
Auricular Acupressure for Dry Eye Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection
2.2.1. P (Population)
2.2.2. I (Intervention)
2.2.3. C (comparison)
2.2.4. O (Outcome)
Primary Outcome
Secondary Outcome
2.3. Screening Procedures of Eligible Studies and Data Extraction
2.3.1. Screening Procedures of Eligible Studies
2.3.2. Data Extraction
2.4. Assessment of Risk of Bias in Included Studies
2.5. Quality of Evidence
2.6. Assessment of Heterogeneity and Data Synthesis
2.7. Sensitivity Analysis
2.8. Assessment of Reporting Bias
2.9. Ethic Approval
3. Results
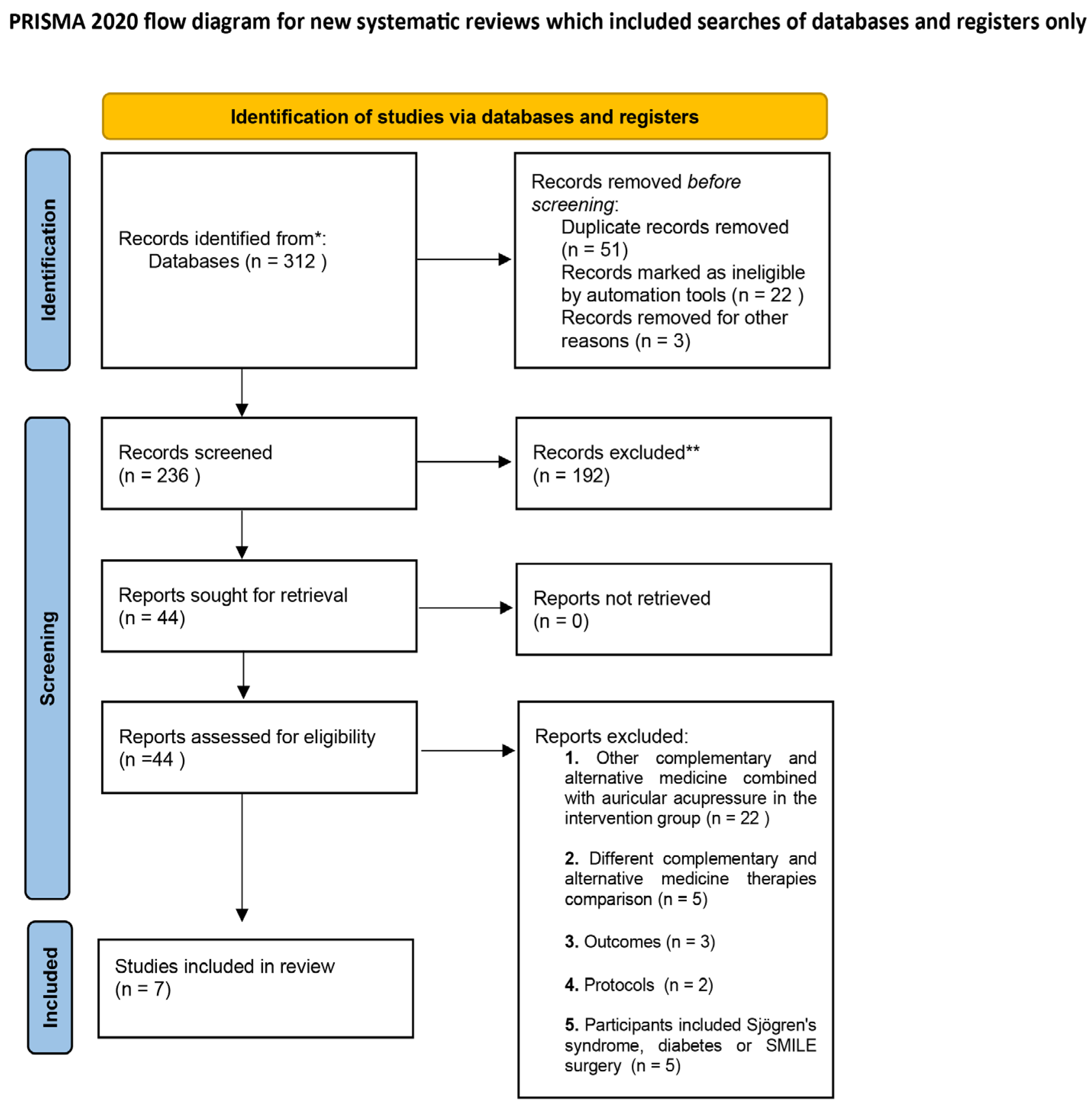
3.1. Search Results and Study Characteristics
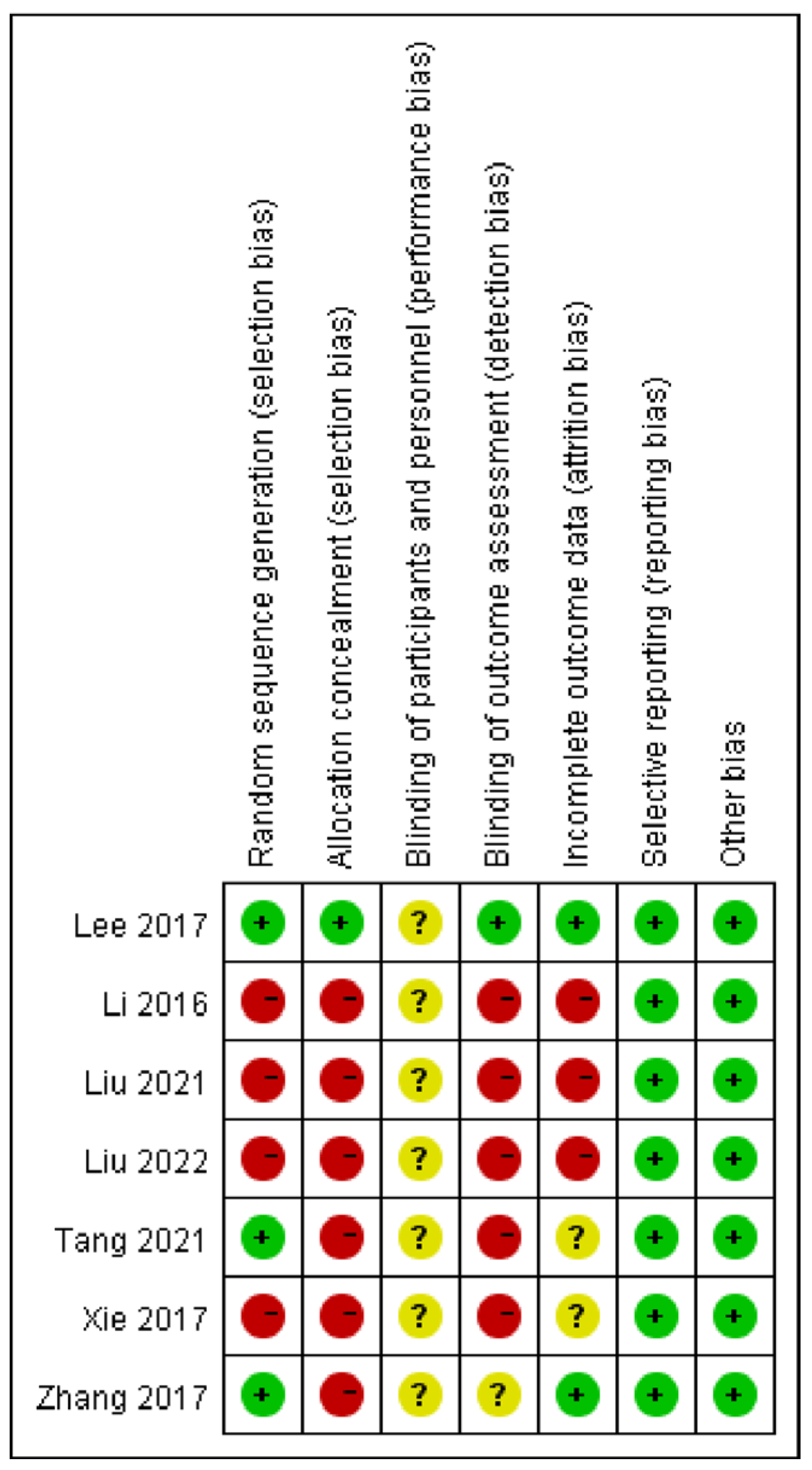
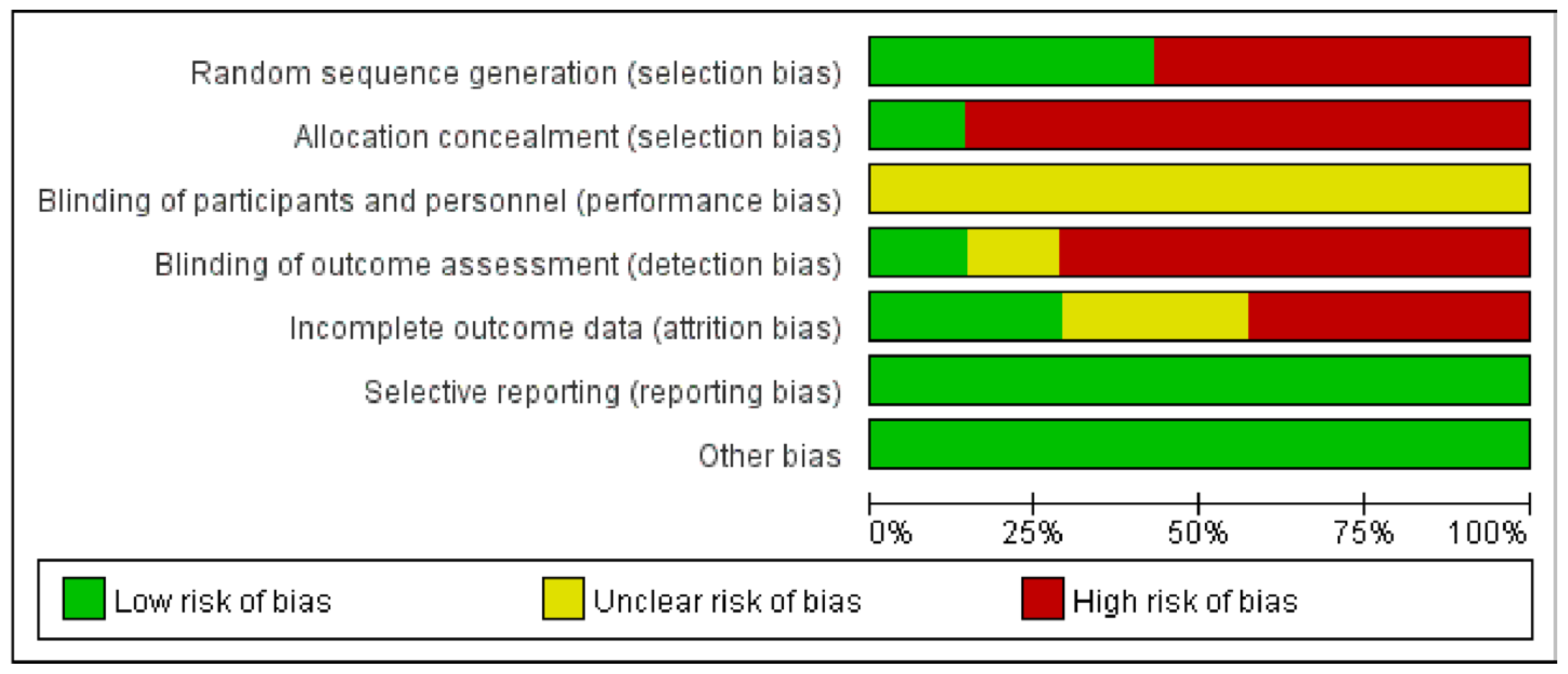
3.2. Risk of Bias and Quality of Evidence
3.3. Quantitative Data Synthesis
3.3.1. Artificial Tears vs. Auricular Acupressure
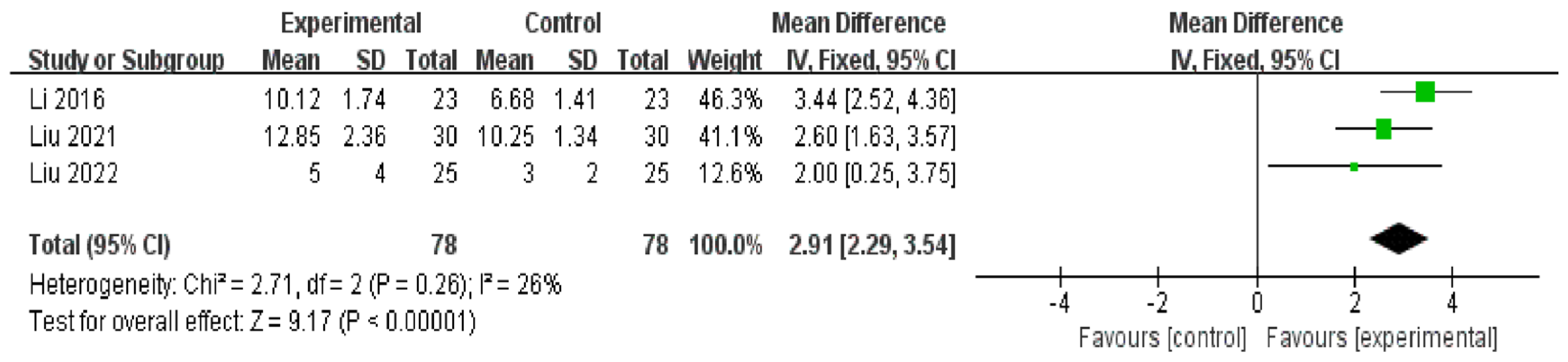
TBUT
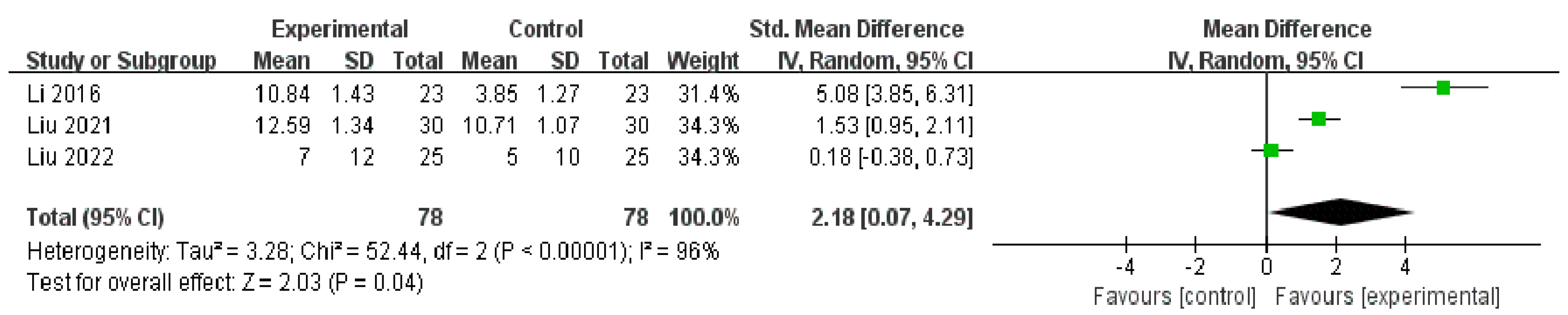
SIT
SOS
OSDI
3.3.2. Artificial Tears vs. Auricular Acupressure plus Artificial Tears
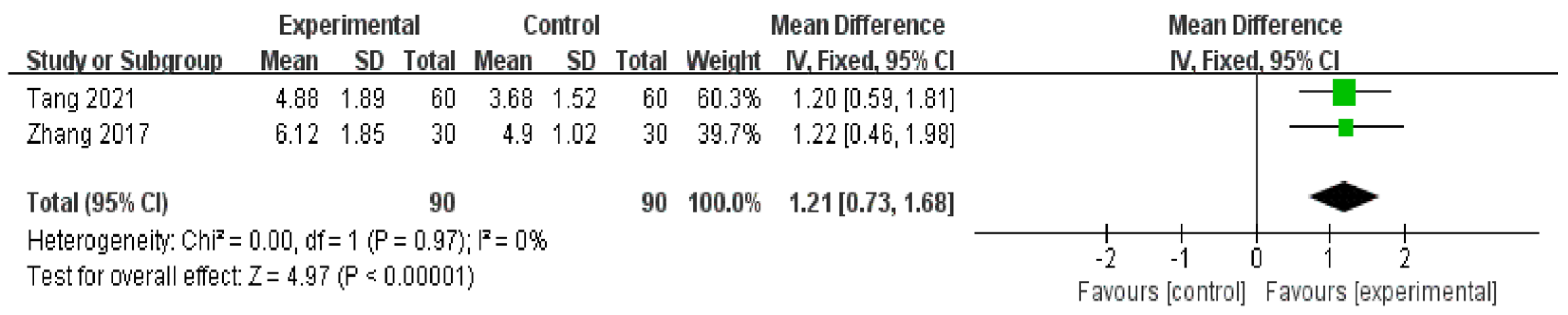
TBUT
SIT
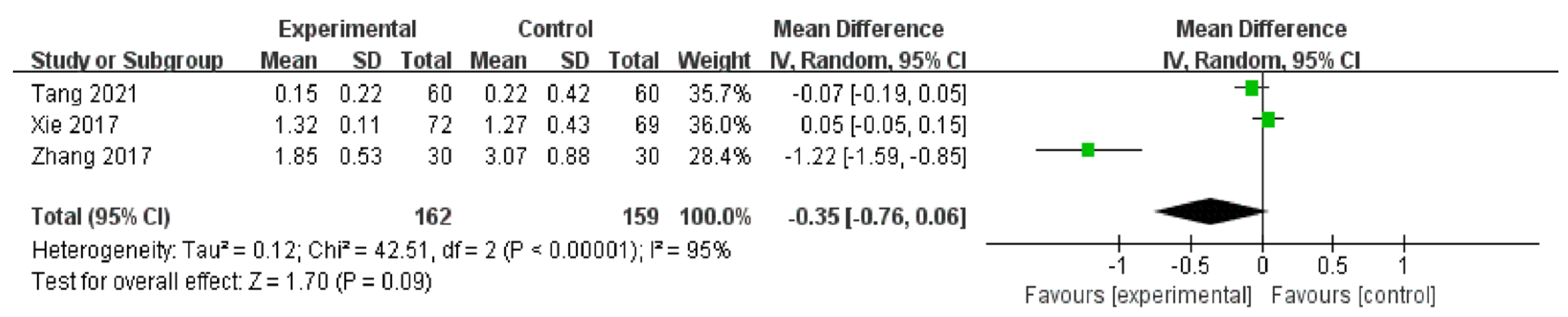
CFS
Response Rate
SOS
OSDI
3.3.3. Auricular Acupressure vs. Sham Auricular Acupressure
3.4. Sensitive Analysis
3.5. Adverse Events
4. Discussion
4.1. Principal Findings
4.2. Comparison with the Previous Literature
4.3. Risk of Bias and Evidence Quality
4.4. Exploration of Heterogeneity
4.5. The Cumulative and Lasting Effects of Auricular Acupressure
4.6. Safety Assessment and Placebo Effect
4.7. Possible Mechanism of Action of Auricular Acupressure
4.8. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.-K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef]
- The epidemiology of dry eye disease: Report of the Epidemiology Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007, 5, 93–107. [CrossRef]
- Li, M.; Zeng, L.; Mi, S.; Li, Y.; Liu, Z.; Yu, K.; Hu, Q.; Li, H.; Ma, D.; Zhou, Y.; et al. A Multicenter Study of the Prevalence of Dry Eye Disease in Chinese Refractive Surgery Candidates. Ophthalmic Res. 2021, 64, 224–229. [Google Scholar] [CrossRef]
- Kim, W.J.; Kim, H.S.; Kim, M.S. Current Trends in the Recognition and Treatment of Dry Eye: A Survey of Ophthalmologists. J. Korean Ophthalmol. Soc. 2007, 48, 1614–1622. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.G.; Wang, H. Focusing on the management of chronic dry eye disease. Zhonghua Yan Ke Za Zhi 2018, 54, 81–83. [Google Scholar]
- Farrand, K.F.; Fridman, M.; Stillman, I.Ö.; Schaumberg, D.A. Prevalence of Diagnosed Dry Eye Disease in the United States Among Adults Aged 18 Years and Older. Am. J. Ophthalmol. 2017, 182, 90–98. [Google Scholar] [CrossRef] [Green Version]
