
Fetal Growth Restriction and Clinical Parameters of Newborns from HIV-Infected Romanian Women
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
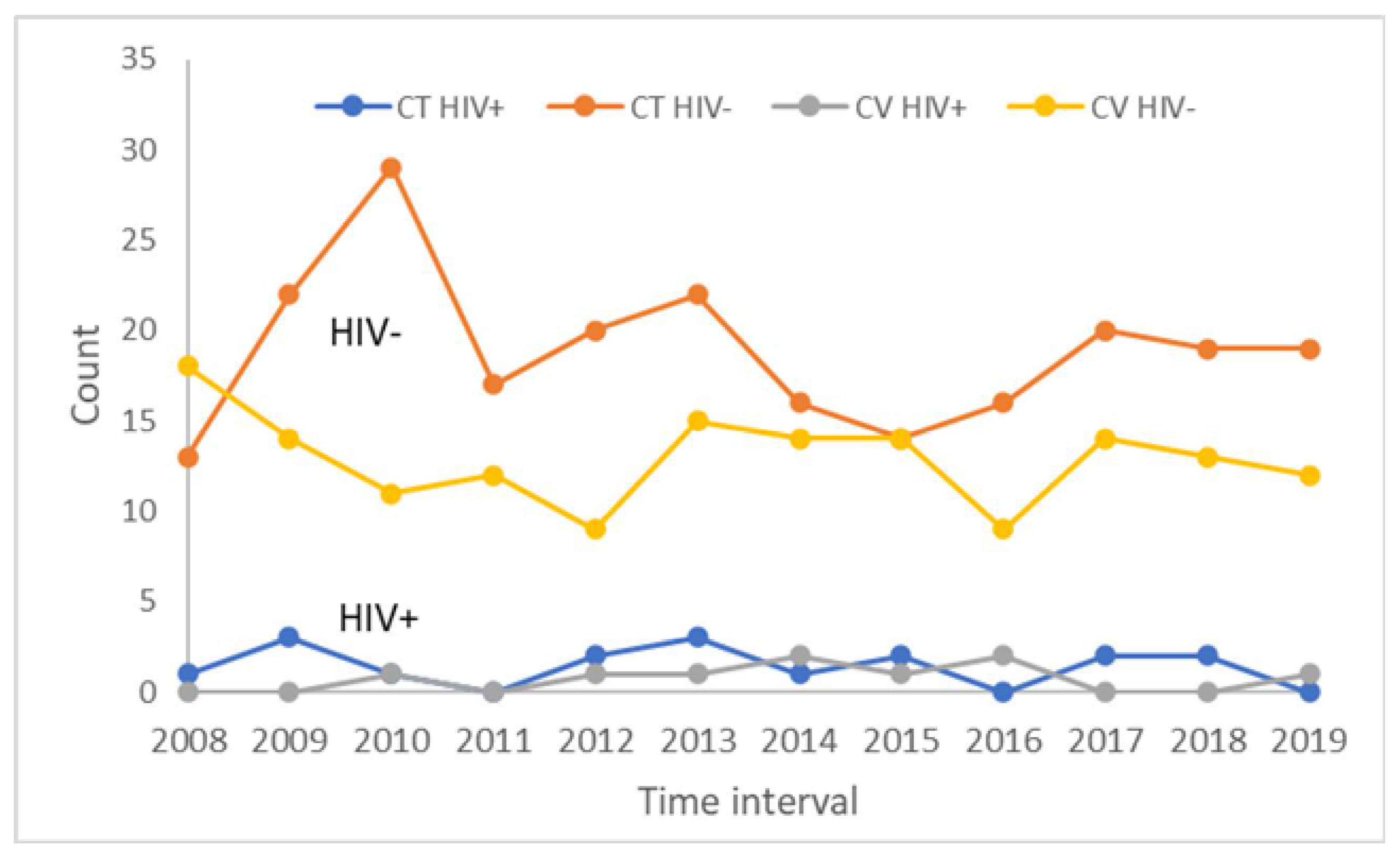
3.1. HIV Transmissibility Rates to Newborns
