
Associations between Vitamin D Deficiency and Carbohydrate Intake and Dietary Factors in Taiwanese Pregnant Women
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
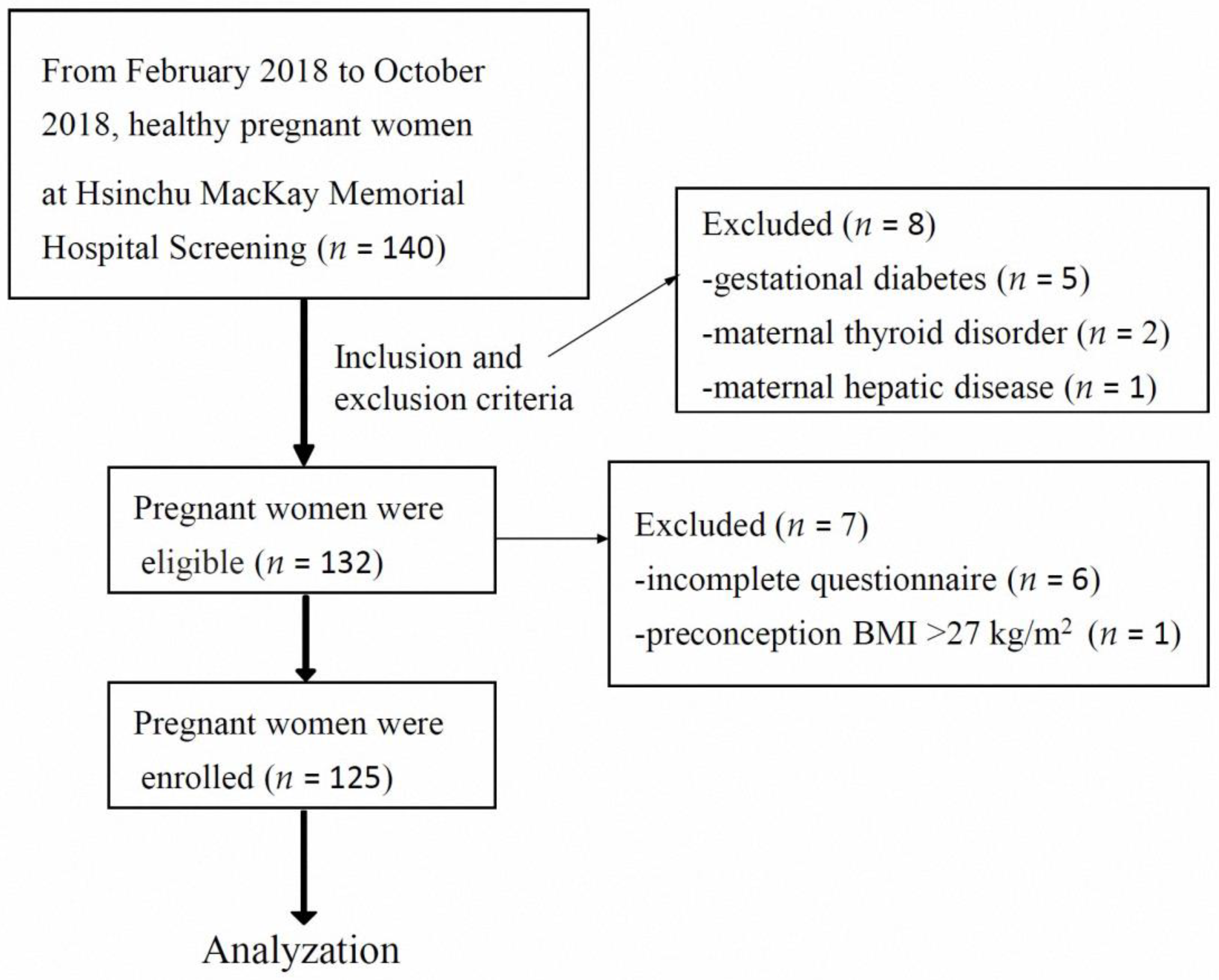
2.1. Study Design and Participants
2.2. Dietary Intake Assessment
2.3. Anthropometric Measurements and Biochemical Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Charoenngam, N.; Rujirachun, P.; Holick, M.F.; Ungprasert, P. Oral vitamin D(3) supplementation increases serum fibroblast growth factor 23 concentration in vitamin D-deficient patients: A systematic review and meta-analysis. Osteoporos. Int. 2019, 30, 2183–2193. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Hossein-nezhad, A.; Holick, M.F. Optimize dietary intake of vitamin D: An epigenetic perspective. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 567–579. [Google Scholar] [CrossRef] [PubMed]
- Helde-Frankling, M.; Björkhem-Bergman, L. Vitamin D in pain management. Int. J. Mol. Sci. 2017, 18, 2170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kellermann, L.; Jensen, K.B.; Bergenheim, F.; Gubatan, J.; Chou, N.D.; Moss, A.; Nielsen, O.H. Mucosal vitamin D signaling in inflammatory bowel disease. Autoimmun. Rev. 2020, 19, 102672. [Google Scholar] [CrossRef]
- Lo, T.H.; Wu, T.Y.; Li, P.C.; Ding, D.C. Effect of vitamin D supplementation during pregnancy on maternal and perinatal outcomes. Tzu-Chi Med. J. 2019, 31, 201–206. [Google Scholar]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- De-Regil, L.M.; Palacios, C.; Lombardo, L.K.; Peña-Rosas, J.P. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2016, Cd008873. [Google Scholar] [CrossRef] [Green Version]
- Pham, T.T.M.; Huang, Y.L.; Chao, J.C.; Chang, J.S.; Chen, Y.C.; Wang, F.F.; Bai, C.H. Plasma 25(OH)D concentrations and gestational diabetes mellitus among pregnant women in Taiwan. Nutrients 2021, 13, 2538. [Google Scholar] [CrossRef]
- Elsori, D.H.; Hammoud, M.S. Vitamin D deficiency in mothers, neonates and children. J. Steroid Biochem. Mol. Biol. 2018, 175, 195–199. [Google Scholar] [CrossRef]
- Principi, N.; Bianchini, S.; Baggi, E.; Esposito, S. Implications of maternal vitamin D deficiency for the fetus, the neonate and the young infant. Eur. J. Nutr. 2013, 52, 859–867. