1. Introduction
The management of anticoagulation in patients with a mechanical prosthetic heart valve who are receiving long-term oral anticoagulant therapy and are undergoing elective non-cardiac surgery can be especially difficult and problematic [
1,
2]. Temporary discontinuation of anticoagulants increases the risk of valve thrombosis and systemic embolism [
1,
2,
3,
4]. On the other hand, continuing anticoagulants perioperative, or stopping and restarting anticoagulants too soon after surgery, can cause life-threatening bleeding [
5]. The optimal anticoagulation strategy has to minimize the risk of thromboembolism, without causing excessive postoperative bleeding [
6,
7,
8].
The pharmacokinetic and pharmacodynamic properties of low-molecular-weight heparins (LMWH) [
9,
10,
11,
12] are attractive compared to other anticoagulant strategies, but unfortunately there are not enough studies to take into account their safety and effectiveness for the anticoagulation of mechanical heart valve prosthesis. Unlike unfractionated heparin (UH), LMWH have further predictable kinetics, are less protein bound, have lower potential for platelet activation and bear no monitoring, so they are a better alternative for the perioperative anticoagulation in patients with mechanical heart valves undergoing non-cardiac interventions [
9]. The few studies of LMWH used in general surgery, specifically in patients with heart valve prosthesis, have shown a decrease in the incidence of prosthesis obstructive dysfunctions, as well as an increase in postoperative convenience and the quality of life in LMWH versus UH patients [
12,
13,
14,
15,
16]. Large-scale studies of LMWH given in the perioperative anticoagulant therapy of mechanical prosthetic valve patients undergoing general surgery interventions have never been conducted before.
2. Materials and Methods
We performed a real-world data study with open study period, which included 380 consecutive patients from a single center with mechanical prosthetic heart valves in mitral, aortic or tricuspid positions/combinations of the three, who underwent noncardiac surgery interventions between 1 January 2017 and 1 January 2020. Non-eligibility criteria were listed in
Table 1. Study drop-out criteria were severe thrombocytopenia, active bleeding. The essential inclusion criteria (gender, age, diagnosis), the duration of treatment and assessment criteria were similar in the two treatment groups (
p < 0.0001). The protocol was approved by the institute management, and every patient signed the informed consent form.
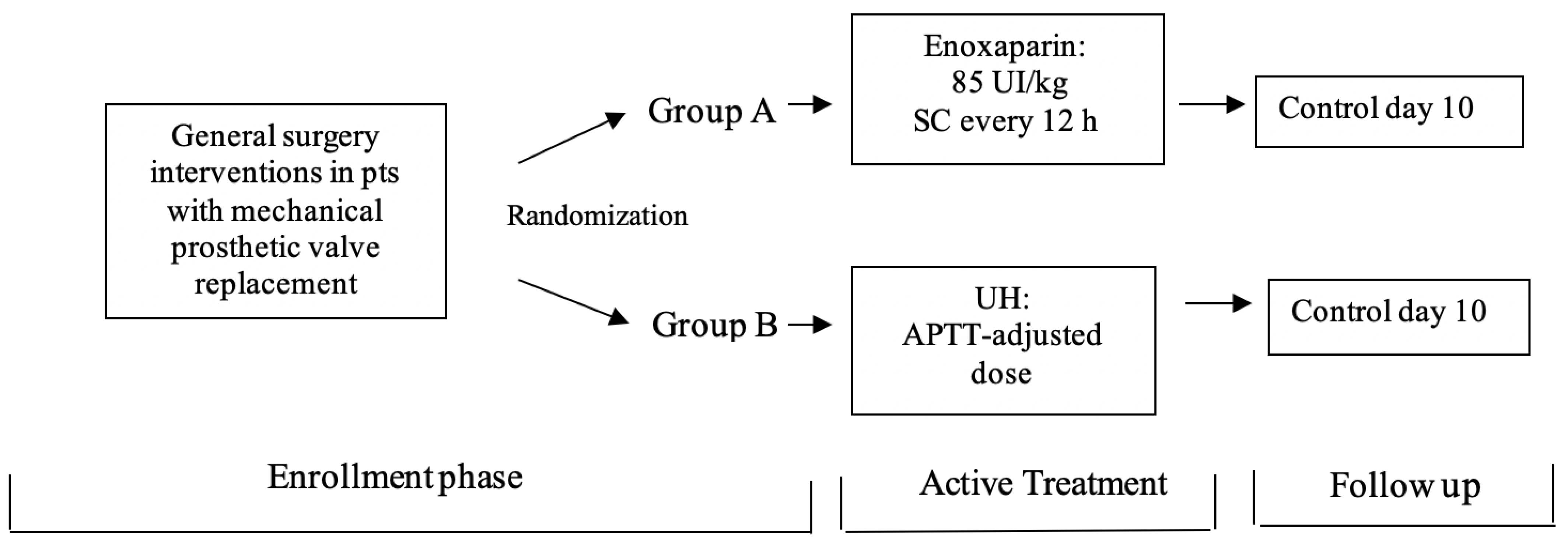
Patients were randomized (using stratified randomization method) to receive enoxaparin or UH as antithrombotic treatment (