- Shimazaki, J. Definition and Diagnostic Criteria of Dry Eye Disease: Historical Overview and Future Directions. Investig. Ophthalmol. Vis. Sci. 2018, 59, DES7–DES12. [Google Scholar] [CrossRef] [Green Version]
- Akpek, E.K.; Amescua, G.; Farid, M.; Garcia-Ferrer, F.J.; Lin, A.; Rhee, M.K.; Varu, D.M.; Musch, D.C.; Dunn, S.P.; Mah, F.S. Dry Eye Syndrome Preferred Practice Pattern®. Ophthalmology 2018, 126, P286–P334. [Google Scholar] [CrossRef] [Green Version]
- Bron, A.J.; Tomlinson, A.; Foulks, G.N.; Pepose, J.S.; Baudouin, C.; Geerling, G.; Nichols, K.K.; Lemp, M.A. Rethinking Dry Eye Disease: A Perspective on Clinical Implications. Ocul. Surf. 2014, 12, S1–S31. [Google Scholar] [CrossRef]
- Sriprasert, I.; Warren, D.W.; Mircheff, A.K.; Stanczyk, F.Z. Dry eye in postmenopausal women: A hormonal disorder. Menopause 2016, 23, 343–351. [Google Scholar] [CrossRef]
- Yu, J.; Asche, C.V.; Fairchild, C.J. The Economic Burden of Dry Eye Disease in the United States: A Decision Tree Analysis. Cornea 2011, 30, 379–387. [Google Scholar] [CrossRef]
- Pflugfelder, S.C. Prevalence, burden, and pharmacoeconomics of dry eye disease. Am. J. Manag. Care 2008, 14, S102–S106. [Google Scholar]
- Friedman, N.J. Impact of dry eye disease and treatment on quality of life. Curr. Opin. Ophthalmol. 2010, 21, 310–316. [Google Scholar] [CrossRef]
- Brown, M.M.; Brown, G.C.; Brown, H.C.; Peet, J.; Roth, Z. Value-Based Medicine, Comparative Effectiveness, and Cost-effectiveness Analysis of Topical Cyclosporine for the Treatment of Dry Eye Syndrome. Arch. Ophthalmol. 2009, 127, 146–152. [Google Scholar] [CrossRef]
- Bunya, V.Y.; Fernandez, K.B.; Ying, G.-S.; Massaro-Giordano, M.; Macchi, I.; Sulewski, M.E.; Hammersmith, K.M.; Nagra, P.K.; Rapuano, C.J.; Orlin, S.E. Survey of Ophthalmologists Regarding Practice Patterns for Dry Eye and Sjogren Syndrome. Eye Contact Lens Sci. Clin. Pract. 2018, 44 (Suppl. S2), S196–S201. [Google Scholar] [CrossRef]
- Stapleton, F.; Alves, M.; Bunya, V.Y.; Jalbert, I.; Lekhanont, K.; Malet, F.; Na, K.-S.; Schaumberg, D.; Uchino, M.; Vehof, J.; et al. TFOS DEWS II epidemiology report. Ocul. Surf. 2017, 15, 334–365. [Google Scholar] [CrossRef]
- Thode, A.R.; Latkany, R.A. Current and Emerging Therapeutic Strategies for the Treatment of Meibomian Gland Dysfunction (MGD). Drugs 2015, 75, 1177–1185. [Google Scholar] [CrossRef]
- Lemp, M.A. Management of dry eye disease. Am. J. Manag. Care 2008, 14, S88–S101. [Google Scholar]