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.H.; Lin, C.Y.; Sung, Y.H.; Li, S.T.; Cheng, B.W.; Weng, S.L.; Chang, S.J.; Lee, H.C.; Lee, Y.J.; Ting, W.H.; et al. Effect of oral vitamin D3 supplementation in exclusively breastfed newborns: Prospective, randomized, double-blind, placebo-controlled trial. J. Bone Miner. Res. 2022, 37, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Liao, S.L.; Lai, S.H.; Tsai, M.H.; Hua, M.C.; Yeh, K.W.; Su, K.W.; Chiang, C.H.; Huang, S.Y.; Kao, C.C.; Yao, T.C.; et al. Maternal vitamin D level is associated with viral toll-like receptor triggered IL-10 response but not the risk of infectious diseases in infancy. Mediat. Inflam. 2016, 2016, 8175898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodnar, L.M.; Simhan, H.N.; Powers, R.W.; Frank, M.P.; Cooperstein, E.; Roberts, J.M. High prevalence of vitamin D insufficiency in black and white pregnant women residing in the northern United States and their neonates. J. Nutr. 2007, 137, 447–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamudoni, P.; Poole, C.; Davies, S.J. An estimate of the economic burden of vitamin D deficiency in pregnant women in the United Kingdom. Gynecol. Endocrinol. 2016, 32, 592–597. [Google Scholar] [CrossRef]
- Wong, R.S.; Tung, K.T.S.; Chan, Y.W.K.; Chan, B.N.K.; Leung, W.C.; Yam, J.C.; Ip, P. Adequate dietary intake and vitamin D supplementation: A study of their relative importance in determining serum vitamin D and ferritin concentrations during pregnancy. Nutrients 2022, 14, 3083. [Google Scholar] [CrossRef]
- Aji, A.S.; Lipoeto, N.I.; Yusrawati, Y.; Malik, S.G.; Kusmayanti, N.A.; Susanto, I.; Nurunniyah, S.; Alfiana, R.D.; Wahyuningsih, W.; Majidah, N.M.; et al. Impact of maternal dietary carbohydrate intake and vitamin D-related genetic risk score on birth length: The Vitamin D Pregnant Mother (VDPM) cohort study. BMC Pregnancy Childbirth 2022, 22, 690. [Google Scholar] [CrossRef]
- Alathari, B.E.; Aji, A.S.; Ariyasra, U.; Sari, S.R.; Tasrif, N.; Yani, F.F.; Sudji, I.R.; Lovegrove, J.A.; Lipoeto, N.I.; Vimaleswaran, K.S. Interaction between vitamin D-related genetic risk score and carbohydrate intake on body fat composition: A study in Southeast Asian Minangkabau women. Nutrients 2021, 13, 326. [Google Scholar] [CrossRef]
- Institute of Medicine (IOM; U.S.). Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; National Academies Press: Washington, DC, USA, 2005; Available online: https://www.researchgate.net/publication/318780697_Dietary_Reference_Intakes_for_Energy_Carbohydrate_Fiber_Fat_Fatty_Acids_Cholesterol_Protein_and_Amino_Acids_Macronutrients (accessed on 10 October 2022).