Figure 1): Group A—Enoxaparin (E) SC 85 IU/kg twice daily (every 12 h); Group B—Unfractionated heparin (UH) given as IV continuous infusion of doses adjusted to maintain the APTT at 2.5 the normal value. The treatment was given for a period of no less than 72 h and up to 10 days. We measured INR after admission the first hours and before starting the enoxaparin treatment. INR was considered correct if it was in the target range of the recently published recommendations in managing oral anticoagulation for the valvular prosthesis type, or incorrect if it was not [
17]. For each patient, we prospectively determined the following: demographic details, the reason for stopping acenocumarol, the global risk for thromboembolic events, INR before starting enoxaparin/UH, days number with enoxaparin/UH and mean anti-Xa activity level during treatment and the appearance of hemorrhagic or thromboembolic events during hospitalization and follow-up.
The bleeding events were classified as minor events (which did not require additional testing requirement), and major events (life-threatening or fatal bleeding episodes needing transfusion or hospitalization).
We assessed clinical and laboratory parameters both at baseline and at the end of the treatment. From clinical point of view, we measured: NYHA class for heart failure, clinical parameters for the prostheses, patient compliance and quality of life. Laboratory parameters included: the usual blood tests, echocardiographic measurements of the prosthetic valves and clotting tests (INR for both arms and APTT for arm B) [
18]. Based both on clinical criteria and through thoracic and transesophageal echocardiography we diagnosed early development of prosthetic thrombosis.
Enoxaparin dosing was performed according to patients’ kidney function. In those with normal estimated glomerular filtration ratio (eGFR), the standard enoxaparin dose was 1 mg/kg administered subcutaneously twice a day once the INR was below 1.5. Patients with serum creatinine ≥ 1.5 mg/dL (≥133 μmol/L) received the lowest dose of E required to obtain an anti-Xa activity level above 0.4 IU/mL [
18]. Enoxaparin was withheld in all patients 12–18 h before the procedure and restarted with the same schedule after the procedure once hemostasis was achieved.
In patients with a bleeding episode, we stopped acenocumarol and started enoxaparin at the prophylactic dose of 40 mg/day, immediately after INR was below 1.5. Additionally, we kept Enoxaparin until hemostasis was achieved, and we considered that the risk of new bleeding episodes is low, after which we administrated the standard dose of 1 mg/kg two times daily. We restarted Acenocumarol at the patient’s usual dosage a few days before discharge, and we stopped enoxaparin when INR became > 2.
We measured anti-Xa activity six hours after administration of enoxaparin and, after that, depending on the level of anti-Xa activity, new measurements were taken at 3-day intervals. Patients were followed up using telemedicine application/telephone, clinical evaluation and echocardiography during hospitalization, and in the first three months after surgery.
