
Randomized Clinical Trial Comparing Insertion Torque and Implant Stability of Two Different Implant Macrogeometries in the Initial Periods of Osseointegration

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
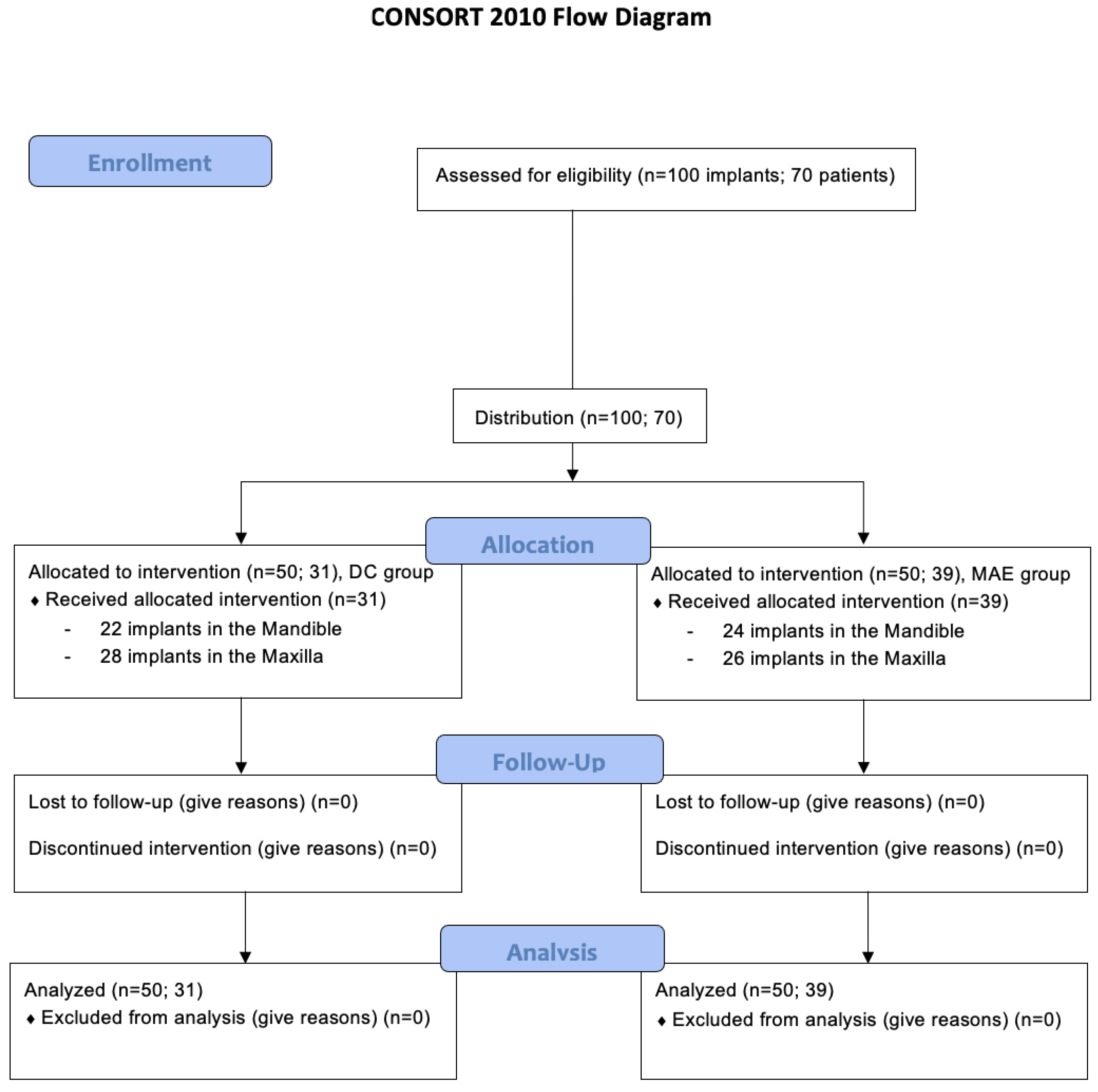
2.1. Patient Population and Distribution
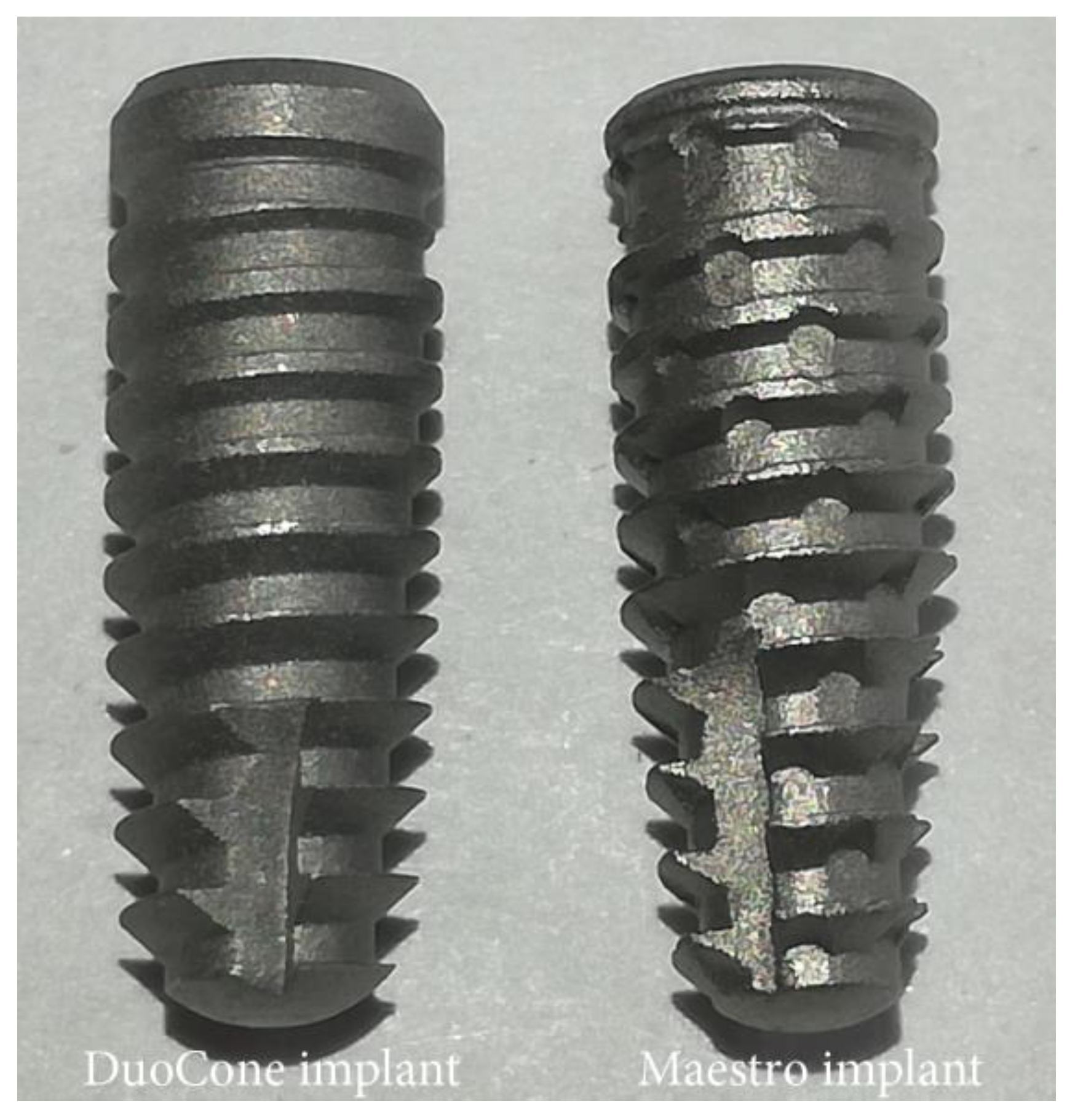
2.2. Implant Macrogeometries and Surface Treatment