- Health Promotion Administration (Taiwan). Dietary Reference Intake, 8th ed.; Health Promotion Administration: Taipei, Taiwan, 2022. Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=4248&pid=12285 (accessed on 10 October 2022).
- van Schoor, N.M.; Lips, P. Worldwide vitamin D status. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 671–680. [Google Scholar] [CrossRef]
- Amegah, A.K.; Nsoh, M.; Ashley-Amegah, G.; Anaman-Togbor, J. What factors influences dietary and non-dietary vitamin D intake among pregnant women in an African population? Nutrition 2018, 50, 36–44. [Google Scholar] [CrossRef]
- Johnson, D.D.; Wagner, C.L.; Hulsey, T.C.; McNeil, R.B.; Ebeling, M.; Hollis, B.W. Vitamin D deficiency and insufficiency is common during pregnancy. Am. J. Perinatol. 2011, 28, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Kiel, D.P.; Kraft, P. The genetics of vitamin D. Bone 2019, 126, 59–77. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Huang, Y.C.; Wahlqvist, M.L.; Wu, T.Y.; Chou, Y.C.; Wu, M.H.; Yu, J.C.; Sun, C.A. Vitamin D decreases risk of breast cancer in premenopausal women of normal weight in subtropical Taiwan. J. Epidemiol. 2011, 21, 87–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, G.T.; Sachdev, H.S.; Chellani, H.; Rehman, A.M.; Singh, V.; Arora, H.; Filteau, S. Effect of weekly vitamin D supplements on mortality, morbidity, and growth of low birthweight term infants in India up to age 6 months: Randomised controlled trial. BMJ 2011, 342, d2975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wójcik, M.; Jaworski, M.; Pludowski, P. 25(OH)D concentration in neonates, infants, and toddlers from Poland-evaluation of trends during years 1981–2011. Front. Endocrinol. 2018, 9, 656. [Google Scholar] [CrossRef] [Green Version]
- Carpagnano, G.E.; Di Lecce, V.; Quaranta, V.N.; Zito, A.; Buonamico, E.; Capozza, E.; Palumbo, A.; Di Gioia, G.; Valerio, V.N.; Resta, O. Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19. J. Endocrinol. Investig. 2021, 44, 765–771. [Google Scholar] [CrossRef]
