
Relation of Maternal Pre-Pregnancy Factors and Childhood Asthma: A Cross-Sectional Survey in Pre-School Children Aged 2–5 Years Old
 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
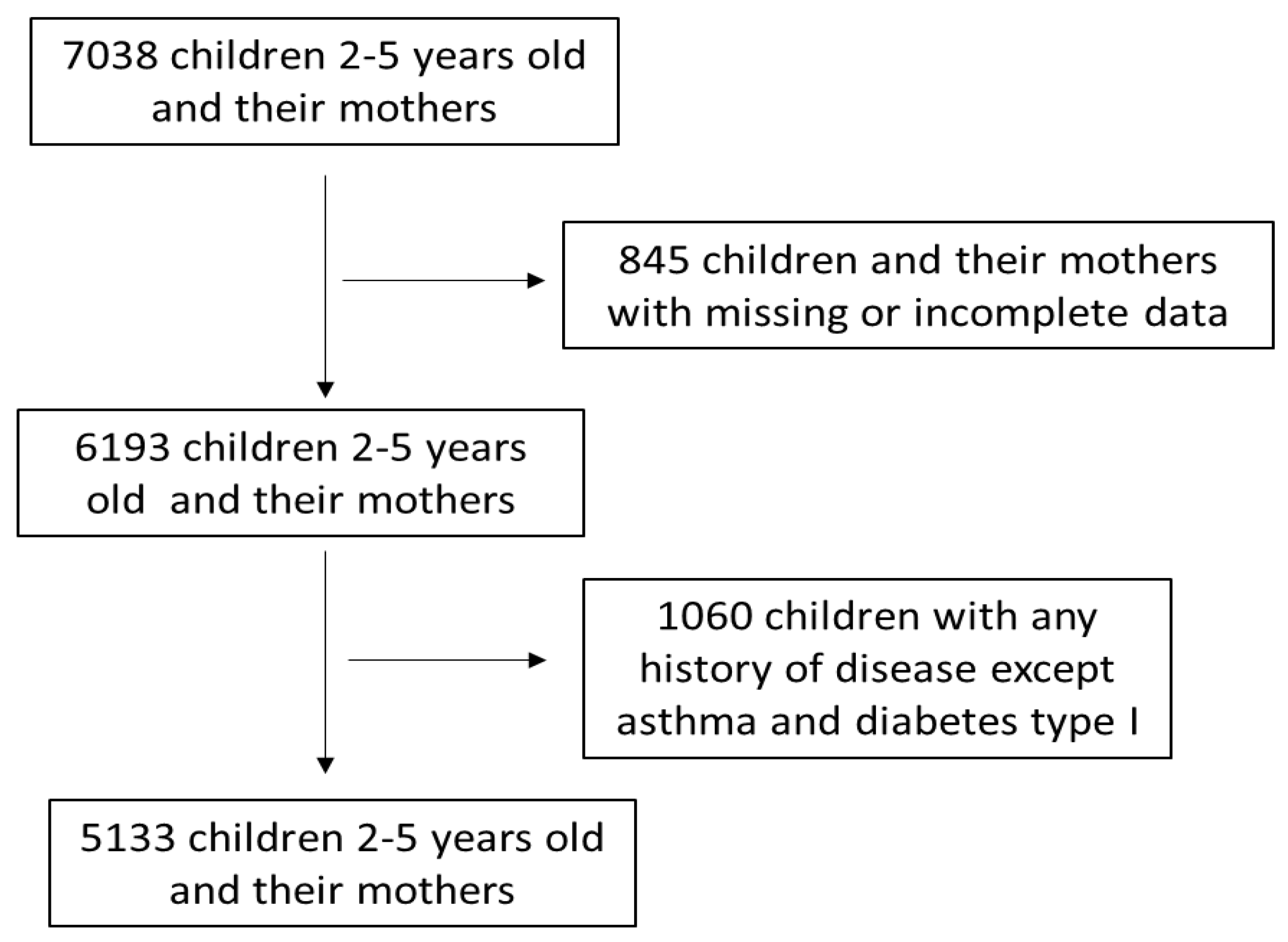
2.1. Subjects
2.2. Study Design
2.3. Statistical Analysis
3. Results
3.1. Maternal Sociodemographic Anthropometric and Lifestyle Characteristics and Perinatal Outcomes of the Study Population
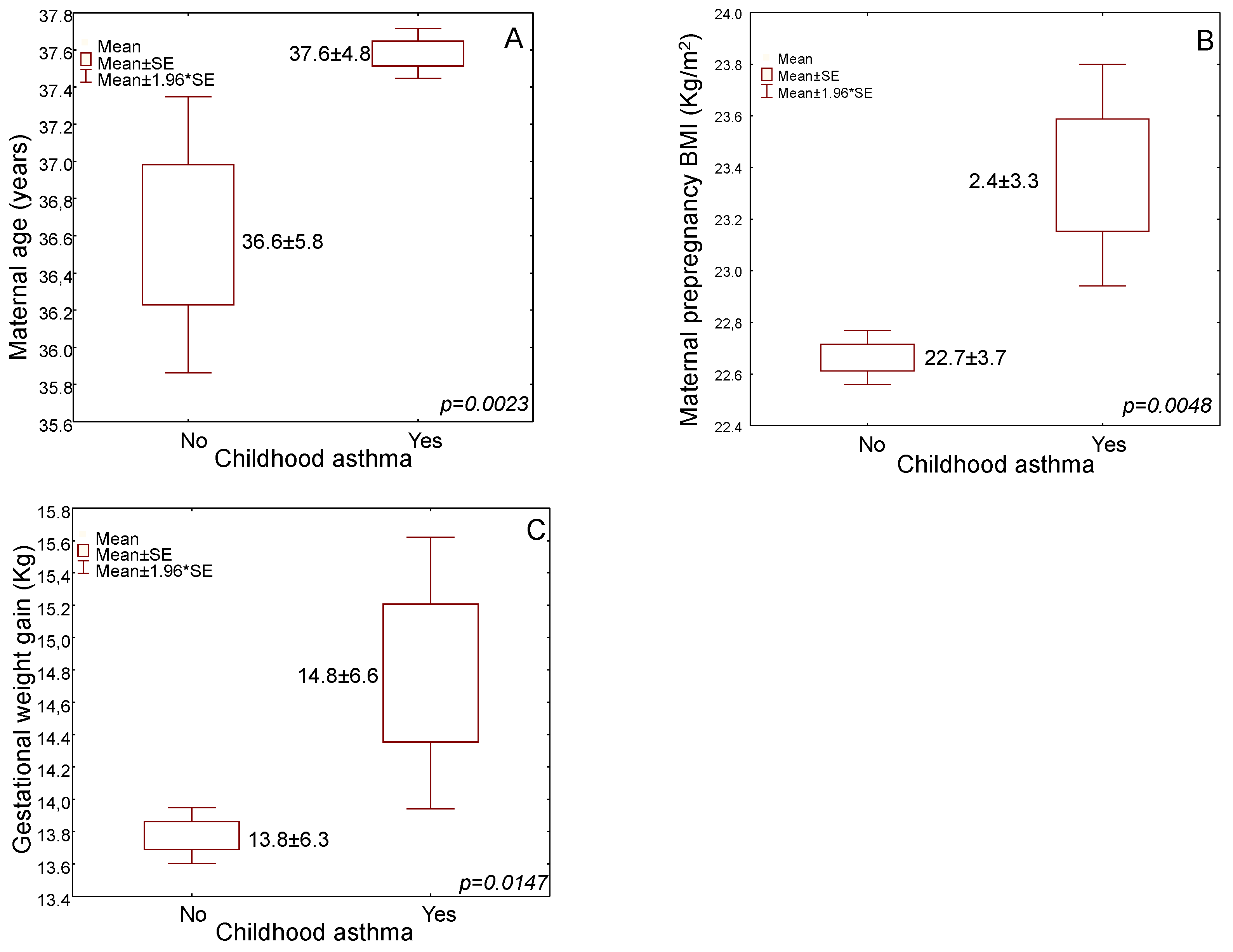
3.2. Childhood Asthma in Association with Maternal Sociodemographic and Anthropometric Factors
3.3. Childhood Asthma in Association with Maternal Perinatal Factors
3.4. Multivariate Regression Analysis for Childhood Asthma
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pearce, N.; Aït-Khaled, N.; Beasley, R.; Mallol, J.; Keil, U.; Mitchell, E.; Robertson, C. ISAAC Phase Three Study Group. Worldwide trends in the prevalence of asthma symptoms: Phase III of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax 2007, 62, 758–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loftus, P.A.; Wise, S.K. Epidemiology of asthma. Curr. Opin. Otolaryngol. Head Neck Surg. 2016, 24, 245–249. [Google Scholar] [CrossRef]
- GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef] [Green Version]
- Baseley, R.; Semprini, A.; Mitchell, E.A. Risk factors for asthma: Is prevention possible? Lancet 2015, 386, 1075–1085. [Google Scholar] [CrossRef] [PubMed]
- Nunes, C.; Pereira, A.M.; Morais-Almeida, M. Asthma costs and social impact. Asthma Res. Pract. 2017, 3, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGeachie, M.J. Childhood asthma is a risk factor for the development of chronic obstructive pulmonary disease. Curr. Opin. Allergy Clin. Immunol. 2017, 17, 104–109. [Google Scholar] [CrossRef] [Green Version]
- Annesi-Maesano, I.; Moreau, D.; Strachan, D. In utero and perinatal complications preceding asthma. Allergy 2001, 56, 491–497. [Google Scholar] [CrossRef]
- Davidson, R.; Roberts, S.E.; Wotton, C.J.; Goldacre, M.J. Influence of maternal and perinatal factors on subsequent hospitalization for asthma in children: Evidence from the Oxford record linkage study. BMC Pulm. Med. 2010, 10, 14. [Google Scholar] [CrossRef] [Green Version]
- Schäfer, S.; Wang, K.; Sundling, F.; Yang, J.; Liu, A.; Nanan, R. Modelling maternal and perinatal risk factors to predict poorly controlled childhood asthma. PloS ONE 2021, 16, e0252215. [Google Scholar] [CrossRef]
- Rusconi, F.; Popovic, M. Maternal obesity and childhood wheezing and asthma. Paediatr. Respir. Rev. 2017, 22, 66–71. [Google Scholar] [CrossRef]
