
Knowledge of Human Monkeypox and Its Relation to Conspiracy Beliefs among Students in Jordanian Health Schools: Filling the Knowledge Gap on Emerging Zoonotic Viruses

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Ethical Permission
2.3. Overview of the Questionnaire and Study Variables
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Sample
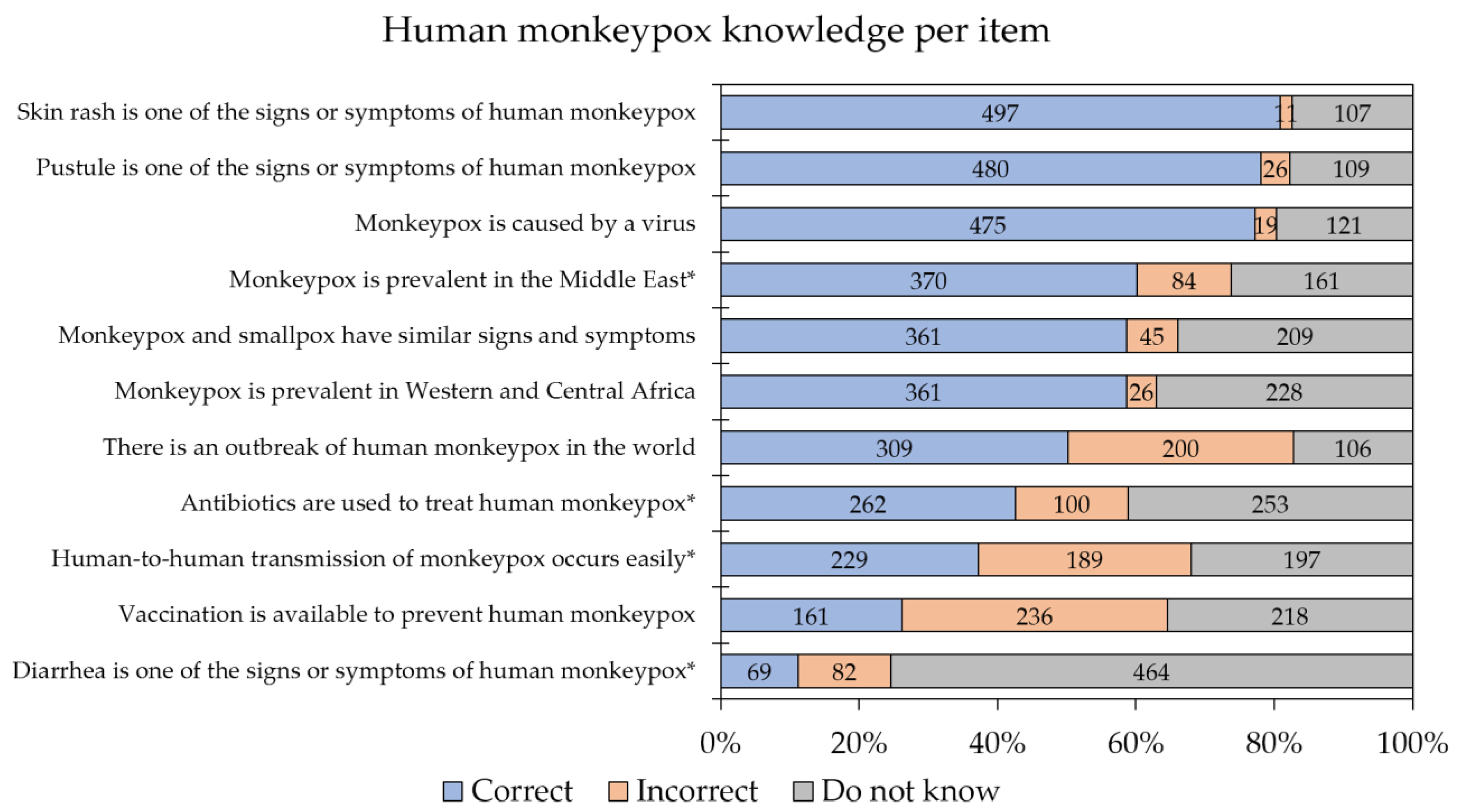
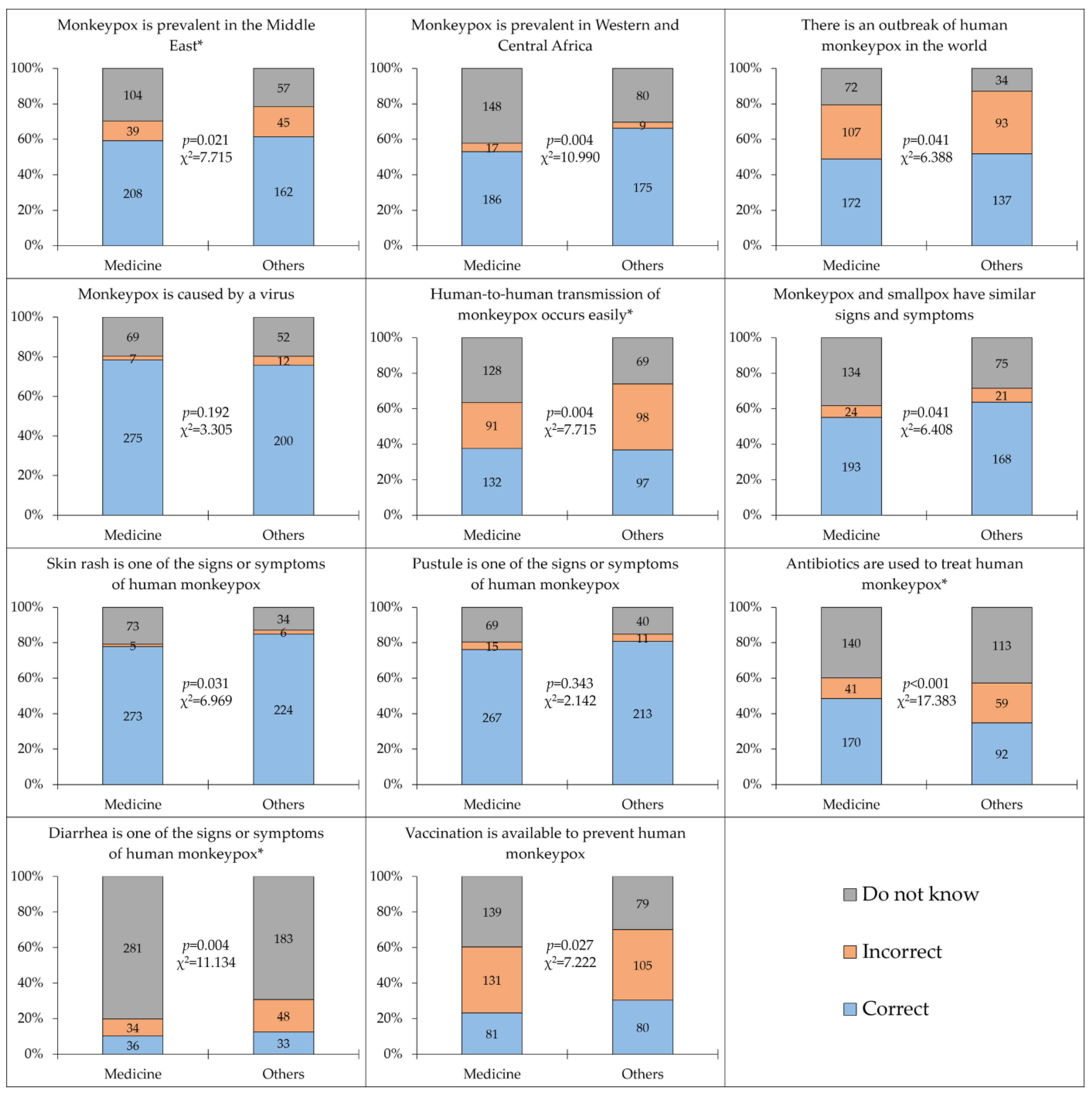
3.2. Human Monkeypox Knowledge and Associated Determinants
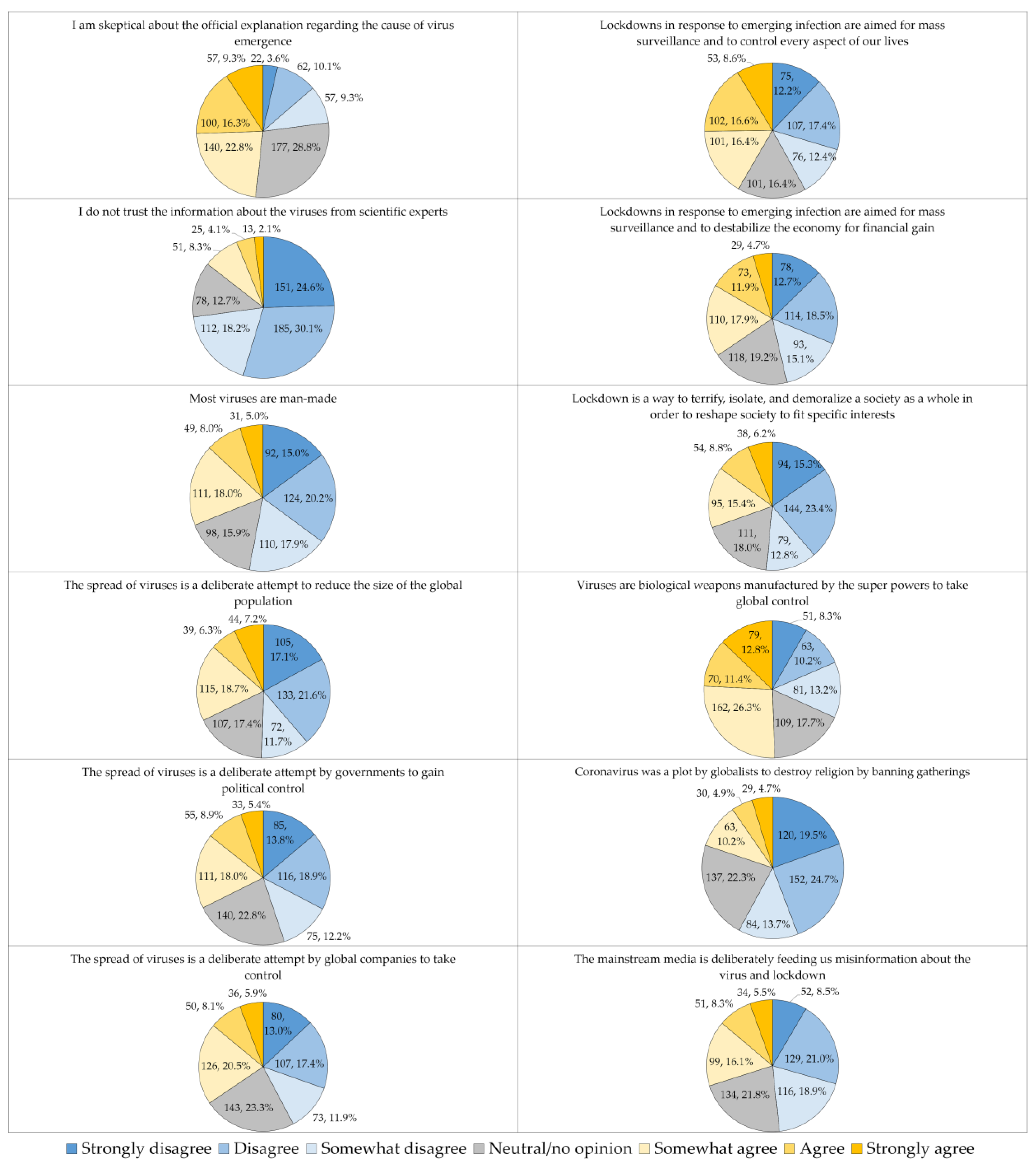
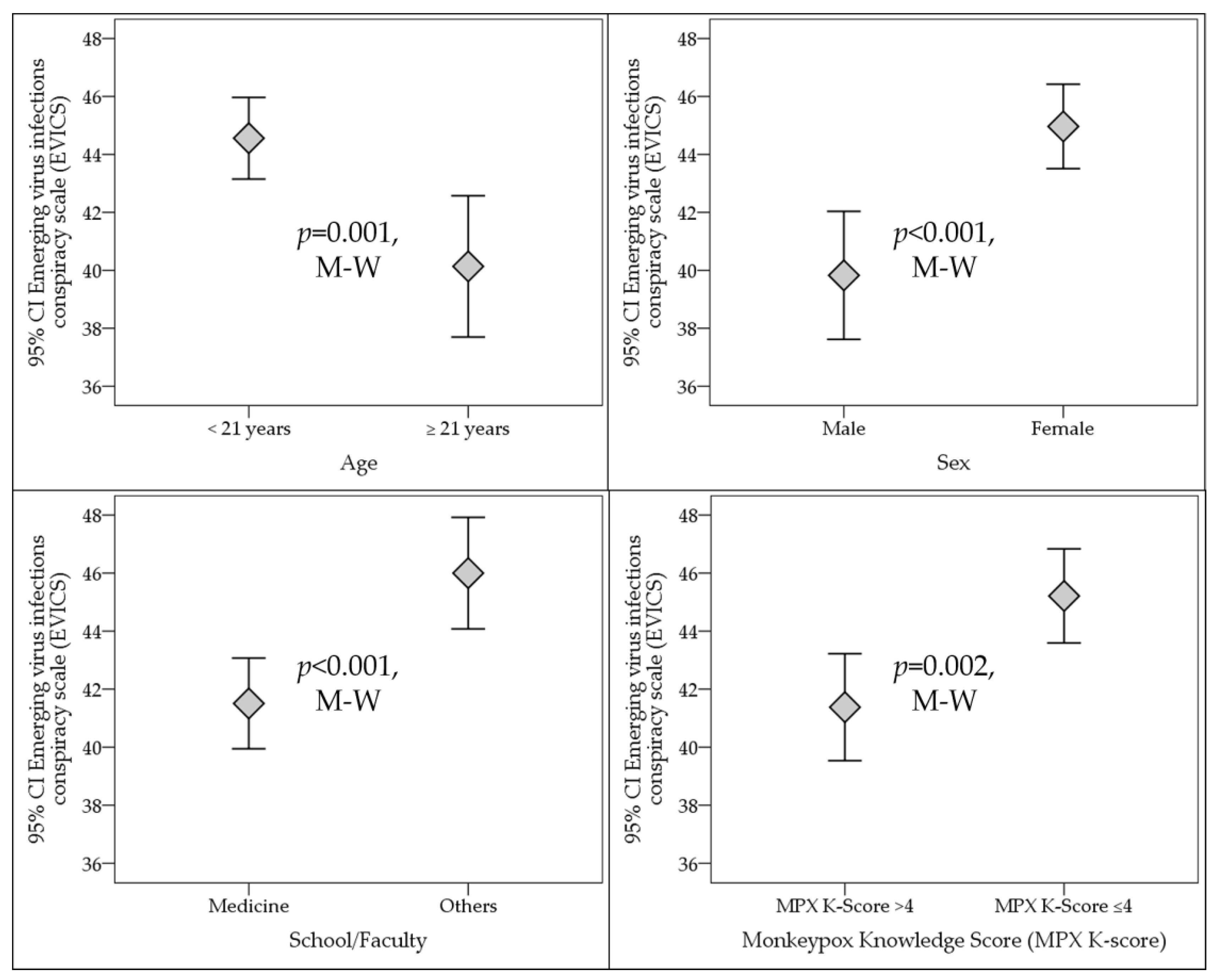
3.3. Conspiracy Beliefs regarding Emergence of Virus Infections and Its Associated Determinants
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CFR | Case-fatality ratio |
| COVID-19 | Coronavirus disease 2019 |