- O’Callaghan, K.M.; Hennessy, Á.; Hull, G.L.J.; Healy, K.; Ritz, C.; Kenny, L.C.; Cashman, K.D.; Kiely, M.E. Estimation of the maternal vitamin D intake that maintains circulating 25-hydroxyvitamin D in late gestation at a concentration sufficient to keep umbilical cord sera ≥25–30 nmol/L: A dose-response, double-blind, randomized placebo-controlled trial in pregnant women at northern latitude. Am. J. Clin. Nutr. 2018, 108, 77–91. [Google Scholar]
- Christoph, P.; Challande, P.; Raio, L.; Surbek, D. High prevalence of severe vitamin D deficiency during the first trimester in pregnant women in Switzerland and its potential contributions to adverse outcomes in the pregnancy. Swiss Med. Wkly. 2020, 150, w20238. [Google Scholar] [CrossRef]
- Shrestha, D.; Saha, R.; Karki, C.; Mahato, S. Study of vitamin-D deficiency among pregnant women in their first trimester visiting a tertiary care hospital: A descriptive cross-sectional study. JNMA J. Nepal. Med. Assoc. 2021, 59, 626–629. [Google Scholar] [CrossRef]
- Yang, C.; Jing, W.; Ge, S.; Sun, W. Vitamin D status and vitamin D deficiency risk factors among pregnancy of Shanghai in China. BMC Pregnancy Childbirth 2021, 21, 431. [Google Scholar] [CrossRef]
- Kanatani, K.T.; Nakayama, T.; Adachi, Y.; Hamazaki, K.; Onishi, K.; Konishi, Y.; Kawanishi, Y.; Go, T.; Sato, K.; Kurozawa, Y.; et al. High frequency of vitamin D deficiency in current pregnant Japanese women associated with UV avoidance and hypo-vitamin D diet. PloS ONE 2019, 14, e0213264. [Google Scholar] [CrossRef] [PubMed]
- Aji, A.S.; Yerizel, E.; Desmawati; Lipoeto, N.I. The association between lifestyle and maternal vitamin D during pregnancy in West Sumatra, Indonesia. Asia Pac. J. Clin. Nutr. 2018, 27, 1286–1293. [Google Scholar] [PubMed]
- Palacios, C.; Kostiuk, L.K.; Peña-Rosas, J.P. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2019, 7, CD008873. [Google Scholar] [CrossRef] [Green Version]