- Godfrey, K.M.; Reynolds, R.M.; Prescott, S.L.; Nyirenda, M.; Jaddoe, V.W.; Eriksson, J.G.; Broekman, B.F.P. Influence of maternal obesity on the long-term health of offspring. Lancet Diabetes Endocrinol. 2017, 5, 53–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polinski, K.J.; Liu, J.; Boghossian, N.S.; McLain, A.C. Maternal obesity, gestational weight gain, and asthma in offspring. Prev. Chronic Dis. 2017, 14, E109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, M.; Bhattacharya, S.; Philip, S.; Norman, J.E.; McLernon, D.J. Planned cesarean delivery at term and adverse outcomes in childhood health. JAMA 2015, 314, 2271–2279. [Google Scholar] [CrossRef] [PubMed]
- Brix, N.; Stokholm, L.; Jonsdottir, F.; Kristensen, K.; Scher, N.J. Comparable risk of childhood asthma after vaginal delivery and emergency caesarean section. Dan. Med. J. 2016, 64, A5313. [Google Scholar]
- Tollånes, M.C.; Moster, D.; Daltveit, A.K.; Irgens, L.M. Cesarean section and risk of severe childhood asthma: A population-based cohort study. J. Pediatr. 2018, 153, 112–126. [Google Scholar] [CrossRef] [PubMed]
- Adgent, M.A.; Gebretsadik, T.; Reedus, J.; Graves, C.; Garrison, E.; Bush, N.; Davis, R.; LeWinn, K.Z.; Tylavsky, F.; Carroll, K.N. Gestational diabetes and childhood asthma in a racially diverse US pregnancy cohort. Pediatr Allergy Immunol. 2021, 32, 1190–1196. [Google Scholar] [CrossRef]
- Been, J.V.; Lugtenberg, M.J.; Smets, E.; van Schayck, C.P.; Kramer, B.W.; Mommers, M.; Sheikh, A. Preterm birth and childhood wheezing disorders: A systematic review and meta-analysis. PLoS Med. 2014, 11, e1001596. [Google Scholar] [CrossRef] [Green Version]
- Drehmer, J.E.; Walters, B.H.; Nabi-Burza, E.; Winickoff, J.P. Guidance for the clinical management of thirdhand smoke exposure in the child health care setting. J. Clin. Outcomes Manag. 2017, 24, 551. [Google Scholar]
- Lossius, A.K.; Magnus, M.C.; Lunde, J.; Størdal, K. Prospective Cohort Study of Breastfeeding and the Risk of Childhood Asthma. J. Pediatr. 2018, 195, 182–189. [Google Scholar] [CrossRef]
- Kumar, P.H.; Devgan, A. The Association of Breastfeeding With Childhood Asthma: A Case-Control Study From India. Cureus 2021, 13, e19810. [Google Scholar]
- Wilson, K.; Gebretsadik, T.; Adgent, M.A.; Loftus, C.; Karr, C.; Moore, P.E.; Sathyanarayana, S.; Byington, N.; Barrett, E.; Bush, N.; et al. The association between duration of breastfeeding and childhood asthma outcomes. Ann. Allergy Asthma Immunol. 2022, 129, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Koutelidakis, A.E.; Alexatou, O.; Kousaiti, S.; Gkretsi, E.; Vasios, G.; Sampani, A.; Tolia, M.; Kiortsis, D.N.; Giaginis, C. Higher adherence to Mediterranean diet prior to pregnancy is associated with decreased risk for deviation from the maternal recommended gestational weight gain. Int. J. Food Sci. Nutr. 2018, 69, 84–92. [Google Scholar] [CrossRef]