| EVICS | Emerging virus infections conspiracy scale |
| HMPX | Human monkeypox |
| K-S | Kolmogorov–Smirnov test |
| MPX K-score | Monkeypox knowledge score |
| MPXV | Monkeypox virus |
| MSM | Men having sex with men |
| M-W | Mann–Whitney U test |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| SD | Standard deviation |
| SPSS | Statistical Package for the Social Sciences |
| U.S. | United States |
| WHO | World Health Organization |
References
- Ladnyj, I.D.; Ziegler, P.; Kima, E. A human infection caused by monkeypox virus in Basankusu Territory, Democratic Republic of the Congo. Bull. World Health Organ. 1972, 46, 593–597. [Google Scholar] [PubMed]
- Sklenovská, N.; Van Ranst, M. Emergence of Monkeypox as the Most Important Orthopoxvirus Infection in Humans. Front. Public Health 2018, 6, 241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shchelkunov, S.N.; Marennikova, S.S.; Moyer, R.W. Orthopoxviruses Pathogenic for Humans, 1st ed.; Springer: New York, NY, USA, 2005; p. 425. [Google Scholar] [CrossRef]
- Silva, N.I.O.; de Oliveira, J.S.; Kroon, E.G.; Trindade, G.d.S.; Drumond, B.P. Here, There, and Everywhere: The Wide Host Range and Geographic Distribution of Zoonotic Orthopoxviruses. Viruses 2020, 13, 43. [Google Scholar] [CrossRef] [PubMed]
- Petersen, E.; Abubakar, I.; Ihekweazu, C.; Heymann, D.; Ntoumi, F.; Blumberg, L.; Asogun, D.; Mukonka, V.; Lule, S.A.; Bates, M.; et al. Monkeypox—Enhancing public health preparedness for an emerging lethal human zoonotic epidemic threat in the wake of the smallpox post-eradication era. Int. J. Infect. Dis. 2019, 78, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, A.; Aarons, E.; Astbury, J.; Balasegaram, S.; Beadsworth, M.; Beck, C.R.; Chand, M.; O’Connor, C.; Dunning, J.; Ghebrehewet, S.; et al. Two cases of monkeypox imported to the United Kingdom, September 2018. Eurosurveillance 2018, 23, 1800509. [Google Scholar] [CrossRef] [PubMed]
- Melski, J.; Reed, K.; Stratman, E.; Graham, M.B.; Fairley, J.; Edmiston, C.; Kehl, K.S.; Foldy, S.L.; Swain, G.R.; Biedrzycki, P.; et al. Multistate outbreak of monkeypox-Illinois, Indiana, and Wisconsin, 2003. MMWR. Morb. Mortal. Wkly. Rep. 2003, 52, 537–540. [Google Scholar] [PubMed]
- European Centre for Disease Prevention and Control (ECDC). Epidemiological Update: Monkeypox Multi-Country Outbreak. Available online: https://www.ecdc.europa.eu/en/news-events/epidemiological-update-monkeypox-multi-country-outbreak-0 (accessed on 1 June 2022).
