Oral Manifestations Associated with HIV/AIDS Patients

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
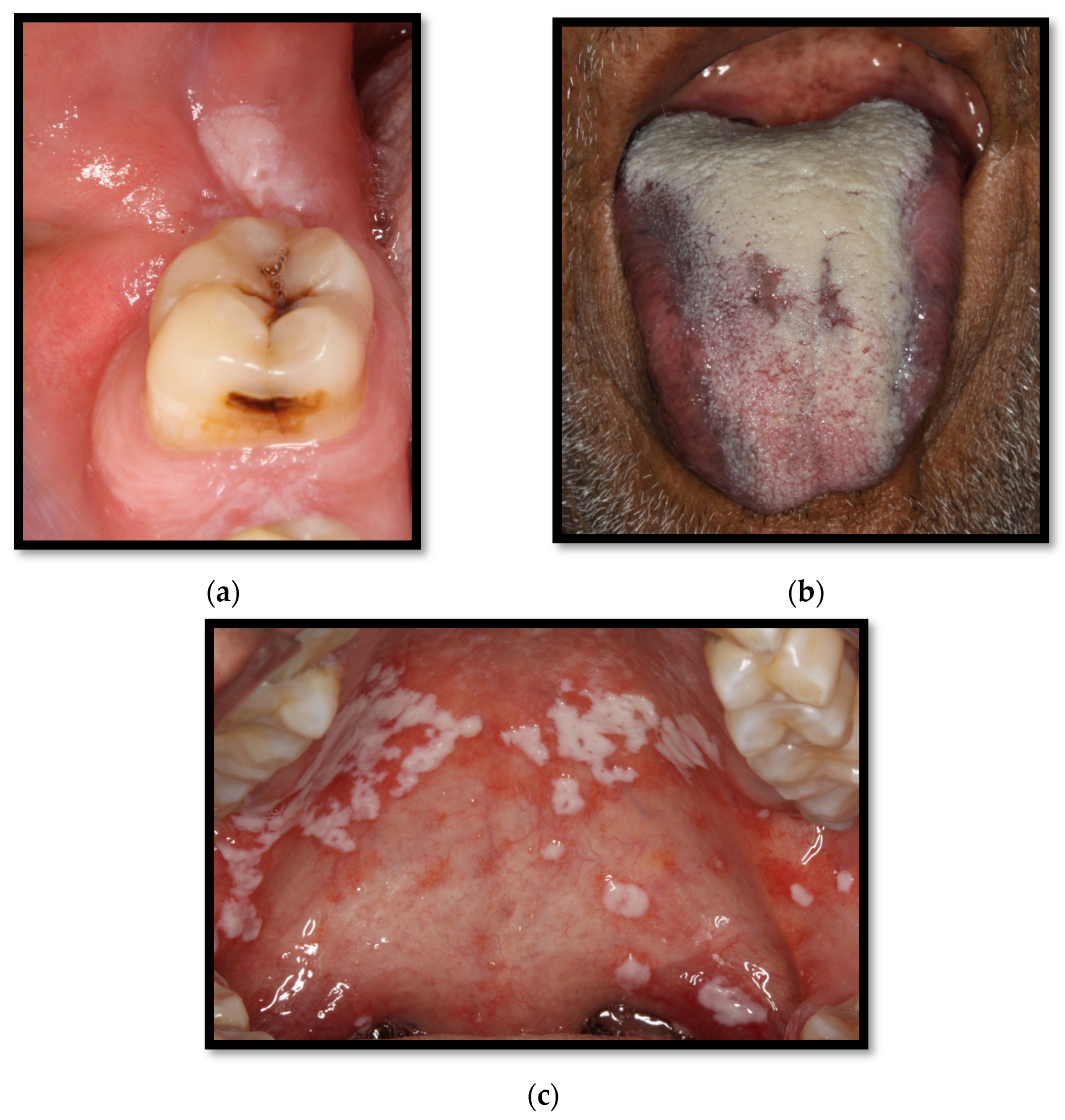
2. Oral Candidiasis
2.1. Oral Thrush
2.2. Erythematous Candidiasis
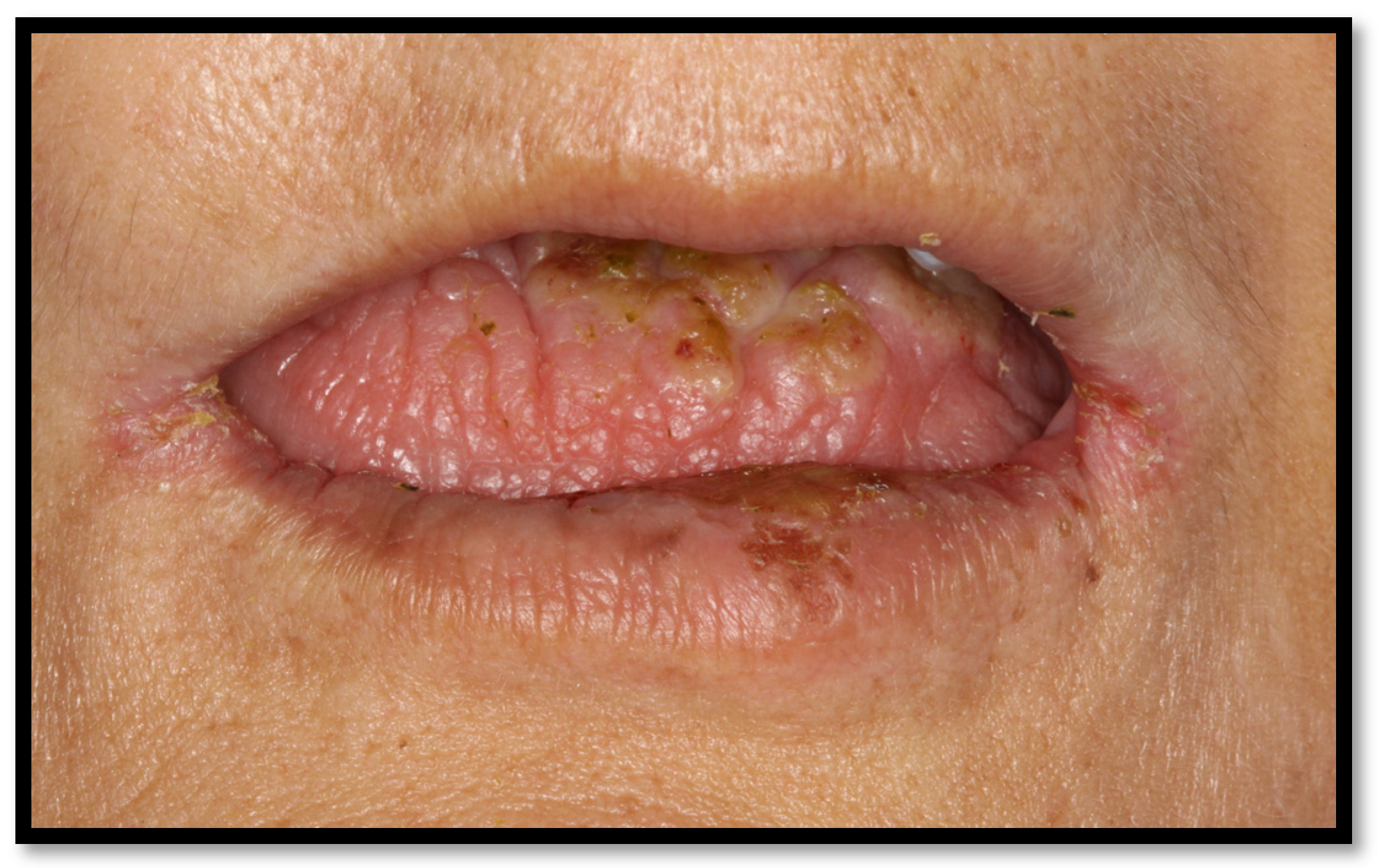
2.3. Angular Cheilitis
3. Periodontal Disease
