
Multi-Modal Brain Tumor Detection Using Deep Neural Network and Multiclass SVM


Abstract
:1. Introduction
- A linear contrast stretching method is used to improve the edge details of the original image as a pre-processing step;
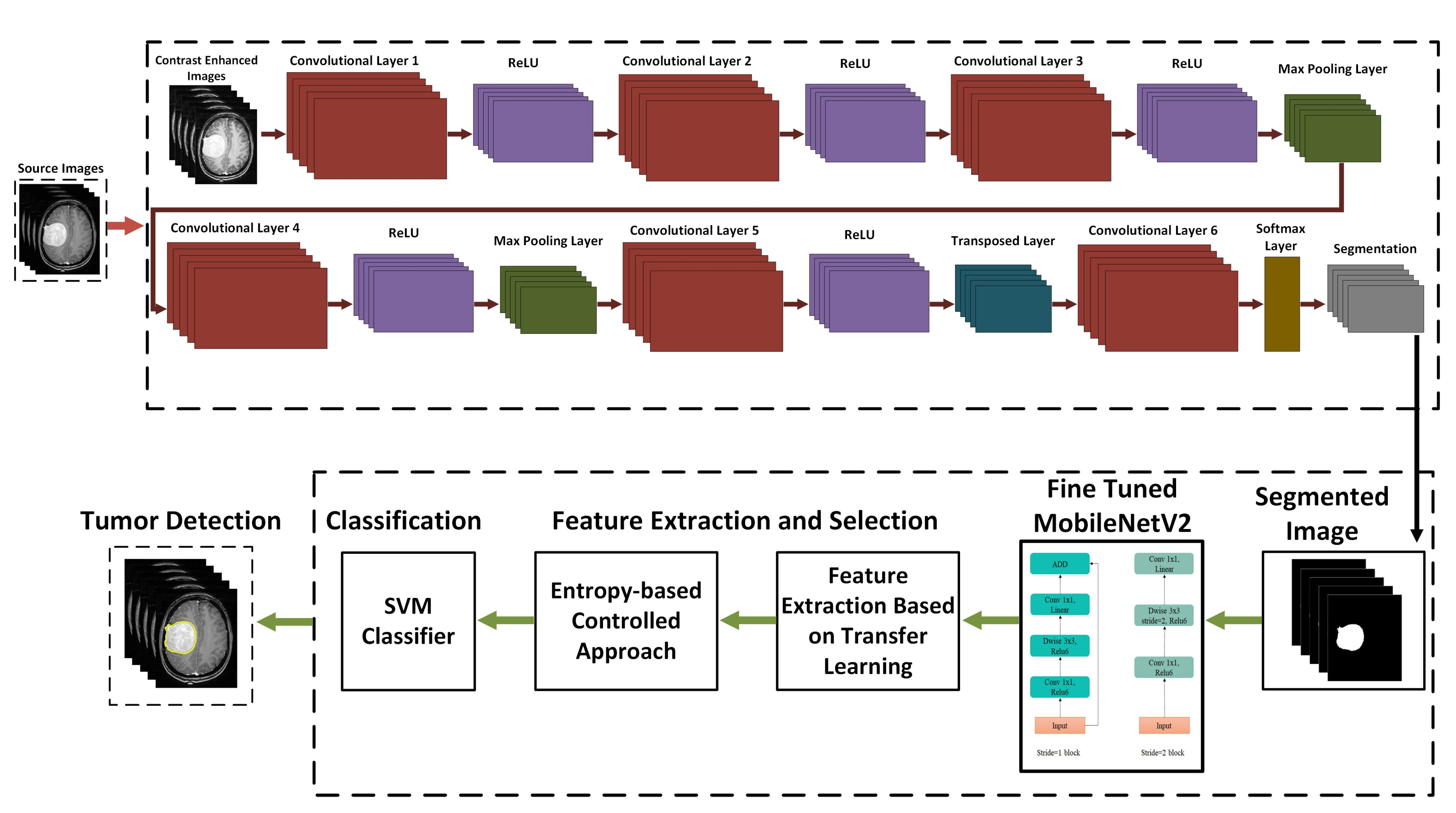
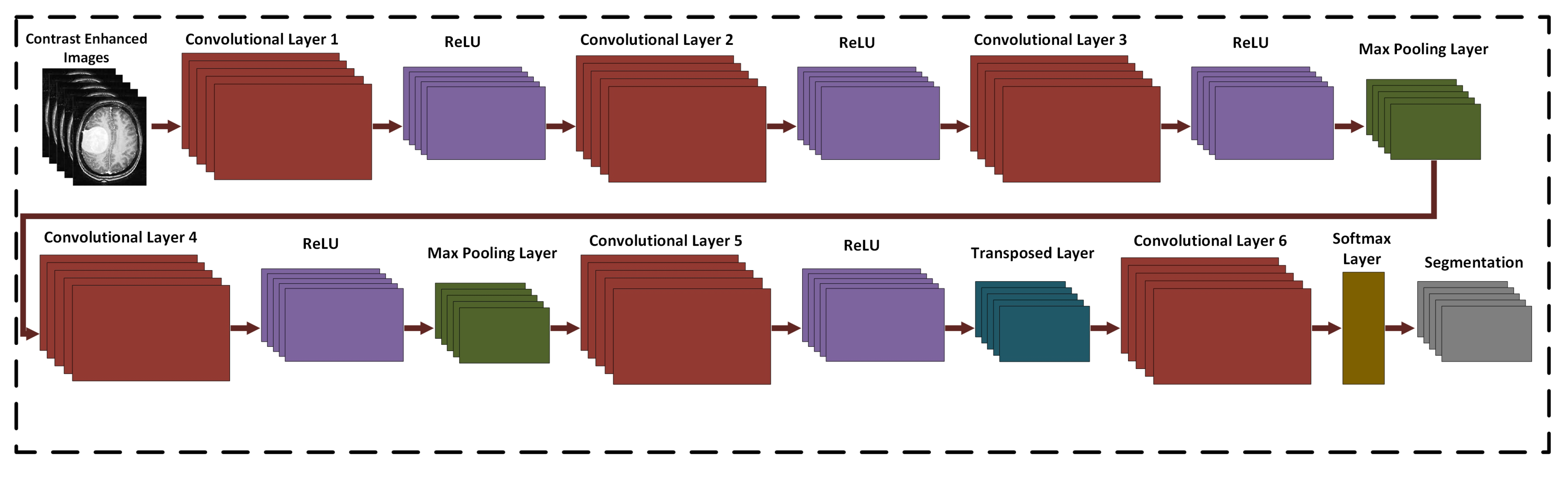
- Designed a custom 17-layered CNN architecture for brain tumor segmentation, which is trained from the scratch to recognize the tumor area;
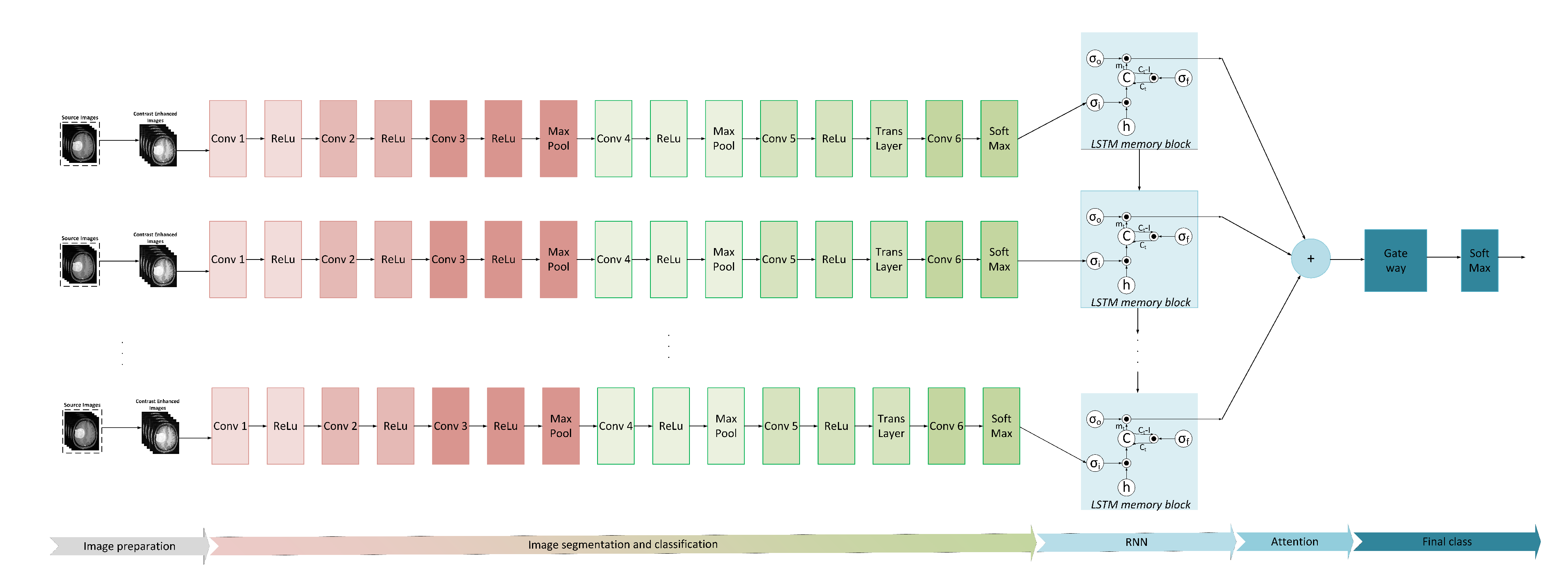
- We used transfer learning from modified MobileNetV2 to retrieve the selected datasets for the deep feature extraction;
- To optimize feature selection, we use an entropy-based controlled method, where the best features are selected based on the entropy value. The final features are classified using a multi-class SVM classifier;
- To confirm the stability of the proposed algorithm, a complete statistical analysis and comparison with the most modern methods are conducted.
2. Related Work
3. The Proposed Framework
3.1. Contrast Enhancement
3.2. Tumor Segmentation
3.3. Modified MobileNetV2 for Feature Extraction
3.4. Deep Feature Extraction Using Transfer Learning
3.5. Feature Selection and Classification
4. Experimental Setup
4.1. Simulation Setup
4.2. Dataset
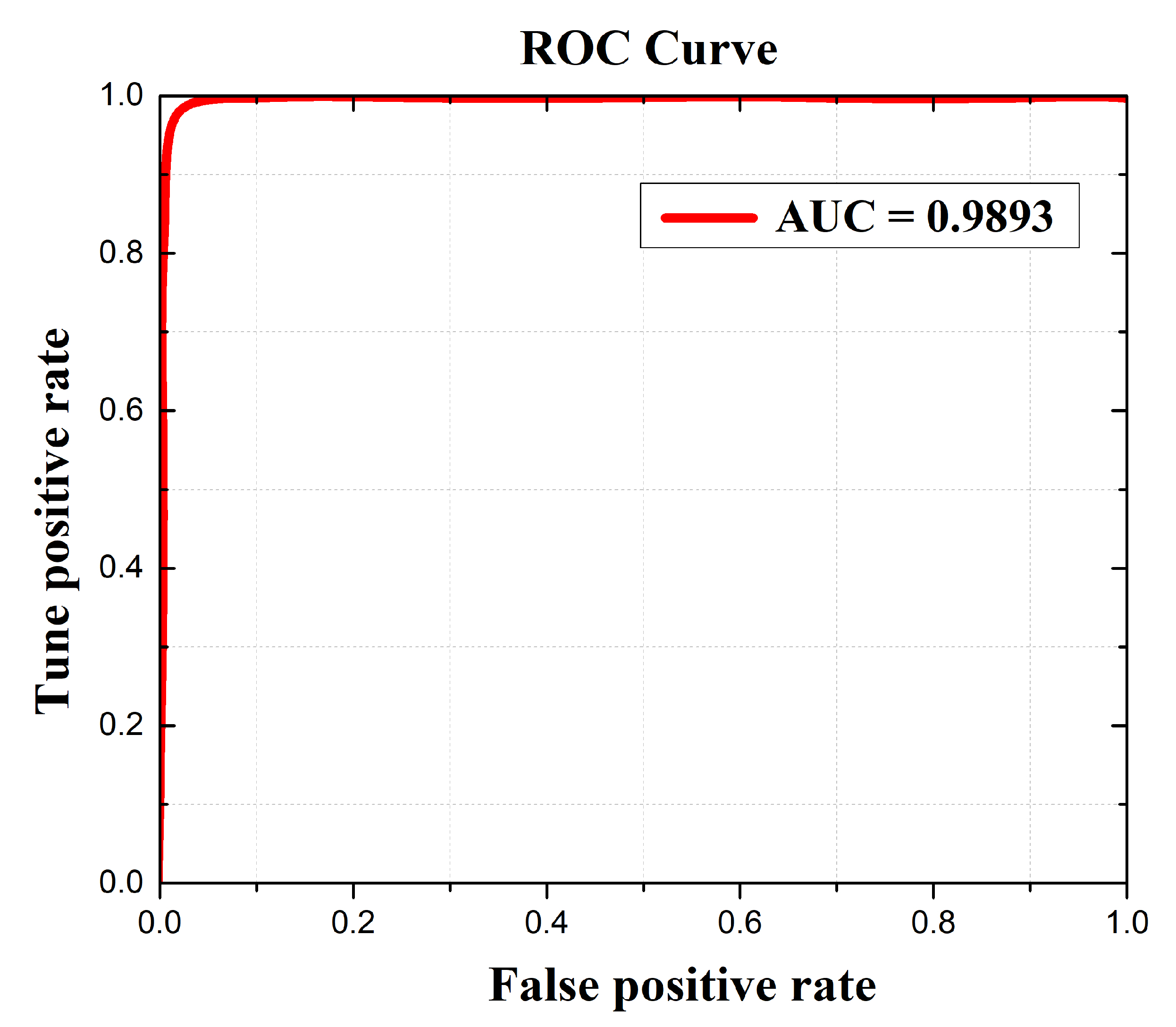
4.3. Evaluation Matrices
5. Results and Discussion
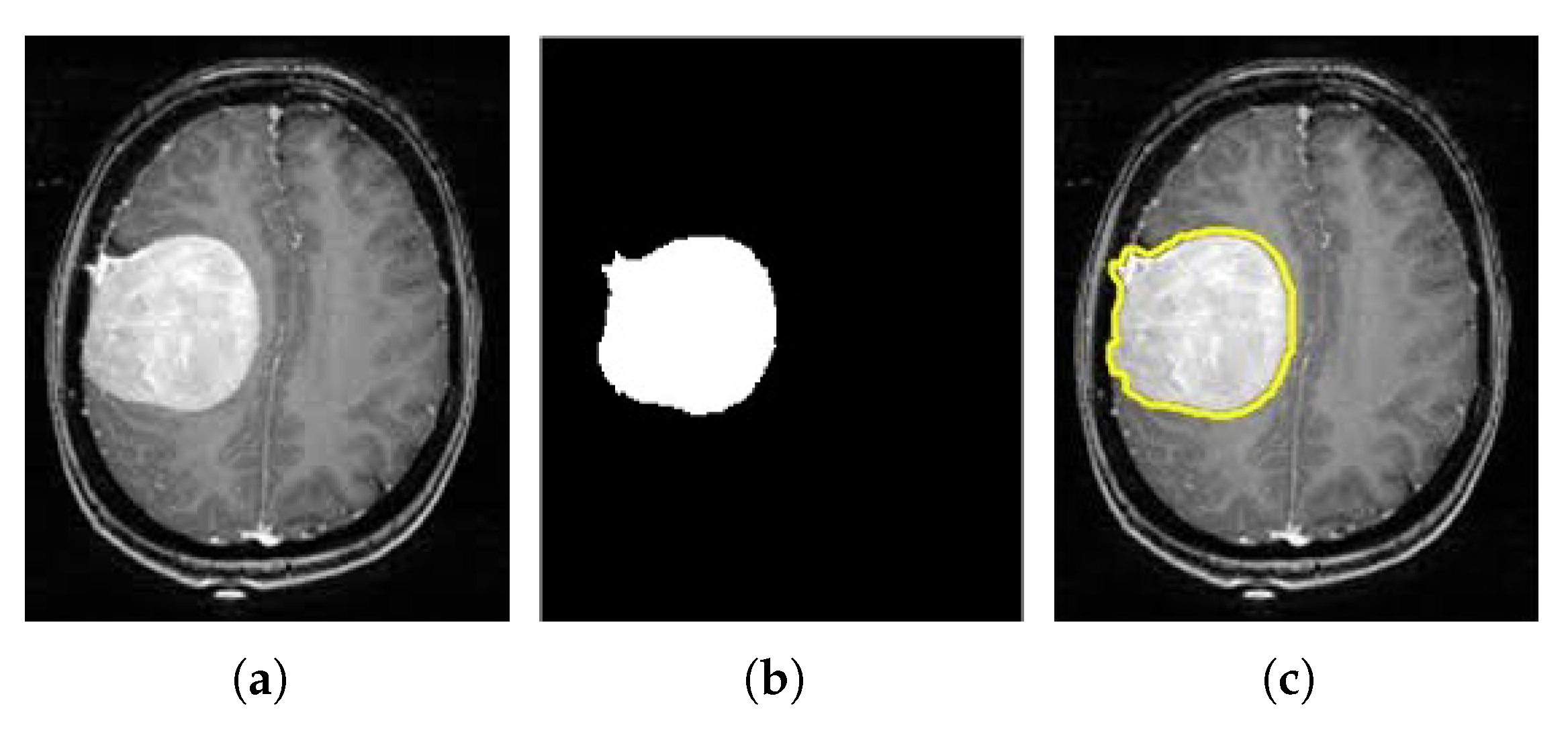
5.1. Brain Tumor Segmentation Results
5.2. Classification Results
5.2.1. BraTS 2018 Dataset Results
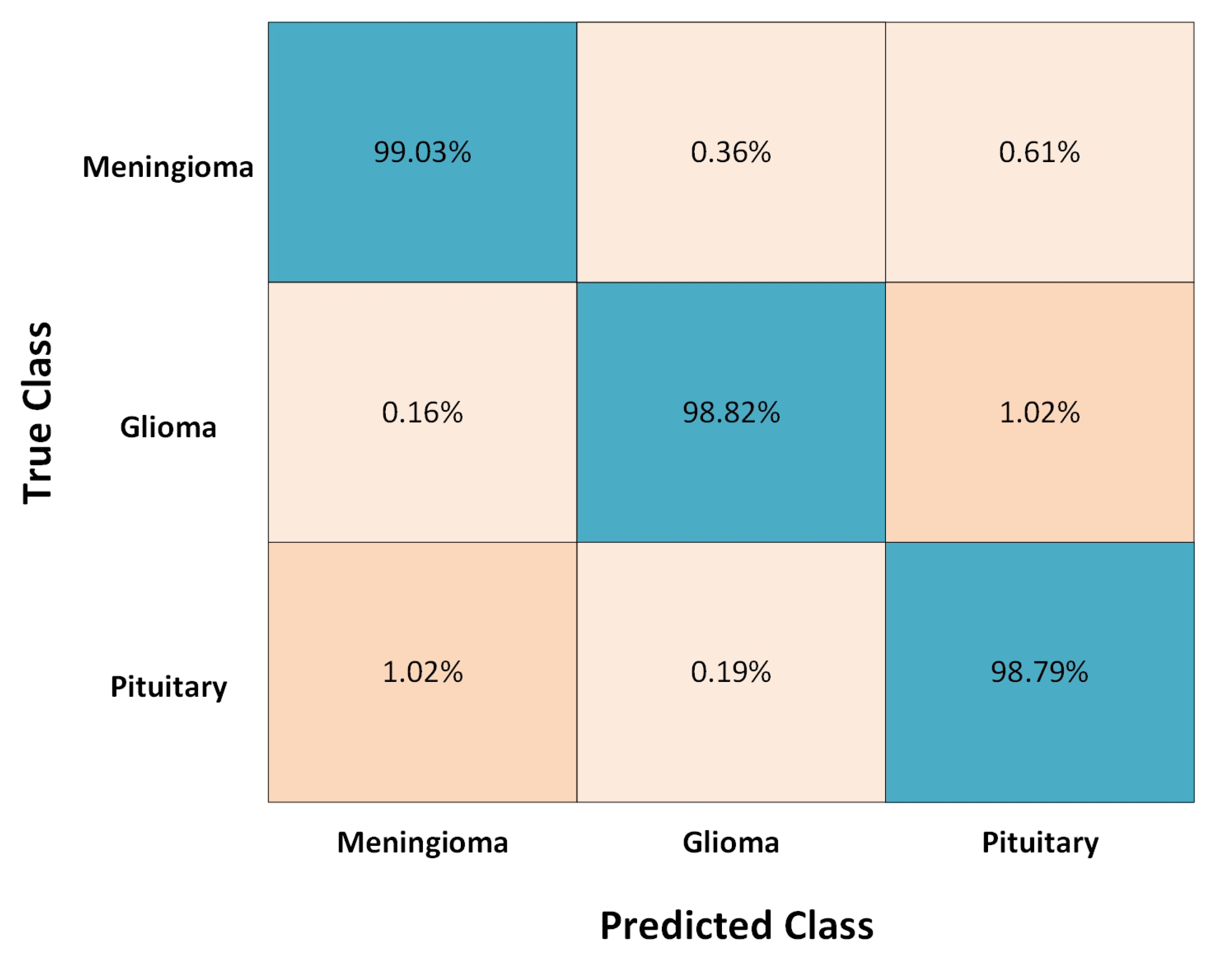
5.2.2. Figshare Dataset Results
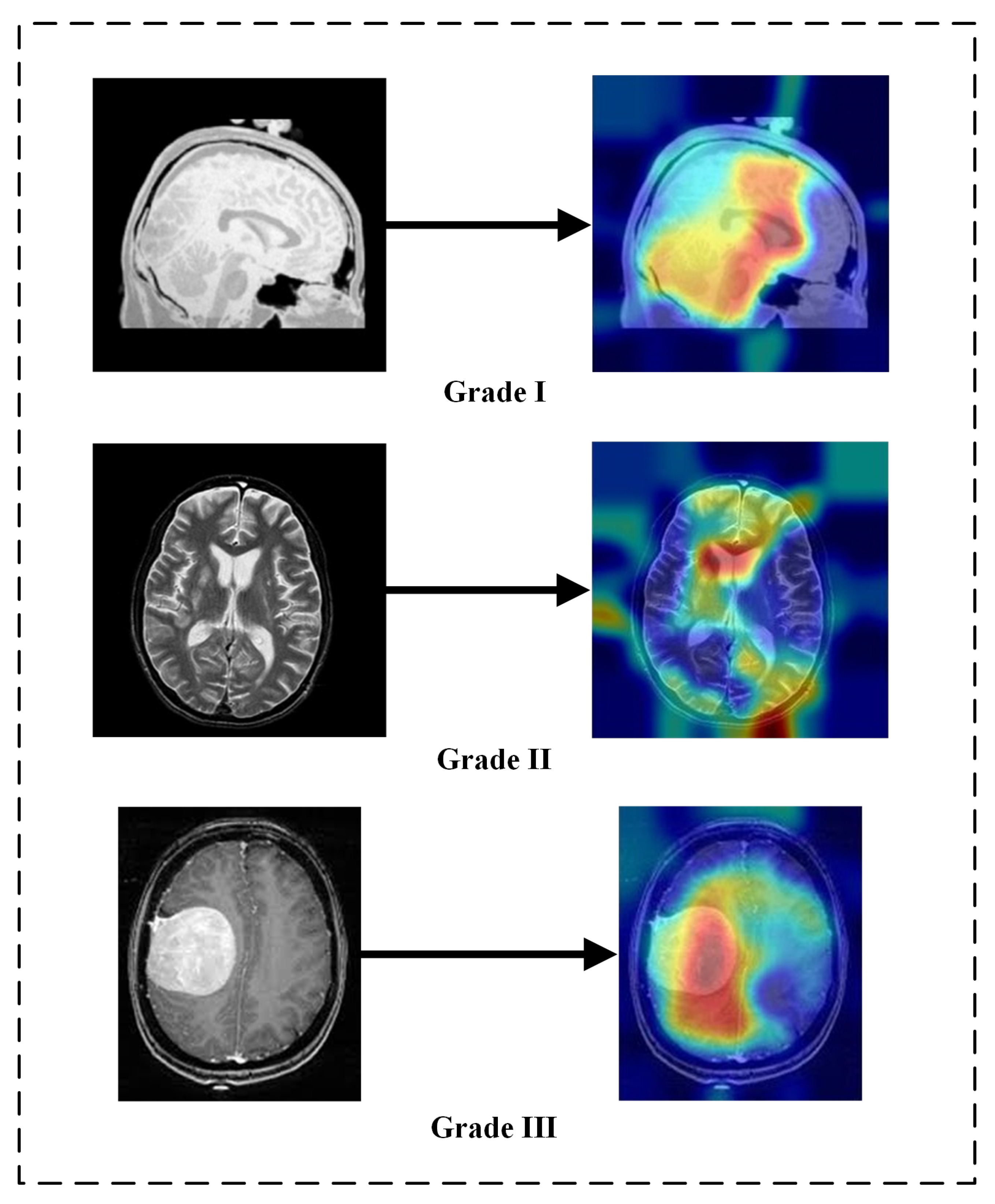
5.3. Explainability of the Results
5.4. Ablation Study
5.5. Limitations and Future Work
- Because the suggested model employs a custom CNN, automatic feature extraction has been realized;
- Computational time is reduced because of the use of MobileNetV2;
- Because the Adam Optimizer is being used, the proposed method achieves quicker convergence;
