
Cancer-Oriented Comprehensive Nursing Services in Republic of Korea: Lessons from an Oncologist’s Perspective
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Participant Selection and Data Collection
2.3. Measurements
2.3.1. Structure
2.3.2. Process
2.3.3. Patient/Nurse Outcome
2.4. Statistical Analysis
3. Results
3.1. Structure
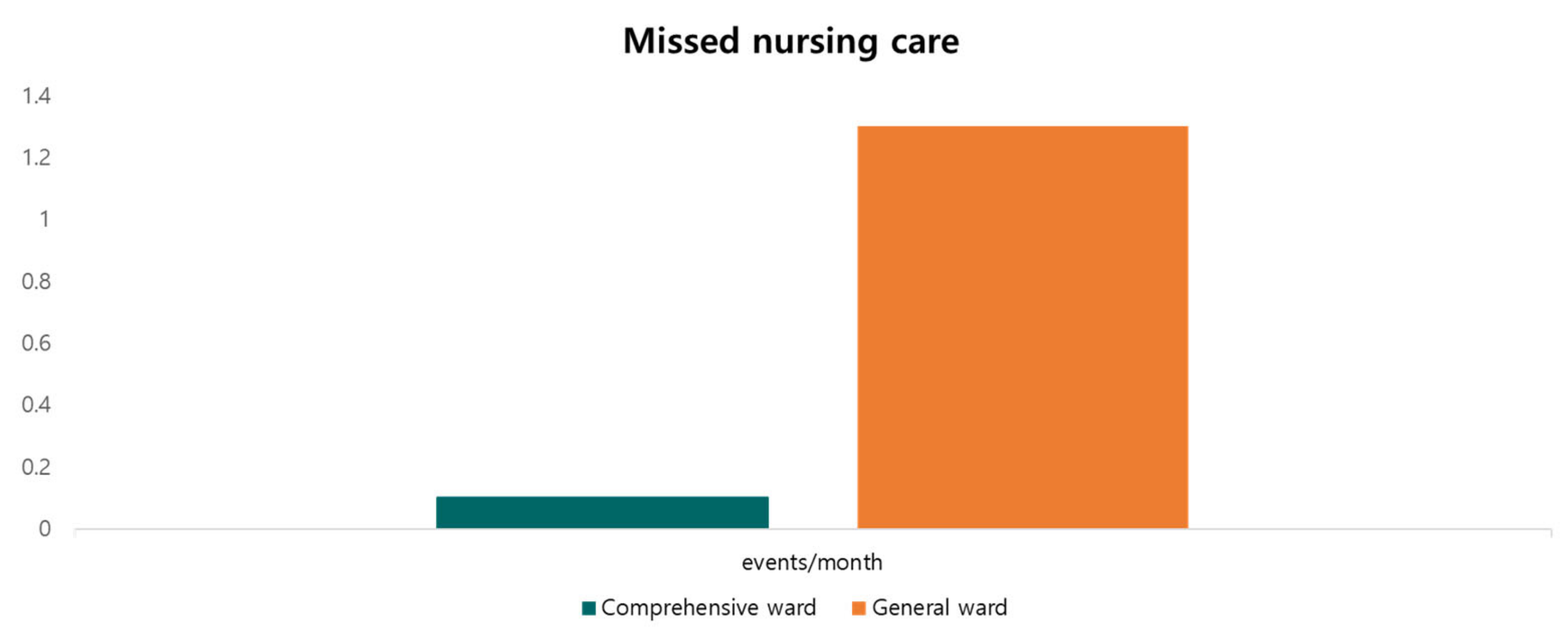
3.2. Process
3.3. Outcomes
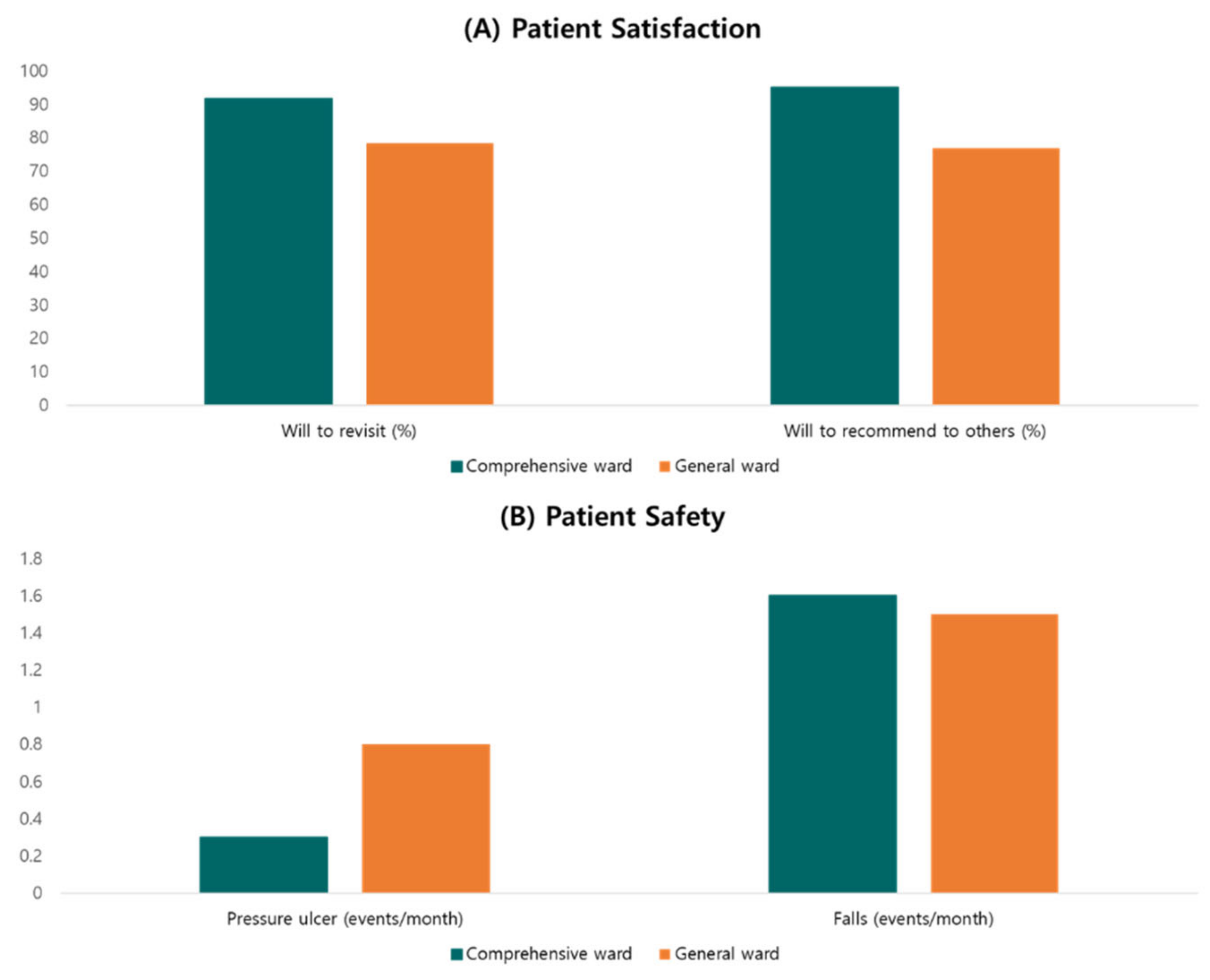
3.3.1. Patient Outcome
3.3.2. Nurse Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, J.; Kim, S.; Park, E.; Jeong, S.; Lee, E. Policy Issues and New Direction for Comprehensive Nursing Service in the National Health Insurance. J. Korean Acad. Nurs. Adm. 2017, 23, 312–322. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Yu, S.; Kim, M.; Kim, H. Impact of South Korea’s Comprehensive Nursing Service Policy on Nurse and Patient Outcomes. Healthcare 2020, 8, 223. [Google Scholar] [CrossRef] [PubMed]
- Park, K.-O.; Yu, M.; Kim, J.-K. Experience of Nurses Participating in Comprehensive Nursing Care. J. Korean Acad. Nurs. Adm. 2017, 23, 76–89. [Google Scholar] [CrossRef] [Green Version]
- You, S.-J.; Choi, Y.-K. Institutionalization of a Patient-Sitter Program in Acute Care Hospitals. J. Korea Contents Assoc. 2013, 13, 370–379. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Choi, H.S. Research Trends in Korea on Integrated Nursing Care Service: A Scoping Review. Korean J. Adult Nurs. 2020, 32, 455–471. [Google Scholar] [CrossRef]
- Policy Direction of Comprehensive Nursing Care. Available online: http://www.nhis.or.kr/bbs7/boards/B0040/21012 (accessed on 2 December 2022).