3.1. Linear Gingival Erythema
3.2. Periodontitis
3.3. Necrotizing Gingivitis (NG)
3.4. Necrotizing Periodontitis (NP)
4. Xerostomia
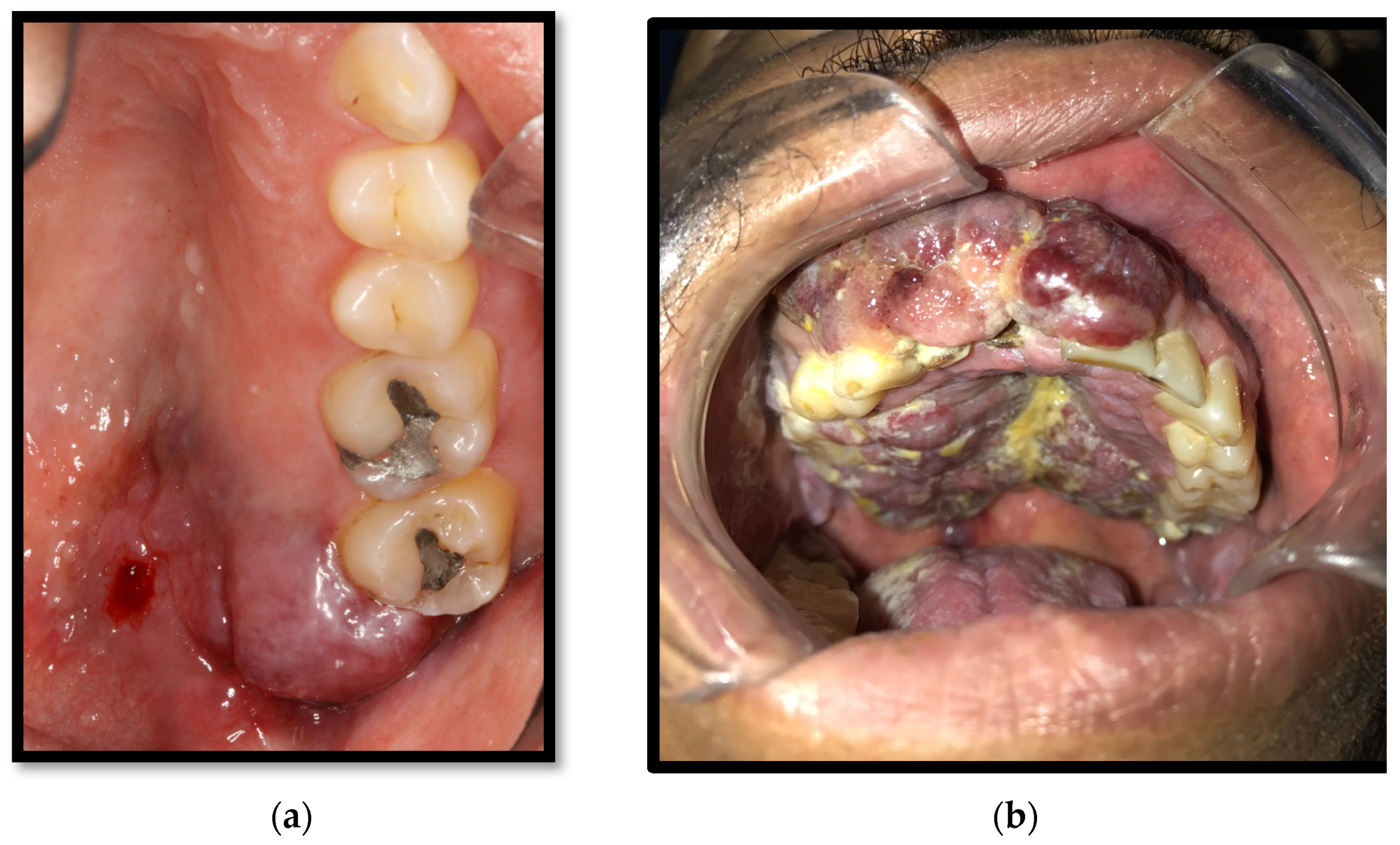
5. Kaposi’s Sarcoma
6. Recurrent Aphthous Ulcers
6.1. Minor Aphthous Ulcers
6.2. Major Aphthous Ulcers
7. Oral Hairy Leukoplakia
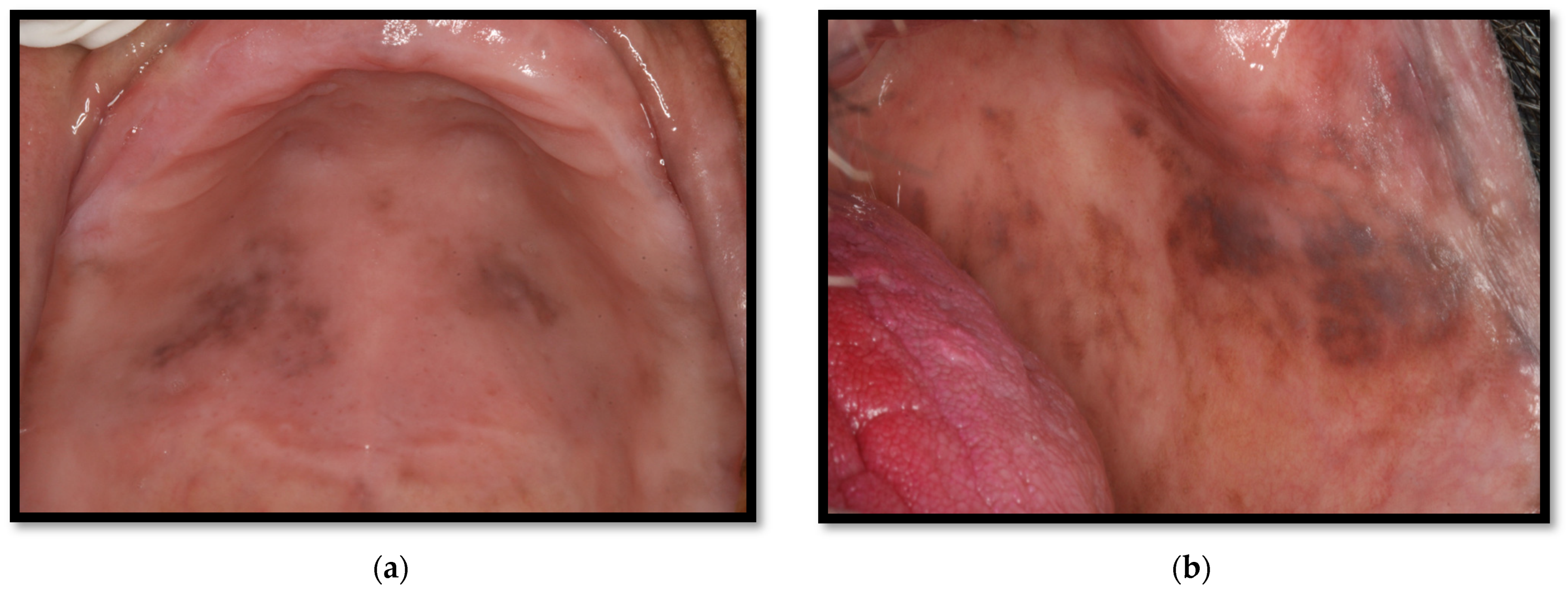
8. Oral Hyperpigmentation
9. Oral Herpes Virus
10. Oral Warts
11. Caries
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Vohram, P.; Jamatia, K.; Subhada, B.; Tiwari, R.V.C.; Althaf, M.N.; Jain, C. Correlation of CD4 counts with oral and systemic manifestations in HIV patients. J. Fam. Med. Prim Care 2019, 8, 3247–3252. [Google Scholar] [CrossRef] [PubMed]
- World Dental Federation. The Challenge of Oral Disease, a Call for Global Action. The Oral Health Atlas. Second Edition. 2015. Available online: https://www.fdiworlddental.org/sites/default/files/202103/complete_oh_atlas-2_0.pdf (accessed on 15 June 2022).
