeill, A.M. Dialysis after lung transplantation: Prevalence, risk factors and outcome. J. Heart Lung Transplant. 2007, 26, 1155–1162. [Google Scholar] [CrossRef]
- Crothers, E.; Kennedy, D.S.; Emmanuel, S.; Molan, N.; Scott, S.; Rogers, K.; Glanville, A.R.; Ntoumenopoulos, G. Incidence of early diaphragmatic dysfunction after lung transplantation: Results of a prospective observational study. Clin. Transplant. 2021, 35, e14409. [Google Scholar] [CrossRef]
- Diamond, J.M.; Lee, J.C.; Kawut, S.M.; Shah, R.J.; Localio, A.R.; Bellamy, S.L.; Lederer, D.J.; Cantu, E.; Kohl, B.A.; Lama, V.N.; et al. Clinical risk factors for primary graft dysfunction after lung transplantation. Am. J. Respir. Crit. Care Med. 2013, 187, 527–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yserbyt, J.; Dooms, C.; Vos, R.; Dupont, L.J.; Van Raemdonck, D.E.; Verleden, G.M. Anastomotic airway complications after lung transplantation: Risk factors, treatment modalities and outcome—A single-centre experience. Eur. J. Cardio-Thorac. Surg. 2016, 49, e1–e8. [Google Scholar] [CrossRef] [Green Version]
- Santacruz, J.F.; Mehta, A.C. Airway complications and management after lung transplantation: Ischemia, dehiscence, and stenosis. Proc. Am. Thorac. Soc. 2009, 6, 79–93. [Google Scholar] [CrossRef] [PubMed]
- Tang, A.; Siddiqui, H.U.; Thuita, L.; Rappaport, J.; Bribriesco, A.C.; McCurry, K.R.; Yun, J.; Unai, S.; Budev, M.; Murthy, S.C. Natural history of pleural complications after lung transplantation. Ann. Thorac. Surg. 2021, 111, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, J.; Roldan, J.; Roman, A.; Bravo, C.; Monforte, V.; Pallissa, E.; Gic, I.; Sole, J.; Morell, F. Acute and chronic pleural complications in lung transplantation. J. Heart Lung Transplant. 2003, 22, 1217–1225. [Google Scholar] [CrossRef] [PubMed]
- Hodgin, K.E.; Nordon-Craft, A.; McFann, K.K.; Mealer, M.L.; Moss, M. Physical therapy utilization in intensive care units: Results from a national survey. Crit. Care Med. 2009, 37, 561. [Google Scholar] [CrossRef]
- Taito, S.; Shime, N.; Ota, K.; Yasuda, H. Early mobilization of mechanically ventilated patients in the intensive care unit. J. Intensive Care 2016, 4, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Singbartl, K.; Murugan, R.; Kaynar, A.; Crippen, D.; Tisherman, S.; Shutterly, K.; Stuart, S.; Simmons, R.; Darby, J. Intensivist-led management of brain-dead donors is associated with an increase in organ recovery for transplantation. Am. J. Transplant. 2011, 11, 1517–1521. [Google Scholar] [CrossRef]
- Rosendale, J.D.; Kauffman, H.M.; McBride, M.A.; Chabalewski, F.L.; Zaroff, J.G.; Garrity, E.R.; Delmonico, F.L.; Rosengard, B.R. Aggressive pharmacologic donor management results in more transplanted organs1. Transplantation 2003, 75, 482–487. [Google Scholar] [CrossRef]
- Turco, L.M.; Glorsky, S.L.; Winfield, R.D. Hormone replacement therapy in brain-dead organ donors: A comprehensive review with an emphasis on traumatic brain injury. J. Trauma Acute Care Surg. 2019, 86, 702–709. [Google Scholar] [CrossRef]
- Kotloff, R.M.; Blosser, S.; Fulda, G.J.; Malinoski, D.; Ahya, V.N.; Angel, L.; Byrnes, M.C.; DeVita, M.A.; Grissom, T.E.; Halpern, S.D. Management of the potential organ donor in the ICU: Society of critical care medicine/American college of chest physicians/association of organ procurement organizations consensus statement. Crit. Care Med. 2015, 43, 1291–1325. [Google Scholar] [CrossRef] [PubMed]
- Tramm, R.; Ilic, D.; Murphy, K.; Sheldrake, J.; Pellegrino, V.; Hodgson, C. Experience and needs of family members of patients treated with extracorporeal membrane oxygenation. J. Clin. Nurs. 2017, 26, 1657–1668. [Google Scholar] [CrossRef] [PubMed]
- Akkermans, A.; Lamerichs, J.; Schultz, M.; Cherpanath, T.; van Woensel, J.; van Heerde, M.; van Kaam, A.; van de Loo, M.; Stiggelbout, A.; Smets, E. How doctors actually (do not) involve families in decisions to continue or discontinue life-sustaining treatment in neonatal, pediatric, and adult intensive care: A qualitative study. Palliat. Med. 2021, 35, 1865–1877. [Google Scholar] [CrossRef] [PubMed]
