
Changing Susceptibility of Staphylococci in Patients with Implant-Based Breast Reconstructions: A Single-Center Experience

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Perioperative Procedures
2.3. Microbiology and Microbial Susceptibility
2.4. Statistical Analysis
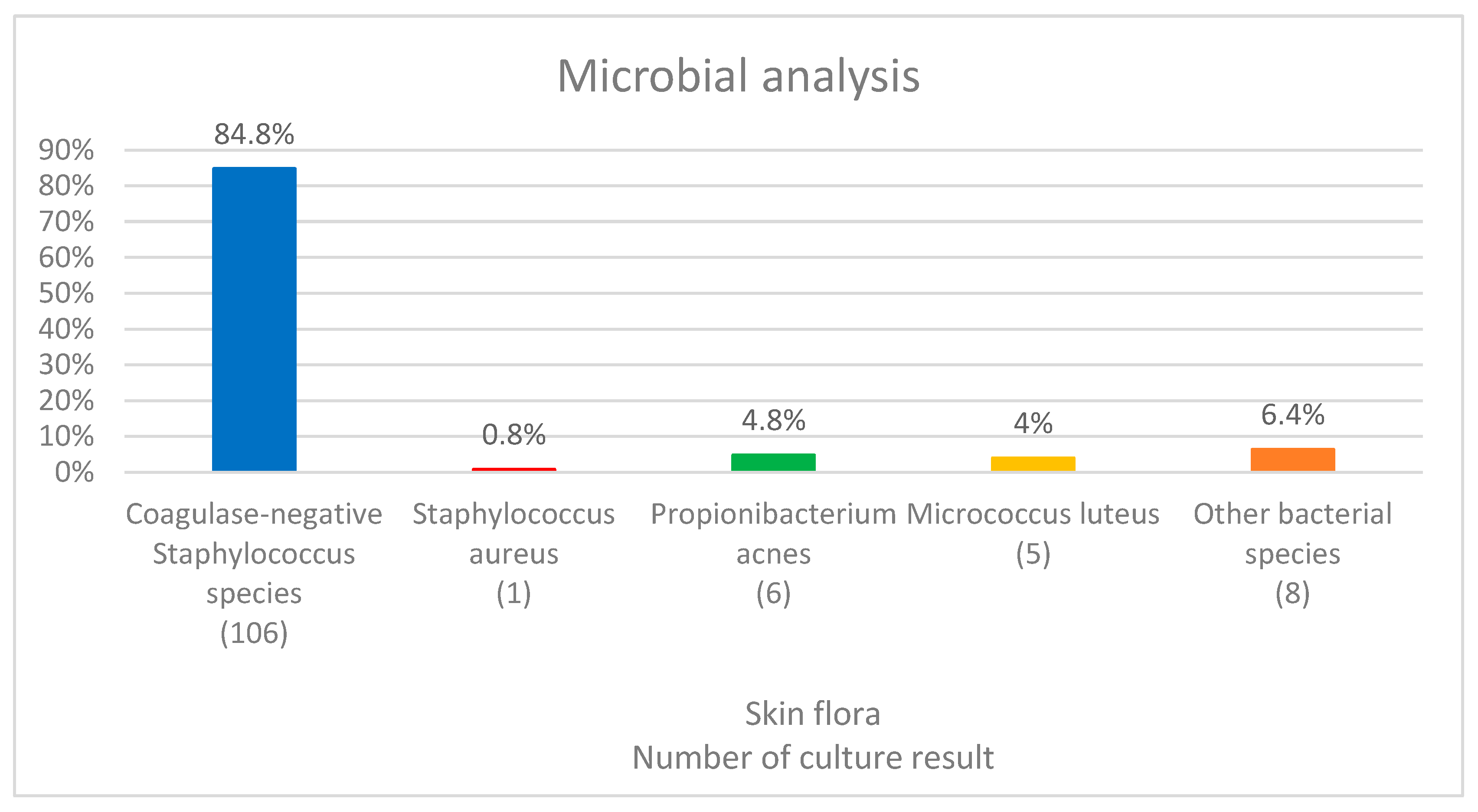
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Phillips, B.T.; Bishawi, M.; Dagum, A.B.; Khan, S.U.; Bui, D.T. A systematic review of antibiotic use and infection in breast reconstruction: What is the evidence? Plast. Reconstr. Surg. 2013, 131, 1–13. [Google Scholar] [PubMed]
- Spear, S.L.; Howard, M.A.; Boehmler, J.H.; Ducic, I.; Low, M.; Abbruzzesse, M.R. The infected or exposed breast implant: Management and treatment strategies. Plast. Reconstr. Surg. 2004, 113, 1634–1644. [Google Scholar] [PubMed] [Green Version]
- Ooi, A.S.H.; Song, D.H. Reducing infection risk in implant-based breast-reconstruction surgery: Challenges and solutions. Breast Cancer Targets Ther. 2016, 8, 161–172. [Google Scholar]
- Ziebuhr, W.; Krimmer, V.; Rachid, S.; Lößner, I.; Götz, F.; Hacker, J. A novel mechanism of phase variation of virulence in Staphylococcus epidermidis: Evidence for control of the polysaccharide intercellular adhesin synthesis by alternating insertion and excision of the insertion sequence element IS256. Mol. Microbiol. 1999, 32, 345–356. [Google Scholar] [PubMed]
- Mladick, R.A.; Netscher, D.T. Significance of Staphylococcus epidermidis causing subclinical infection. Plast. Reconstr. Surg. 2005, 115, 1426–1428. [Google Scholar] [PubMed]
- Palubicka, A.; Jaworski, R.; Wekwejt, M.; Swieczko-Zurek, B.; Pikula, M.; Jaskiewicz, J.; Zielinski, J. Surgical Site Infection after Breast Surgery: A Retrospective Analysis of 5-Year Postoperative Data from a Single Center in Poland. Medicina 2019, 21, 512. [Google Scholar]
- Page, C.P.; Bohnen, J.M.A.; Fletcher, J.R.; McManus, A.T.; Solomkin, J.S.; Wittmann, D.H. Antimicrobial Prophylaxis for Surgical Wounds: Guidelines for Clinical Care. Arch. Surg. 1993, 128, 79–88. [Google Scholar]
- Todd, B. New CDC Guideline for the Prevention of Surgical Site Infection. Am. J. Nurs. 2017, 117, 17. [Google Scholar]