- Perry, H.D.; Solomon, R.; Donnenfeld, E.D.; Perry, A.R.; Wittpenn, J.R.; Greenman, H.E.; Savage, H.E. Evaluation of Topical Cyclosporine for the Treatment of Dry Eye Disease. Arch. Ophthalmol. 2008, 126, 1046. [Google Scholar] [CrossRef] [Green Version]
- Mah, F.; Milner, M.; Yiu, S.; Donnenfeld, E.; Conway, T.M.; Hollander, D.A. PERSIST: Physician’s Evaluation of Restasis® Satisfaction in Second Trial of topical cyclosporine ophthalmic emulsion 0.05% for dry eye: A retrospective review. Clin. Ophthalmol. 2012, 6, 1971–1976. [Google Scholar] [CrossRef] [Green Version]
- Zhou, W.Y.; Li, Y.H. A survey on treatment of dry eye by traditional Chinese medicine and integrative Chinese and Western medicine. Chin. J. Integr. Med. 2006, 12, 154–159. [Google Scholar] [CrossRef]
- Smith, J.; Spurrier, N.; Martin, J.; Rosenbaum, J. Prevalent use of complementary and alternative medicine by patients with inflammatory eye disease. Ocul. Immunol. Inflamm. 2004, 12, 203–214. [Google Scholar] [CrossRef]
- Lee, M.S.; Shin, B.-C.; Choi, T.-Y.; Ernst, E. Acupuncture for treating dry eye: A systematic review. Acta Ophthalmol. 2011, 89, 101–106. [Google Scholar] [CrossRef]
- Pomeranz, B.; Stux, G. Scientific Bases of Acupuncture; Springer: Berlin/Heidelberg, Germany, 1989. [Google Scholar]
- Prinz, J.; Maffulli, N.; Fuest, M.; Walter, P.; Hildebrand, F.; Migliorini, F. Acupuncture for the management of dry eye disease. Front. Med. 2022, 16, 975–983. [Google Scholar] [CrossRef]
- Kim, T.-H.; Kang, J.W.; Kim, K.H.; Kang, K.-W.; Shin, M.-S.; Jung, S.-Y.; Kim, A.-R.; Jung, H.-J.; Choi, J.-B.; Hong, K.E.; et al. Acupuncture for the Treatment of Dry Eye: A Multicenter Randomised Controlled Trial with Active Comparison Intervention (Artificial Teardrops). PLoS ONE 2012, 7, e36638. [Google Scholar] [CrossRef]
- Liu, X.-R.; Rana, N.; Wong, N.-S.; James, C.; Lu, J.; Xu, X. The Effect of Auricular Acupressure on Sleep Disturbance Among Patients with Leukemia: A Feasibility Study. Holist. Nurs. Pract. 2020, 34, 103–112. [Google Scholar] [CrossRef]
- Gao, H.; Zhang, L.; Liu, J. Auricular acupressure for myopia in children and adolescents: A systematic review. Complement. Ther. Clin. Pract. 2020, 38, 101067. [Google Scholar] [CrossRef]
- Liang, C.-K.; Ho, T.-Y.; Li, T.-C.; Hsu, W.-M.; Li, T.-M.; Lee, Y.-C.; Ho, W.-J.; Cheng, J.-T.; Tzeng, C.-Y.; Liu, I.-T.; et al. A combined therapy using stimulating auricular acupoints enhances lower-level atropine eyedrops when used for myopia control in school-aged children evaluated by a pilot randomized controlled clinical trial. Complement. Ther. Med. 2008, 16, 305–310. [Google Scholar] [CrossRef]