- Pakfetrat, A.; Falaki, F.; Delavarian, Z.; Dalirsani, Z.; Sanatkhani, M.; Zabihi, M. Oral Manifestations of Human Immunodeficiency Virus-Infected Patients. Iran. J. Otorhinolaryngol. 2015, 27, 43–54. [Google Scholar] [PubMed]
- Donoso, F. Oral lesions associated with human immunodeficiency virus disease in adult patients, a clinical perspective. Rev. Chil. Infectol. 2016, 33, 27–35. [Google Scholar]
- Frimpong, P.; Kofi, E.; Abebrese, J.; Min, S. Oral manifestations and their correlation to baseline CD4 count of HIV/AIDS patients in Ghana. J. Korean Assoc. Oral Maxillofac. Surg. 2017, 43, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Sharma, G.; Pai, K.M.; Setty, S.; Ramapuram, J.T.; Nagpal, A. Oral manifestations as predictors of immune suppression in a HIV-/AIDS-infected population in south India. Clin. Oral Investig. 2009, 13, 141–148. [Google Scholar] [CrossRef] [PubMed]
- El Howati, A.; Tappuni, A. Systematic review of the changing pattern of the oral manifestations of HIV. J. Investig. Clin. Dent. 2018, 9, e12351. [Google Scholar] [CrossRef] [PubMed]
- López, S.; Andrade, J.; Zamora, A.L.; Bologna, R.; Cervantes, J.J.; Molina, N. Differences in salivary flow level, xerostomia, and flavor alteration in mexican HIV patients who did or did not receive antiretroviral therapy. AIDS Res. Treat. 2013, 2013, 613278. [Google Scholar]
- Lomelí, S.M.; Gonzalez, L.A.; Andrade, J.; Valentin, E.; Ratkovich, S.; Alvarez, M.; Sanchez, K.; Cabrera, R.I.; Varela, J.J. In vitro Azole antifungals susceptibility of Candida spp. isolates from HIV-infected patients with periodontitis. J. Mycol. Med. 2022, 32, 101294. [Google Scholar] [CrossRef]
- Koo, H.; Bowen, W.H. Candida albicans and Streptococcus mutans: A potential synergistic alliance to cause virulent tooth decay in children. Future Microbiol. 2014, 9, 1295–1297. [Google Scholar] [CrossRef]
- Charone, S.; Portela, M.; Martins, K.; Soare, R.; Castro, G. Role of Candida species from HIV infected children in enamel caries lesions: An in vitro study. J. Appl. Oral Sci. 2017, 25, 53–60. [Google Scholar] [CrossRef]
- Polvora, T.L.S.; Nobre, A.V.V.; Tirapelli, C.; Taba, M.; Macedo, L.D.; Santana, R.C. Relationship between human immunodeficiency virus (HIV-1) infection and chronic periodontitis. Expert Rev. Clin. Immunol. 2018, 14, 315–327. [Google Scholar] [CrossRef] [PubMed]
- Berberi, A.; Noujeim, Z. Epidemiology and Relationships between CD4+ Counts and Oral Lesions among 50 Patients Infected with Human Immunodeciency Virus. J. Int. Oral Health 2015, 7, 18. [Google Scholar] [PubMed]
- Hellstein, J.W.; Marek, C.L. Candidiasis: Red and White Manifestations in the Oral Cavity. Head Neck Pathol. 2019, 13, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Lekshmi, L.; Anithalekshmi, M.R.; Abraham, L.; Nair, M.; Aniyan, N.; Nair, N.; Varghese, R.; Abraham, S. Oral Candidiasis Review. Int. J. Res. Pharm. Nano Sci. 2015, 4, 409–417. [Google Scholar]