- WHO | World Health Organization. Multi-Country Monkeypox Outbreak in Non-Endemic Countries: Update. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON388 (accessed on 1 June 2022).
- Macneil, A.; Reynolds, M.G.; Braden, Z.; Carroll, D.S.; Bostik, V.; Karem, K.; Smith, S.K.; Davidson, W.; Li, Y.; Moundeli, A.; et al. Transmission of atypical varicella-zoster virus infections involving palm and sole manifestations in an area with monkeypox endemicity. Clin. Infect. Dis. 2009, 48, e6–e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Formenty, P.; Muntasir, M.O.; Damon, I.; Chowdhary, V.; Opoka, M.L.; Monimart, C.; Mutasim, E.M.; Manuguerra, J.C.; Davidson, W.B.; Karem, K.L.; et al. Human monkeypox outbreak caused by novel virus belonging to Congo Basin clade, Sudan, 2005. Emerg. Infect. Dis. 2010, 16, 1539–1545. [Google Scholar] [CrossRef]
- Vaughan, A.; Aarons, E.; Astbury, J.; Brooks, T.; Chand, M.; Flegg, P.; Hardman, A.; Harper, N.; Jarvis, R.; Mawdsley, S.; et al. Human-to-Human Transmission of Monkeypox Virus, United Kingdom, October 2018. Emerg. Infect. Dis. 2020, 26, 782–785. [Google Scholar] [CrossRef]
- Nolen, L.D.; Osadebe, L.; Katomba, J.; Likofata, J.; Mukadi, D.; Monroe, B.; Doty, J.; Hughes, C.M.; Kabamba, J.; Malekani, J.; et al. Extended Human-to-Human Transmission during a Monkeypox Outbreak in the Democratic Republic of the Congo. Emerg. Infect. Dis. 2016, 22, 1014–1021. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control (ECDC). Risk Assessment: Monkeypox Multi-Country Outbreak. Available online: https://www.ecdc.europa.eu/en/publications-data/risk-assessment-monkeypox-multi-country-outbreak (accessed on 1 June 2022).
- WHO | World Health Organization. Monkeypox: Public Health Advice for Gay, Bisexual and Other Men Who Have Sex with Men. Available online: https://www.who.int/publications/m/item/monkeypox-public-health-advice-for-men-who-have-sex-with-men (accessed on 1 June 2022).
- Kozlov, M. Monkeypox Outbreaks: 4 Key Questions Researchers Have. Available online: https://doi.org/10.1038/d41586-022-01493-6 (accessed on 1 June 2022).
- Huhn, G.D.; Bauer, A.M.; Yorita, K.; Graham, M.B.; Sejvar, J.; Likos, A.; Damon, I.K.; Reynolds, M.G.; Kuehnert, M.J. Clinical Characteristics of Human Monkeypox, and Risk Factors for Severe Disease. Clin. Infect. Dis. 2005, 41, 1742–1751. [Google Scholar] [CrossRef] [PubMed]
- McCollum, A.M.; Damon, I.K. Human Monkeypox. Clin. Infect. Dis. 2014, 58, 260–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention (CDC). Monkeypox. Available online: https://www.cdc.gov/poxvirus/monkeypox/index.html (accessed on 2 June 2022).