- Luo, T.; Lin, Y.; Lu, J.; Lian, X.; Guo, Y.; Han, L.; Guo, Y. Effects of vitamin D supplementation during pregnancy on bone health and offspring growth: A systematic review and meta-analysis of randomized controlled trials. PLoS ONE 2022, 17, e0276016. [Google Scholar] [CrossRef]
- Lee, M.S.; Li, H.L.; Hung, T.H.; Chang, H.Y.; Yang, F.L.; Wahlqvist, M.L. Vitamin D intake and its food sources in Taiwanese. Asia Pac. J. Clin. Nutr. 2008, 17, 397–407. [Google Scholar] [PubMed]
- ACOG Committee Opinion No. 495. Vitamin D: Screening and supplementation during pregnancy. Obstet Gynecol. 2011, 118, 197–198. [Google Scholar]
- World Health Orgnization (WHO). Nutritional Interventions Update: Vitamin D Supplements during Pregnancy; WHO: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/9789240008120 (accessed on 10 October 2022).
- Brown, H.M.; Bucher, T.; Rollo, M.E.; Collins, C.E. Pregnant women have poor carbohydrate knowledge and do not receive adequate nutrition education. Matern. Child Health J. 2021, 25, 909–918. [Google Scholar] [CrossRef]
- Bolesławska, I.; Kowalówka, M.; Dobrzyńska, M.; Karaźniewicz-Łada, M.; Przysławski, J. Differences in the concentration of vitamin D metabolites in plasma due to the low-carbohydrate-high-fat diet and the Eastern European diet-A pilot study. Nutrients 2021, 13, 2774. [Google Scholar] [CrossRef]
- Alathari, B.E.; Bodhini, D.; Jayashri, R.; Lakshmipriya, N.; Shanthi Rani, C.S.; Sudha, V.; Lovegrove, J.A.; Anjana, R.M.; Mohan, V.; Radha, V.; et al. A Nutrigenetic Approach to investigate the relationship between metabolic traits and vitamin D status in an Asian Indian population. Nutrients 2020, 12, 1357. [Google Scholar] [CrossRef]
- Vranić, L.; Mikolašević, I.; Milić, S. Vitamin D deficiency: Consequence or cause of obesity? Medicina 2019, 55, 541. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Pregnant Women n = 125 | |
|---|---|
| Age (years) | 32.9 ± 4.4 |
| Primiparous, n (%) | 67 (53.6) |
| Multiparous, n (%) | 58 (46.4) |
| Height (cm) | 160.6 ± 5.3 |
| Weight (kg) | 67.4 ± 7.8 |
| Preconception BMI (kg/m2) | 21.1 ± 2.5 |
| BMI (kg/m2) | 26.2 ± 3.0 |