- Hou, P.-W.; Hsu, H.-C.; Lin, Y.-W.; Tang, N.-Y.; Cheng, C.-Y.; Hsieh, C.-L. The History, Mechanism, and Clinical Application of Auricular Therapy in Traditional Chinese Medicine. Evid.-Based Complement. Altern. Med. 2015, 2015, 495684. [Google Scholar] [CrossRef] [Green Version]
- Pesavento, F.; Lovato, A.; Cappello, S.; Postiglione, M. Acupuncture in the treatment of Dry Eye Syndrome with anxiety symptoms. A case report. Eur. J. Transl. Myol. 2022, 32, 10482. [Google Scholar] [CrossRef]
- Lee, J.S.; Hwang, S.H.; Shin, B.C.; Park, Y.M. Electrical stimulation of auricular acupressure for dry eye: A randomized controlled-clinical trial. Chin. J. Integr. Med. 2016, 23, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.; Akl, E.; Brennan, S.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Na, J.; Jung, J.; Park, J.; Song, P.H.; Song, C. Therapeutic effects of acupuncture in typical dry eye: A systematic review and meta-analysis. Acta Ophthalmol. 2020, 99, 489–498. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, P.D.; Collum, L.M.T. Dry eye: Diagnosis and current treatment strategies. Curr. Allergy Asthma Rep. 2004, 4, 314–319. [Google Scholar] [CrossRef]
- Krenzer, K.L.; Dana, M.R.; Ullman, M.D.; Cermak, J.M.; Tolls, D.B.; Evans, J.E.; Sullivan, D.A. Effect of Androgen Deficiency on the Human Meibomian Gland and Ocular Surface1. J. Clin. Endocrinol. Metab. 2000, 85, 4874–4882. [Google Scholar] [CrossRef] [Green Version]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and Validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef]
- van Bijsterveld, O.P. Diagnostic Tests in the Sicca Syndrome. Arch. Ophthalmol. 1969, 82, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Lemp, M.A.; Foulks, G.N. The definition and classification of dry eye disease: Report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007, 5, 75–92. [Google Scholar] [CrossRef]
- Zheng, X.; Zheng, Y.; Zheng, Y.; Zheng, X. Guiding Principles for Clinical Research on New Drug of Traditional Chinese Medicine; China Pharmaceutical Science and Technology Press: Beijing, China, 2002. [Google Scholar]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Schuenemann, H.J.; Tugwell, P.; Knottnerus, A. GRADE guidelines: A new series of articles in the Journal of Clinical Epidemiology. J. Clin. Epidemiol. 2011, 64, 380–382. [Google Scholar] [CrossRef]
- Norris, S.L.; Meerpohl, J.J.; Akl, E.A.; Schünemann, H.J.; Gartlehner, G.; Chen, Y.; Whittington, C. The skills and experience of GRADE methodologists can be assessed with a simple tool. J. Clin. Epidemiology 2016, 79, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef] [PubMed]