- The entropy-based controlled feature selection scheme is employed to select the best features. Based on the entropy value, the entropy removes unnecessary and redundant attributes and selects only the highest priority features.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bauer, S.; May, C.; Dionysiou, D.; Stamatakos, G.; Buchler, P.; Reyes, M. Multiscale modeling for image analysis of brain tumor studies. IEEE Trans. Biomed. Eng. 2011, 59, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Havaei, M.; Davy, A.; Warde-Farley, D.; Biard, A.; Courville, A.; Bengio, Y.; Larochelle, H. Brain tumor segmentation with deep neural networks. Med. Image Anal. 2017, 35, 18–31. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Arshad, H.; Nisar, W.; Javed, M.Y.; Sharif, M. An integrated design of fuzzy C-means and NCA-based multi-properties feature reduction for brain tumor recognition. In Signal and Image Processing Techniques for the Development of Intelligent Healthcare Systems; Springer: Berlin/Heidelberg, Germany, 2021; pp. 1–28. [Google Scholar]
- Maqsood, S.; Damasevicius, R.; Shah, F.M. An efficient approach for the detection of brain tumor using fuzzy logic and U-NET CNN classification. In International Conference on Computational Science and Its Applications; Springer: Cham, Switzerland, 2021; pp. 105–118. [Google Scholar]
- Amin, J.; Sharif, M.; Yasmin, M.; Fernandes, S.L. Big data analysis for brain tumor detection: Deep convolutional neural networks. Future Gener. Comput. Syst. 2018, 87, 290–297. [Google Scholar] [CrossRef]
- Ostrom, T.Q.; Gittleman, H.; Liao, P.; Vecchione-Koval, T.; Wolinsky, Y.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2010–2014. In Neuro-oncology; Oxford University Press: Oxford, UK, 2017; Volume 19, pp. v1–v88. [Google Scholar] [CrossRef]
- Nawaz, S.A.; Khan, D.M.; Qadri, S. Brain Tumor Classification Based on Hybrid Optimized Multi-features Analysis Using Magnetic Resonance Imaging Dataset. Appl. Artif. Intell. 2022, 36, 1–27. [Google Scholar] [CrossRef]