- Mercadante, S.; Gregoretti, C.; Cortegiani, A. Palliative care in intensive care units: Why, where, what, who, when, how. BMC Anesthesiol. 2018, 18, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarze, M.L.; Brasel, K.J.; Mosenthal, A.C. Beyond 30-day mortality: Aligning surgical quality with outcomes that patients value. JAMA Surg. 2014, 149, 631–632. [Google Scholar] [CrossRef] [PubMed]
- Walkey, A.J.; Barnato, A.E.; Wiener, R.S.; Nallamothu, B.K. Accounting for patient preferences regarding life-sustaining treatment in evaluations of medical effectiveness and quality. Am. J. Respir. Crit. Care Med. 2017, 196, 958–963. [Google Scholar] [CrossRef]
- Turnbull, A.E.; Sahetya, S.K.; Biddison, E.; Hartog, C.S.; Rubenfeld, G.D.; Benoit, D.D.; Guidet, B.; Gerritsen, R.T.; Tonelli, M.R.; Curtis, J.R. Competing and conflicting interests in the care of critically ill patients. Intensive Care Med. 2018, 44, 1628–1637. [Google Scholar] [CrossRef]
- Kayser, J.B.; Kaplan, L.J. Conflict management in the ICU. Crit. Care Med. 2020, 48, 1349–1357. [Google Scholar] [CrossRef]
- Spijkers, A.S.; Akkermans, A.; Smets, E.; Schultz, M.J.; Cherpanath, T.G.; van Woensel, J.; van Heerde, M.; van Kaam, A.H.; van de Loo, M.; Willems, D.L. How doctors manage conflicts with families of critically ill patients during conversations about end-of-life decisions in neonatal, pediatric, and adult intensive care. Intensive Care Med. 2022, 48, 910–922. [Google Scholar] [CrossRef]
- Kim, J.M.; Godfrey, S.; O’Neill, D.; Sinha, S.S.; Kochar, A.; Kapur, N.K.; Katz, J.N.; Warraich, H.J. Integrating palliative care into the modern cardiac intensive care unit: A review. Eur. Heart J. Acute Cardiovasc. Care 2022, 11, 442–449. [Google Scholar] [CrossRef]
- Yefimova, M.; Aslakson, R.A.; Yang, L.; Garcia, A.; Boothroyd, D.; Gale, R.C.; Giannitrapani, K.; Morris, A.M.; Johanning, J.M.; Shreve, S. Palliative care and end-of-life outcomes following high-risk surgery. JAMA Surg. 2020, 155, 138–146. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Historical |
| Failure of unification of critical care medicine in the 1980s, creating specialty silos |
| Operating room economic incentives superior to critical care, limiting interest in subspecializing |
| Balanced Budget Act of 1997 caping residency spots, reducing pool of candidates available to pursue critical care |
| Underappreciation of importance of postoperative care on overall outcomes |
| Absence of recognition of CT-CCM as a unique medical science |
| Surgical dominance of the field |
| Scientific |
| Shortage of scientists and mentors specializing in CT-CCM specific research |
| Deficiency in well-established animal models specific to CT-ICU patient populations |
| Scarcity in hypothesis-generating research specific to CT-CCM |
| Paucity of CT-CCM translational research |
| Lack of dissemination and implementation research |
| Systemic/Organizational |
| Absence of a central governing body responsible for promotion and cultivation of CT-CCM |
| Knowledge silos resulting from wide array of subspecialties and societies involved in CT-CCM |
| Clinical and administrative workload limiting individual’s bandwidth for research projects |
| Educational |
| Absence of well-defined, unified CT-CCM training curriculum |
| Shortage of mentorship promoting CT-CCM inquiry |
| Deficiency in quality improvement training |
| Financial |
| Prohibitive costs of creating cardiopulmonary bypass animal models |
| Insufficient funding of CT-CCM specific research |
| Title | Authors | Year | Journal | Findings |
|---|---|---|---|---|
| Cardiothoracic Surgical Critical Care Leadership and Training | ||||