The primary endpoints were the composite of 30-day mortality, in-hospital prosthesis obstructive dysfunction–thrombotic obstruction (safety endpoints), duration of hospital stay and immobilization, and the above endpoint plus in-hospital intracranial hemorrhage or in-hospital major bleeding other than intracranial bleeding (primary-efficacy-plus-safety endpoint). Safety data were reported monthly to the safety monitoring committee. Safety data were reported monthly, and stroke cases were evaluated by an independent commission in which the members were blinded of treatment assignment. The data were collected and processed using the Visual Fox Pro Excel, EpiInfo, Systat, and SPSS programs. We defined a detailed analysis plan before the database was locked, but with no confirmatory pre-specified statistical hypothesis. For categorical data we used numbers and percentages, and for continuous data mean ± standard deviation or median (interquartile range) as appropriate. For the pairwise comparisons of primary interest, we generate risk ratios and CIs (CI = confidence index) which were presented with the two-sided 95% CI of the relative risk and with normal p values. For the primary endpoints the study groups were compared using Kaplan–Meier curves and log-rank tests. Additionally, a two-sided 95% CI was calculated for each endpoint, and the treatment groups were compared using an overall chi-square test, alpha level value of 0.05. The frequency of the primary-efficacy-plus-safety endpoint for the UH group as a reference group was 