| Weight gain during pregnancy (kg) | 13.0 ± 3.0 |
| 25(OH)D (ng/mL) | 17.2 ± 6.8 |
| Severe VD deficiency, n (%) | 16 (12.8) |
| VD deficiency, n (%) | 69 (55.2) |
| VD insufficiency, n (%) | 32 (25.6) |
| VD sufficiency, n (%) | 8 (6.4) |
| Vitamin D supplementation (IU/day) | 214 ± 180 |
| 0 IU/day | 45 (36.0) |
| 150 IU/day | 17 (13.6) |
| 300 IU/day | 10 (8.0) |
| 400 IU/day | 53 (42.4) |
| Duration of daily sun exposure (min) | 20.9 ± 12.0 |
| Daily energy intake (kcal/day) | 2244 ± 756 |
| Total carbohydrate (g) | 335 ± 129 |
| Total protein (g) | 88.9 ± 31.0 |
| Total fat (g) | 59.3 ± 21.4 |
| Carbohydrate (% of energy) | 59.0 ± 8.4 |
| Protein (% of energy) | 16.2 ± 3.4 |
| Fat (% of energy) | 24.3 ± 5.6 |
| Cholesterol (mg) | 335 ± 156 |
| VD from food (IU/day) | 147 ± 97 |
| Total VD intake (IU/day) | 362 ± 206 |
| Variables | 25(OH)D Pearson Coefficient r | p Value |
|---|---|---|
| Age | 0.233 | 0.009 |
| Duration of daily sun exposure | 0.071 | 0.433 |
| Height | 0.069 | 0.445 |
| Weight | −0.105 | 0.242 |
| BMI | −0.139 | 0.122 |
| Preconception BMI | −0.076 | 0.399 |
| Weight gain during pregnancy | −0.125 | 0.164 |
| Daily energy intake | −0.040 | 0.656 |
| Total carbohydrate | −0.023 | 0.802 |
| Total protein | −0.050 | 0.583 |
| Total fat | −0.071 | 0.430 |
| Carbohydrate (% of energy) | 0.059 | 0.516 |
| Protein (% of energy) | −0.054 | 0.549 |
| Fat (% of energy) | −0.073 | 0.421 |
| Cholesterol | −0.070 | 0.436 |
| VD from food | −0.054 | 0.549 |
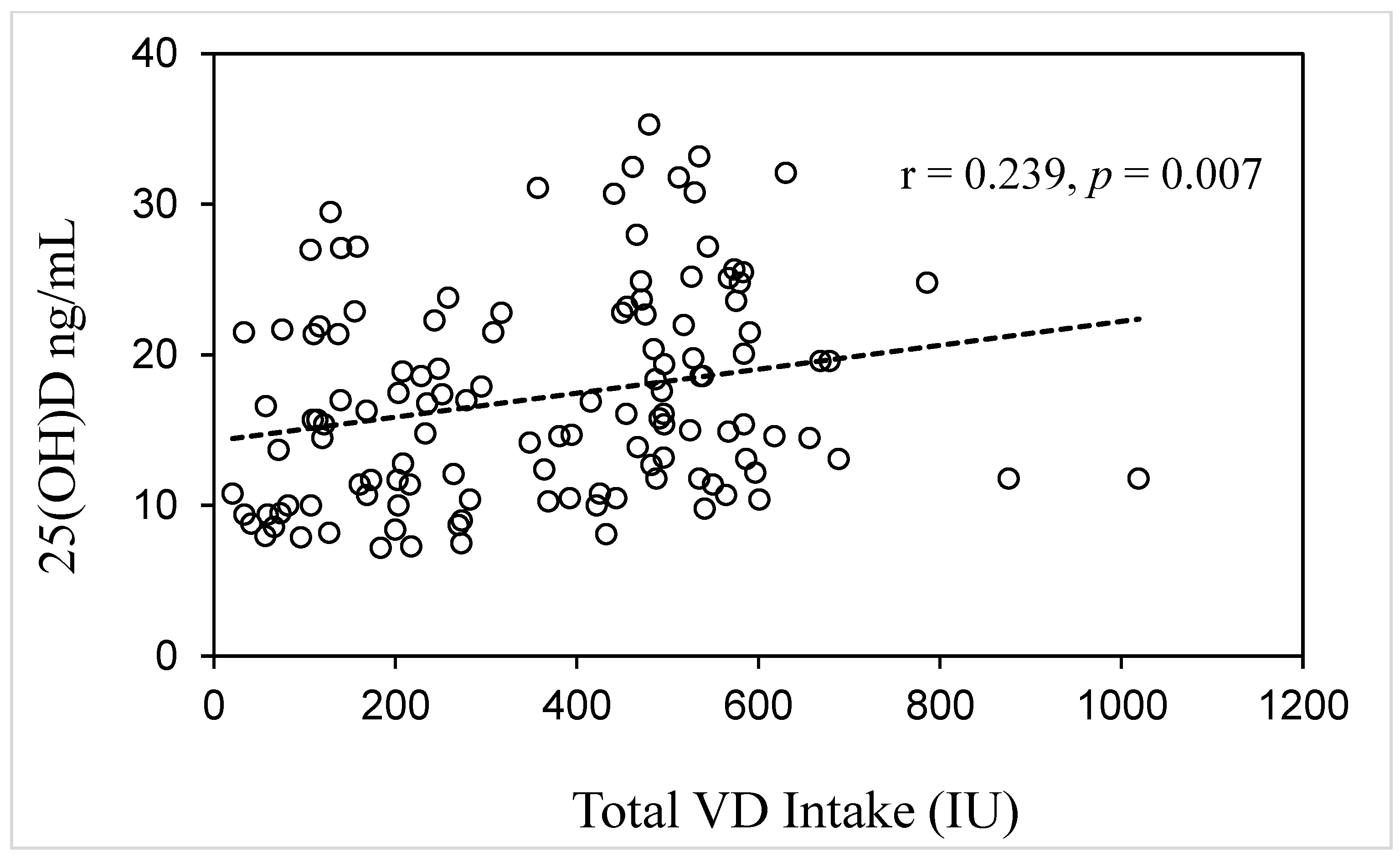
| Total VD intake | 0.239 | 0.007 |
| Characteristics | Severe VD Deficiency (n = 16) a | VD Deficiency (n = 69) b | VD Insufficiency (n = 32) c | VD Sufficiency (n = 8) d | p Value |
|---|---|---|---|---|---|
| Age (years) | 30.2 ± 4.5 | 32.9 ± 4.2 | 33.9 ± 4.9 | 33.8 ± 1.7 | 0.041 c > a |
| 25(OH)D (ng/mL) | 8.5 ± 0.8 | 14.3 ± 3.0 | 23.9 ± 2.4 | 32.2 ± 1.5 | <0.001 d > c > b > a |
| Duration of daily sun exposure (min) | 19.7 ±13.2 | 21.1 ±12.1 | 20.2 ±12.5 | 24.4 ± 8.2 | 0.813 |