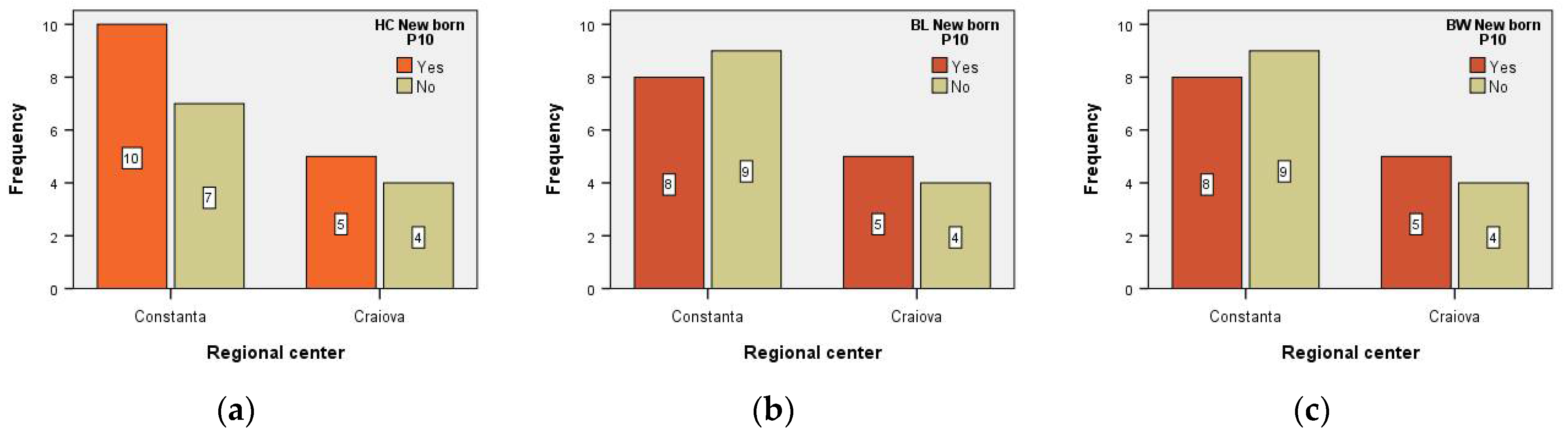
3.2. Clinical and Anthropometrical Parameters of HIV-Positive Newborns
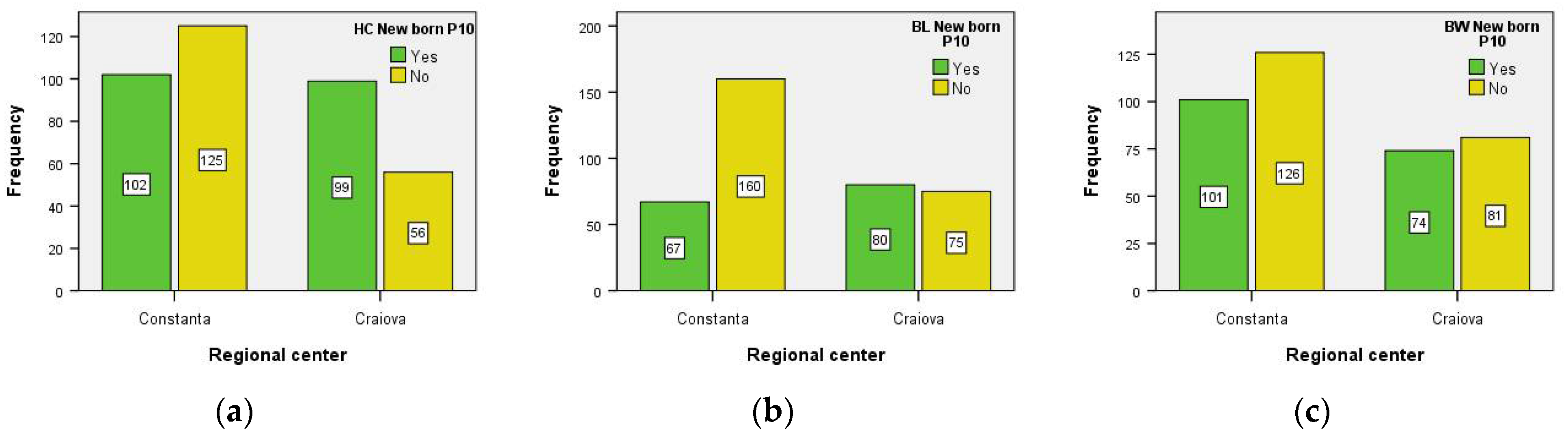
3.3. Clinical and Anthropometrical Parameters of HIV-Negative Newborns
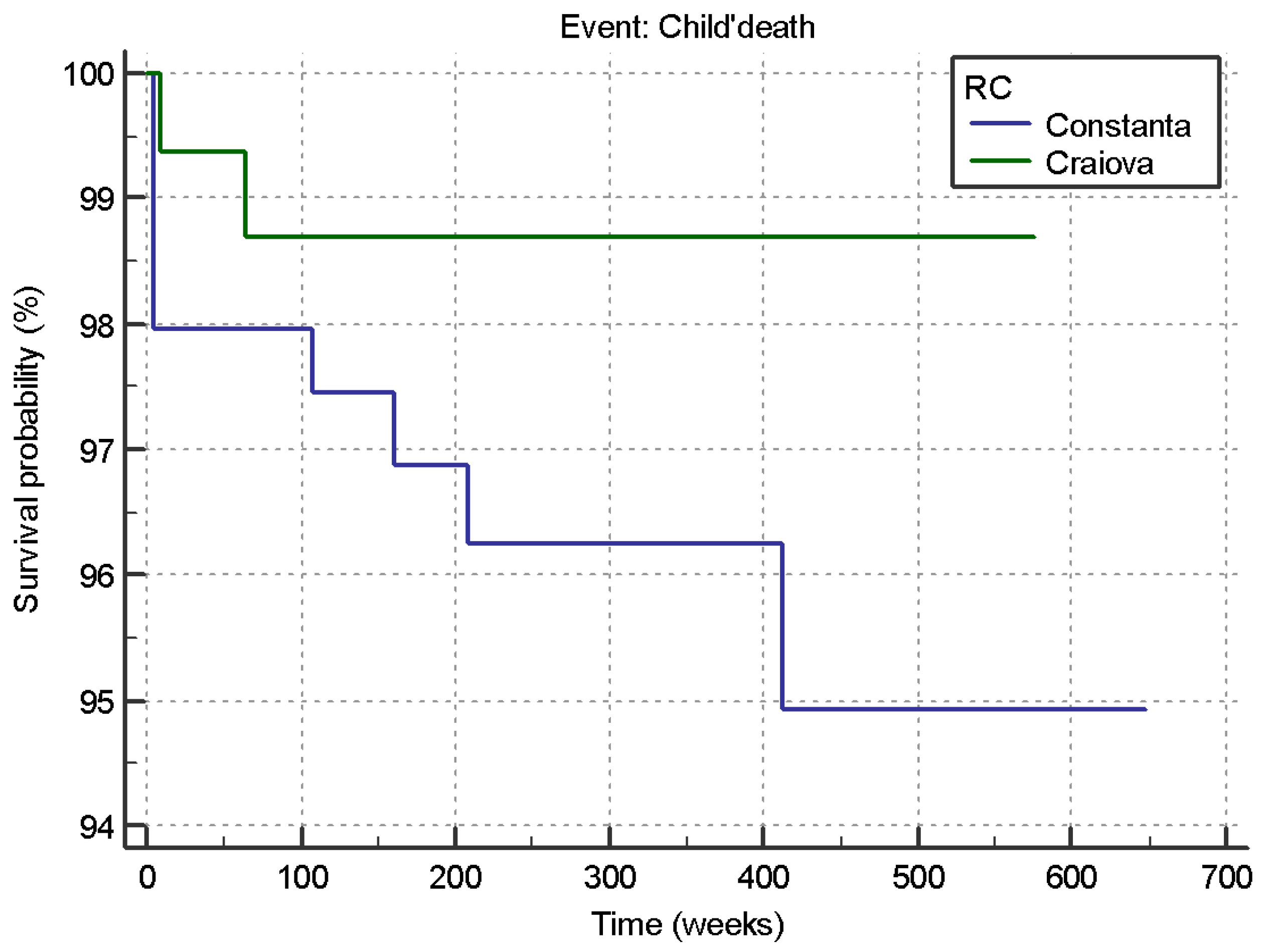
3.4. Survival of HIV-Positive Newborns
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Romanian Academy ‘Stefan S. Nicolau’ Institute of Virology. Available online: https://www.virology.ro/en/research/hiv-aids/highlights.html (accessed on 28 October 2022).