17.7%. Taking into account the basis of phase-II studies, we assumed that the experimental group with E would result in better, or at least similar outcomes when compared with standard treatment. Therefore, based on the non-inferiority of the experimental group versus the reference group, we performed the sample size and power calculations. The study’s power to exclude was 80%, with 95% one-sided confidence. Compared with the reference group, we found in the experimental treatment group 1% higher rate for the primary endpoints, 1.7% lower rate for the efficacy endpoint and 2% lower rate for both the efficacy and safety endpoint.
3. Results
We found similar baseline characteristics in the two groups (
Table 2).
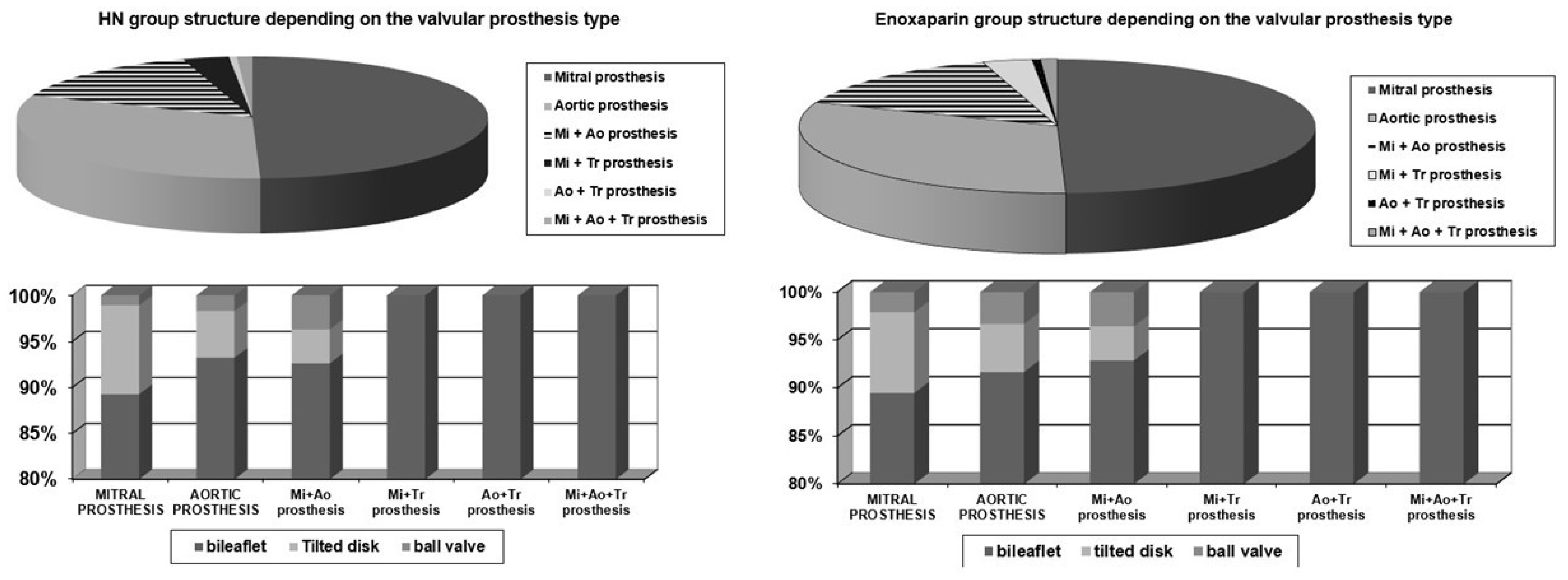
Depending on the type of the valve prosthesis, the two groups were homogenous (
Figure 2).
There were no significant differences between the study groups concerning in-hospital concomitant medications (
Table 3). The proportion of patients receiving antiplatelet therapy with Aspirin, Ticlopidine, or Clopidogrel was 7.81% in group A and 7.45% in group B.
The primary efficacy and efficacy-plus-safety endpoints and their components in the treatment groups are shown in
Table 4.
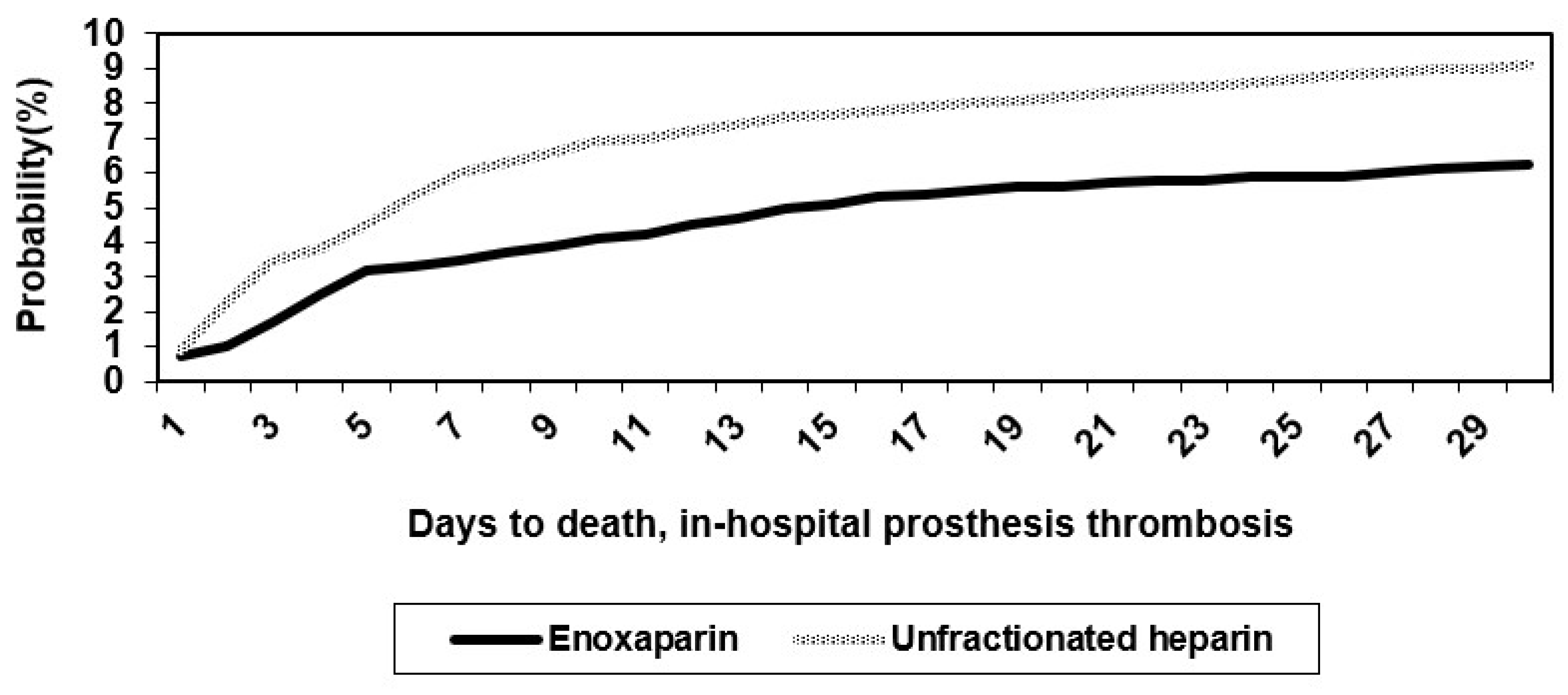
The combined efficacy and safety outcome in the UH group of 20/188 patients (10.64%) was similar to that estimated before the trial commenced (11%). The Kaplan–Meier curves for these primary endpoints are shown in
Figure 3.