- Ke, Q.; Zhang, J.; Wei, W.; Damaševičius, R.; Woźniak, M. Adaptive independent subspace analysis of brain magnetic resonance imaging data. IEEE Access 2019, 7, 12252–12261. [Google Scholar] [CrossRef]
- Jansson, D.; Dieriks, V.B.; Rustenhoven, J.; Smyth, L.C.; Scotter, E.; Aalderink, M.; Dragunow, M. Cardiac glycosides target barrier inflammation of the vasculature, meninges and choroid plexus. Commun. Biol. 2021, 4, 1–17. [Google Scholar] [CrossRef]
- Pereira, S.; Pinto, A.; Alves, V.; Silva, C.A. Brain tumor segmentation using convolutional neural networks in MRI images. IEEE Trans. Med. Imaging 2016, 35, 1240–1251. [Google Scholar] [CrossRef]
- Wadhwa, A.; Bhardwaj, A.; Singh Verma, V. A review on brain tumor segmentation of MRI images. Magn. Reson. Imaging 2019, 61, 247–259. [Google Scholar] [CrossRef]
- Ohgaki, H.; Kleihues, P. Population-based studies on incidence, survival rates, and genetic alterations in astrocytic and oligodendroglial gliomas. J. Neuropathol. Exp. Neurol. 2005, 64, 479–489. [Google Scholar] [CrossRef]
- Dong, H.; Yang, G.; Liu, F.; Mo, Y.; Guo, Y. Automatic brain tumor detection and segmentation using U-Net based fully convolutional networks. In Annual Conference on Medical Image Understanding and Analysis; Springer: Cham, Switzerland, 2017; pp. 506–517. [Google Scholar]
- Abd-Ellah, M.K.; Awad, A.I.; Khalaf, A.A.M.; Hamed, H.F.A. A review on brain tumor diagnosis from MRI images: Practical implications, key achievements, and lessons learned. Magn. Reson. Imaging 2019, 61, 300–318. [Google Scholar] [CrossRef]
- Sharma, A.K.; Nandal, A.; Dhaka, A.; Dixit, R. A survey on machine learning based brain retrieval algorithms in medical image analysis. Health Technol. 2020, 10, 1359–1373. [Google Scholar] [CrossRef]
- Ali, S.; Li, J.; Pei, Y.; Khurram, R.; Rehman, K.; Mahmood, T. A comprehensive survey on brain tumor diagnosis using deep learning and emerging hybrid techniques with multi-modal MR image. Arch. Comput. Methods Eng. 2022, 1–26. [Google Scholar] [CrossRef]