- Bengtson, B.P.; Van Natta, B.W.; Murphy, D.K.; Slicton, A.; Maxwell, G.P. Style 410 US Core Clinical Study Group. Style 410 highly cohesive silicone breast implant core study results at 3 years. Plast. Reconstr. Surg. 2007, 120, 40–48. [Google Scholar]
- Blount, A.L.; Martin, M.D.; Lineberry, K.D.; Kettaneh, N.; Alfonso, D.R. Capsular contracture rate in a low-risk population after primary augmentation mammaplasty. Aesthet. Surg. J. 2013, 33, 516–521. [Google Scholar]
- Hidalgo, D.A.; Weinstein, A.L. Surgical Treatment for Capsular Contracture: A New Paradigm and Algorithm. Plast. Reconstr. Surg. 2020, 146, 516–525. [Google Scholar] [PubMed]
- Cunningham, B. The Mentor study on contour profile gel silicone MemoryGel breast implants. Plast. Reconstr. Surg. 2007, 120, 33–39. [Google Scholar]
- Headon, H.; Kasem, A.; Mokbel, K. Capsular contracture after breast augmentation: An update for clinical practice. Arch. Plast. Surg. 2015, 42, 532–543. [Google Scholar]
- Chun, Y.S.; Verma, K.; Rosen, H.; Lipsitz, S.; Morris, D.; Kenney, P.; Eriksson, E. Implant-based breast reconstruction using acellular dermal matrix and the risk of postoperative complications. Plast. Reconstr. Surg. 2010, 125, 429–436. [Google Scholar] [PubMed]
- Wixtrom, R.N.; Stutman, R.L.; Burke, R.M.; Mahoney, A.K.; Codner, M.A. Risk of breast implant bacterial contamination from endogenous breast flora, prevention with nipple shields, and implications for biofilm formation. Aesthet. Surg. J. 2012, 32, 956–963. [Google Scholar] [PubMed] [Green Version]
- Galdiero, M.; Larocca, F.; Iovene, M.R.; Francesca, M.; Pieretti, G.; D’Oriano, V.; Franci, G.; Ferraro, G.; d’Andrea, F.; Nicoletti, G.F. Microbial Evaluation in Capsular Contracture of Breast Implants. Plast. Reconstr. Surg. 2018, 141, 23–30. [Google Scholar]
- Bartsich, S.; Ascherman, J.A.; Whittier, S.; Yao, C.A.; Rohde, C. The breast: A clean-contaminated surgical site. Aesthet. Surg. J. 2011, 31, 802–806. [Google Scholar] [CrossRef]
- Krutmann, J. Pre- and probiotics for human skin. Clin. Plast. Surg. 2012, 39, 59–64. [Google Scholar]
- Ransjö, U.; Asplund, O.A.; Gylbert, L.; Jurell, G. Bacteria in the female breast. Scand. J. Plast. Reconstr. Surg. Hand. Surg. 1985, 19, 87–89. [Google Scholar]
- Noble, W.C. Antibiotic resistance in the staphylococci. Sci. Prog. 1997, 80, 5–20. [Google Scholar]