Log-rank tests were highly significant. Early after treatment, the curve for the E started to separate from that of UH, and also, at 48 h, differences between the two groups in the primary endpoints were already present. For the primary efficacy endpoint, the event rates were 6.25% for the E group and 8.51% for the UH group (
p < 0.0001). For the primary-efficacy-plus-safety endpoint, the rates were 6.25% for the E group and 9.04% for the UH group (
p = 0.02). The relative risks in the two groups are presented in
Table 5.
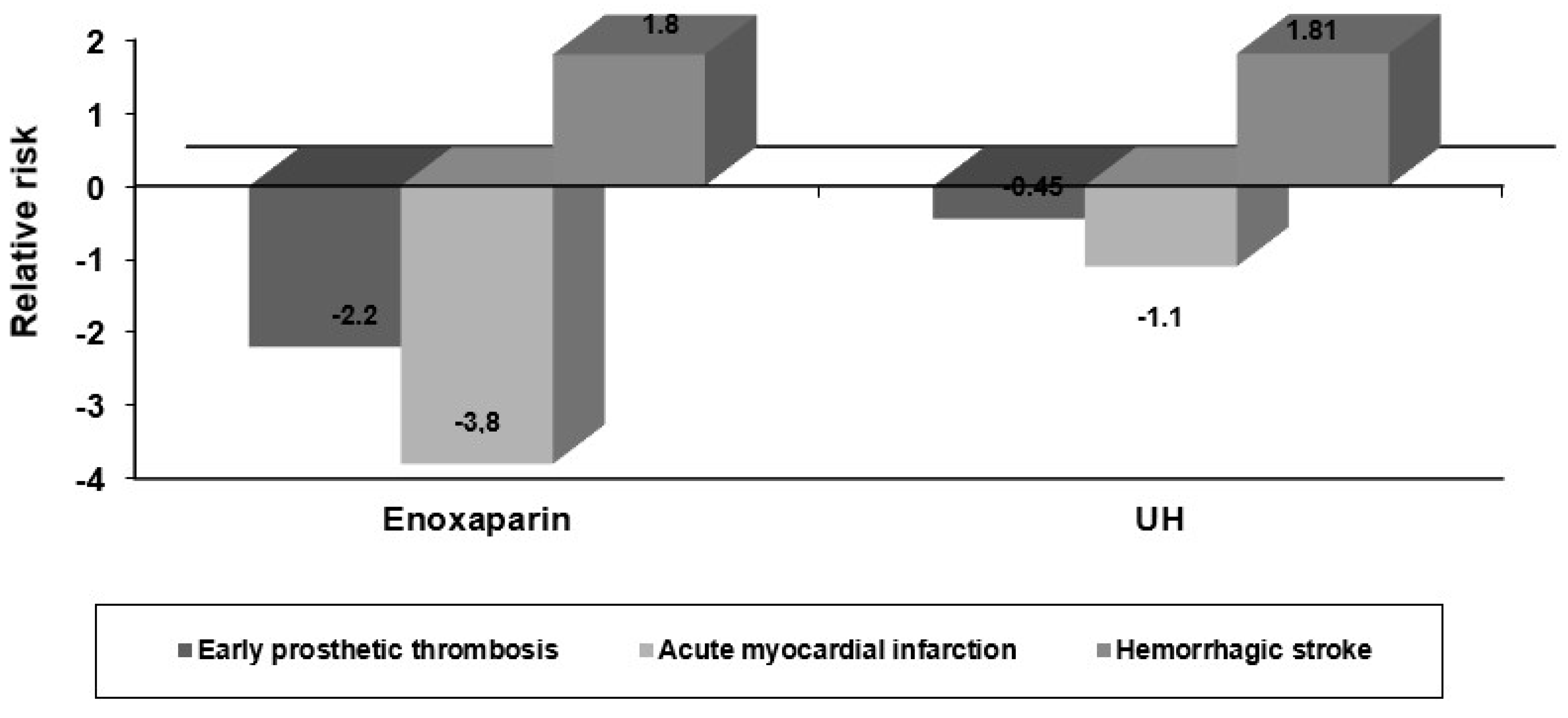
The composite endpoints rates were lower in the group of patients treated with E compared with patients treated with UH. The
p values resulting from conventional statistical testing for E versus HN were statistically significant, being 0.0002 and 0.0003, respectively, for the primary-efficacy-plus-safety composite endpoints. Additionally, in patients treated with E, in-hospital prosthesis thrombosis occurred less frequently than in those treated with UH. The in-hospital death rates were lower in the E group (6.25%) compared to UH group (8.51%). No significant differences in other major cardiovascular complications were seen, with the exception of a significantly lower rate for postoperative myocardial infarction in patients with risk factors in the E versus the UH group (
Figure 4).
The mean duration of hospitalization in the E group was 10.5 ± 4.3 days, compared to 14.5 ± 5.8 days in the UH group. The mean immobilization interval during the immediate postoperative period in group A versus group B was 1.02 ± 3 days versus 5.5 ± 2.8 days, respectively.
Concerning the complications of anticoagulant therapy, the in-hospital strokes data are summarized in
Table 6.
We found similar rates for total stroke and intracranial hemorrhage in the two study groups with a few number of hemorrhagic conversions in each of these. The rates of non-cerebral bleeding complications, number of patients needing transfusions and the thrombocytopenia rates are presented in
Table 7.
In patients with antiplatelet associated treatment with Aspirin, Ticlopidine or Clopidogrel, we found significantly more major bleeding complications (
p = 0.0001), more need for transfusions (
p = 0.002) and a higher rate of thrombocytopenia (
p = 0.001). Additionally, in patients older than 75 years and in diabetics, the rate of major bleeding complications was three times higher in those with associated antiplatelet therapy (4% versus 14% and 2% versus 7%, respectively). Although the differences were not significant, we found more major and minor bleeding complications in the UH group compared with E group, with no more episodes of thrombocytopenia in the E group (
Figure 5).
The total number of re-hospitalizations was similar in the two treatment groups (11.41% in the E group, 11.7% in the UH group) with a few additional strokes occurring after hospital discharge in the two groups. The probability of death, early prosthetic thrombosis and perioperative myocardial infarction were smaller with E versus UH. No significant changes in liver function tests and blood biochemistry were recorded in the groups.