| Total energy intake (kcal/day) | 2145 ± 807 | 2307 ± 830 | 2181 ± 630 | 2150 ± 443 | 0.784 |
| Carbohydrate (g/day) | 330 ± 150 | 340 ± 139 | 327 ± 107 | 337 ± 88 | 0.968 |
| Protein (g/day) | 82.8 ±33.0 | 92.3 ±33.0 | 86.9± 28.0 | 79.4 ±19.7 | 0.516 |
| Fat (g/day) | 53.8 ± 19.3 | 62.6 ±23.9 | 56.9 ±17.1 | 52.0 ±14.8 | 0.264 |
| Carbohydrate (%) | 59.9 ±10.5 | 58.2 ±8.3 | 59.5 ±7.1 | 61.8 ±10.5 | 0.629 |
| Protein (%) | 16.1 ± 4.8 | 16.4 ± 3.3 | 16.0 ± 2.8 | 15.0 ± 3.5 | 0.766 |
| Fat (%) | 23.8 ± 6.7 | 24.9 ± 5.5 | 23.9 ± 4.9 | 22.4 ± 7.6 | 0.577 |
| Cholesterol (mg) | 299 ± 152 | 359 ± 171 | 320 ± 127 | 258 ± 102 | 0.190 |
| VD from food (IU/day) | 115 ± 79 | 159 ± 106 | 146 ± 88 | 105 ± 61 | 0.236 |
| VDs (IU/day) | 68 ± 138 | 221 ± 178 | 226 ± 177 | 387± 35 | <0.001 a < b, c, d & b < d |
| VDs, 0 IU/day | 12 (75) | 23 (33.3) | 10 (31.3) | 0 | |
| VDs, 150 IU/day | 2 (12.5) | 10 (14.5) | 5 (15.6) | 0 | |
| VDs, 300 IU/day | 0 (0) | 6 (8.7) | 3 (9.4) | 1 (12.5) | |
| VDs, 400 IU/day | 2 (12.5) | 30 (43.5) | 14 (43.8) | 7 (82.5) | |
| Total VD intake (IU/day) | 184 ± 147 | 382 ± 207 | 374 ± 206 | 493 ± 79 | 0.001 a < b, c, d |
| Height (cm) | 159.9 ± 4.8 | 160.4 ± 5.5 | 161.0 ± 5.2 | 161.6 ± 5.2 | 0.847 |
| Weight (kg) | 67.2 ± 6.8 | 68.0 ± 8.5 | 66.5 ± 7.2 | 66.9 ± 5.8 | 0.850 |
| BMI (kg/m2) | 26.3 ± 2.5 | 26.4 ± 3.2 | 25.7 ± 3.0 | 25.6 ± 2.4 | 0.699 |
| Preconception BMI (kg/m2) | 21.5 ± 2.0 | 21.2 ± 2.4 | 20.8 ± 2.9 | 21.3 ± 2.8 | 0.790 |
| Weight gain during pregnancy (kg) | 12.3 ± 3.1 | 13.4± 5.2 | 11.3 ± 1.6 | 13.0 ± 4.3 | 0.526 |
| Characteristics | 0 IU/Day (n = 45) a | 150 IU/Day (n = 17) b | 300 IU/Day (n = 10) c | 400 IU/Day (n = 53) d | p Value |
|---|---|---|---|---|---|
| Age (years) | 32.2 ± 4.8 | 32.2 ± 3.8 | 37 ± 3.7 | 32.9 ± 4.1 | 0.015 c > a, b, d |
| 25(OH)D (ng/mL) | 14.6 ± 6.1 | 16.9 ± 5.3 | 18.3 ± 7.2 | 19.2 ± 7.2 | 0.007 d > a |
| Severe VD deficiency, n (%) | 12 (26.7) | 2 (11.8) | 0 (0) | 2 (3.8) | |
| VD deficiency, n (%) | 23 (51.1) | 10 (58.8) | 6 (60) | 30 (56.6) | |