- Ogoina, D.; Iroezindu, M.; James, H.I.; Oladokun, R.; Yinka-Ogunleye, A.; Wakama, P.; Otike-odibi, B.; Usman, L.M.; Obazee, E.; Aruna, O.; et al. Clinical Course and Outcome of Human Monkeypox in Nigeria. Clin. Infect. Dis. 2020, 71, e210–e214. [Google Scholar] [CrossRef] [PubMed]
- Adler, H.; Gould, S.; Hine, P.; Snell, L.B.; Wong, W.; Houlihan, C.F.; Osborne, J.C.; Rampling, T.; Beadsworth, M.B.J.; Duncan, C.J.A.; et al. Clinical features and management of human monkeypox: A retrospective observational study in the UK. Lancet Infect. Dis. 2022, 1–10. [Google Scholar] [CrossRef]
- Hoy, S.M. Tecovirimat: First Global Approval. Drugs 2018, 78, 1377–1382. [Google Scholar] [CrossRef]
- The U.S. Food and Drug Administration (FDA). FDA Approves Drug to Treat Smallpox. Available online: https://www.fda.gov/drugs/news-events-human-drugs/fda-approves-drug-treat-smallpox (accessed on 1 June 2022).
- Jezek, Z.; Marennikova, S.S.; Mutumbo, M.; Nakano, J.H.; Paluku, K.M.; Szczeniowski, M. Human monkeypox: A study of 2510 contacts of 214 patients. J. Infect. Dis. 1986, 154, 551–555. [Google Scholar] [CrossRef]
- Grant, R.; Nguyen, L.-B.L.; Breban, R. Modelling human-to-human transmission of monkeypox. Bull. World Health Organ. 2020, 98, 638–640. [Google Scholar] [CrossRef]
- Reynolds, M.G.; Damon, I.K. Outbreaks of human monkeypox after cessation of smallpox vaccination. Trends Microbiol. 2012, 20, 80–87. [Google Scholar] [CrossRef]
- Al-Tammemi, A.B.; Albakri, R.; Alabsi, S. The Outbreak of Human Monkeypox in 2022: A Changing Epidemiology or an Impending Aftereffect of Smallpox Eradication? Front. Trop. Dis. 2022, 951380, provisionally accepted. [Google Scholar] [CrossRef]
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The changing epidemiology of human monkeypox-A potential threat? A systematic review. PLoS Negl. Trop. Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef]
- Likos, A.M.; Sammons, S.A.; Olson, V.A.; Frace, A.M.; Li, Y.; Olsen-Rasmussen, M.; Davidson, W.; Galloway, R.; Khristova, M.L.; Reynolds, M.G.; et al. A tale of two clades: Monkeypox viruses. J. Gen. Virol. 2005, 86, 2661–2672. [Google Scholar] [CrossRef] [PubMed]
- Selhorst, P.; Rezende, A.M.; de Block, T.; Coppens, S.; Smet, H.; Mariën, J.; Hauner, A.; Brosius, I.; Liesenborghs, L.; Bottieau, E.; et al. Belgian Case of Monkeypox Virus Linked to Outbreak in Portugal. Available online: https://virological.org/t/belgian-case-of-monkeypox-virus-linked-to-outbreak-in-portugal/801 (accessed on 1 June 2022).
- Isidro, J.; Borges, V.; Pinto, M.; Ferreira, R.; Sobral, D.; Nunes, A.; Santos, J.D.; Borrego, M.J.; Núncio, S.; Pelerito, A.; et al. First Draft Genome Sequence of Monkeypox Virus Associated with the Suspected Multi-Country Outbreak, May 2022 (Confirmed Case in Portugal). Available online: https://virological.org/t/first-draft-genome-sequence-of-monkeypox-virus-associated-with-the-suspected-multi-country-outbreak-may-2022-confirmed-case-in-portugal/799 (accessed on 2 June 2022).
- Happi, C.; Adetifa, I.; Mbala, P.; Njouom, R.; Nakoune, E.; Happi, A.; Ndodo, N.; Ayansola, O.; Mboowa, G.; Bedford, T.; et al. Urgent Need for a Non-Discriminatory and Non-Stigmatizing Nomenclature for Monkeypox Virus. Available online: https://virological.org/t/urgent-need-for-a-non-discriminatory-and-non-stigmatizing-nomenclature-for-monkeypox-virus/853 (accessed on 19 June 2022).
- Rambaut, A.; Holmes, E.C.; O’Toole, Á.; Hill, V.; McCrone, J.T.; Ruis, C.; du Plessis, L.; Pybus, O.G. A dynamic nomenclature proposal for SARS-CoV-2 lineages to assist genomic epidemiology. Nat. Microbiol. 2020, 5, 1403–1407. [Google Scholar] [CrossRef] [PubMed]
- WHO | World Health Organization. Monkeypox: Current Status in West and Central Africa. Report of a WHO Informal Consultation. Available online: https://apps.who.int/iris/bitstream/handle/10665/272620/WHO-WHE-IHM-2018.3-eng.pdf?sequence=1&isAllowed=y (accessed on 1 June 2022).