- Arabahmadi, M.; Farahbakhsh, R.; Rezazadeh, J. Deep learning for smart Healthcare—A survey on brain tumor detection from medical imaging. Sensors 2022, 22, 1960. [Google Scholar] [CrossRef] [PubMed]
- Magadza, T.; Viriri, S. Deep learning for brain tumor segmentation: A survey of state-of-the-art. J. Imaging 2021, 7, 19. [Google Scholar] [CrossRef] [PubMed]
- Valverde, J.M.; Imani, V.; Abdollahzadeh, A.; De Feo, R.; Prakash, M.; Ciszek, R.; Tohka, J. Transfer learning in magnetic resonance brain imaging: A systematic review. J. Imaging 2021, 7, 66. [Google Scholar] [CrossRef] [PubMed]
- Muzammil, S.R.; Maqsood, S.; Haider, S.; Damaševičius, R. CSID: A novel multimodal image fusion algorithm for enhanced clinical diagnosis. Diagnostics 2020, 10, 904. [Google Scholar] [CrossRef]
- Maqsood, S.; Damaševičius, R.; Maskeliūnas, R. TTCNN: A Breast Cancer Detection and Classification towards Computer-Aided Diagnosis Using Digital Mammography in Early Stages. Appl. Sci. 2022, 12, 3273. [Google Scholar] [CrossRef]
- Maqsood, S.; Damaševičius, R.; Maskeliūnas, R. Hemorrhage detection based on 3D CNN deep learning framework and feature fusion for evaluating retinal abnormality in diabetic patients. Sensors 2021, 21, 3865. [Google Scholar] [CrossRef]
- Maqsood, S.; Damasevicius, R.; Siłka, J.; Woźniak, M. Multimodal Image Fusion Method Based on Multiscale Image Matting. In International Conference on Artificial Intelligence and Soft Computing; Springer: Cham, Switzerland, 2021; pp. 57–68. [Google Scholar]
- Sobhaninia, Z.; Rezaei, S.; Noroozi, A.; Ahmadi, M.; Zarrabi, H.; Karimi, N.; Samavi, S. Brain tumor segmentation using deep learning by type specific sorting of images. arXiv 2018, arXiv:1809.07786. [Google Scholar]
- Johnpeter, J.H.; Ponnuchamy, T. Computer aided automated detection and classification of brain tumors using CANFIS classification method. Int. J. Imaging Syst. Technol. 2019, 29, 431–438. [Google Scholar] [CrossRef]