| VD insufficiency, n (%) | 10 (22.2) | 5 (29.4) | 3 (30) | 14 (26.4) | |
| VD sufficiency, n (%) | 0 (0) | 0 (0) | 1 (10) | 7 (13.2) | |
| Duration of daily sun exposure (min) | 21.4 ± 11.4 | 17.9 ±12.6 | 26.0 ±9.7 | 20.4 ± 12.7 | 0.394 |
| Total VD intake (IU/day) | 151 ± 92 | 276 ± 89 | 442 ± 72 | 553 ± 108 | <0.001 d > c > b > a |
| VD from food (IU/day) | 148 ± 92 | 126 ± 89 | 142.± 72 | 153 ± 108 | 0.799 |
| Height (cm) | 161.6 ± 5.5 | 160.2 ± 5.9 | 158.5 ± 3.3 | 160.2 ± 5.1 | 0.328 |
| Weight (kg) | 68.9 ± 8.1 | 66.3 ± 6.2 | 66.9 ± 9.1 | 66.6 ± 7.8 | 0.466 |
| BMI (kg/m2) | 26.4 ± 3.2 | 25.9 ± 2.7 | 26.6 ± 3.1 | 26.0 ± 3.1 | 0.842 |
| Preconception BMI (kg/m2) | 21.5 ± 2.6 | 21.6 ± 2.4 | 21.2 ± 2.0 | 20.7 ± 2.5 | 0.409 |
| Weight gain during pregnancy (kg) | 12.9 ± 4.0 | 11.1± 3.7 | 13.5 ± 4.4 | 13.5 ± 4.7 | 0.251 |
| Variables | B | β | p Value |
|---|---|---|---|
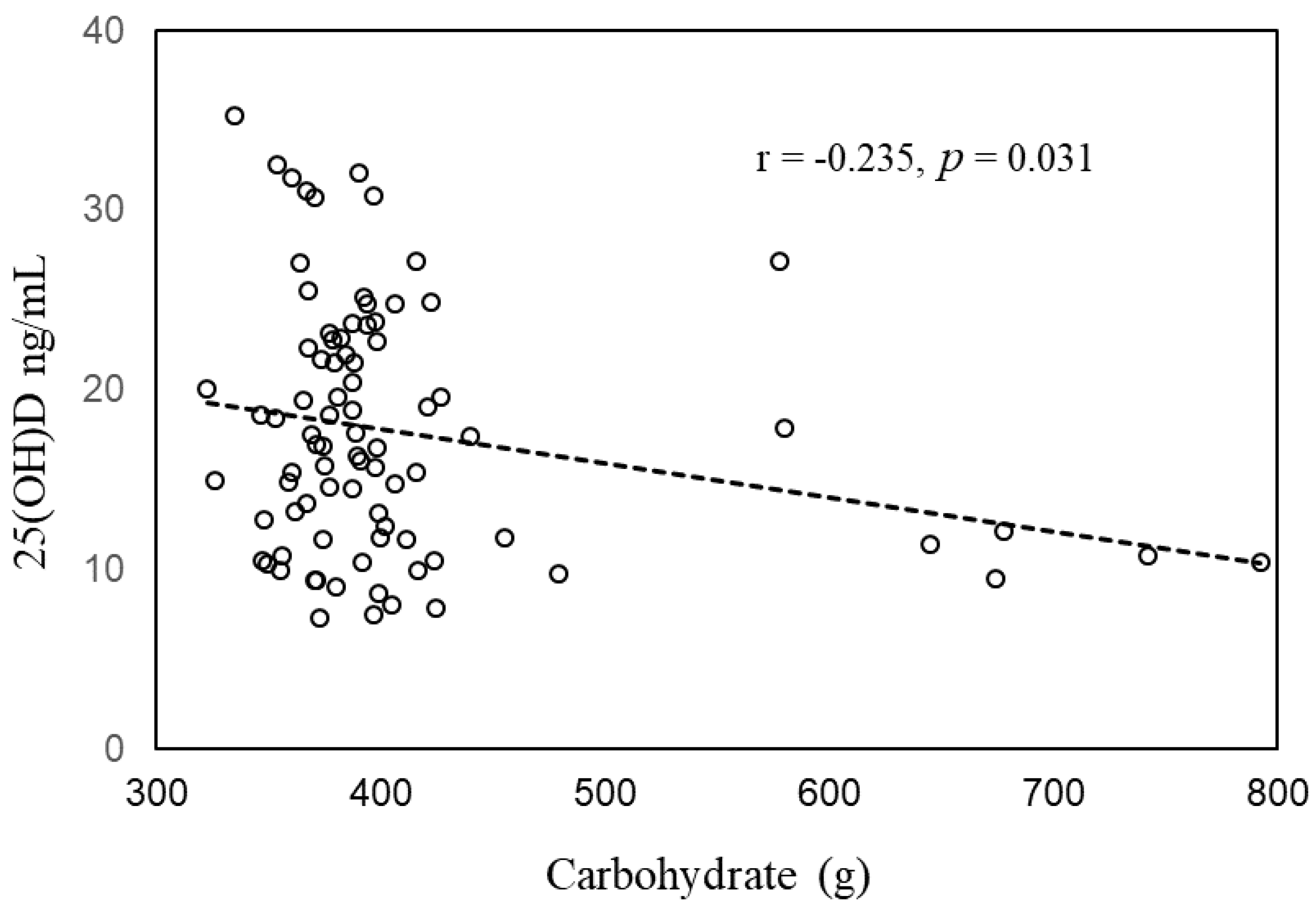
| Carbohydrate intake | −0.019 | −0.236 | 0.022 |
| Total VD intake | 0.014 | 0.377 | 0.021 |
| VDs (400 IU/day) | −0.200 | −0.014 | 0.929 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-H.; Lin, P.-S.; Lee, M.-S.; Lin, C.-Y.; Sung, Y.-H.; Li, S.-T.; Weng, S.-L.; Chang, S.-J.; Lee, H.-C.; Lee, Y.-J.; et al. Associations between Vitamin D Deficiency and Carbohydrate Intake and Dietary Factors in Taiwanese Pregnant Women. Medicina 2023, 59, 107. https://doi.org/10.3390/medicina59010107
Lin C-H, Lin P-S, Lee M-S, Lin C-Y, Sung Y-H, Li S-T, Weng S-L, Chang S-J, Lee H-C, Lee Y-J, et al. Associations between Vitamin D Deficiency and Carbohydrate Intake and Dietary Factors in Taiwanese Pregnant Women. Medicina. 2023; 59(1):107. https://doi.org/10.3390/medicina59010107
Chicago/Turabian StyleLin, Chao-Hsu, Pei-Shun Lin, Meei-Shyuan Lee, Chien-Yu Lin, Yi-Hsiang Sung, Sung-Tse Li, Shun-Long Weng, Shing-Jyh Chang, Hung-Chang Lee, Yann-Jinn Lee, and et al. 2023. "Associations between Vitamin D Deficiency and Carbohydrate Intake and Dietary Factors in Taiwanese Pregnant Women" Medicina 59, no. 1: 107. https://doi.org/10.3390/medicina59010107