- Agbelusi, G.A.; Eweka, O.M.; Ùmeizudikea, K.A.; Okoh, M. Oral Manifestations of HIV. Curr. Perspect. HIV Infect. 2013, 209–242. [Google Scholar] [CrossRef]
- Souza, L.; Lopo, B.; Vascocellos, T. Periodontal disease in HIV-infected adults in the HAART era: Clinical, inmunological, and microbiological aspects. Arch. Oral Biol. 2013, 58, 1385–1396. [Google Scholar]
- Aas, J.A.; Barbuto, S.M.; Alpagot, T.; Olsen, I.; Dewhirst, F.E.; Paster, B.J. Subgingival plaque microbiota in HIV positive patients. J. Clin. Periodontol. 2007, 34, 189–195. [Google Scholar] [CrossRef]
- Portela, M.B.; Souza, I.P.; Costa, E.M.; Hagler, A.N.; Soares, R.M.; Santos, A.L. Differencial recovery of Candida species from subgingival sites in human immunodeficiency virus-positive and healthy children from Rio de Janeiro, Brazil. J. Clin. Microbiol. 2004, 42, 5925–5927. [Google Scholar] [CrossRef]
- Elerson, G.J.; Nakano, V.; Wahasugui, T.; Cabral, F.; Gamba, R.; Avila, M. Ocurrence of yeasts, enterococci and other enteric bacteria in subgingival biofilm of HIV-positive patients with chronic gingivitis and necrotizing periodontitis. Braz. J. Microbiol. 2008, 39, 257–261. [Google Scholar]
- Sardi, J.; Duque, C.; Mariano, F.; Peixoto, I.; Hofling, J.; Goncalves, R. Candida spp. in periodontal disease: A brief review. J. Oral Sci. 2010, 52, 177–185. [Google Scholar] [CrossRef]
- Urzúa, B.; Hermosilla, G.; Gamonal, J.; Morales, I.; Canals, M.; Barahona, S.; Cóccola, C.; Cifuentes, V. Yeast diversity in the oral microbiota of subjects with periodontitis: Candida albicans and Candida dubliniensis colonize the periodontal pockets. Med. Mycol. 2008, 46, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Mataftsi, M.; Skoura, L.; Sakellari, D. HIV infection and periodontal diseases: An overview of the post-HAART era. Oral Dis. 2011, 17, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Jordan, R.; Lucaciu, A.; Zimmer, S. Influence of highly-active antiretroviral therapy on the subgingival biofilm in HIV-infected patients. J. Investig. Clin. Dent. 2016, 7, 65–67. [Google Scholar] [CrossRef] [PubMed]
- Lourenço, A.; Ribeiro, A.; Nakao, C.; Motta, A.; Antonio, L.; Machado, A.; Komesu, C. Oral Candida spp. carriage and periodontal diseases in HIV-infected patients in Ribeirão Preto, Brazil. Rev. Inst. Med. Trop. Sao Paulo 2017, 59, e29. [Google Scholar] [CrossRef]
- Zia, A.; Mukhtar-Un-Nisar, A.; Qadri, S.; Bey, A. Necrotizing periodontitis in a heavy smoker and tobacco chewer—A case report. Singap. Dent J. 2015, 36, 35–38. [Google Scholar] [CrossRef] [Green Version]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89, S159–S172. [Google Scholar] [CrossRef]
- Tsuchida, S.; Satoh, M.; Takiwaki, M.; Nomura, F. Ubiquitination in Periodontal Disease: A Review. Int. J. Mol. Sci. 2017, 10, 18. [Google Scholar] [CrossRef]