| Pro: Cardiothoracic Anesthesiologists Should Run Postcardiac Surgical Intensive Care Units [38] | Weiss, S.J. | 2004 | JCVA | Pro and con debate about cardiothoracic anesthesiologists running CT-ICUs |
| Con: Cardiothoracic Anesthesiologists Should Not Run Postcardiac Surgical Intensive Care Units [39] | Ramsey, J. | 2004 | JCVA | Pro and con debate about cardiothoracic anesthesiologists running CT-ICUs |
| The Emerging Specialty of Cardiothoracic Surgical Critical Care: The Leadership Role of Cardiothoracic Surgeons on the Multidisciplinary Team [16] | Katz, N.M. | 2007 | JTCVS | Editorial on CT-CCM as a new specialty and importance of CT surgeons in CT-ICU leadership |
| The Evolution of Cardiothoracic Critical Care [40] | Katz, N.M. | 2011 | JTCVS | Editorial on importance of CT-CCM and leading role of a CT surgeon |
| The Thoracic Surgical Intensivist: The Best Critical Care Doctor for Our Thoracic Surgical Patients [41] | Whitson, B.A. and D’Cunha, J. | 2011 | Semin. Thorac. Cardiovasc. Surg. | Editorial on recognition of critical care as integral component of cardiac surgery with surgeons as leaders |
| Cardiothoracic Surgical Critical Care: Principles, Goals and Direction [42] | Sherif, H.M. | 2012 | Int. J. Surg. | Editorial on CT-CCM as distinct discipline, its basic principles, and future directions |
| Developing A Curriculum for Cardiothoracic Surgical Critical Care: Impetus and Goals [43] | Sherif, H.M. | 2012 | JTCVS | Sample curriculum for surgical CT-CCM training |
| It Is Time for Certification In Cardiothoracic Critical Care [44] | Katz, N.M. | 2013 | JTCVS | Editorial calling for unique cardiothoracic surgical certification in critical care |
| The American Board of Thoracic Surgery: Update [45] | Calhoon, J.H. | 2013 | JTCVS | Official ABTS statement regarding all the certifications provided by the board. Additionally, addresses critical care pathways for surgeons and decline development of ABTS CCM certification. |
| Critical Care: American Board of Thoracic Surgery Update [46] | Baumgartner, W.A. et al. | 2013 | JTCVS | ABTS explaining its reasoning why it will not support certification in cardiothoracic critical care, written in response to Katz, 2013. |
| Certification in Cardiothoracic Surgical Critical Care [47] | Sherif, H.M., and L.H. Cohn | 2014 | JTCVS | Editorial in response to Katz 2013 supporting development of certification by ABTS |
| Meeting The Expanded Challenges of The Cardiothoracic Intensive Care Unit [48] | Katz, N.M. | 2015 | JTCVS | Editorial addressing changes in organization and technology in CT-ICUs, with surgical leadership at the forefront. |
| Is Cardiac Anaesthesiologist The Best Person to Look After Cardiac Critical Care? [49] | Mehta, Y. | 2015 | Ann. Card. Anaesth. | Editorial outlining benefits of cardiac anesthesiologists as CT-ICU intensivists |
| Cardiothoracic Surgical Critical Care Certification: A Future Of Distinction [50] | Sherif, H.M. | 2016 | JTCVS | Editorial highlighting the need for CT-CCM certification within cardiothoracic surgery board |
| Cardiothoracic Surgical Critical Care Surgeons: Many Of The Few [51] | Sherif, H.M. | 2016 | JTCVS | Letter to the editor in repones to N.D. Andersen, highlighting benefits of establishing CT-CCM as a subspecialty |
| Certification in Cardiothoracic Surgical Critical Care: A Distinction For Some Or For All? [52] | Andersen, N.D. | 2016 | JTCVS | Call for CT-CCM surgical certification process attainable by current and future surgeons |
| Cardiothoracic Surgical Critical Care Is Critical to Cardiothoracic Surgery [53] | Whitson, B.A. | 2016 | JTCVS | Letter to the editor highlighting importance of critical care to practice of cardiothoracic surgery |
| Redifining Our Cardiothoracic Surgical Intensive Care Units: Change is Good [54] | Chan, E.G., and J. D’Cunha | 2016 | JTCVS | Letter to the editor from ABTS members outline steps needed to advance the process of CT-CCM certification |