- Department for Monitoring and Evaluation of HIV/AIDS Infection in Romania, National Institute of Infectious Diseases ‘Prof.Dr. Matei Bals’. Available online: https://www.cnlas.ro/images/doc/01122022.pdf (accessed on 12 October 2022).
- Padyana, M.; Bhat, R.V.; Dinesha; Nawaz, A. HIV in Females: A Clinico-epidemiological Study. J. Fam. Med. Prim. Care 2013, 2, 149–152. [Google Scholar] [CrossRef]
- Deeks, S.; Tracy, R.; Douek, D. Systemic effects of inflammation on health during chronic HIV infection. Immunity 2013, 39, 633–645. [Google Scholar] [CrossRef] [Green Version]
- Ørbæk, M.; Thorsteinsson, K.; Moseholm Larsen, E.; Katzenstein, T.; Storgaard, M.; Johansen, I.; Pedersen, G.; Bach, D.; Helleberg, M.; Weis, N.; et al. Risk factors during pregnancy and birth-related complications in HIV-positive versus HIV-negative women in Denmark, 2002–2014. HIV Med. 2020, 21, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Cotter, A.M.; Garcia, A.G.; Duthely, M.L.; Luke, B.; O’Sullivan, M.J. Is antiretroviral therapy during pregnancy associated with an increased risk of preterm delivery, low birth weight, or stillbirth? J. Infect. Dis. 2006, 193, 1195–1201. [Google Scholar] [CrossRef] [PubMed]
- Fleiss, B.; Wong, F.; Brownfoot, F.; Shearer, I.K.; Baud, O.; Walker, D.W.; Gressens, P.; Tolcos, M. Knowledge Gaps and Emerging Research Areas in Intrauterine Growth Restriction-Associated Brain Injury. Front. Endocrinol. 2019, 10, 188. [Google Scholar] [CrossRef] [Green Version]
- Beune, I.M.; Bloomfield, F.H.; Ganzevoort, W.; Embleton, N.D.; Rozance, P.J.; van Wassenaer-Leemhuis, A.; Wynia, K.; Gordijn, S.J. Consensus Based Definition of Growth Restriction in the Newborn. J. Pediatr. 2018, 196, 71–76.e1. [Google Scholar] [CrossRef]
- Dos Reis, H.L.; Araujo Kda, S.; Ribeiro, L.P.; Da Rocha, D.R.; Rosato, D.P.; Passos, M.R.; Merçon De Vargas, P.R. Preterm birth and fetal growth restriction in HIV-infected Brazilian pregnant women. Rev. Inst. Med. Trop. Sao Paulo 2015, 57, 111–120. [Google Scholar] [CrossRef] [Green Version]
- WHO Recommendations on the Diagnosis of HIV Infection in Infants and Children. Available online: https://www.ncbi.nlm.nih.gov/books/NBK138552/ (accessed on 2 October 2022).
- The Apgar Score. Committee Opinion No. 644. American College of Obstetricians and Gynecologists. Obs. Gynecol. 2015, 126, e52–e55. [Google Scholar] [CrossRef] [PubMed]
- Hasmasanu, M.G.; Bolboaca, S.D.; Baizat, M.I.; Drugan, T.C.; Zaharie, G.C. Neonatal short-term outcomes in infants with intrauterine growth restriction. Saudi Med. J. 2015, 36, 947–953. [Google Scholar] [CrossRef]
- Cambrea, S.C.; Marcu, E.A.; Cucli, E.; Badiu, D.; Penciu, R.; Petcu, C.L.; Dumea, E.; Halichidis, S.; Pazara, L.; Mihai, C.M.; et al. Clinical and Biological Risk Factors Associated with Increased Mother-to-Child Transmission of HIV in Two South-East HIV-AIDS Regional Centers in Romania. Medicina 2022, 58, 275. [Google Scholar] [CrossRef]
- Cambrea, S.C.; Popescu, G.G.; Resul, G.; Petcu, L.C. The spectrum of infectious diseases hospital mortality by HIV status. Acta Med. Mediterr. 2019, 35, 3517–3522. [Google Scholar]