2.3. Experimental Design
2.4. Surgical Procedure
2.5. Statistical Analysis
3. Results
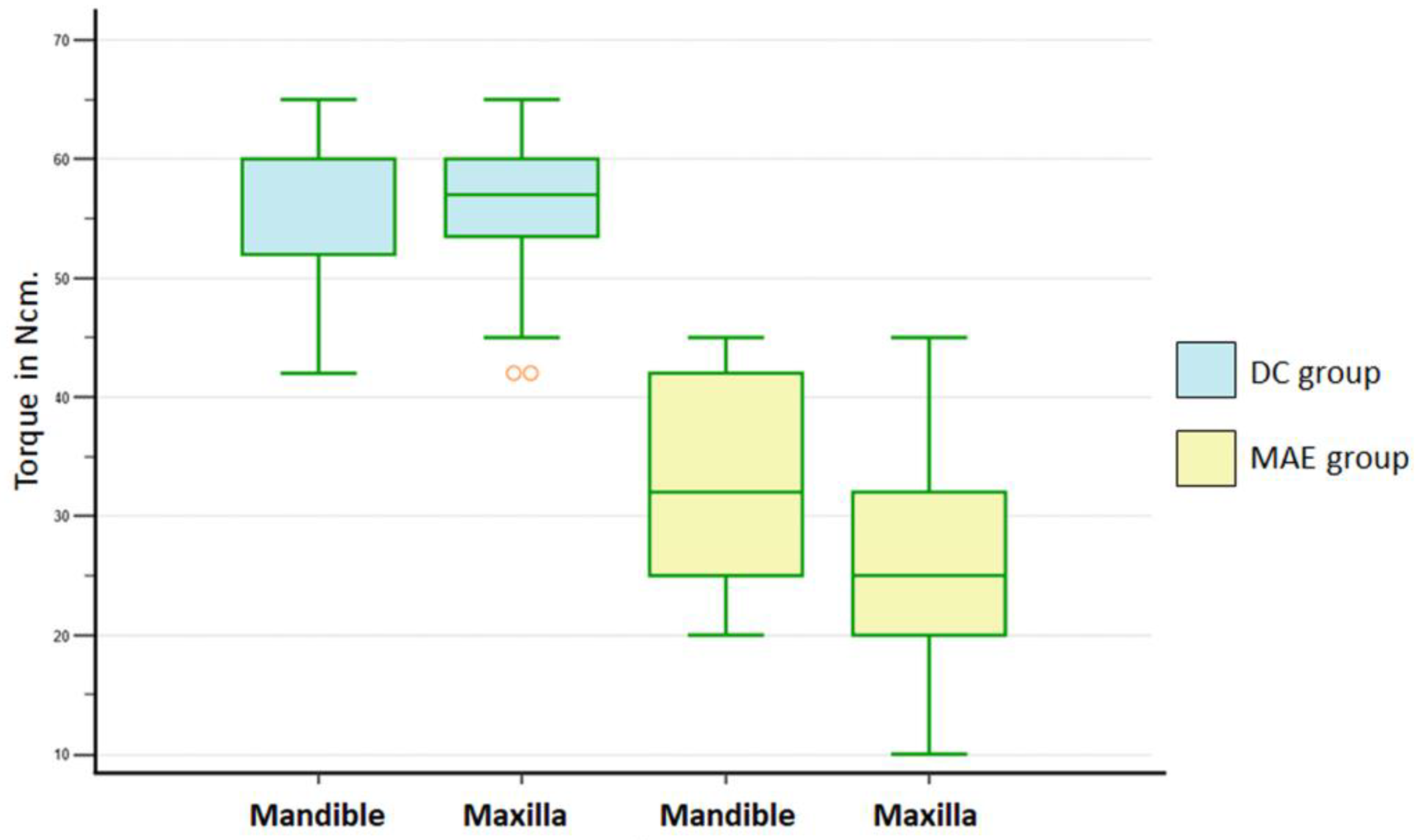
3.1. Insertion Torque Values
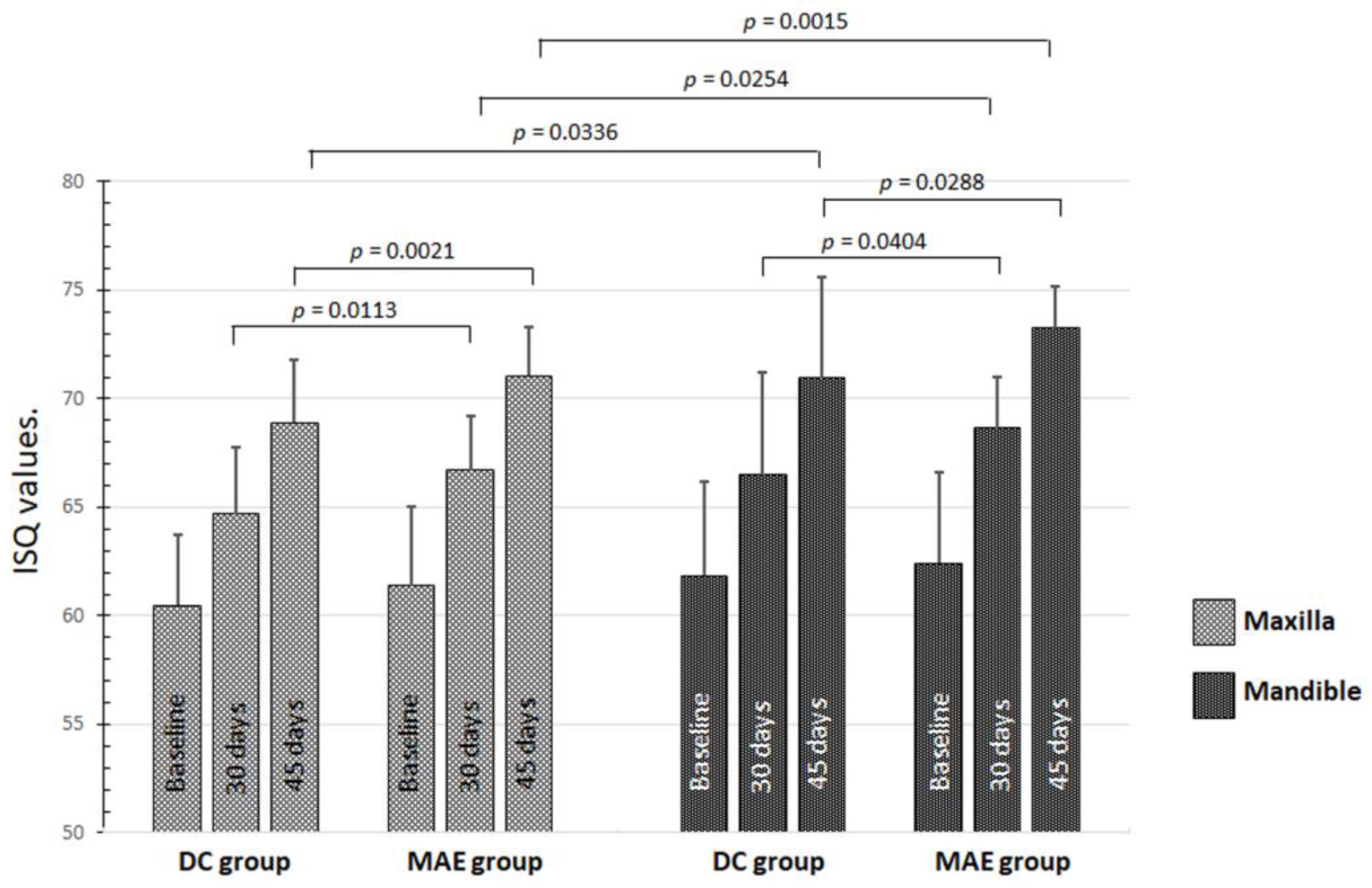
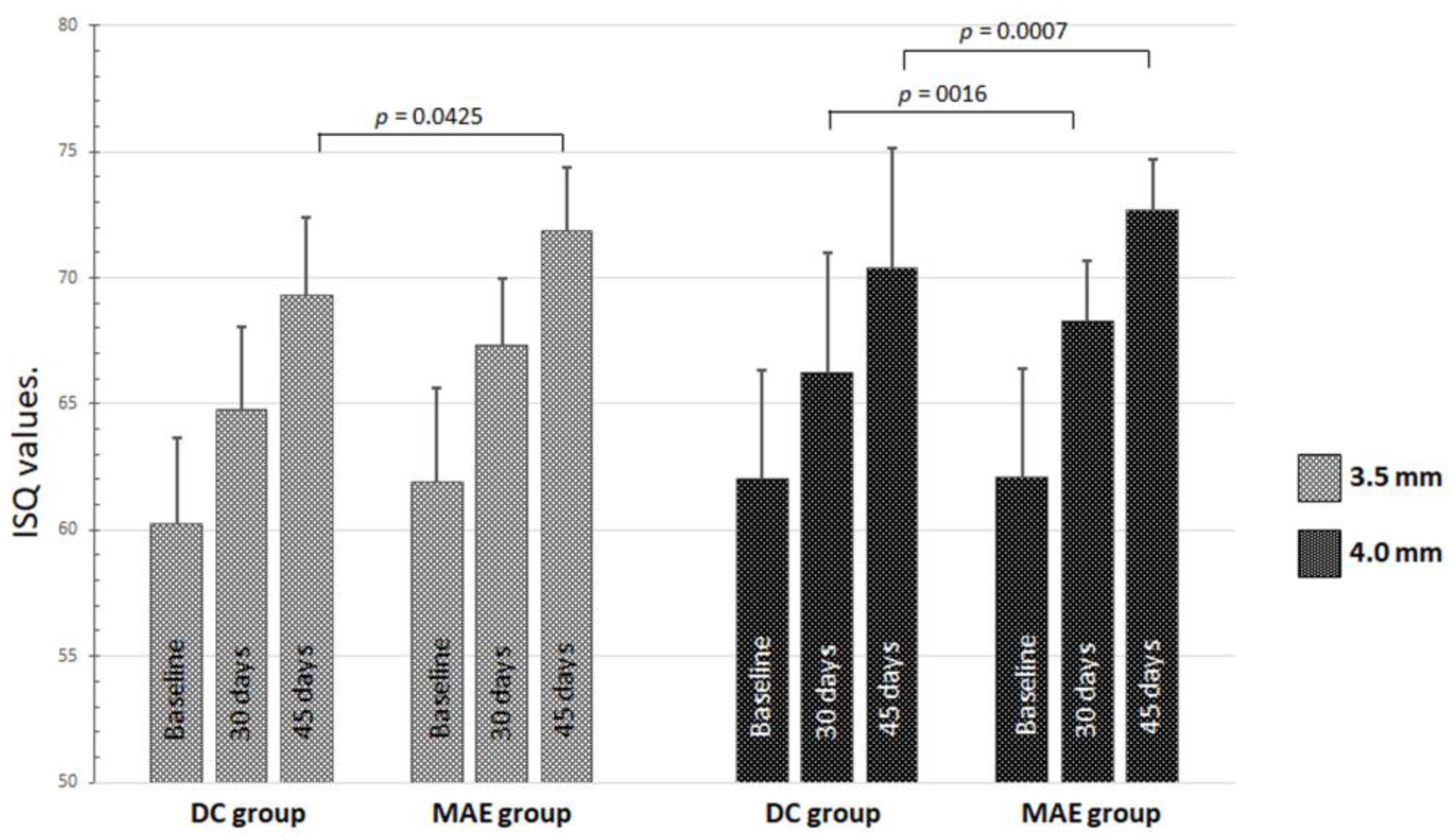
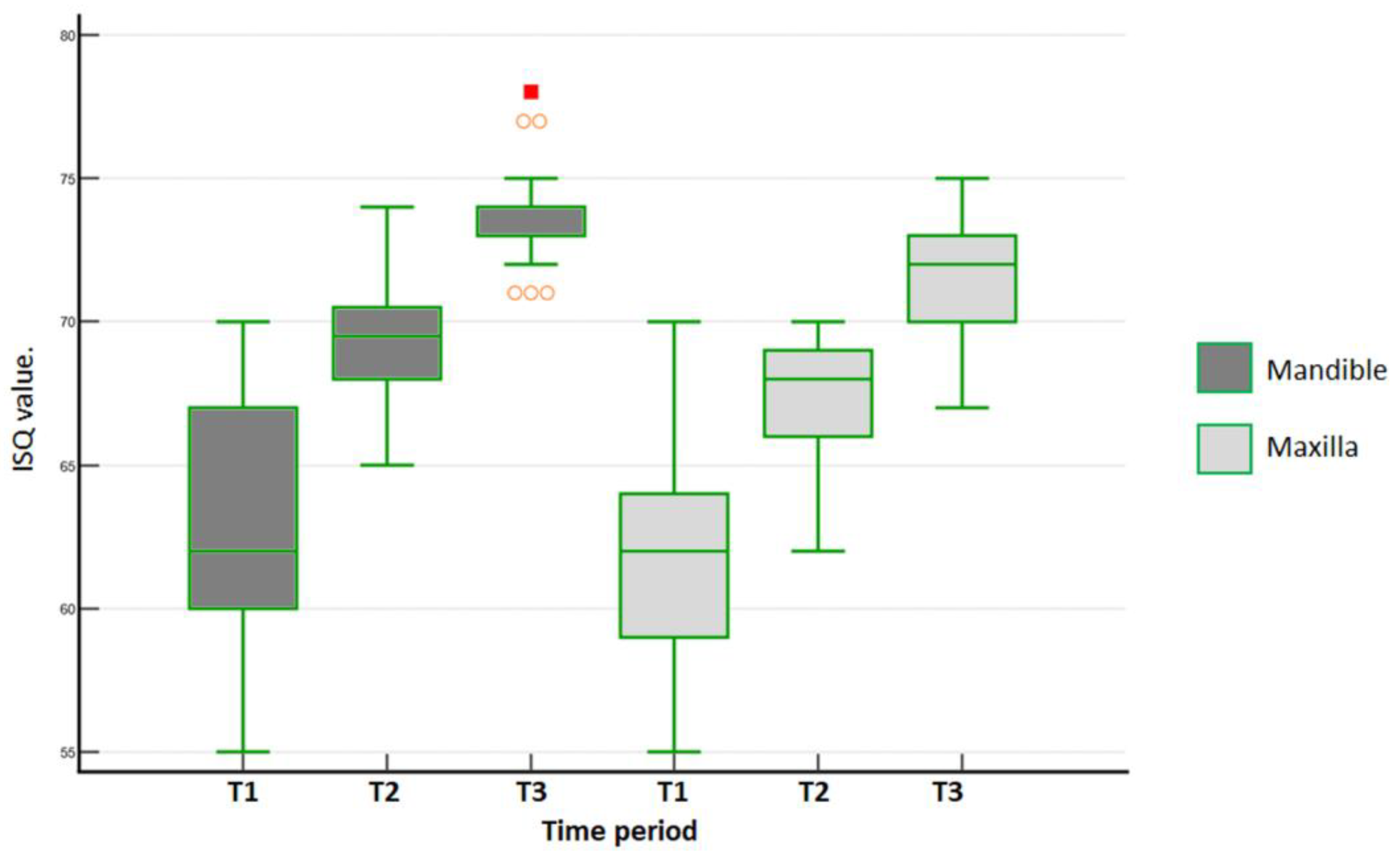
3.2. ISQ Values
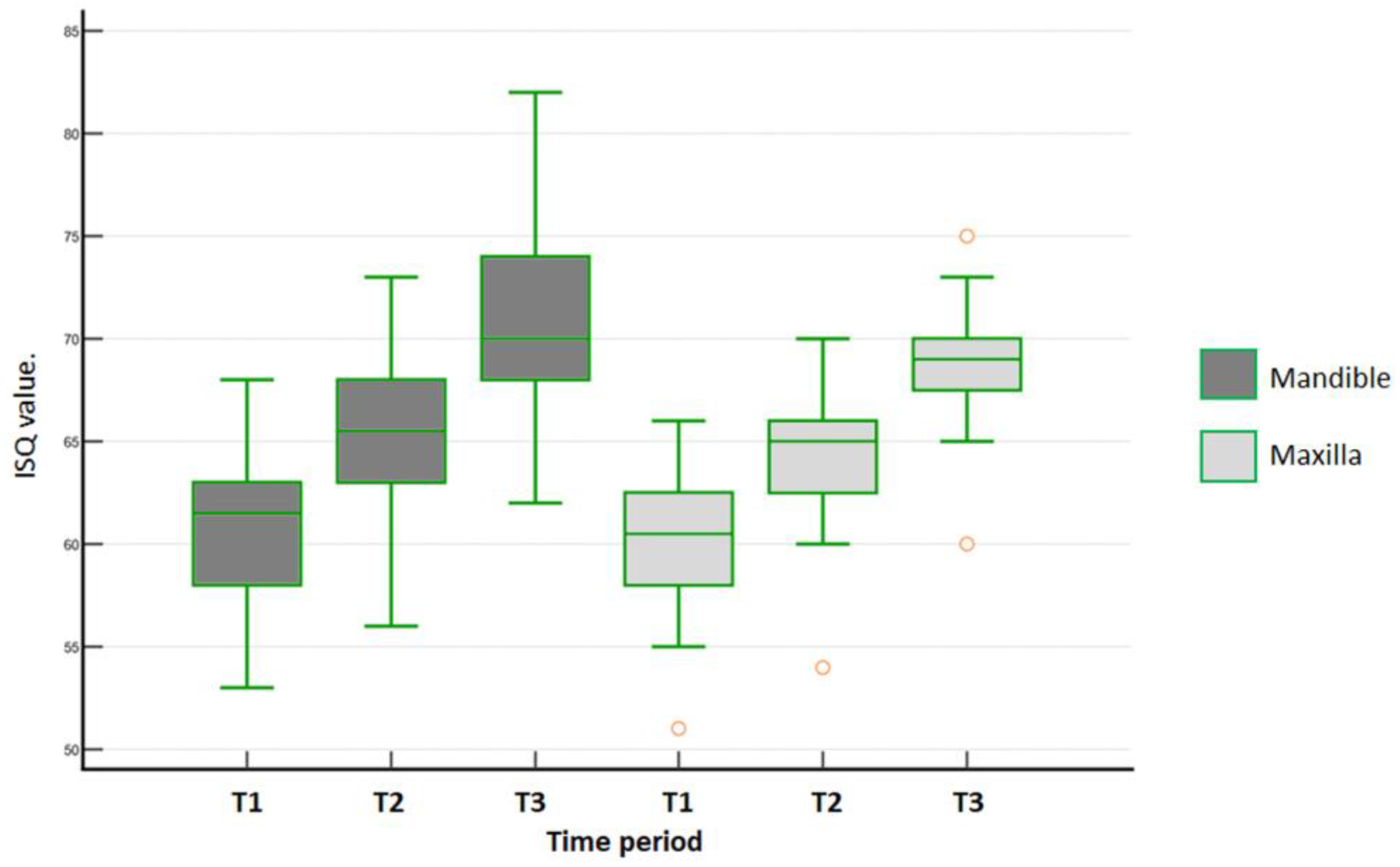
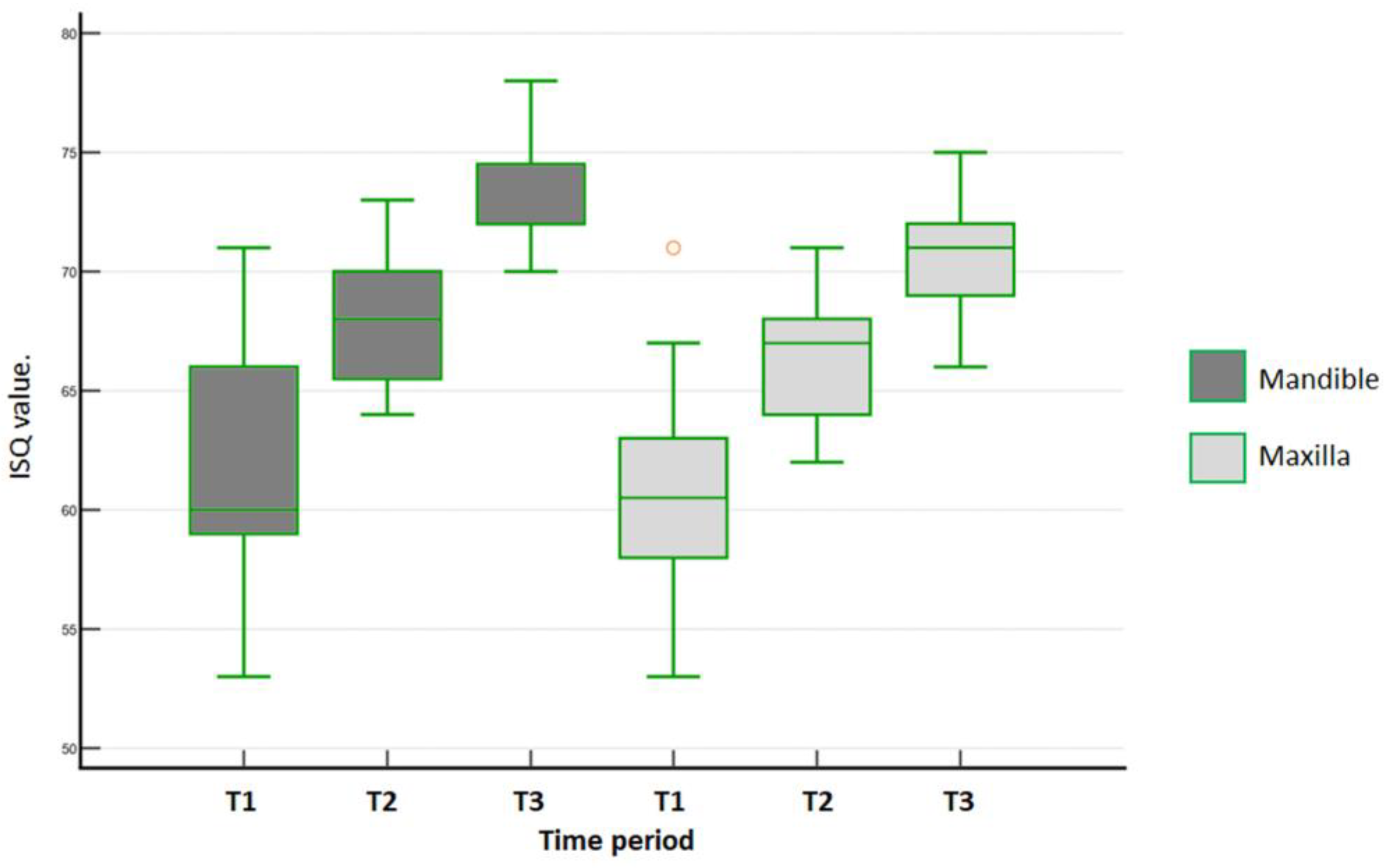