- Hamilton, N.; Blignaut, E.; Lemmer, J.; Meyerov, R.; Feller, L. Necrotizing Periodontal Diseases in a Semirural District of South Africa. AIDS Res. Treat. 2011, 2011, 638584. [Google Scholar]
- Tejeda, E.; Rodríguez, F.; García, L.; Durán, L. Gingivitis ulceronecrosante aguda. Acta Pediatr. Mex. 2015, 36, 497–498. [Google Scholar]
- Umeizudike, K.A.; Savage, K.O.; Ayanbadejo, P.O.; Akanmu, S.A. Severe presentation of necrotizing ulcerative periodontitis in a Nigerian HIV-positive patient: A case report. Med. Princ. Pract. 2011, 20, 374–376. [Google Scholar] [CrossRef]
- González, E.; Aguilar, M.; Guisado, R.; Tristan, J.; García, P.; Alvarez, J. Xerostomía: Diagnóstico y Manejo Clínico. Rev. Clin. Med. Fam. 2009, 2, 300–304. [Google Scholar]
- Hopcraft, M.S.; Tan, C. Xerostomia: An update for clinicians. Aust. Dent. J. 2010, 55, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Shimazaki, Y.; Fu, B.; Yonemoto, K.; Akifusa, S.; Shibata, Y.; Takeshita, T.; Ninomiya, T.; Kiyoharam, Y.; Yamashita, Y. Stimulated salivary flow rate and oral health status. J. Oral Sci. 2017, 59, 55–62. [Google Scholar] [CrossRef]
- Toida, M.; Nanya, Y.; Takeda-Kawaguchi, T.; Baba, S.; Lida, K.; Kato, K. Oral complaints and stimulated salivary low rate in 1188 adults. J. Oral Pathol. Med. 2010, 39, 407–419. [Google Scholar] [PubMed]
- Pedreira, E.N.; Cardoso, C.L.; Barroso, E.C.; Souza, J.A.; Fonseca, F.P.; Taveira, L.A. Epidemiological and oral manifestations of HIV-positive patients in a specialized service in brazil. J. Appl. Oral Sci. 2008, 16, 369–375. [Google Scholar] [CrossRef]
- Leao, J.C.; Ribeiro, C.M.B.; Carvalho, A.A.T.; Frezzini, C.; Porter, S. Oral complications of HIV disease. Clinics 2009, 64, 459–470. [Google Scholar] [CrossRef]
- Schneider, J.W.; Dittmer, D.P. Diagnosis and Treatment of Kaposi Sarcoma. Am. J. Clin. Dermatol. 2017, 18, 529–539. [Google Scholar] [CrossRef]
- Agaimy, A.; Mueller, S.K.; Harrer, T.; Bauer, S.; Thompson, L.D.R. Head and Neck Kaposi Sarcoma: Clinicopathological Analysis of 11 Cases. Head Neck Pathol. 2018, 12, 511–516. [Google Scholar] [CrossRef]
- Bodhade, A.; Ganvir, S.; Hazarey, V. Oral manifestations of HIV infection and their correlation with CD4 count. J. Oral Sci. 2011, 2, 203–211. [Google Scholar] [CrossRef]
- Vaillant, L.; Samimi, M. Aphthous ulcers and oral ulcerations. Presse Med. 2016, 45, 215–226. [Google Scholar] [CrossRef]
- Vale, D.; Martins, F.; Silva, P.; Ortega, K. Retrospective analysis of the clinical behavior of oral hairy leukoplakia in 215 HIV-seropositive patients. Braz. Oral Res. 2006, 28, e118. [Google Scholar] [CrossRef] [PubMed]
- Greenspan, J.S.; Greenspan, D.; Webster-Cyriaque, J. Hairy leukoplakia; lessons learned: 30-plus years. Oral Dis. 2016, 22, 120–127. [Google Scholar] [CrossRef]