- Toğaçar, M.; Ergen, B.; Cömert, Z. BrainMRNet: Brain tumor detection using magnetic resonance images with a novel convolutional neural network model. Med. Hypotheses 2020, 134, 109531. [Google Scholar] [CrossRef] [PubMed]
- Kibriya, H.; Amin, R.; Alshehri, A.H.; Masood, M.; Alshamrani, S.S.; Alshehri, A. A Novel and Effective Brain Tumor Classification Model Using Deep Feature Fusion and Famous Machine Learning Classifiers. Comput. Intell. Neurosci. 2022, 7897669. [Google Scholar] [CrossRef] [PubMed]
- Sajjad, M.; Khan, S.; Muhammad, K.; Wu, W.; Ullah, A.; Baik, S.W. Multi-grade brain tumor classification using deep CNN with extensive data augmentation. J. Comput. Sci. 2019, 30, 174–182. [Google Scholar] [CrossRef]
- Shanthakumar, P.; Ganesh Kumar, P. Computer aided brain tumor detection system using watershed segmentation techniques. Int. J. Imaging Syst. Technol. 2015, 25, 297–301. [Google Scholar] [CrossRef]
- Prastawa, M.; Bullitt, E.; Ho, S.; Gerig, G. A brain tumor segmentation framework based on outlier detection. Med. Image Anal. 2004, 8, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Gumaei, A.; Hassan, M.M.; Hassan, M.R.; Alelaiwi, A.; Fortino, G. A hybrid feature extraction method with regularized extreme learning machine for brain tumor classification. IEEE Access 2019, 7, 36266–36273. [Google Scholar] [CrossRef]
- Swati, Z.N.K.; Zhao, Q.; Kabir, M.; Ali, F.; Ali, Z.; Ahmed, S.; Lu, J. Brain tumor classification for mr images using transfer learning and fine-tuning. Comput. Med. Imaging Graph. 2019, 75, 34–46. [Google Scholar] [CrossRef]
- Kumar, R.L.; Kakarla, J.; Isunuri, B.V.; Singh, M. Multi-class brain tumor classification using residual network and global average pooling. Multimed. Tools Appl. 2021, 80, 13429–13438. [Google Scholar] [CrossRef]