3.3. B-L ISQ Values of Mandible and Maxilla
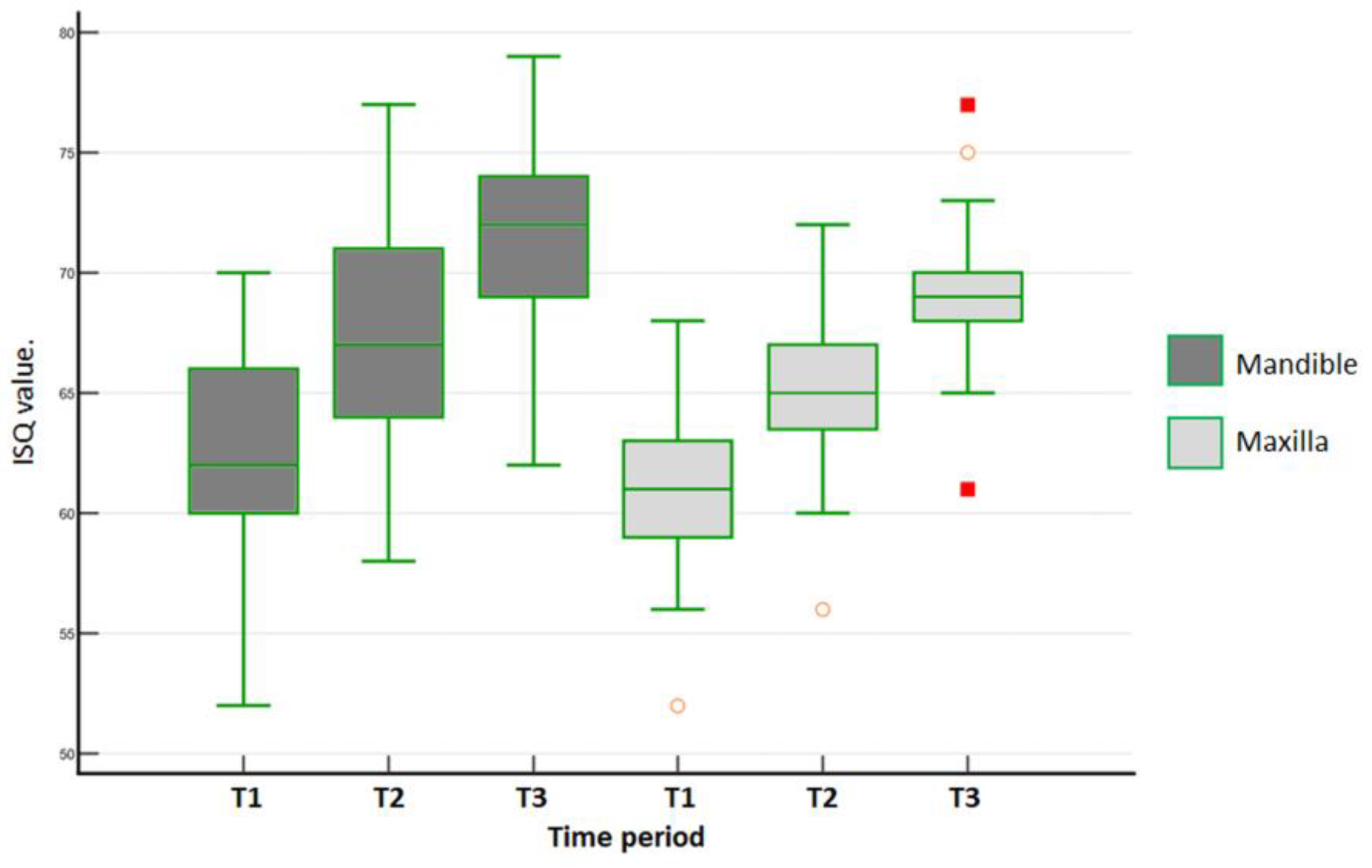
3.4. M-D ISQ Values of Mandible and Maxilla
3.5. Multiple Linear Regression for Dependent Variable
3.6. Correlations between ITV and ISQ over Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, H.C.; Tsai, P.I.; Huang, C.C.; Chen, S.Y.; Chao, C.G.; Tsou, N.T. Numerical Method for the Design of Healing Chamber in Additive-Manufactured Dental Implants. BioMed Res. Int. 2017, 2017, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gehrke, S.A.; Aramburú, J.; Pérez-Díaz, L.; do Prado, T.D.; Dedavid, B.A.; Mazon, P.; De Aza, P.N. Can changes in implant macrogeometry accelerate the osseointegration process?: An in vivo experimental biomechanical and histological evaluations. PLoS ONE 2020, 15, e0233304. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, S.A. Characteristics of Implant Systems That Can Accelerate and Improve the Osseointegration Process. In Current Concepts in Dental Implantology—From Science to Clinical Research; Gabrić, D., Vuletić, M., Eds.; IntechOpen: London, UK, 2022; Available online: https://www.intechopen.com/chapters/79241 (accessed on 1 December 2022).