- Shin, S.-R.; Park, K.-Y. Comparing Satisfaction with Nursing Care and Factors Relevant to Hospital Revisit Intent among Hospitalized Patients in Comprehensive Nursing Care Units and General Care Units. J. Korean Acad. Nurs. Adm. 2015, 21, 469–479. [Google Scholar] [CrossRef] [Green Version]
- Park, J.H.; Lee, M.H. Effects of Nursing and Care = Giving Integrated Service on nursing work performance, nurses’ job satisfaction and patient safety. J. Korean Acad. Soc. Home Care Nurs. 2017, 24, 14–22. [Google Scholar]
- Bang, M.R.; Sim, S.S.; Lee, D.-S. Comparison of Patient-Sitter Ward Nurses and General Ward Nurses on Work-Related Musculoskeletal Symptoms, Occupational Stress and Nursing Work Environments. J. Korean Biol. Nurs. Sci. 2015, 17, 169–178. [Google Scholar] [CrossRef] [Green Version]
- Lim, H.-S.; Song, E.J. Influences of Emotional Labor, Hardiness on Job Satisfaction of Nurses in Comprehensive Nursing Care Service Units. J. Korea Acad. Ind. Coop. Soc. 2020, 21, 65–72. [Google Scholar]
- Kim, S.-E.; Han, J.-Y. Clinical Nurses’ Job Stress, Emotional labor, Nursing Performance, and Burnout in Comprehensive Nursing Care Service Wards and General Wards. J. Korean Acad. Nurs. Adm. 2017, 23, 336–345. [Google Scholar] [CrossRef]
- Donabedian, A. An Introduction to Quality Assurance in Health Care; Oxford University Press: Oxford, UK, 2002. [Google Scholar]
- Recio-Saucedo, A.; Dall’Ora, C.; Maruotti, A.; Ball, J.; Briggs, J.; Meredith, P.; Redfern, O.C.; Kovacs, C.; Prytherch, D.; Smith, G.B.; et al. What impact does nursing care left undone have on patient outcomes? Review of the literature. J. Clin. Nurs. 2018, 27, 2248–2259. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.-A.; Gong, S.-W.; Cho, S.-J. Relationship among Nursing Service Quality, Medical Service Satisfaction, and Hospital Revisit Intent. J. Korean Acad. Nurs. Adm. 2012, 18, 96–105. [Google Scholar] [CrossRef]
- Parasuraman, A.; Zeithaml, V.A.; Berry, L.L. Reassessment of Expectations as a Comparison Standard in Measuring Service Quality: Implications for Further Research. J. Mark. 1994, 58, 111–124. [Google Scholar] [CrossRef] [Green Version]
- Weiss, D.J.; Dawis, R.V.; England, G.W.; Lofquist, L.H. Manual for the Minnesota Satisfaction Questionnaire. In Minnesota Studies in Vocational Rehabilitation; University of Minnesota, Industrial Relations Center: Minneapolis, MN, USA, 1967. [Google Scholar]
- Park, I.J. A Validation Study of the Minnesota Satisfaction Questionnaire (MSQ). Unpublished. Master’s Thesis, University of Minnesota, Minneapolis, MN, USA, 2005. [Google Scholar]
- Stamps, P.L.; Piedmont, E.B.; Slavitt, D.B.; Haase, A.M. Measurement of Work Satisfaction among Health Professionals. Med. Care 1978, 16, 337–352. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.R. Influential Factors on Turnover Intention of Nurses: The Effect of Nurse’s Organizational Commitment and Career Commitment to Turnover Intention; Ewha Woman’s University: Seoul, Republic of Korea, 2007. [Google Scholar]
- Mobley, W.H. Employee Turnover: Causes, Consequences, and Control; Addison-Wesley Publishing Co.: Reading, UK, 1982. [Google Scholar]