4. Discussion
Despite the high global risk of thromboembolism in our study, during hospitalization or follow-up (with a mean of 2.8 months), no thromboembolic event was detected. Although the method used during the follow-up for detecting all the thromboembolic events (particularly valve thrombosis) may have limitations, we think it is sensitive enough for the detection of those with clinical or ecographic signs, who are reported mostly in other studies.
Regarding safety, we observed only one important bleeding complication in the E group, but we have to take into account that most of the procedures were in low-to-medium bleeding risk, and the mean levels of anti-Xa activity were in the lower limit of the therapeutic range (95% of patients had anti-Xa activity < 1.1 IU/mL). In patients who bled during E treatment, the highest anti-Xa activity was 1.1 IU/mL.
E has shown increased efficacy over UH in the perioperative anticoagulation in general surgery interventions of mechanical prosthetic heart valve patients. Subjective measures in patients achieving a more favorable response included the improvement of clinical status with decreased hospitalization time, decreased immobilization and so fewer gluteal ulcerations and fewer postoperative episodes of depression and anxiety. Objective measures of E efficacy in patients with mechanical prosthetic heart valves included the following: maintenance of all ultrasound prosthetic functioning parameters within the normal range, absence of early prosthesis thrombosis in the study group, decreased parenteral anticoagulation period with rapid achievement of optimal INR. The probability of death was smaller in the E group compared with the UH group. No major hemorrhagic event was reported in either of the two groups. In the UH group, we found more episodes of minor hemorrhage and thrombocytopenia. Additionally, patients’ compliance and quality of life were improved due to shortened hospital stay, fewer coagulation tests (every 6 h for UH), increased dosing convenience (SC every 12 h for E versus continuous infusion for UH), shortened immobilization during the immediate postoperative period with subsequent improvement in the psychological status, as well as the lack of significant side effects.
Limitations
First, although this is one of the largest studies using E for perioperative anticoagulation in patients with mechanical valve prosthesis, the number of patients was still moderate. Second, data on thromboembolic events (particularly valve thrombosis) were obtained from clinical evaluation and transthoracic echocardiography rather than transesophageal eco. However, the cardiologists performing these examinations were experienced in evaluating patients with valve prostheses. Third, the study design and the number of patients did not allow conclusions about the efficacy and safety of E in these patients compared with other methods. Taking into account that our patients were not selected, our results represent a real clinical practice observation of using E perioperatively in mechanical heart valves patients.
5. Conclusions
Considering efficacy and safety and additional advantages, such as the ease of administration, lack of need for long-term monitoring of anticoagulation, and reduction in the hospitalization duration, E should be regarded as an attractive alternative pharmacological anticoagulation strategy in patients with mechanical heart valves undergoing noncardiac interventions, thus deserving further study.
Author Contributions
Conceptualization, L.I. and M.R.-A.; methodology, L.I.; software, L.I. and G.C.; validation, L.I. and A.A.; formal analysis, L.I. and G.C.; investigation, A.A.; data curation, L.I.; writing—original draft preparation, L.I., G.C. and M.R.-A.; writing—review and editing, A.A.; supervision, L.I.; project administration, L.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Institute for Cardiovascular Diseases C.C. Iliescu (protocol code 758/12.12.2018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Acknowledgments