- Falco, A.; Berardini, M.; Trisi, P. Correlation Between Implant Geometry, Implant Surface, Insertion Torque, and Primary Stability: In Vitro Biomechanical Analysis. Int. J. Oral Maxillofac. Implants 2018, 33, 824–830. [Google Scholar] [CrossRef]
- Eom, T.G.; Kim, H.W.; Jeon, G.R.; Yun, M.J.; Huh, J.B.; Jeong, C.M. Effects of different implant osteotomy preparation sizes on implant stability and bone response in the Minipig mandible. Int. J. Oral Maxillofac. Implants 2016, 31, 997–1006. [Google Scholar] [CrossRef]
- Marin, C.; Bonfante, E.; Granato, R.; Neiva, R.; Gil, L.F.; Marão, H.F.; Suzuki, M.; Coelho, P.G. The effect of osteotomy dimension on implant insertion torque, healing mode, and osseointegration indicators: A study in dogs. Implant Dent. 2016, 25, 739–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Zhang, Y.; Miron, R.J. Health, Maintenance, and Recovery of Soft Tissues around Implants. Clin. Implant Dent. Relat. Res. 2016, 18, 618–634. [Google Scholar] [CrossRef]
- Choi, J.Y.; Sim, J.H.; Yeo, I.L. Characteristics of contact and distance osteogenesis around modified implant surfaces in rabbit tibiae. J. Periodontal Implant Sci. 2017, 47, 182–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebenezer, S.; Kumar, V.V.; Thor, A. Basics of Dental Implantology for the Oral Surgeon. In Oral and Maxillofacial Surgery for the Clinician; Bonanthaya, K., Panneerselvam, E., Manuel, S., Kumar, V.V., Rai, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2021; pp. 385–405. [Google Scholar] [CrossRef]
- Kuzyk, P.R.; Schemitsch, E.H. The basic science of peri-implant bone healing. Indian J. Orthop. 2011, 45, 108–115. [Google Scholar] [CrossRef]
- Bergamo, E.T.; Zahoui, A.; Barrera, R.B.; Huwais, S.; Coelho, P.G.; Karateew, E.D.; Bonfante, E.A. Osseodensification effect on implants primary and secondary stability: Multicenter controlled clinical trial. Clin. Implant Dent. Relat. Res. 2021, 23, 317–328. [Google Scholar] [CrossRef]
- Stacchi, C.; Troiano, G.; Montaruli, G.; Mozzati, M.; Lamazza, L.; Antonelli, A.; Giudice, A.; Lombardi, T. Changes in Implant Stability Using Different Site Preparation Techniques: Osseodensification Drills versus Piezoelectric Surgery. A Multi-Center Prospective Randomized Controlled Clinical Trial. Clin. Implant Dent. Relat. Res. 2022; Online ahead of print. [Google Scholar] [CrossRef]
- Bavetta, G.; Bavetta, G.; Randazzo, V.; Cavataio, A.; Paderni, C.; Grassia, V.; Dipalma, G.; Isacco, C.G.; Scarano, A.; De Vito, D.; et al. A Retrospective Study on Insertion Torque and Implant Stability Quotient (ISQ) as Stability Parameters for Immediate Loading of Implants in Fresh Extraction Sockets. BioMed Res. Int. 2019, 2019, 9720419. [Google Scholar] [CrossRef] [Green Version]
- Saridakis, S.K.; Wagner, W.; Noelken, R. Retrospective cohort study of a tapered implant with high primary stability in patients with local and systemic risk factors-7-year data. Int. J. Implant Dent. 2018, 4, 41. [Google Scholar] [CrossRef] [PubMed]
- Heinemann, F.; Hasan, I.; Bourauel, C.; Biffar, R.; Mundt, T. Bone stability around dental implants: Treatment related factors. Ann. Anat. 2015, 199, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, S.A.; Scarano, A.; de Lima, J.H.; Bianchini, M.A.; Dedavid, B.A.; De Aza, P.N. Effects of the Healing Chambers in Implant Macrogeometry Design in a Low-Density Bone Using Conventional and Undersized Drilling. J. Int. Soc. Prev. Community Dent. 2021, 11, 437–447. [Google Scholar]
- Di Stefano, D.A.; Arosio, P.; Capparè, P.; Barbon, S.; Gherlone, E.F. Stability of Dental Implants and Thickness of Cortical Bone: Clinical Research and Future Perspectives. A Systematic Review. Materials 2021, 14, 7183. [Google Scholar] [CrossRef] [PubMed]
- Attanasio, F.; Antonelli, A.; Brancaccio, Y.; Averta, F.; Figliuzzi, M.M.; Fortunato, L.; Giudice, A. Primary Stability of Three Different Osteotomy Techniques in Medullary Bone: An In Vitro Study. Dent. J. 2020, 8, 21. [Google Scholar] [CrossRef] [Green Version]
- Yu, X.; Chang, C.; Guo, W.; Wu, Y.; Zhou, W.; Yu, D. Primary implant stability based on alternative site preparation techniques: A systematic review and meta-analysis. Clin. Implant Dent. Relat. Res. 2022, 24, 580–590. [Google Scholar] [CrossRef]
- Ivanova, V.; Chenchev, I.; Zlatev, S.; Mijiritsky, E. Correlation between Primary, Secondary Stability, Bone Density, Percentage of Vital Bone Formation and Implant Size. Int. J. Environ. Res. Public Health 2021, 18, 6994. [Google Scholar] [CrossRef] [PubMed]
- Niu, Y.; Wang, Z.; Shi, Y.; Dong, L.; Wang, C. Modulating macrophage activities to promote endogenous bone regeneration: Biological mechanisms and engineering approaches. Bioact. Mater. 2020, 6, 244–261. [Google Scholar] [CrossRef]
- Brouwers, J.E.I.G.; Buis, S.; de Groot, P.G.; de Laat, B.; Remijn, J.A. Resonance frequency analysis with two different devices after conventional implant placement with ridge preservation: A prospective pilot cohort study. Clin. Implant Dent. Relat. Res. 2021, 23, 789–799. [Google Scholar] [CrossRef]
- Becker, W.; Hujoel, P.; Becker, B.E. Resonance frequency analysis: Comparing two clinical instruments. Clin. Implant Dent. Relat. Res. 2018, 20, 308–312. [Google Scholar] [CrossRef]
- Díaz-Sánchez, R.M.; Delgado-Muñoz, J.M.; Hita-Iglesias, P.; Pullen, K.T.; Serrera-Figallo, M.Á.; Torres-Lagares, D. Improvement in the Initial Implant Stability Quotient Through Use of a Modified Surgical Technique. J. Oral Implantol. 2017, 43, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, S.A.; da Silva Neto, U.T.; Rossetti, P.H.O.; Watinaga, S.E.; Giro, G.; Shibli, J.A. Stability of implants placed in fresh sockets versus healed alveolar sites: Early findings. Clin. Oral Implant Res. 2016, 27, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Osstell Instructions. Available online: https://www.osstell.com/de/clinical-guidelines/die-isq-skala/ (accessed on 1 December 2022).