- Irwig, L.; Macaskill, P.; Berry, G.; Glasziou, P. Bias in meta-analysis detected by a simple, graphical test. Graphical test is itself biased. BMJ 1998, 316, 470–471. [Google Scholar]
- Liu, X.Q.; Yao, X.Y. Study on the Effect of Auricular Point Pressing Pill in the Treatment of Dry Eye. World Latest Med. Inf. 2021, 21, 237–238. [Google Scholar]
- Li, Q.; Wu, W.J.; Zhang, B.Y. Observation of Auricular–praster Therapy on Dry Eye in Premenopausal Woman. Strait Pharm. J. 2016, 28, 71–73. [Google Scholar]
- Liu, X.M. Effects of Auricular Acupressure Pill Therapy in Dry Eye Patients. Advice Health 2022, 2, 76–84. [Google Scholar]
- Xie, X.F.; Chen, X.H. Application of Auricular Acupuncture Point Pressing Pill Method in the Treatment of Dry Eye. Psychologist 2017, 24, 184–185. [Google Scholar]
- Tang, T.; Xu, J.J.; Wang, F. Treatment of dry eyes with auricular point pressing combined with sodium hyaluronate eye drops: A randomized controlled trial. Mod. Chin. Clin. Med. 2021, 28, 20–23. [Google Scholar]
- Zhang, Y.T.; Chen, Y. Clinical study on menopausal women with severe dry eye treated by Chinese medicine. Chin. J. Tradit. Chin. Ophthalmol. 2017, 27, 315–318. [Google Scholar]
- Kim, B.H.; Kim, M.H.; Kang, S.H.; Nam, H.J. Optimizing acupuncture treatment for dry eye syndrome: A systematic review. BMC Complement. Altern. Med. 2018, 18, 145. [Google Scholar] [CrossRef] [Green Version]
- Schulz, K.F.; Chalmers, I.; Hayes, R.J.; Altman, D.G. Empirical evidence of bias. Dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 1995, 273, 408–412. [Google Scholar] [CrossRef]
- Tierney, J.F.; Stewart, L.A. Investigating patient exclusion bias in meta-analysis. Int. J. Epidemiol. 2005, 34, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Gong, L.; Sun, X.; Chapin, W.J. Clinical Curative Effect of Acupuncture Therapy on Xerophthalmia. Am. J. Chin. Med. 2010, 38, 651–659. [Google Scholar] [CrossRef]
- Wang, H.-Y.; Xu, X.; Li, L.; Ding, C.-Y.; Lu, J.; Zhang, Y.-Y.; Zhang, Y.-F.; Zhang, Y.-L.; Sun, Z.-Q. Moxibustion therapy in Chinese patients with ankylosing spondylitis: A randomized controlled pilot trial. Eur. J. Integr. Med. 2019, 31, 100952. [Google Scholar] [CrossRef]
- Hui, K.K.; Liu, J.; Marina, O.; Napadow, V.; Haselgrove, C.; Kwong, K.K.; Kennedy, D.N.; Makris, N. The integrated response of the human cerebro-cerebellar and limbic systems to acupuncture stimulation at ST 36 as evidenced by fMRI. Neuroimage 2005, 27, 479–496. [Google Scholar] [CrossRef]
- Tan, J.-Y.; Molassiotis, A.; Wang, T.; Suen, L.K.P. Adverse Events of Auricular Therapy: A Systematic Review. Evid.-Based Complement. Altern. Med. 2014, 2014, 506758. [Google Scholar] [CrossRef]