- Francis, A. Monkeypox Conspiracy Theories: Five False Claims about the Virus Debunked as Misinformation Spreads Online. Available online: https://inews.co.uk/news/monkeypox-conspiracy-theories-false-claims-virus-debunked-misinformation-online-1645306 (accessed on 1 June 2022).
- BBC Arabic. Monkeypox: Conspiracy Theories Spread about Its Dispersal Amid Fears of a New Lockdown. Available online: https://www.bbc.com/arabic/trending-61553890 (accessed on 1 June 2022).
- Kroesen, M.; Handy, S.; Chorus, C. Do attitudes cause behavior or vice versa? An alternative conceptualization of the attitude-behavior relationship in travel behavior modeling. Transp. Res. Part A Policy Pract. 2017, 101, 190–202. [Google Scholar] [CrossRef]
- Fabrigar, L.R.; Petty, R.E.; Smith, S.M.; Crites Jr, S.L. Understanding knowledge effects on attitude-behavior consistency: The role of relevance, complexity, and amount of knowledge. J. Pers. Soc. Psychol. 2006, 90, 556–577. [Google Scholar] [CrossRef]
- Patel, R.; Wattamwar, K.; Kanduri, J.; Nahass, M.; Yoon, J.; Oh, J.; Shukla, P.; Lacy, C.R. Health Care Student Knowledge and Willingness to Work in Infectious Disease Outbreaks. Disaster Med. Public Health Prep. 2017, 11, 694–700. [Google Scholar] [CrossRef]
- Jain, M.; Sharma, A.; Khanna, T.; Arora, K.; Khari, P.M.; Jain, V. Primordial prevention: Promoting preparedness for ebola virus disease. J. Clin. Diagn. Res. 2015, 9, OC21–OC24. [Google Scholar] [CrossRef]
- Milošević Đorđević, J.; Mari, S.; Vdović, M.; Milošević, A. Links between conspiracy beliefs, vaccine knowledge, and trust: Anti-vaccine behavior of Serbian adults. Soc. Sci. Med. 2021, 277, 113930. [Google Scholar] [CrossRef]
- Čavojová, V.; Šrol, J.; Ballová Mikušková, E. How scientific reasoning correlates with health-related beliefs and behaviors during the COVID-19 pandemic? J. Health Psychol. 2020, 27, 534–547. [Google Scholar] [CrossRef]
- Chesser, A.; Drassen Ham, A.; Keene Woods, N. Assessment of COVID-19 Knowledge Among University Students: Implications for Future Risk Communication Strategies. Health Educ. Behav. 2020, 47, 540–543. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Hasan, H.; Taim, D.; Al-Mahzoum, K.; Al-Haidar, A.; Yaseen, A.; Ababneh, N.A.; Assaf, A.; et al. Low COVID-19 Vaccine Acceptance Is Correlated with Conspiracy Beliefs among University Students in Jordan. Int. J. Env. Res. Public Health 2021, 18, 2407. [Google Scholar] [CrossRef]
- van Mulukom, V.; Pummerer, L.J.; Alper, S.; Bai, H.; Čavojová, V.; Farias, J.; Kay, C.S.; Lazarevic, L.B.; Lobato, E.J.C.; Marinthe, G.; et al. Antecedents and consequences of COVID-19 conspiracy beliefs: A systematic review. Soc. Sci. Med. 2022, 301, 114912. [Google Scholar] [CrossRef] [PubMed]
- van Mulukom, V. Engagement in COVID-19 Protective Behaviours: A Complex Interaction of Trust and Information in Twelve Countries. PsyArXiv 2020. web (preprint). [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Yaseen, A.; Al-Haidar, A.; Taim, D.; Eid, H.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. COVID-19 misinformation: Mere harmless delusions or much more? A knowledge and attitude cross-sectional study among the general public residing in Jordan. PLoS ONE 2020, 15, e0243264. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Dababseh, D.; Yaseen, A.; Al-Haidar, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. Conspiracy Beliefs Are Associated with Lower Knowledge and Higher Anxiety Levels Regarding COVID-19 among Students at the University of Jordan. Int. J. Env. Res. Public Health 2020, 17, 4915. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Carballo-Carbajal, I.; Science Feedback. Monkeypox Outbreak Triggers Conspiracy Theories on Social Media Claiming That It Was Planned or Incorrectly Linking It to COVID-19 Vaccines. Available online: https://healthfeedback.org/claimreview/monkeypox-outbreak-conspiracy-theories-claiming-it-was-planned-linking-with-covid-19-vaccines/ (accessed on 30 May 2022).