- Kadry, S.; Taniar, D.; Damasevicius, R.; Rajinikanth, V. Automated detection of schizophrenia from brain MRI slices using optimized deep-features. In Proceedings of the 2021 IEEE 7th International Conference on Bio Signals, Images and Instrumentation, ICBSII 2021, Chennai, India, 25–27 March 2021. [Google Scholar] [CrossRef]
- Odusami, M.; Maskeliūnas, R.; Damaševičius, R. An intelligent system for early recognition of Alzheimer’s disease using neuroimaging. Sensors 2022, 22, 740. [Google Scholar] [CrossRef]
- Maqsood, S.; Javed, U.; Riaz, M.M.; Muzammil, M.; Muhammad, F.; Kim, S. Multiscale image matting based multi-focus image fusion technique. Electronics 2020, 9, 472. [Google Scholar] [CrossRef]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L.C. Mobilenetv2: Inverted residuals and linear bottlenecks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 4510–4520. [Google Scholar]
- Jang, B.-S.; Park, A.J.; Jeon, S.H.; Kim, I.H.; Lim, D.H.; Park, S.-H.; Lee, J.H.; Chang, J.H.; Cho, K.H.; Kim, J.H.; et al. Machine Learning Model to Predict Pseudoprogression Versus Progression in Glioblastoma Using MRI: A Multi-Institutional Study (KROG 18-07). Cancers 2020, 12, 2706. [Google Scholar] [CrossRef] [PubMed]
- Vankdothu, R.; Hameed, M.A.; Fatima, H. A Brain Tumor Identification and Classification Using Deep Learning based on CNN-LSTM Method. Comput. Electr. Eng. 2022, 101, 107960. [Google Scholar] [CrossRef]
- Fasihi, M.S.; Mikhael, W.B. Brain tumor grade classification Using LSTM Neural Networks with Domain Pre-Transforms. In Proceedings of the 2021 IEEE International Midwest Symposium on Circuits and Systems (MWSCAS), Lansing, MI, USA, 9–11 August 2021. [Google Scholar]
- Kale, G.A.; Yüzgeç, U. Advanced strategies on update mechanism of Sine Cosine Optimization Algorithm for feature selection in classification problems. Eng. Appl. Artif. Intell. 2022, 107, 104506. [Google Scholar] [CrossRef]
- Nanfang Hospital and General Hospital, Tianjin Medical University: Tianjin, China. Available online: https://figshare.com/articles/dataset/brain_tumor_dataset/1512427/5 (accessed on 9 June 2022).