- Martins, B.G.S.; Fernandes, J.C.H.; Martins, A.G.; de Moraes Castilho, R.; de Oliveira Fernandes, G.V. Surgical and Nonsurgical Treatment Protocols for Peri-implantitis: An Overview of Systematic Reviews. Int. J. Oral Maxillofac. Implant 2022, 37, 660–676. [Google Scholar] [CrossRef] [PubMed]
- Kensy, J.; Dobrzyński, M.; Wiench, R.; Grzech-Leśniak, K.; Matys, J. Fibroblasts Adhesion to Laser-Modified Titanium Surfaces—A Systematic Review. Materials 2021, 14, 7305. [Google Scholar] [CrossRef]
- Butera, A.; Maiorani, C.; Gallo, S.; Pascadopoli, M.; Venugopal, A.; Marya, A.; Scribante, A. Evaluation of Adjuvant Systems in Non-Surgical Peri-Implant Treatment: A Literature Review. Healthcare 2022, 10, 886. [Google Scholar] [CrossRef]
- Gehrke, S.A.; da Silva, U.T.; Del Fabbro, M. Does Implant Design Affect Implant Primary Stability? A Resonance Frequency Analysis-Based Randomized Split-Mouth Clinical Trial. J. Oral Implantol. 2015, 41, e281–e286. [Google Scholar] [CrossRef] [Green Version]
- Staedt, H.; Palarie, V.; Staedt, A.; Wolf, J.M.; Lehmann, K.M.; Ottl, P.; Kämmerer, P.W. Primary Stability of Cylindrical and Conical Dental Implants in Relation to Insertion Torque-A Comparative Ex Vivo Evaluation. Implant Dent. 2017, 26, 250–255. [Google Scholar] [CrossRef]
- Sugiura, T.; Yamamoto, K.; Horita, S.; Murakami, K.; Kirita, T. Evaluation of Primary Stability of Cylindrical and Tapered Implants in Different Bone Types by Measuring Implant Displacement: An In vitro Study. Contemp. Clin. Dent. 2019, 10, 471–476. [Google Scholar] [CrossRef]
- Baires-Campos, F.E.; Jimbo, R.; Bonfante, E.A.; Fonseca-Oliveira, M.T.; Moura, C.; Zanetta-Barbosa, D.; Coelho, P.G. Drilling dimension effects in early stages of osseointegration and implant stability in a canine model. Med. Oral Patol. Oral Cir. Bucal 2015, 20, e471–e479. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Júnior, J.A.; Treichel, T.L.E.; do Prado, T.D.; Dedavid, B.A.; de Aza, P.N. Effects of insertion torque values on the marginal bone loss of dental implants installed in sheep mandibles. Sci. Rep. 2022, 12, 538. [Google Scholar] [CrossRef]
- Lozano-Carrascal, N.; Salomó-Coll, O.; Gilabert-Cerdà, M.; Farré-Pagés, N.; Gargallo-Albiol, J.; Hernández-Alfaro, F. Effect of implant macro-design on primary stability: A prospective clinical study. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e214–e221. [Google Scholar] [CrossRef] [PubMed]
- Triches, D.F.; Alonso, F.R.; Mezzomo, L.A.; Schneider, D.R.; Villarinho, E.A.; Rockenbach, M.I.; Teixeira, E.R.; Shinkai, R.S. Relation between insertion torque and tactile, visual, and rescaled gray value measures of bone quality: A cross-sectional clinical study with short implants. Int. J. Implant Dent. 2019, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Baldi, D.; Lombardi, T.; Colombo, J.; Cervino, G.; Perinetti, G.; Di Lenarda, R.; Stacchi, C. Correlation between Insertion Torque and Implant Stability Quotient in Tapered Implants with Knife-Edge Thread Design. BioMed Res. Int. 2018, 2018, 7201093. [Google Scholar] [CrossRef]
- Satwalekar, P.; Nalla, S.; Reddy, R.; Chowdary, S.G. Clinical evaluation of osseointegration using resonance frequency analysis. J. Indian Prosthodont. Soc. 2015, 15, 192–199. [Google Scholar] [CrossRef]
- Dewi, R.S.; Odang, R.W.; Odelia, L. Osseointegration of Dental Implants in Macaca Fascicularis. In Journal of Physics: Conference Series; IOP Publishing: Bristol, UK, 2017; Volume 884. [Google Scholar] [CrossRef]
- Açil, Y.; Sievers, J.; Gülses, A.; Ayna, M.; Wiltfang, J.; Terheyden, H. Correlation between resonance frequency, insertion torque and bone-implant contact in self-cutting threaded implants. Odontology 2017, 105, 347–353. [Google Scholar] [CrossRef]
- Bilhan, H.; Geckili, O.; Mumcu, E.; Bozdag, E.; Sünbüloğlu, E.; Kutay, O. Influence of surgical technique, implant shape and diameter on the primary stability in cancellous bone. J. Oral Rehabil. 2010, 37, 900–907. [Google Scholar] [CrossRef]
- Hong, J.; Lim, Y.J.; Park, S.O. Quantitative biomechanical analysis of the influence of the cortical bone and implant length on primary stability. Clin. Oral Implant Res. 2012, 23, 1193–1197. [Google Scholar] [CrossRef]
- Bedrossian, E. Do Dental Implant Width and Length Matter? Compend. Contin. Educ. Dent. 2020, 41, e1–e5. [Google Scholar]
- Huang, H.; Wu, G.; Hunziker, E. The clinical significance of implant stability quotient (ISQ) measurements: A literature review. J. Oral Biol. Craniofac. Res. 2020, 10, 629–638. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Bercianos, M.; Aguerrondo, J.G.; Calvo-Guirado, J.L.; Prados-Frutos, J.C. Influence of Mucosal Thickness, Implant Dimensions and Stability in Cone Morse Implant Installed at Subcrestal Bone Level on the Peri-Implant Bone: A Prospective Clinical and Radiographic Study. Symmetry 2019, 11, 1138. [Google Scholar] [CrossRef] [Green Version]