- Rosa, M.J.; Hartman, T.J.; Adgent, M.; Gardner, K.; Gebretsadik, T.; Moore, P.E.; Davis, R.L.; LeWinn, K.Z.; Bush, N.R.; Tylavsky, F.; et al. Prenatal polyunsaturated fatty acids and child asthma: Effect modification by maternal asthma and child sex. J. Allergy Clin. Immunol. 2020, 145, 800–807.e4. [Google Scholar] [CrossRef] [PubMed]
- Asher, M.I.; Keil, U.; Anderson, H.R.; Beasley, R.; Crane, J.; Martinez, F.; Mitchell, E.A.; Pearce, N.; Sibbald, B.; Stewart, A.W.; et al. International Study of Asthma and Allergies in Childhood (ISAAC): Rationale and methods. Eur. Respir. J. 1995, 8, 483–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez, M.P.; Lin, J.; Chow, T.; Chung, J.; Wang, X.; Xiang, A.H. Maternal Gestational Diabetes and Type 2 Diabetes During Pregnancy and Risk of Childhood Asthma in Offspring. J. Pediatr. 2020, 219, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Silva, B.B.D.; Silva, J.D.; Traebert, J.L.; Schlindwein, A.D. Maternal and early childhood factors associated with asthma and obesity in children aged 6 to 7 years: A case control study. Einstein 2022, 20, eAO5609. [Google Scholar] [CrossRef]
- Wadden, D.; Farrell, J.; Smith, M.J.; Laurie, K.; Twells, L.K.; Gao, Z. Maternal history of asthma modifies the risk of childhood persistent asthma associated with maternal age at birth: Results from a large prospective cohort in Canada. J. Asthma 2021, 58, 38–45. [Google Scholar] [CrossRef]
- Reichman, N.E.; Nepomnyaschy, L. Maternal pre-pregnancy obesity and diagnosis of asthma in offspring at age 3 years. Matern. Child Health J. 2008, 12, 725–733. [Google Scholar] [CrossRef]
- Forno, E.; Young, O.M.; Kumar, R.; Simhan, H.; Celedón, J.C. Maternal obesity in pregnancy, gestational weight gain, and risk of childhood asthma. Pediatrics 2014, 134, e535–e546. [Google Scholar] [CrossRef] [Green Version]
- Leermakers, E.T.; Sonnenschein-van der Voort, A.M.; Gaillard, R.; Hofman, A.; de Jongste, J.C.; Jaddoe, V.W.; Duijts, L. Maternal weight, gestational weight gain and preschool wheezing: The Generation R Study. Eur. Respir. J. 2013, 42, 1234–1243. [Google Scholar] [CrossRef] [Green Version]