- Menze, B.H.; Jakab, A.; Bauer, S.; Kalpathy-Cramer, J.; Farahani, K.; Kirby, J.; Van Leemput, K. The multimodal brain tumor image segmentation benchmark (BRATS). IEEE Trans. Med. Imaging 2014, 34, 1993–2024. [Google Scholar] [CrossRef] [PubMed]
- Sharif, M.I.; Li, J.P.; Khan, M.A.; Saleem, M.A. Active deep neural network features selection for segmentation and recognition of brain tumors using MRI images. Pattern Recognit. Lett. 2020, 129, 181–189. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Raza, M.; Saba, T.; Sial, R.; Shad, S.A. Brain tumor detection: A long short-term memory (LSTM)-based learning model. Neural Comput. Appl. 2020, 32, 15965–15973. [Google Scholar] [CrossRef]
- Narmatha, C.; Eljack, S.M.; Tuka, A.A.R.M.; Manimurugan, S.; Mustafa, M. A hybrid fuzzy brain-storm optimization algorithm for the classification of brain tumor MRI images. J. Ambient. Intell. Humaniz. Comput. 2020, 1–9. [Google Scholar] [CrossRef]
- Khan, M.A.; Ashraf, I.; Alhaisoni, M.; Damaševičius, R.; Scherer, R.; Rehman, A.; Bukhari, S.A.C. Multimodal brain tumor classification using deep learning and robust feature selection: A machine learning application for radiologists. Diagnostics 2020, 10, 565. [Google Scholar] [CrossRef]
- Cheng, J.; Huang, W.; Cao, S.; Yang, R.; Yang, W.; Yun, Z.; Feng, Q. Enhanced performance of brain tumor classification via tumor region augmentation and partition. PLoS ONE 2015, 10, e0140381. [Google Scholar] [CrossRef]
- Badža, M.M.; Barjaktarović, M.Č. Classification of brain tumors from MRI images using a convolutional neural network. Appl. Sci. 2020, 10, 1999. [Google Scholar] [CrossRef]
- Tripathi, P.C.; Bag, S. Non-invasively grading of brain tumor through noise robust textural and intensity based features. In Computational Intelligence in Pattern Recognition; Springer: Singapore, 2020; pp. 531–539. [Google Scholar]
- Ahuja, S.; Panigrahi, B.K.; Gandhi, T.K. Enhanced performance of Dark-Nets for brain tumor classification and segmentation using colormap-based superpixel techniques. Mach. Learn. Appl. 2022, 7, 100212. [Google Scholar] [CrossRef]
- Noreen, N.; Palaniappan, S.; Qayyum, A.; Ahmad, I.O.; Alassafi, M. Brain Tumor Classification Based on Fine-Tuned Models and the Ensemble Method. Comput. Mater. Contin. 2021, 67, 3967–3982. [Google Scholar] [CrossRef]
- Bodapati, J.D.; Shaik, N.S.; Naralasetti, V.; Mundukur, N.B. Joint training of two-channel deep neural network for brain tumor classification. Signal Image Video Process. 2020, 15, 753–760. [Google Scholar] [CrossRef]
- Anaraki, A.K.; Ayati, M.; Kazemi, F. Magnetic resonance imaging-based brain tumor grades classification and grading via convolutional neural networks and genetic algorithms. Biocybern. Biomed. Eng. 2019, 39, 63–74. [Google Scholar] [CrossRef]
- Deepak, S.; Ameer, P.M. Brain tumor classification using deep cnn features via transfer learning. Comput. Biol. Med. 2019, 111, 103345. [Google Scholar] [CrossRef]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-CAM: Visual Explanations from Deep Networks via Gradient-Based Localization. Int. J. Comput. Vis. 2019, 128, 336–359. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| References | Method and Methods Used | Modality | Results |
|---|---|---|---|
| Maqsood et al. [4] | Fuzzy logic and U-NET CNN classification | MRI | Accuracy = 98.59% |
| Sobhaninia et al. [24] | Linknet networks | MRI | Dice Score = 0.79 |
| Johnpeter et al. [25] | Fusion based CANFIS classifier | MRI | Accuracy = 98.80% |
| Togacar et al. [26] | BrainMRNet | MRI | Accuracy = 96.05% |
| Kibriya et al. [27] | CNN, SVM, and KNN | MRI | Accuracy = 97.70% |
| Sajjad et al. [28] | Cascade CNN and VGG19 | MRI | Accuracy = 94.58% |
| Shanthakumar [29] | Gray Level Co-occurrence and SVM | MRI | Accuracy = 94.52% |
| Prastawa et al. [30] | Geometric and Spatial Constraints | MRI | Accuracy = 88.17% |
| Gumaei et al. [31] | PCA-NGIST and RELM | MRI | Accuracy = 94.23% |
| Swati et al. [32] | Fine-tuned VGG19 | MRI | Accuracy = 94.82% |
| Kumar et al. [33] | ResNet50 and Global Average Pooling | MRI | Accuracy = 97.48% |
| Layers | Name | Type | Activations | Learnables |
|---|---|---|---|---|
| 1 | InputImage 256 × 256 × 3 images with “zero center” normalization | Input Image | 256 × 256 × 3 | - |
| 2 | Conv_1 32 3 × 3 × 3 convolution with stride [1 1] and padding ’same’ | Convolution | 256 × 256 × 32 | Weights 3 × 3 × 3 × 32 Bias 1 × 1 × 32 |
| 3 | ReLu_1 relu | ReLu | 256 × 256 × 32 | - |
| 4 | Conv_2 64 3 × 3 × 32 convolution with stride [1 1] and padding ’same’ | Convolution | 128 × 128 × 64 | Weights 3 × 3 × 32 × 64 ias 1 × 1 × 64 |