- Yeh, C.H.; Chien, L.-C.; Lin, W.-C.; Bovbjerg, D.H.; van Londen, G. Pilot Randomized Controlled Trial of Auricular Point Acupressure to Manage Symptom Clusters of Pain, Fatigue, and Disturbed Sleep in Breast Cancer Patients. Cancer Nurs. 2016, 39, 402–410. [Google Scholar] [CrossRef]
- Lund, I.; Lundeberg, T. Are minimal, superficial or sham acupuncture procedures acceptable as inert placebo controls? Acupunct. Med. 2006, 24, 13–15. [Google Scholar] [CrossRef]
- Tong, L.; Htoon, H.M.; Hou, A.; Acharya, R.U.; Tan, J.-H.; Wei, Q.-P.; Lim, P. Acupuncture and herbal formulation compared with artificial tears alone: Evaluation of dry eye symptoms and associated tests in randomised clinical trial. BMJ Open Ophthalmol. 2018, 3, e000150. [Google Scholar] [CrossRef]
- Nepp, J.; Tsubota, K.; Goto, E.; Schauersberger, J.; Schild, G.; Jandrasits, K.; Abela, C.; Wedrich, A. The Effect of Acupuncture on the Temperature of the Ocular Surface in Conjunctivitis Sicca Measured by Non-Contact Thermography: Preliminary Results. Adv. Exp. Med. Biol. 2002, 506, 723–726. [Google Scholar] [CrossRef]
- Shi, J.L.; Miao, W.H. [Effects of acupuncture on lactoferrin content in tears and tear secretion in patients suffering from dry eyes: A randomized controlled trial]. Zhong Xi Yi Jie He Xue Bao 2012, 10, 1003–1008. [Google Scholar] [CrossRef]
- Gong, L.; Sun, X. Treatment of Intractable Dry Eyes: Tear Secretion Increase and Morphological Changes of The Lacrimal Gland of Rabbit After Acupuncture. Acupunct. Electro-Ther. Res. 2007, 32, 223–233. [Google Scholar] [CrossRef]
- Liu, C.Y.; Qin, S.; Gao, W.P.; Xi, H.Q.; Xing, X.Y.; Ding, N.; Wei, Q.-B.; Xu, Q. Effect of acupuncture on expression of transfer growth factor-β1 in lacrimal gland of rabbits with dry eye. Zhen Ci Yan Jiu 2020, 45, 726–730. [Google Scholar] [CrossRef]
- Zhang, D.; Zhao, Y.; Yang, Y.-T.; Zhao, Y.; Wu, D.-Y.; Liu, X.-X.; Shi, Z.; Hong, J.; Liu, J.; Ma, X.-P. A Mechanism Study of Electroacupuncture for Dry Eye Syndrome by Targeting Conjunctival Cytokine Expressions. Curr. Eye Res. 2019, 45, 419–427. [Google Scholar] [CrossRef]
- Jones, L.; Downie, L.E.; Korb, D.; Benitez-Del-Castillo, J.M.; Dana, R.; Deng, S.X.; Dong, P.N.; Geerling, G.; Hida, R.Y.; Liu, Y.; et al. TFOS DEWS II Management and Therapy Report. Ocul. Surf. 2017, 15, 575–628. [Google Scholar] [CrossRef]
- Rouen, P.A.; White, M.L. Dry Eye Disease: Prevalence, Assessment, and Management. Home Healthc. Now. 2018, 36, 74–83. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Design | Study (Author, Year, and Country) | Sample Size/ Gender (F:M) | Intervention Group | Control Group | Acupuncture Points | Main Outcomes | AEs |