- Altmäe, S.; Segura, M.T.; Esteban, F.J.; Bartel, S.; Brandi, P.; Irmler, M.; Beckers, J.; Demmelmair, H.; López-Sabater, C.; Koletzko, B.; et al. Maternal Pre-Pregnancy Obesity Is Associated with Altered Placental Transcriptome. PLoS ONE 2017, 12, e0169223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polinski, K.J.; Bell, G.A.; Trinh, M.-H.; Sundaram, R.; Mendola, P.; Robinson, S.L.; Bell, E.M.; Adeyeye, T.; Lin, T.-C.; Yeung, E.H. Maternal obesity, gestational weight gain, and offspring asthma and atopy. Ann. Allergy Asthma Immunol. 2022, 129, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Zhou, B.; Wang, Y.; Wang, K.; Zhang, Z.; Niu, W. Pre-pregnancy Maternal Weight and Gestational Weight Gain Increase the Risk for Childhood Asthma and Wheeze: An Updated Meta-Analysis. Front. Pediatr. 2020, 8, 134. [Google Scholar] [CrossRef]
- Chen, Y.; Zhu, J.; Lyu, J.; Xia, Y.; Ying, Y.; Hu, Y.; Qu, J.; Tong, S.; Li, S. Association of Maternal Prepregnancy Weight and Gestational Weight Gain With Children’s Allergic Diseases. JAMA Netw. Open 2020, 3, e2015643. [Google Scholar] [CrossRef]
- Lodge, C.J.; Tan, D.J.; Lau, M.X.; Dai, X.; Tham, R.; Lowe, A.J.; Bowatte, G.; Allen, K.J.; Dharmage, S.C. Breastfeeding and asthma and allergies: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 38–53. [Google Scholar] [CrossRef]
- Dogaru, C.M.; Nyffenegger, D.; Pescatore, A.M.; Spycher, B.D.; Kuehni, C.E. Breastfeeding and childhood asthma: Systematic review and meta-analysis. Am. J. Epidemiol. 2014, 179, 1153–1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brew, B.K.; Allen, C.W.; Toelle, B.G.; Marks, J.B. Systematic review and meta-analysis investigating breast feeding and childhood wheezing illness. Paediatr. Perinat. Epidemiol. 2011, 25, 507–518. [Google Scholar] [CrossRef]
- Xue, M.; Dehaas, E.; Chaudhary, N.; O’Byrne, P.; Satia, I.; Kurmi, O.P. Breastfeeding and risk of childhood asthma: A systematic review and meta-analysis. Eur. Respir. Soc. Open Res. 2021, 7, 00504–02021. [Google Scholar] [CrossRef]
- Kapourchali, F.R.; Cresci, G.A.M. Early-Life Gut Microbiome-The Importance of Maternal and Infant Factors in Its Establishment. Nutr. Clin. Pract. 2020, 35, 386–405. [Google Scholar] [CrossRef]
- Notarbartolo, V.; Giuffrè, M.; Montante, C.; Corsello, G.; Carta, M. Composition of Human Breast Milk Microbiota and Its Role in Children’s Health. Pediatr. Gastroenterol. Hepatol. Nutr. 2022, 25, 194–210. [Google Scholar] [CrossRef]
- Johnson, C.C.; Ownby, D.R. Allergies and Asthma: Do Atopic Disorders Result from Inadequate Immune Homeostasis arising from Infant Gut Dysbiosis? Expert Rev. Clin. Immunol. 2016, 12, 379–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sozańska, B. Microbiome in the primary prevention of allergic diseases and bronchial asthma. Allergol. Immunopathol. 2019, 47, 79–84. [Google Scholar] [CrossRef]