Special thanks to Danut Andronesi—General Surgeon Fundeni Clinical Institute, Bucharest, Romania.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rechenmacher, S.J.; Fang, J.C. Bridging Anticoagulation: Primum Non Nocere. J. Am. Coll. Cardiol. 2015, 66, 1392–1403. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Fleisher, L.A.; Jneid, H.; Mack, M.J.; McLeod, C.J.; O’Gara, P.T.; et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e1159–e1195. [Google Scholar] [CrossRef] [PubMed]
- Douketis, J.D.; Spyropoulos, A.C.; Spencer, F.A.; Mayr, M.; Jaffer, A.K.; Eckman, M.H.; Dunn, A.S.; Kunz, R. Perioperative management of antithrombotic therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141 (Suppl. S2), e326S–e350S, Erratum in: Chest 2012, 141, 1129. [Google Scholar] [CrossRef] [PubMed]
- Mérie, C.; Køber, L.; Skov Olsen, P.; Andersson, C.; Gislason, G.; Skov Jensen, J.; Torp-Pedersen, C. Association of warfarin therapy duration after bioprosthetic aortic valve replacement with risk of mortality, thromboembolic complications, and bleeding. JAMA 2012, 308, 2118–2125. [Google Scholar] [CrossRef] [PubMed]
- Shoeb, M.; Fang, M.C. Assessing bleeding risk in patients taking anticoagulants. J. Thromb. Thrombolysis 2013, 35, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Yanagawa, B.; Whitlock, R.P.; Verma, S.; Gersh, B.J. Anticoagulation for prosthetic heart valves: Unresolved questions requiring answers. Curr. Opin. Cardiol. 2016, 31, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Iliuta, L.; Filipescu, D.; Macarie, C. Low Molecular Weight Heparin versus Unfractionated heparin for The Perioperative Anticoagulant Therapy in Patients Undergoing Mechanical Prosthetic Valve Replacement. Eur. Heart J. 2006, 27, 833. [Google Scholar]
- Whitlock, R.P.; Sun, J.C.; Fremes, S.E.; Rubens, F.D.; Teoh, K.H. Antithrombotic and thrombolytic therapy for valvular disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141, e576S–e600S. [Google Scholar] [CrossRef] [PubMed]
- White, R.H.; Ginsberg, J.S. Low-molecular-weight heparins: Are they all the same? Br. J. Haematol. 2003, 121, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Kearon, C.; Akl, E.A.; Ornelas, J.; Blaivas, A.; Jimenez, D.; Bounameaux, H.; Huisman, M.; King, C.S.; Morris, T.A.; Sood, N.; et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest 2016, 149, 315–352, Erratum in: Chest 2016, 150, 988. [Google Scholar] [CrossRef] [PubMed]
- Xia, Z.N.; Zhou, Q.; Zhu, W.; Weng, X.S. Low molecular weight heparin for the prevention of deep venous thrombosis after total knee arthroplasty: A systematic review and meta-analysis. Int. J. Surg. 2018, 54, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Meurin, P.; Tabet, J.Y.; Weber, H.; Renaud, N.; Ben Driss, A. Low-molecular-weight heparin as a bridging anticoagulant early after mechanical heart valve replacement. Circulation 2006, 113, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Kindo, M.; Gerelli, S.; Minh, T.H.; Zhang, M.; Meyer, N.; Announe, T.; Bentz, J.; Mansour, Z.; Mommerot, A.; Petit-Eisenmann, H.; et al. Exclusive low-molecular-weight heparin as bridging anticoagulant after mechanical valve replacement. Ann. Thorac. Surg. 2014, 97, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Erkens, P.M.; Prins, M.H. Fixed dose subcutaneous low molecular weight heparins versus adjusted dose unfractionated heparin for venous thromboembolism. Cochrane Database Syst. Rev. 2010, 8, CD001100. [Google Scholar] [CrossRef]
- Spandorfer, J.M.; Lynch, S.; Weitz, H.H.; Fertel, S.; Merli, G.J. Use of enoxaparine for the chronically anticoagulated patient before and after procedures. Am. J. Cardiol. 1999, 84, 478–480. [Google Scholar] [CrossRef]
- Ryan, F.; Byrne, S.; O’Shea, S. Managing oral anticoagulation therapy: Improving clinical outcomes. A review. J. Clin. Pharm. Ther. 2008, 33, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., III; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2021, 77, e25–e197. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.; Szeki, I.; Nash, M.J.; Thachil, J. Anticoagulation in chronic kidney disease patients-the practical aspects. Clin. Kidney J. 2014, 7, 442–449. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}