| 5 | ReLu_2 relu | ReLu | 128 × 128 × 64 | - |
| 6 | Conv_3 128 3 × 3 × 64 convolution with stride [1 1] and padding ’same’ | Convolution | 128 × 128 × 128 | Weights 3 × 3 × 64 × 128 Bias 1 × 1 × 128 |
| 7 | ReLu_3 relu | ReLu | 128 × 128 × 128 | - |
| 8 | Maxpool_1 5 × 5 max pooling with stride [1 1] and padding ’same’ | Max Pooling | 64 × 64 × 128 | - |
| 9 | Conv_4 128 3 × 3 × 128 convolution with stride [1 1] and padding ’same’ | Convolution | 64 × 64 × 256 | Weights 3 × 3 × 128 × 256 Bias 1 × 1 × 256 |
| 10 | ReLu_4 relu | ReLu | 64 × 64 × 256 | - |
| 11 | Maxpool_2 5 × 5 max pooling with stride [1 1] and padding ’same’ | Max Pooling | 32 × 32 × 256 | - |
| 12 | Conv_5 512 3 × 3 × 256 convolution with stride [1 1] and padding ’same’ | Convolution | 32 × 32 × 512 | Weights 3 × 3 × 256 × 512 Bias 1 × 1 × 512 |
| 13 | ReLu_5 relu | ReLu | 32 × 32 × 512 | - |
| 14 | Transposed conv 256 3 × 3 × 512 transposed convolution stride [1 1] and cropping ’same’ | Transposed Convolution | 32 × 32 × 512 | Weights 3 × 3 × 256 × 512 Bias 1 × 1 × 512 |
| 15 | Conv_6 1024 3 × 3 × 512 convolution with stride [1 1] and padding ’same’ | Convolution | 16 × 16 × 1024 | Weights 3 × 3 × 256 × 1024 Bias 1 × 1 × 1024 |
| 16 | Softmax | Softmax | 1 × 1 × 256 | - |
| 17 | Pixel class Cross entropy loss | Pixel Classification | - | - |
| Proposed Method | |
|---|---|
| Evaluation Metrics | Performance |
| Accuracy () | 97.47% |
| Sensitivity () | 97.22% |
| Specificity () | 97.94% |
| Dice coefficient index () | 96.71% |
| Authors | Methods | Accuracy of Classification |
|---|---|---|
| Irfan et al. [44] | CNN, LBP, & PSO | 92.50% |
| Amin et al. [45] | LSTM | 93.85% |
| Narmatha et al. [46] | Brain-storm optimization | 92.50% |
| Khan et al. [47] | DCT, CNN, & ELM | 93.40% |
| Proposed Method | 17-layered CNN, MobileNetV2 & M-SVM | 97.47% |
| Proposed Method | |
|---|---|
| Evaluation Metrics | Performance |
| Accuracy () | 98.92% |
| Sensitivity () | 98.82% |
| Specificity () | 99.02% |
| Dice coefficient index () | 97.87% |
| Authors | Methods | Accuracy of Classification |
|---|---|---|
| Maqsood et al. [4] | U-NET CNN | 98.59% |
| Sajjad et al. [28] | VGG19 & image augmentation | 94.58% |
| Gumaei et al. [31] | Regularized Extreme Learning MAchine | 94.23% |
| Swati et al. [32] | Fine-tuned VGG19 | 94.82% |
| Kumar et al. [33] | ResNet50 & Global Average Pooling | 97.48% |
| Cheng et al. [48] | Linear discriminant analysis (LDA) | 93.60% |
| Badza et al. [49] | CNN | 96.50% |
| Tripathi et al. [50] | SVM | 94.63% |
| Ahuja et al. [51] | DarkNet-53 | 98.15% |
| Noreen et al. [52] | InceptionV3 & ensemble of KNN, SVM & RF | 94.34% |
| Bodapati et al. [53] | Two channel DNN | 97.23% |
| Anaraki et al. [54] | CNN & Genetic Algorithm | 94.20% |
| Deepak et al. [55] | GoogleNet | 97.10% |
| Proposed Method | 17-layered CNN, MobileNetV2 & M-SVM | 98.92% |
| Network | Images Size | Number of Parameters (in Millions) | Depth | Updated Layers | Training Accuracy |
|---|---|---|---|---|---|
| ResNet18 | 224 × 224 × 3 | 12 | 18 | 71 | 90.3% |
| DenseNet201 | 224 × 224 × 3 | 20 | 201 | 708 | 91.5% |
| SqueezeNet | 227 × 227 × 3 | 2 | 18 | 68 | 92.7% |
| Inceptionv3 | 299 × 299 × 3 | 24 | 48 | 315 | 95.3% |
| DarkNet19 | 256 × 256 × 3 | 21 | 19 | 64 | 97.7% |
| MobileNetV2 | 224 × 224 × 3 | 4 | 53 | 154 | 98.8% |
| Optimizer | Accuracy | Sensitivity | Specificity |
|---|---|---|---|
| Sgdm | 98.16% | 97.71% | 98.25% |
| RMSprop | 98.78% | 97.89% | 98.86% |
| Adam | 99.31% | 98.76% | 99.42% |
| Method | Cross-Validation | Accuracy |
|---|---|---|
| GoogleNet (Deepak et al. [55]) | 5-fold | 97.10% |
| DarkNet-53 (Ahuja et al. [51]) | 5-fold | 98.15% |
| U-Net CNN (Maqsood et al. [4]) | 5-fold | 98.59% |
| Proposed | 5-fold | 98.92% |
| Method | Sensitivity | Accuracy | Time (s) |
|---|---|---|---|
| Fine tree | 89.00% | 89.20% | 28.60 |
| E-Bst tree | 96.25% | 96.40% | 577.68 |
| Fine KNN | 97.50% | 97.70% | 37.78 |
| M-SVM | 98.82% | 98.92% | 15.64 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maqsood, S.; Damaševičius, R.; Maskeliūnas, R. Multi-Modal Brain Tumor Detection Using Deep Neural Network and Multiclass SVM. Medicina 2022, 58, 1090. https://doi.org/10.3390/medicina58081090
Maqsood S, Damaševičius R, Maskeliūnas R. Multi-Modal Brain Tumor Detection Using Deep Neural Network and Multiclass SVM. Medicina. 2022; 58(8):1090. https://doi.org/10.3390/medicina58081090
Chicago/Turabian StyleMaqsood, Sarmad, Robertas Damaševičius, and Rytis Maskeliūnas. 2022. "Multi-Modal Brain Tumor Detection Using Deep Neural Network and Multiclass SVM" Medicina 58, no. 8: 1090. https://doi.org/10.3390/medicina58081090