- Wood, H.; Acharjee, A.; Pearce, H.; Quraishi, M.N.; Powell, R.; Rossiter, A.; Beggs, A.; Ewer, A.; Moss, P.; Toldi, G. Breastfeeding promotes early neonatal regulatory T-cell expansion and immune tolerance of non-inherited maternal antigens. Allergy 2021, 76, 2447–2460. [Google Scholar] [CrossRef] [PubMed]
- Kull, I.; Wickman, M.; Lilja, G.; Nordvall, S.L.; Pershagen, G. Breast feeding and allergic diseases in infants-a prospective birth cohort study. Arch. Dis. Child. 2002, 87, 478–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Yassen, A.Q.; Al-Asadi, J.N.; Khalaf, S.K. The role of Caesarean section in childhood asthma. Malays. Fam. Physician 2019, 14, 10–17. [Google Scholar]
- Wypych-Ślusarska, A.; Niewiadomska, E.; Oleksiuk, K.; Krupa-Kotara, K.; Głogowska-Ligus, J.; Słowiński, J. Caesarean delivery and risk of childhood asthma development: Meta-analysis. Postep. Dermatol. I Alergol. 2021, 38, 819–826. [Google Scholar] [CrossRef]
- Burlina, S.; Dalfra, M.G.; Lapolla, A. Short- and long-term consequences for offspring exposed to maternal diabetes: A review. J. Matern.-Fetal Neonatal Med. 2019, 32, 687–694. [Google Scholar] [CrossRef]
- Lock, M.; McGillick, E.V.; Orgeig, S.; McMillen, I.C.; Morrison, J.L. Regulation of fetal lung development in response to maternal overnutrition. Clin. Exp. Pharmacol. Physiol. 2013, 40, 803–816. [Google Scholar] [CrossRef]
- Pagano, F.; Conti, M.G.; Boscarino, G.; Pannucci, C.; Dito, L.; Regoli, D.; Di Chiara, M.; Battaglia, G.; Prota, R.; Cinicola, B.; et al. Atopic Manifestations in Children Born Preterm: A Long-Term Observational Study. Children 2021, 8, 843. [Google Scholar] [CrossRef]
- Azad, M.B.; Moyce, B.L.; Guillemette, L.; Pascoe, C.D.; Wicklow, B.; McGavock, J.M.; Halayko, A.J.; Dolinsky, V.W. Diabetes in pregnancy and lung health in offspring: Developmental origins of respiratory disease. Paediatr. Respir. Rev. 2017, 21, 19–26. [Google Scholar] [CrossRef]
- Stick, S.M.; Burton, P.R.; Gurrin, L.; Sly, P.D.; LeSouëf, P.N. Effects of maternal smoking during pregnancy and a family history of asthma on respiratory function in newborn infants. Lancet 1996, 348, 1060–1064. [Google Scholar] [CrossRef] [PubMed]