| Cardiothoracic Critical Care: A New Specialty [55] | Andrews, M.C. et al. | 2017 | ASA Monitor | Editorial highlighting benefits of dual training in cardiothoracic and critical care anesthesiology |
| Cardiothoracic Anesthesia and Critical Care: An Ever-Changing (and Evolving) Field [56] | Bartels, K., and S.J. Dieleman | 2019 | Anes. Clin. | Preface to Special Issue of the journal centered on cardiothoracic anesthesia and critical care |
| Evolving role of anesthesiology intensivists in cardiothoracic critical care [57] | Shelton, K.T. and J.P. Wiener-Kronish, | 2020 | Anesthesiology | Editorial highlighting cardiothoracic surgical intensivists at Massachusetts General Hospital |
| Staffing of CT-ICUs | ||||
| Cardiothoracic Intensive Care: Operation and Administration [58] | Savino, J.S. et al. | 2000 | Semin. Thorac. Cardiovasc. Surg. | Review article outlining emerging importance of physicians dedicated to postoperative medical and surgical management. |
| Quality Improvement Program Decreases Mortality After Cardiac Surgery [59] | Stamou, S.C. et al. | 2008 | JTCVS | Single center retrospective analysis of outcomes before and after implementation of quality improvement program, including multidisciplinary rounding involving intensivists. Implementation was associated with a decrease in mortality. |
| Continous Quality Improvement Program and Major Morbidity After Cardiac Surgery [60] | Stamou, S.C. et al. | 2008 | Am. J. Cardiol. | Single-center retrospective analysis of continuous quality improvement program including multidisciplinary involvement and intensivists rounding decreased sepsis and cardiac tamponade |
| Quality Improvement Program Increases Early Tracheal Extubation Rate and Decreases Pulmonary Complications and Resource Utilization After Cardiac Surgery | Camp S.L. et al. | 2009 | J. Card. Surg. | Single center retrospective analysis of quality improvement program implementation increased early extubation and decreased pulmonary complications |
| Impact of 24-Hour In-House Intensivists on a Dedicated Cardiac Surgery Intensive Care Unit [61] | Kumar, K. et al. | 2009 | Ann. Thorac. Surg. | Retrospective cohort study of 24 h in-house intensivist coverage associated with reduced hospital stay, transfusions, and requirement for mechanical ventilation |
| Cardiothoracic Surgeon Management of Postoperative Cardiac Critical Care [62] | Withman, G.J. et al. | 2011 | JAMA | Retrospective data review of patients after cardiac surgery where noncardiac intensivists were changed to cardiothoracic surgeons showing decreased length of stay and decrease drug cost |
| The Benefits of 24/7 In-House Intensivist Coverage For Prolonged-Stay Cardiac Surgery Patients [63] | Kumar, K. | 2014 | JTCVS | Retrospective before-and-after observational study assessing outcomes in patients requiring prolonged CT-ICU stay after implementation of 24/7 in-house intensivists. Reduction in transfusions, ICU complications, total hospital stay, but no changes in ICU stay or 30-day mortality were observed. |
| Postoperative Complications and Outcomes Associated with a Transition to 24/7 Intensivist Management of Cardiac Surgery Patients [64] | Benoit, M.A. et al. | 2017 | Crit. Care Med. | Retrospective before-and-after observational study comparing outcomes between night resident coverage to 24/7 in-house intensivists coverage. Change was associated with reduction in major postoperative complications, duration of mechanical ventilation, CT-ICU readmissions, and surgical postponement. |
| Does The Full-Time Presence of An Intensivist Lead to Better Outcomes in The Cardiac Surgical Intensive Care Unit? [65] | Huard, P. et al. | 2020 | JTCVS | Retrospective before-and-after study comparing outcomes nighttime resident/fellow coverage to 24 h intensivist coverage. Implementation reduced mortality in patients with expected operative mortality of ≥5%, duration of mechanical ventilation, and the risk of prolonged ventilation. |