- Deribe, B.; Ayalew, M.; Geleta, D.; Gemechu, L.; Bogale, N.; Mengistu, K.; Gadissa, A.; Dula, D.; Ababi, G.; Gebretsadik, A. Perceived Quality of Nursing Care Among Cancer Patients Attending Hawassa University Comprehensive Specialized Hospital Cancer Treatment Center; Hawassa Southern Ethiopia: Cross-Sectional Study. Cancer Manag. Res. 2021, 13, 1225–1231. [Google Scholar] [CrossRef]
- The Lancet Oncology. The importance of nurses in cancer care. Lancet Oncol. 2015, 16, 737. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.H.; Kang, H.Y. Job satisfaction, job stress, burnout, and turnover intention of comprehensive nursing care service ward nurses and general ward nurses. J. Korea Acad. Ind. Coop. Soc. 2018, 19, 459–469. [Google Scholar]
- Jung, Y.A.; Sung, K.M. A Comparison of Patients’ Nursing Service Satisfaction, Hospital Commitment and Revisit Intention between General Care Unit and Comprehensive Nursing Care Unit. J. Korean Acad. Nurs. Adm. 2018, 24, 30–39. [Google Scholar] [CrossRef] [Green Version]
- Yeun, Y.-R. Effects of Comprehensive Nursing Service on the Nursing Performance, Job Satisfaction and Customer Orientation among Nurses. J. Korea Acad. Ind. Coop. Soc. 2015, 16, 317–323. [Google Scholar] [CrossRef] [Green Version]
- Shim, O.S.; Lee, H.J. A comparative study on the job satisfaction, nursing professionalism and nursing work environment of nurses in comparative nursing care service wards and nurses in general wards. J. Converg. Inform. Technol. 2017, 7, 25–33. [Google Scholar]
- Aiken, L.H.; Sloane, D.M.; Bruyneel, L.; Van den Heede, K.; Griffiths, P.; Busse, R.; Diomidous, M.; Kinnunen, J.; Kózka, M.; Lesaffre, E.; et al. Nurse staffing and education and hospital mortality in nine European countries: A retrospective observational study. Lancet 2014, 383, 1824–1830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, B.; Lee, K.-S.; Park, Y.-K.; Choi, Y.-A.; Cho, S.-M.; Kim, S.-Y.; Han, G.-Y.; Shim, M. A Study of Nurses’ Perception of the Comprehensive Nursing Service. Korean J. Fam. Pract. 2017, 7, 99–104. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Category | Facilities and Equipment | Purpose | ||
|---|---|---|---|---|
| General Ward | Comprehensive Ward | |||
| Ward | Auxiliary nurse station per team | None | A table with one PC * per team | Proximity nursing |
| Patient lounge | Shared and small | More spacious | Providing comfortable space | |
| Corridor surveillance cameras | Same | Incident/accident monitoring | ||
| Corridor guard rail | In compliance with government regulations | Twice as protective as required per the regulations | Fall prevention | |
| Patient room | Interval between beds | 1.5 m | 2 m | Infection prevention |
| Emergency call bell per bed | Same | Fall prevention | ||
| Mat with fall prevention sensor | None | Yes | ||
| Electric bed with remote control | Beds in private rooms only | All of the beds | Patient convenience | |
| Air mattress | None | Yes | Bedsore prevention | |
| Sink per room | Same | Infection prevention | ||
| Alcohol-rub dispenser per bed | Same | |||
| Toilet in room | Beds in OB/GYN ** ward and private rooms | About 30% of beds | Patient convenience | |
| Shower room | Beds in private rooms only | About 30% of beds | ||
| Medical equipment | Wheelchair, walker | In compliance with the government regulations | More than 1.5 times as many as required per the regulations | Fall prevention |
| Mobile toilet | None | Yes | Sanitary nursing | |
| Shampoo aid | None | Yes | ||