- Leopa, N.; Dumitru, E.; Dumitru, A.; Tocia, C.; Prazaru, M.D.; Costea, D.O.; Popescu, R.C. The Clinicopathological Differences of Colon Cancer in Young Adults versus Older Adults. J. Adolesc. Young Adult Oncol. 2022. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Stefanopol, I.A.; Baroiu, L.; Constantin, G.B.; Danila, D.M.; Anghel, L.; Nechifor, A.; Tatu, A.L. Diagnostic and Management of Undescended Ovary–A Preoperative Dilemma: A Case-Based Systematic Review. Int. J. Women’s Health 2022, 14, 15–27. [Google Scholar] [CrossRef]
- Zugravu, C.; Nanu, M.I.; Moldovanu, F.; Arghir, O.C.; Mihai, C.M.; Otelea, M.R.; Cambrea, S.C. The influence of Perinatal Education on Breastfeeding Decision and Duration. Int. J. Child Health Nutr. 2018, 7, 74–81. [Google Scholar] [CrossRef]
- Pătru, S.; Pădureanu, R.; Dumitrescu, F.; Pădureanu, V.; Rădulescu, D.; Dragoi, D.; Matei, D. Influence of multidisciplinary therapeutic approach on fibromyalgia patients. Exp. Ther. Med. 2021, 21, 528. [Google Scholar] [CrossRef] [PubMed]
- Ghita, C.; Vilcea, I.D.; Dumitrescu, M.; Vilcea, A.M.; Mirea, C.S.; Aschie, M.; Vasilescu, F. The prognostic value of immunohistochemical aspects of tumor suppressor genes p53, bcl-2, PTEN and nuclear proliferative antigen Ki-67 in resected colorectal carcinoma. Rom. J. Morphol. Embryol. 2012, 53, 549–556. [Google Scholar] [PubMed]
- Bjørklund, G.; Peana, M.; Pivina, L.; Dosa, A.; Aaseth, J.; Semenova, Y.; Chirumbolo, S.; Medici, S.; Dadar, M.; Costea, D.O. Iron Deficiency in Obesity and after Bariatric Surgery. Biomolecules 2021, 11, 613. [Google Scholar] [CrossRef] [PubMed]
- Șerban, D.; Popa Cherecheanu, A.; Dascalu, A.M.; Socea, B.; Vancea, G.; Stana, D.; Smarandache, G.C.; Sabau, A.D.; Costea, D.O. Hypervirulent Klebsiella pneumoniae Endogenous Endophthalmitis—A Global Emerging Disease. LIFE-BASEL 2021, 11, 676. [Google Scholar] [CrossRef]
- Sebastiani, G.; Borrás-Novell, C.; Casanova, M.A.; Pascual Tutusaus, M.; Ferrero Martínez, S.; Gómez Roig, M.D.; García-Algar, O. The Effects of Alcohol and Drugs of Abuse on Maternal Nutritional Profile during Pregnancy. Nutrients 2018, 10, 1008. [Google Scholar] [CrossRef] [Green Version]
- Mazzitelli, M.; Micieli, M.; Votino, C.; Visconti, F.; Quaresima, P.; Strazzulla, A.; Torti, C.; Zullo, F. Knowledge of Human Cytomegalovirus Infection and Prevention in Pregnant Women: A Baseline, Operational Survey. Infect. Dis. Obstet. Gynecol. 2017, 2017, 5495927. [Google Scholar] [CrossRef] [Green Version]
- Birkhead, G.S.; Pulver, W.P.; Warren, B.L.; Hackel, S.; Rodríguez, D.; Smith, L. Acquiring human immunodeficiency virus during pregnancy and mother-to-child transmission in New York: 2002–2006. Obstet. Gynecol. 2010, 115, 1247–1255. [Google Scholar] [CrossRef]
- Zenebe, A.; Eshetu, B.; Gebremedhin, S. Association between maternal HIV infection and birthweight in a tertiary hospital in southern Ethiopia: Retrospective cohort study. Ital. J. Pediatr. 2020, 46, 70. [Google Scholar] [CrossRef]
- Fentie, E.A.; Yeshita, H.Y.; Bokie, M.M. Low birth weight and associated factors among HIV positive and negative mothers delivered in northwest Amhara region referral hospitals, Ethiopia, 2020 a comparative crossectional study. PLoS ONE 2022, 17, e0263812. [Google Scholar] [CrossRef] [PubMed]