- Silvestri, M.; Franchi, S.; Pistorio, A.; Petecchia, L.; Rusconi, F. Smoke exposure, wheezing, and asthma development: A systematic review and meta-analysis in unselected birth cohorts. Pediatr. Pulmonol. 2015, 50, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, S.O.; Macdonald-Wallis, C.; Lawlor, D.A.; Henderson, A.J. Hypertensive disorders of pregnancy, respiratory outcomes and atopy in childhood. Eur. Respir. J. 2016, 47, 156–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Midya, V.; Pal, S.; Sinharoy, A.; Das, J.K.; Rao, H.; Abu-Hasan, M.; Mondal, P. The Association Between Female Smoking and Childhood Asthma Prevalence-A Study Based on Aggregative Data. Front. Public Health 2018, 6, 295. [Google Scholar] [CrossRef]
- Burke, H.; Leonardi-Bee, J.; Hashim, A.; Pine-Abata, H.; Chen, Y.; Cook, D.G.; Britton, J.R.; McKeever, T.M. Prenatal and passive smoke exposure and incidence of asthma and wheeze: Systematic review and meta-analysis. Pediatrics 2012, 129, 735–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, H.; Butz, A.; Keet, C.A.; Minkovitz, C.S.; Hong, X.; Caruso, D.M.; Pearson, C.; Cohen, R.T.; Wills-Karp, M.; Zuckerman, B.S.; et al. Preterm Birth with Childhood Asthma: The Role of Degree of Prematurity and Asthma Definitions. Am. J. Respir. Crit. Care Med. 2015, 192, 520–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crump, C.; Winkleby, M.A.; Sundquist, J.; Sundquist, K. Risk of asthma in young adults who were born preterm: A Swedish national cohort study. Pediatrics 2011, 127, e913–e920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyake, Y.; Tanaka, K. Lack of relationship between birth conditions and allergic disorders in Japanese children aged 3 years. J. Asthma 2013, 50, 555–559. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameters (n = 5133) | Childhood Asthma | ||
|---|---|---|---|
| No (95.5%) | Yes (4.5%) | p-Value | |
| Age (years) | 36.6 ± 5.8 | 37.6 ± 4.8 | p = 0.0023 |
| Nationality (n, %) | p = 0.0475 | ||
| Greek | 4684 (95.6) | 229 (98.3) | |
| Other | 216 (4.5) | 4 (1.7) | |
| Pre-pregnancy BMI (kg/m2) | 22.7 ± 3.7 | 23.4 ± 3.3 | p = 0.0048 |
| Pre-pregnancy BMI status (n, %) | p < 0.0001 | ||
| Normal weight | 3864 (78.9) | 117 (50.2) | |
| Overweight | 814 (16.6) | 84 (36.1) | |
| The bold iObese | 222 (4.5) | 32 (13.7) | |
| Education (years ± SD) | 15.1 ± 2.3 | 15.1 ± 2.0 | p = 0.9505 |
| Economic status (n, %) | p = 0.4309 | ||
| Low | 1356 (45.8) | 58 (42.3) | |
| Medium or high | 1607 (54.2) | 79 (57.7) | |
| Smoking habits (n, %) | p = 0.0921 | ||
| No smokers | 3617 (73.8) | 201 (86.3) | |
| Smokers | 1283 (26.2) | 32 (13.7) | |
| Gestational weight gain (kg) | 13.8 ± 6.3 | 14.8 ± 6.6 | p = 0.0147 |
| Exclusive breastfeeding (n, %) | p = 0.0006 | ||
| No | 2441 (49.8) | 143 (61.4) | |
| Yes | 2459 (50.2) | 90 (38.6) | |