- Sytnik, S.I. Antibiotic sensitivity of staphylococci isolated from skin surface of the mammary glands of pregnant women. Antibiot. Khim. 1988, 33, 536–539. [Google Scholar]
- Pajkos, A.; Deva, A.K.; Vickery, K.; Cope, C.; Chang, L.; Cossart, Y.E. Detection of subclinical infection in significant breast implant capsules. Plast. Reconstr. Surg. 2003, 111, 1605–1611. [Google Scholar]
- National Healthcare Safety Network. Surgical Site Infection Event (SSI). Centres Dis. Control Prev. 2021, 1–39. [Google Scholar]
- Phillips, B.T.; Wang, E.D.; Mirrer, J.; Lanier, S.T.; Khan, S.U.; Dagum, A.B.; Bui, D.T. Current practice among plastic surgeons of antibiotic prophylaxis and closed-suction drains in breast reconstruction: Experience, evidence, and implications for postoperative care. Ann. Plast. Surg. 2011, 66, 460–465. [Google Scholar] [PubMed]
- Seng, R.; Kitti, T.; Thummeepak, R.; Kongthai, P.; Leungtongkam, U.; Wannalerdsakun, S.; Sitthisak, S. Biofilm formation of methicillin-resistant coagulase negative staphylococci (MR-CoNS) isolated from community and hospital environments. PLoS ONE 2017, 12, e0184172. [Google Scholar]
- Mirzabeigi, M.N.; Lee, M.; Smartt, J.M.; Jandali, S.; Sonnad, S.S.; Serletti, J.M. Extended trimethoprim/sulfamethoxazole prophylaxis for implant reconstruction in the previously irradiated chest wall. Plast. Reconstr. Surg. 2012, 129, 37–45. [Google Scholar]
- Feldman, E.M.; Kontoyiannis, D.P.; Sharabi, S.E.; Lee, E.; Kaufman, Y.; Heller, L. Breast implant infections: Is cefazolin enough? Plast. Reconstr. Surg. 2010, 126, 779–785. [Google Scholar]
- Berrondo, C.; Carone, M.; Katz, C.; Kenny, A. Adherence to Perioperative Antibiotic Prophylaxis Recommendations and Its Impact on Postoperative Surgical Site Infections. Cureus 2022, 14, e25859. [Google Scholar]
- Vardakas, K.Z.; Soteriades, E.S.; Chrysanthopoulou, S.A.; Papagelopoulos, P.J.; Falagas, M.E. Perioperative anti-infective prophylaxis with teicoplanin compared to cephalosporins in orthopaedic and vascular surgery involving prosthetic material. Clin. Microbiol. Infect. 2005, 11, 775–777. [Google Scholar]
- Choi, J.H.K.; Duong, H.A.; Williams, S.; Lee, J.; Oh, M.; Rosen, C.; Lee, Y.P.; Bhatia, N. The efficacy of bactrim in reducing surgical site infections after spine surgery. N. Am. Spine Soc. J. 2022, 9, 100095. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Value (Range, %) |