- Baccaglini, L.; Atkinson, J.; Patton, L.; Glick, M.; Ficarra, G.; Peterson, D. Management of oral lesions in HIV-positive patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, S50.e1–S50.e23. [Google Scholar] [CrossRef]
- De Almeida, V.L.; Lima, I.F.P.; Ziegelmann, P.K.; Paranhos, L.R.; De Matos, F.R. Impact of highly active antiretroviral therapy on the prevalence of oral lesions in HIV-positive patients: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 1497–1504. [Google Scholar] [CrossRef]
- Aguirre, J.M.; Echebarría, M.A. Síndrome de inmunodeficiencia adquirida: Manifestaciones en la cavidad bucal. Med. Oral Patol. Oral Cir. Bucal. 2004, 9, 148–157. [Google Scholar]
- Cofrancesco, J.; Scherzer, R.; Tien, P.C.; Gibert, C.L.; Southwell, H.; Sidney, S.; Grunfeld, C. Illicit drug use and HIV treatment outcomes in a US cohort. AIDS 2008, 22, 357. [Google Scholar] [CrossRef]
- Toche, P.; Salinas, J.; Guzmán, M.A.; Afani, A.; Jadue, N. Úlceras orales recurrentes: Características clínicas y diagnóstico diferencial. Rev. Chil. Infect. 2007, 24, 215–219. [Google Scholar] [CrossRef]
- Menezes, T.; Rodrigues, M.; Nogueira, B.; Menezes, S.; Silva, S.; Vallinoto, A. Oral and systemic manifestations in HIV-1 patients. Rev. Soc. Bras. Med. Trop. 2015, 48, 83–86. [Google Scholar] [CrossRef]
- Kalanzi, D.; Mayanja-Kizza, H.; Nakanjako, D.; Mwesigwa, C.L.; Ssenyonga, R.; Amaechi, B.T. Prevalence and factors associated with dental caries in patients attending an HIV care clinic in Uganda: A cross sectional study. BMC Oral Health 2019, 19, 159. [Google Scholar] [CrossRef]
- Rezaei-Soufi, L.; Davoodi, P.; Jazaeri, M.; Niknami, H. The comparison of root caries experience between HIV-positive patients and HIV-negative individuals, in a selected Iranian population. Int. J. Dent. Hyg. 2011, 9, 261–265. [Google Scholar] [CrossRef]















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lomelí-Martínez, S.M.; González-Hernández, L.A.; Ruiz-Anaya, A.d.J.; Lomelí-Martínez, M.A.; Martínez-Salazar, S.Y.; Mercado González, A.E.; Andrade-Villanueva, J.F.; Varela-Hernández, J.J. Oral Manifestations Associated with HIV/AIDS Patients. Medicina 2022, 58, 1214. https://doi.org/10.3390/medicina58091214
Lomelí-Martínez SM, González-Hernández LA, Ruiz-Anaya AdJ, Lomelí-Martínez MA, Martínez-Salazar SY, Mercado González AE, Andrade-Villanueva JF, Varela-Hernández JJ. Oral Manifestations Associated with HIV/AIDS Patients. Medicina. 2022; 58(9):1214. https://doi.org/10.3390/medicina58091214
Chicago/Turabian StyleLomelí-Martínez, Sarah Monserrat, Luz Alicia González-Hernández, Antonio de Jesús Ruiz-Anaya, Manuel Arturo Lomelí-Martínez, Silvia Yolanda Martínez-Salazar, Ana Esther Mercado González, Jaime Federico Andrade-Villanueva, and Juan José Varela-Hernández. 2022. "Oral Manifestations Associated with HIV/AIDS Patients" Medicina 58, no. 9: 1214. https://doi.org/10.3390/medicina58091214