- Gupta, G. Implant Stability Quotient (ISQ): A Reliable Guide for Implant Treatment. In Current Concepts in Dental Implantology—From Science to Clinical Research; Gabrić, D., Vuletić, M., Eds.; IntechOpen: London, UK, 2022; Available online: https://www.intechopen.com/chapters/79724 (accessed on 1 December 2022). [CrossRef]
- Gahona, O.; Granic, X.; Antunez, C.; Domancic, S.; Díaz-Narváez, V.; Utsman, R. Insertion torque and resonance frequency analysis (ISQ) as predictor methods of Implant osseointegration. J. Osseointegr. 2018, 10, 103–107. [Google Scholar]
- Gehrke, S.A.; da Silva Neto, U.T. Does the time of osseointegration in the maxilla and mandible differ? J. Craniofac. Surg. 2014, 25, 2117–2120. [Google Scholar] [CrossRef] [PubMed]
- Öztürk, K.; Kış, H.C. Peri-implant bone microstructural analysis and comparison of resonance frequency analysis before prosthetic placement: A retrospective study. Clin. Oral Investig. 2022, 26, 4967–4975. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.Y.; Shin, S.I.; Kye, S.B.; Chang, S.W.; Hong, J.; Paeng, J.Y.; Yang, S.M. Bone cement grafting increases implant primary stability in circumferential cortical bone defects. J. Periodontal Implant Sci. 2015, 45, 30–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lages, F.S.; Douglas-de Oliveira, D.W.; Costa, F.O. Relationship between implant stability measurements obtained by insertion torque and resonance frequency analysis: A systematic review. Clin. Implant Dent. Relat. Res. 2018, 20, 26–33. [Google Scholar] [CrossRef]
- do Vale Souza, J.P.; de Moraes Melo Neto, C.L.; Piacenza, L.T.; da Silva, E.V.F.; de Melo Moreno, A.L.; Penitente, P.A.; Brunetto, J.L.; Dos Santos, D.M.; Goiato, M.C. Relation Between Insertion Torque and Implant Stability Quotient: A Clinical Study. Eur. J. Dent. 2021, 15, 618–623. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surgical Site Condition | ||||||
|---|---|---|---|---|---|---|
| DuoCone (DC Group) | Maestro (MAE Group) | |||||
| Number of patients (total) | 31 | 39 | ||||
| Number of implants (total) | 50 | 50 | ||||
| Maxilla (per implant) | ||||||
| diameter | ||||||
| 3.5 mm | 7 | 5 | ||||
| 4.0 mm | 21 | 21 | ||||
| Length | ||||||
| 9 mm | 2 | 10 | ||||
| 11 mm | 17 | 14 | ||||
| 13 mm | 9 | 2 | ||||
| Mandible (per implant) | ||||||
| diameter | ||||||
| 3.5 mm | 15 | 16 | ||||
| 4.0 mm | 7 | 8 | ||||
| Length | ||||||
| 9 mm | 20 | 21 | ||||
| 11 mm | 2 | 3 | ||||
| 13 mm | 0 | 0 | ||||
| Maxilla (ISQ values) | T1 | T2 | T3 | T1 | T2 | T3 |
| Mean | 60.5 | 64.7 | 68.9 | 61.4 | 66.7 | 71.1 |
| SD | 3.25 | 3.09 | 2.88 | 3.67 | 2.51 | 2.27 |
| no. of implants ISQ ≤ 60 | 13 | 2 | 0 | 10 | 0 | 0 |
| no. of implants ISQ 60–65 | 14 | 15 | 2 | 12 | 7 | 0 |
| no. of implants ISQ 65–70 | 1 | 10 | 20 | 3 | 19 | 8 |
| no. of implants ISQ > 70 | 0 | 1 | 6 | 1 | 0 | 18 |
| Mandible (ISQ values) | T1 | T2 | T3 | T1 | T2 | T3 |
| Mean | 61.9 | 66.5 | 71.0 | 62.4 | 68.7 | 73.3 |
| SD | 4.33 | 4.71 | 4.65 | 4.19 | 2.33 | 2.94 |
| no. of implants ISQ < 60 | 6 | 2 | 0 | 8 | 0 | 0 |
| no. of implants ISQ 60–65 | 11 | 6 | 3 | 7 | 2 | 0 |
| no. of implants ISQ 65–70 | 5 | 9 | 5 | 8 | 18 | 0 |
| no. of implants ISQ > 70 | 0 | 5 | 14 | 1 | 4 | 24 |
| DuoCone | Maestro | |||
|---|---|---|---|---|
| Maxilla | Mandible | Maxilla | Mandible | |
| Mean | 56.21 a | 56.72 c | 25.30 a,b | 33.62 b,c |
| SD | 6.27 | 6.71 | 8.58 | 8.97 |
| 95% CI | 53.78–58.64 | 53.75–59.60 | 21.83–28.77 | 29.83–37.41 |
| Insertion Torque | ISQ Bucco-Lingual | ISQ Mesio-Distal | ||||
|---|---|---|---|---|---|---|
| Baseline | 30 Days | 45 Days | Baseline | 30 Days | 45 Days | |
| ITV DC maxilla | 0.32 | 0.34 | 0.34 | 0.35 | 0.35 | 0.36 |
| ITV DC mandible | −0.07 | 0.008 | −0.14 | −0.03 | −0.07 | −0.1 |
| ITV MAE maxilla | 0.24 | 0.16 | −0.01 | 0.27 | 0.01 | −0.04 |
| ITV MAE mandible | −0.12 | −0.06 | −0.22 | −0.10 | −0.22 | −0.08 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gehrke, S.A.; Cortellari, G.C.; de Oliveira Fernandes, G.V.; Scarano, A.; Martins, R.G.; Cançado, R.M.; Mesquita, A.M.M. Randomized Clinical Trial Comparing Insertion Torque and Implant Stability of Two Different Implant Macrogeometries in the Initial Periods of Osseointegration. Medicina 2023, 59, 168. https://doi.org/10.3390/medicina59010168
Gehrke SA, Cortellari GC, de Oliveira Fernandes GV, Scarano A, Martins RG, Cançado RM, Mesquita AMM. Randomized Clinical Trial Comparing Insertion Torque and Implant Stability of Two Different Implant Macrogeometries in the Initial Periods of Osseointegration. Medicina. 2023; 59(1):168. https://doi.org/10.3390/medicina59010168
Chicago/Turabian StyleGehrke, Sergio Alexandre, Guillermo Castro Cortellari, Gustavo Vicentis de Oliveira Fernandes, Antonio Scarano, Rafael Garcia Martins, Renata Moreira Cançado, and Alfredo Mikail Melo Mesquita. 2023. "Randomized Clinical Trial Comparing Insertion Torque and Implant Stability of Two Different Implant Macrogeometries in the Initial Periods of Osseointegration" Medicina 59, no. 1: 168. https://doi.org/10.3390/medicina59010168