- Xiao, P.L.; Zhou, Y.B.; Chen, Y.; Yang, M.X.; Song, X.X.; Shi, Y.; Jiang, Q.W. Association between maternal HIV infection and low birth weight and prematurity: A meta-analysis of cohort studies. BMC Pregnancy Childbirth 2015, 15, 246. [Google Scholar] [CrossRef] [Green Version]
- Delicio, A.M.; Lajos, G.J.; Amaral, E.; Cavichiolli, F.; Polydoro, M.; Milanez, H. Adverse effects in children exposed to maternal HIV and antiretroviral therapy during pregnancy in Brazil: A cohort study. Reprod. Health 2018, 15, 76. [Google Scholar] [CrossRef]
- Kennedy, C.E.; Yeh, P.T.; Pandey, S.; Betran, A.P.; Narasimhan, M. Elective caesarean section for women living with HIV: A systematic review of risks and benefits. AIDS 2017, 31, 1579–1591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cambrea, S.C.; Tănase, D.E.; Ilie, M.M.; Diaconu, S.; Marcaş, C.; Carp, D.S.; Halichidis, S.; Petcu, L.C. Can HIV infection during pregnancy cause an intrauterine growth restriction? BMC Infect. Dis 2013, 13, O5. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Infant Parameters | Regional Center | Minim | Maxim | Median | IQR | p |
|---|---|---|---|---|---|---|
| HC (cm) | Constanta | 23.00 | 35.00 | 32.00 | 5.00 | 0.430 |
| Craiova | 26.00 | 35.00 | 33.00 | 4.25 | ||
| BL (cm) | Constanta | 38.00 | 51.00 | 48.00 | 5.00 | 0.786 |
| Craiova | 37.00 | 50.00 | 48.00 | 3.50 | ||
| BW (g) | Constanta | 1500.00 | 3500.00 | 2800.00 | 975.00 | 0.914 |
| Craiova | 1100.00 | 3900.00 | 2640.00 | 1085.00 | ||
| Apgar Score | Constanta | 6.00 | 10.00 | 8.00 | 1.00 | 0.544 |
| Craiova | 7.00 | 10.00 | 8.00 | 1.00 |
| Infant Parameters | Regional Center | Minim | Maxim | Median | IQR | p |
|---|---|---|---|---|---|---|
| HC (cm) | Constanta | 23.00 | 38.00 | 33.00 | 3.00 | 0.389 |
| Craiova | 24.00 | 37.00 | 33.00 | 2.00 | ||
| BL (cm) | Constanta | 35.00 | 55.00 | 48.00 | 4.00 | 0.758 |
| Craiova | 35.00 | 52.00 | 48.00 | 3.00 | ||
| BW (g) | Constanta | 1000.00 | 4000.00 | 2800.00 | 700.00 | 0.221 |
| Craiova | 950.00 | 4300.00 | 2830.00 | 720.00 | ||
| Apgar Score | Constanta | 4.00 | 10.00 | 9.00 | 1.00 | 0.108 |
| Craiova | 5.00 | 9.00 | 9.00 | 1.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cambrea, S.C.; Dumea, E.; Petcu, L.C.; Mihai, C.M.; Ghita, C.; Pazara, L.; Badiu, D.; Ionescu, C.; Cambrea, M.A.; Botnariu, E.G.; et al. Fetal Growth Restriction and Clinical Parameters of Newborns from HIV-Infected Romanian Women. Medicina 2023, 59, 111. https://doi.org/10.3390/medicina59010111
Cambrea SC, Dumea E, Petcu LC, Mihai CM, Ghita C, Pazara L, Badiu D, Ionescu C, Cambrea MA, Botnariu EG, et al. Fetal Growth Restriction and Clinical Parameters of Newborns from HIV-Infected Romanian Women. Medicina. 2023; 59(1):111. https://doi.org/10.3390/medicina59010111
Chicago/Turabian StyleCambrea, Simona Claudia, Elena Dumea, Lucian Cristian Petcu, Cristina Maria Mihai, Constantin Ghita, Loredana Pazara, Diana Badiu, Costin Ionescu, Mara Andreea Cambrea, Eosefina Gina Botnariu, and et al. 2023. "Fetal Growth Restriction and Clinical Parameters of Newborns from HIV-Infected Romanian Women" Medicina 59, no. 1: 111. https://doi.org/10.3390/medicina59010111