|---|---|---|---|---|---|---|---|
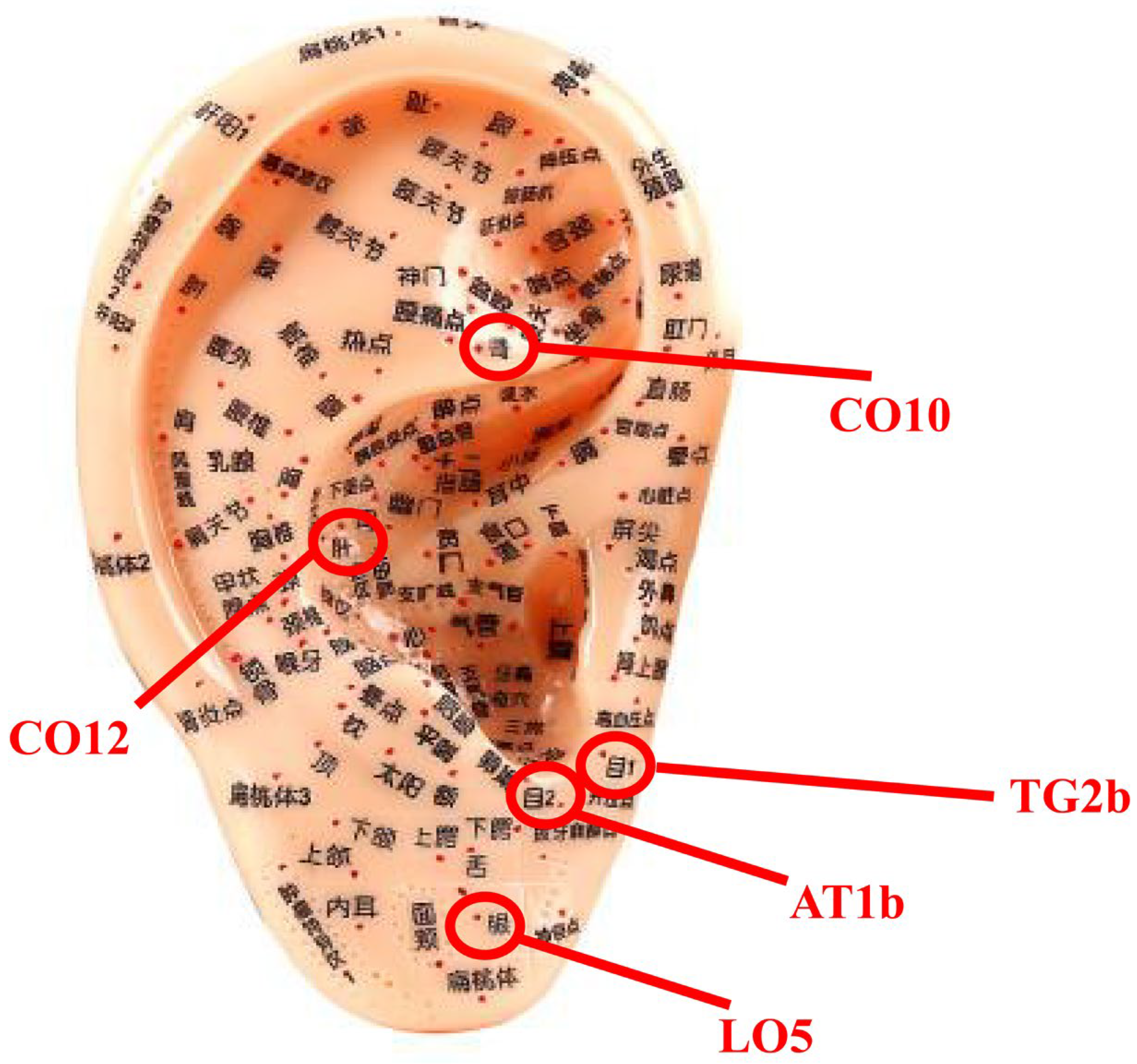
| AA vs. AT | Liu 2021 China [47] | 60 (50:10) | (A) AA (AA for 1 min/time, several times/day, total 2 weeks, n = 30) | (B) AT (one drop or two drops per time, total 2 weeks, n = 30) | Sympathy (AH6a), Kidney (CO10), Liver (CO12), Mu 1 (TG2b), Mu 2 (AT1b) | 1. Tear-film Breakup Time (TBUT) 2. Schirmer I test (SIT) | n.r. |
| Li 2016 China [48] | 46 (46:0) | (A) AA (AA time of each acupuncture point should not be less than 30 s, AA for Deqi/time, total 8 weeks, n = 23) | (B) AT (Polyethylene Glycol Eye Drops: one drop or two drops/time, 4 times/day, total 8 weeks, n = 23) | Kidney (CO10), Liver (CO12), Internal genitalia (TF2), Endocrine (CO18), Pizhixia (AT4), Shenmen (TF4), Eye (LO5), Mu 1 (TG2b), Mu 2 (AT1b) | 1. Tear-film Breakup Time (TBUT) 2. Schirmer I test (SIT) 3. The score of symptoms (SOS) | n.r. | |
| Liu 2022 China [49] | 50 (30:20) | (A) AA (AA for 1~2 min/time, several times/day for Deqi, total 4 weeks, n = 25) | (B) AT (one drop or two drops per time, total 4 weeks, n = 25) | Eye (LO5), Mu 1 (TG2b), Mu 2 (AT1b), Kindy (CO10), Liver (CO12), Spleen (CO12), Stomach (CO4), gallbladder (CO11), Heart (CO15) | 1. Ocular Surface Disease Index (OSDI) 2. Tear-film Breakup Time (TBUT) 3. Schirmer I test (SIT) | n.r. | |
| SAA plus AT vs. AT | Xie 2017 China [50] | 141 (120:21) | (A) AA (AA for 1~2 min/time, several times/day for Deqi, total 4 weeks, n = 72). Plus (B). | (B) AT (one drop or two drops per time, total 4 weeks, n = 69) | Eye (LO5), Mu 1 (TG2b), Mu 2 (AT1b), Kidney (CO10), Liver (CO12), Spleen (CO12), Stomach (CO4), gallbladder (CO11), Heart (CO15) | 1.Response rate 2. Cornea Fluorescein Staining (CFS) | n.r. |
| Tang 2021 China [51] | 120 (66:54) | (A) AA (AA for 1~2 min/time, several times/day for Deqi, total 8 weeks, n = 60). Plus (B). | (B) AT (0.1% Sodium Hyaluronate Eye Drops: one drop or two drops/time, 4 times/day, total 8 weeks, n = 60) | Eye (LO5), Mu 1 (TG2b), Mu 2 (AT1b), Kidney (CO10), Liver (CO12), Spleen (CO12), Stomach (CO4), Endocrine (CO18), Pizhixia (AT4) | 1. Tear-film Breakup Time (TBUT) 2. Schirmer I test (SIT) 3. Cornea Fluorescein Staining (CFS) | n.r. | |
| Zhang 2017 China [52] | 60 (60:0) | (A) AA (AA for 1~2 min/time, 4 times/day, total 2 weeks, n = 30). Plus (B). | (B) AT (0.1% Sodium Hyaluronate Eye Drops: one drop or two drops/time, 4 times/day, total 2 weeks, n = 30) | Mu 1 (TG2b), Mu 2 (AT1b), Kidney (CO10), Liver (CO12), Spleen (CO12) | 1. Tear-film Breakup Time (TBUT) 2. Schirmer I test (SIT) 3. Cornea Fluorescein Staining (CFS) 4.Ocular Surface Disease Index (OSDI) 5. The score of symptoms (SOS) | ||