| Influence of High-Intensity Staffing Model in a Cardiac Srugery Intensive Care Unit on Postoperative Clinical Outcomes [66] | Lim, J.Y. et al. | 2020 | JTCVS | Retrospective before-and-after analysis comparing resident ran service to daytime intensivists and night resident. Implementation reduced readmissions, infections, transfusions, but did not affect 30-day mortality. |
| Survey of Contemporary Cardiac Surgery Intensive Care Unit Models in The United States [67] | Arora, R.C. et al. | 2020 | Ann. Thorac. Surg. | Survey of current staffing models in CT-ICUs in the US. 47% open, 41% semi-open, and 12% closed. 67% were pulmonary/CCM and 44% of after-hours providers were physician assistants. |
| The Presence of A Dedicated Cardiac Surgical Intensive Care Service Impacts Clinical Outcomes in Adult Cardiac Surgery Patients [68] | Lee, L.S. et al. | 2022 | J. Card. Surg. | Retrospective before-and-after study assessing outcomes after implementation of intensive care service. Length of stay, duration of mechanical ventilation, and renal failure were significantly reduced, with greatest improvement in CABG patients. |
| Importance of High-Performing Teams in the Cardiovascular Intensive Care Unit [69] | Kennedy-Metz, L.R. et al. | 2022 | JTCVS | Expert editorial on high-functioning clinical teams relating to CT-ICU practice. |
| Nationwide Clinical Practice Patterns of Anesthesiology Critical Care Physicians—A Survey to Members of The Society of Critical Care Anesthesiologists [70] | Shaefi, S. et al. | 2022 | Anesth. & Analg. | Nationwide survey of critical care anesthesiologist showing that nearly 70% practice in CT-ICUs. |
| Selected CT-ICU Knowledge Reviews | ||||
| Critical Care of the Cardiac Patient [71] | Tung, A. | 2013 | Anesthesiol. Clin. | Review of rapidly evolving areas of CT-ICU care: mechanical ventilation, transfusion thresholds, hemodynamic monitoring, and central line insertion |
| Cardiothoracic Critical Care [72] | Lobdell, K.W. et al. | 2017 | Surg. Clin. N. Am. | Review of CT-CCM concentrated on high-performing teams, system, and culture, demanding proactive, interactive, precise, and expert team. |
| Advances in Critical Care Management of Patients Undergoing Cardiac Surgery [73] | Aneman, A. et al. | 2018 | Intensive Care Med. | Narrative review outlining standards of care, recent advances, and future areas of research in the critical care management of cardiothoracic patients. |
| End-of-Life Care in Cardiothoracic Surgery [74] | Birriel, B., and K. D’Angelo | 2019 | Crit. Care Nurs. Clin. N. Am. | Review of literature on end-of-line care in CT-ICU |
| Dissemination and Implementation Science in Cardiothoracic Surgery: A Review and Case Study [75] | Heiden, B.T. et al. | 2022 | Ann. Thorac. Surg. | Expert review of dissemination and implementation science in the context of cardiothoracic surgeon, providing tools to implement evidence based practice. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kopanczyk, R.; Lester, J.; Long, M.T.; Kossbiel, B.J.; Hess, A.S.; Rozycki, A.; Nunley, D.R.; Habib, A.; Taylor, A.; Awad, H.; et al. The Future of Cardiothoracic Surgical Critical Care Medicine as a Medical Science: A Call to Action. Medicina 2023, 59, 47. https://doi.org/10.3390/medicina59010047
Kopanczyk R, Lester J, Long MT, Kossbiel BJ, Hess AS, Rozycki A, Nunley DR, Habib A, Taylor A, Awad H, et al. The Future of Cardiothoracic Surgical Critical Care Medicine as a Medical Science: A Call to Action. Medicina. 2023; 59(1):47. https://doi.org/10.3390/medicina59010047
Chicago/Turabian StyleKopanczyk, Rafal, Jesse Lester, Micah T. Long, Briana J. Kossbiel, Aaron S. Hess, Alan Rozycki, David R. Nunley, Alim Habib, Ashley Taylor, Hamdy Awad, and et al. 2023. "The Future of Cardiothoracic Surgical Critical Care Medicine as a Medical Science: A Call to Action" Medicina 59, no. 1: 47. https://doi.org/10.3390/medicina59010047