| Bath bed | None | Yes | ||
| Oxygen monitor | In compliance with the government regulations | Twice as many as required per the regulations | Vital sign measurement | |
| Non-invasive sphygmomanometer | In compliance with the government regulations | Twice as many as required per the regulations | ||
| Bladder scan | Same | Residual urine check | ||
| Various and detailed patient information | Handout only | Handout and video guide | Educating patients and visiting guardians | |
| Characteristic | Comprehensive Nursing Ward (n = 52) | General Ward (n = 50) | p |
|---|---|---|---|
| n (%) or M ± SD * | n (%) or M ± SD | ||
| Age (years, range) | 62.38 ± 11.17 (19–86) | 62.62 ± 10.22 (38–84) | 0.84 |
| Sex | |||
| Male | 32 (61.5%) | 30 (60%) | 0.87 |
| Female | 20 (38.5%) | 20 (40%) | |
| Living status | |||
| Living with family | 27 (75%) | 34 (82.9%) | 0.39 |
| Living alone | 9 (25%) | 7 (17.1%) | |
| ECOG PS ** | |||
| 0–1 | 43 (82.7%) | 38 (76%) | 0.32 |
| 2 | 5 (9.6%) | 6 (12%) | |
| 3 | 3 (5.8%) | 2 (4%) | |
| 4 | 1 (1.9%) | 4 (8%) | |
| Length of stay (days, range) | 9.98 ± 4.51 (2–29) | 10.50 ± 6.40 (3–33) | 0.56 |
| Reason for admission | 0.33 | ||
| Elective | 44 (88%) | 39 (78%) | |
| Emergency | 8 (12%) | 11 (22%) | |
| Cancer stage (solid tumor) | |||
| I-II | 10 (25.0%) | 7 (14.6%) | 0.22 |
| III-IV | 30 (75.0%) | 41 (85.4%) | |
| Cancer type | 0.78 | ||
| Breast | 12 (23.1%) | 9 (18.0%) | |
| Colorectal | 15 (28.9%) | 16 (32.0%) | |
| Hepatobiliary/Pancreatic | 3 (5.8%) | 4 (8.0%) | |
| Lung | 6 (11.5%) | 6 (12.0%) | |
| Stomach | 2 (3.9%) | 5 (10.0%) | |
| Hematologic malignancies | 13 (25.0%) | 7 (14.0%) | |
| Others | 1 (1.8%) | 3 (6.0%) | |
| Nursing requirement severity | |||
| I-II | 51 (98.1%) | 44 (88%) | 0.06 |
| III-IV | 1 (1.9%) | 6 (12%) |
| Characteristic | Comprehensive Nursing Ward (n = 52) | General Ward (n = 50) | p |
|---|---|---|---|
| Score *, M ± SD ** | Score, M ± SD | ||
| Physical satisfaction | 4.32 ± 0.66 | 4.02 ± 0.71 | <0.01 |
| Therapeutic satisfaction | 4.33 ± 0.69 | 4.09 ± 0.66 | <0.01 |
| Environmental satisfaction | 4.41 ± 0.70 | 3.95 ± 0.77 | <0.01 |
| Emotional satisfaction | 4.39 ± 0.66 | 3.99 ± 0.75 | <0.01 |
| Informational satisfaction | 4.29 ± 0.69 | 3.97 ± 0.88 | <0.01 |
| Characteristic | Comprehensive Nursing Ward (n = 23) | General Ward (n = 19) | p |
|---|---|---|---|
| Score *, M ± SD ** | Score, M ± SD | ||
| Job satisfaction | 3.54 ± 0.33 | 3.09 ± 0.55 | <0.01 |
| Turnover intention | 3.10 ± 0.51 | 3.87 ± 0.49 | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ha, S.H.; Kim, M.; Kim, H.; No, B.; Go, A.; Choi, M.; Lee, S.; Ahn, Y. Cancer-Oriented Comprehensive Nursing Services in Republic of Korea: Lessons from an Oncologist’s Perspective. Medicina 2023, 59, 144. https://doi.org/10.3390/medicina59010144
Ha SH, Kim M, Kim H, No B, Go A, Choi M, Lee S, Ahn Y. Cancer-Oriented Comprehensive Nursing Services in Republic of Korea: Lessons from an Oncologist’s Perspective. Medicina. 2023; 59(1):144. https://doi.org/10.3390/medicina59010144
Chicago/Turabian StyleHa, Suk Hun, Moonho Kim, Hyojin Kim, Boram No, Ara Go, Miso Choi, Seol Lee, and Yongchel Ahn. 2023. "Cancer-Oriented Comprehensive Nursing Services in Republic of Korea: Lessons from an Oncologist’s Perspective" Medicina 59, no. 1: 144. https://doi.org/10.3390/medicina59010144