| Preterm birth (<37th week, n, %) | p = 0.6947 | ||
| No | 3424 (69.9) | 160 (68.7) | |
| Yes | 1476 (30.1) | 73 (31.3) | |
| Mode of delivery (n, %) | p = 0.0034 | ||
| Vaginal | 2160 (44.1) | 80 (34.3) | |
| Caesarean section | 2740 (55.9) | 153 (65.7) | |
| Gestational diabetes (n, %) | p = 0.0003 | ||
| No | 4700 (95.9) | 212 (91.0) | |
| Yes | 200 (4.1) | 21 (9.0) | |
| Pregnancy-induced hypertension (n, %) | p < 0000.1 | ||
| No | 4737 (96.7) | 183 (78.5) | |
| Yes | 163 (3.3) | 50 (21.5) | |
| Parameters | Childhood Asthma | |
|---|---|---|
| HR a (95% CI b) | p-Value | |
| Age (Below/Over mean value) | 1.32 (0.83–1.94) | p = 0.0245 |
| Nationality (Greek/Other nationality) | 0.98 (0.20–1.89) | p = 0.4501 |
| Pre-pregnancy BMI status | p = 0.0002 | |
| Normal weight | 1.0 | |
| Overweight | 1.63 (1.12–2.01) | |
| Obese | 1.97 (1.65–2.34) | |
| Education (Below/Over mean value) | 1.20 (0.32–2.19) | p = 0.2402 |
| Economic status (Low/Medium or high) | 0.75 (0.13–1.59) | p = 0.5611 |
| Smoking habits (No/Yes) | 1.53 (0.73–2.38) | p = 0.2749 |
| Gestational weight gain (Below/Over mean value) | 1.62 (0.92–2.46) | p = 0.0763 |
| Exclusive breastfeeding (No/Yes) | 2.25 (1.80–2.49) | p = 0.0095 |
| Preterm birth (No/Yes) | 1.29 (0.47–2.12) | p = 0.2873 |
| Mode of delivery (Vaginal/Caesarean) | 1.89 (1.41–2.30) | p = 0.0194 |
| Gestational diabetes (No/Yes) | 1.43 (0.94–2.01) | p = 0.0298 |
| Pregnancy-induced hypertension (No/Yes) | 1.14 (0.67–1.69) | p = 0.0130 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papandreou, D.; Pavlidou, E.; Tyrovolas, S.; Mantzorou, M.; Andreou, E.; Psara, E.; Antasouras, G.; Vasios, G.K.; Poulios, E.; Giaginis, C. Relation of Maternal Pre-Pregnancy Factors and Childhood Asthma: A Cross-Sectional Survey in Pre-School Children Aged 2–5 Years Old. Medicina 2023, 59, 179. https://doi.org/10.3390/medicina59010179
Papandreou D, Pavlidou E, Tyrovolas S, Mantzorou M, Andreou E, Psara E, Antasouras G, Vasios GK, Poulios E, Giaginis C. Relation of Maternal Pre-Pregnancy Factors and Childhood Asthma: A Cross-Sectional Survey in Pre-School Children Aged 2–5 Years Old. Medicina. 2023; 59(1):179. https://doi.org/10.3390/medicina59010179
Chicago/Turabian StylePapandreou, Dimitrios, Eleni Pavlidou, Stefanos Tyrovolas, Maria Mantzorou, Eleni Andreou, Evmorfia Psara, Georgios Antasouras, Georgios K. Vasios, Efthymios Poulios, and Constantinos Giaginis. 2023. "Relation of Maternal Pre-Pregnancy Factors and Childhood Asthma: A Cross-Sectional Survey in Pre-School Children Aged 2–5 Years Old" Medicina 59, no. 1: 179. https://doi.org/10.3390/medicina59010179