|---|---|
| Total number of swabs | 220 |
| Age (mean ± SD, y) | 49.3 ± 8.3 (27–68) |
| BMI (mean ± SD, kg/m2) | 23.6 ± 3.7 (16.5–37.2) |
| Diabetes (%) | 2 (0.9) |
| Smoking (%) | 0 (0) |
| Neoadjuvant chemotherapy (%) | 61 (27.8) |
| Neoadjuvant Chemotherapy | Methicillin Resistance Group (n = 51) | Methicillin-Susceptible Group (n = 74) | p-Value |
|---|---|---|---|
| Yes | 18 | 14 | 0.039 |
| No | 33 | 60 |
| Characteristic | Methicillin Resistance Group (n = 51) | Methicillin-Susceptible Group (n = 74) | p-Value |
|---|---|---|---|
| Age (mean, y) | 46.16 | 47.71 | 0.235 |
| BMI (mean, kg/m2) | 23.9 | 22.5 | 0.056 |
| Susceptible (%) | Resistant (%) | |
|---|---|---|
| Oxacillin | 0 | 100 |
| Benzylpenicillin | 5.9 | 94.1 |
| Fusidic Acid | 14 | 86 |
| Erythromycin | 42 | 58 |
| Cefoxitin | 44.4 | 55.6 |
| Tigecycline | 47.2 | 52.8 |
| Mupirocin | 47.8 | 52.2 |
| Tetracycline | 62 | 24.5 |
| Gentamicin | 66 | 38 |
| Clindamycin | 66 | 34 |
| Ciprofloxacin | 88 | 12 |
| Teicoplanin | 94 | 6 |
| Telithromycin | 96 | 4 |
| Rifampicin | 100 | 0 |
| Habekacin | 100 | 0 |
| Quinupristin/Dalfopristin | 100 | 0 |
| Linezolid | 100 | 0 |
| Vancomycin | 100 | 0 |
| Nitrofurantoin | 100 | 0 |
| Trimethoprim/Sulfamethoxazole | 100 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.Y.; Yi, H.-S.; Park, J.-J.; In, S.-K.; Kim, H.-I.; Park, J.-H.; Lee, W.-H.; Kim, Y.-S. Changing Susceptibility of Staphylococci in Patients with Implant-Based Breast Reconstructions: A Single-Center Experience. Medicina 2022, 58, 1130. https://doi.org/10.3390/medicina58081130
Kim HY, Yi H-S, Park J-J, In S-K, Kim H-I, Park J-H, Lee W-H, Kim Y-S. Changing Susceptibility of Staphylococci in Patients with Implant-Based Breast Reconstructions: A Single-Center Experience. Medicina. 2022; 58(8):1130. https://doi.org/10.3390/medicina58081130
Chicago/Turabian StyleKim, Hyo Young, Hyung-Suk Yi, Jeong-Jin Park, Seok-Kyung In, Hong-Il Kim, Jin-Hyung Park, Woon-Hyoung Lee, and Yoon-Soo Kim. 2022. "Changing Susceptibility of Staphylococci in Patients with Implant-Based Breast Reconstructions: A Single-Center Experience" Medicina 58, no. 8: 1130. https://doi.org/10.3390/medicina58081130