| AA vs. Sham AA | Lee 2017 Republic of Korea [32] | 100 (78:22) | (A) AA (continuous low-frequency electronic stimulation performed twice a week for 4 weeks for 30 s at each acupuncture point, n = 50). Plus (B). | (B) sham AA (continuous low-frequency electronic stimulation performed twice a week for 4 weeks for 30 s at each non-acupuncture point, n = 50). | Shenmen (TF4), Zero (H1), Liver (CO12), Eye (LO5) | 1. Ocular Surface Disease Index (OSDI) 2. Tear-film Breakup Time (TBUT) 3. Schirmer I test (SIT) | Only 2 participants in the intervention group experienced mild, pricking pain at the auricular acupuncture points. |
| Study Design | Outcomes | Included RCTs/ Participants | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Quality of Evidence |
|---|---|---|---|---|---|---|---|---|
| AA vs. AT | 1. TBUT | 3 RCTs/156 participants | Serious a | Not serious | Not serious | Serious c | undetected | Low |
| 2. SIT | 3 RCTs/156 participants | Serious a | Serious b | Not serious | Serious c | undetected | Very low | |
| AA vs. AA + AT | 1. TBUT | 2 RCTs/180 participants | Serious a | Not serious | Not serious | Serious c | undetected | Low |
| 2. SIT | 2 RCTs/180 participants | Serious a | Not serious | Not serious | Serious c | undetected | Low | |
| 3. CFS | 3 RCTs/321 participants | Serious a | Serious b | Not serious | Serious c | undetected | Very low |
| Variables | Number of Studies | Overall Effects | Heterogeneity | ||
|---|---|---|---|---|---|
| MD | 95% CI | p Value | |||
| AT vs. AA | |||||
| SIT Treatment sessions | I2 = 0 | ||||
| Less than 4 weeks | 2 | 1.88 | [1.27, 2.46] | <0.001 | |
| Over 4 weeks | 1 | 6.99 | [6.21, 7.77] | <0.001 | |
| AT vs. AT + AA | |||||
| CSF Treatment sessions | I2 = 98 | ||||
| Less than 4 weeks | 2 | −0.57 | [−1.82, 0.67] | 0.37 | |
| Over 4 weeks | 1 | −0.07 | [−0.19, 0.05] | 0.25 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Q.; Zhan, M.; Hu, Z. Auricular Acupressure for Dry Eye Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Medicina 2023, 59, 177. https://doi.org/10.3390/medicina59010177
Huang Q, Zhan M, Hu Z. Auricular Acupressure for Dry Eye Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Medicina. 2023; 59(1):177. https://doi.org/10.3390/medicina59010177
Chicago/Turabian StyleHuang, Qiong, Mengqi Zhan, and Zhe Hu. 2023. "Auricular Acupressure for Dry Eye Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Medicina 59, no. 1: 177. https://doi.org/10.3390/medicina59010177