- Penrod, J.; Preston, D.B.; Cain, R.E.; Starks, M.T. A Discussion of Chain Referral As a Method of Sampling Hard-to-Reach Populations. J. Transcult. Nurs. 2003, 14, 100–107. [Google Scholar] [CrossRef]
- Checkmarket. Sample Size Calculator. Available online: https://www.checkmarket.com/ (accessed on 22 May 2022).
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S.; et al. Knowledge of human monkeypox viral infection among general practitioners: A cross-sectional study in Indonesia. Pathog. Glob. Health 2020, 114, 68–75. [Google Scholar] [CrossRef]
- Freeman, D.; Waite, F.; Rosebrock, L.; Petit, A.; Causier, C.; East, A.; Jenner, L.; Teale, A.-L.; Carr, L.; Mulhall, S.; et al. Coronavirus conspiracy beliefs, mistrust, and compliance with government guidelines in England. Psychol. Med. 2020, 52, 251–263. [Google Scholar] [CrossRef]
- Lee, B.Y.; Forbes. Monkeypox Outbreak Triggers New Conspiracy Theories about Bill Gates as #BillGatesBioTerrorist Trends. Available online: https://www.forbes.com/sites/brucelee/2022/05/22/monkeypox-outbreak-triggers-new-conspiracy-theories-about-bill-gates-as-billgatesbioterrorist-trends/ (accessed on 1 June 2022).
- Van Prooijen, J.-W.; Douglas, K.M. Belief in conspiracy theories: Basic principles of an emerging research domain. Eur. J. Soc. Psychol. 2018, 48, 897–908. [Google Scholar] [CrossRef]
- Schumpe, B.M.; Van Lissa, C.J.; Bélanger, J.J.; Ruggeri, K.; Mierau, J.; Nisa, C.F.; Molinario, E.; Gelfand, M.J.; Stroebe, W.; Agostini, M.; et al. Predictors of adherence to public health behaviors for fighting COVID-19 derived from longitudinal data. Sci. Rep. 2022, 12, 3824. [Google Scholar] [CrossRef]
- Ripp, T.; Röer, J.P. Systematic review on the association of COVID-19-related conspiracy belief with infection-preventive behavior and vaccination willingness. BMC Psychol. 2022, 10, 66. [Google Scholar] [CrossRef] [PubMed]
- Šrol, J.; Čavojová, V.; Ballová Mikušková, E. Finding Someone to Blame: The Link between COVID-19 Conspiracy Beliefs, Prejudice, Support for Violence, and Other Negative Social Outcomes. Front. Psychol. 2022, 12, 726076. [Google Scholar] [CrossRef] [PubMed]
- Leibovitz, T.; Shamblaw, A.L.; Rumas, R.; Best, M.W. COVID-19 conspiracy beliefs: Relations with anxiety, quality of life, and schemas. Pers. Individ. Dif. 2021, 175, 110704. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.P.; Efstratiou, A.; Komer, S.R.; Baxter, L.A.; Vasiljevic, M.; Leite, A.C. The impact of risk perceptions and belief in conspiracy theories on COVID-19 pandemic-related behaviours. PLoS ONE 2022, 17, e0263716. [Google Scholar] [CrossRef] [PubMed]
- Schraer, R. Monkeypox Wasn’t Created in a Lab—And Other Claims Debunked. Available online: https://www.bbc.com/news/health-61580089 (accessed on 1 June 2022).
- Roess, A.A.; Monroe, B.P.; Kinzoni, E.A.; Gallagher, S.; Ibata, S.R.; Badinga, N.; Molouania, T.M.; Mabola, F.S.; Mombouli, J.V.; Carroll, D.S.; et al. Assessing the Effectiveness of a Community Intervention for Monkeypox Prevention in the Congo Basin. PLoS Negl. Trop. Dis. 2011, 5, e1356. [Google Scholar] [CrossRef] [Green Version]
- Mullan, J.; Burns, P.; Weston, K.; McLennan, P.; Rich, W.; Crowther, S.; Mansfield, K.; Dixon, R.; Moselen, E.; Osborne, R.H. Health Literacy amongst Health Professional University Students: A Study Using the Health Literacy Questionnaire. Educ. Sci. 2017, 7, 54. [Google Scholar] [CrossRef]
- Al-Azzam, S.I.; Al-Husein, B.A.; Alzoubi, F.; Masadeh, M.M.; Al-Horani, M.A. Self-medication with antibiotics in Jordanian population. Int. J. Occup. Med. Environ. Health 2007, 20, 373–380. [Google Scholar] [CrossRef]
- Shehadeh, M.; Suaifan, G.; Darwish, R.M.; Wazaify, M.; Zaru, L.; Alja’fari, S. Knowledge, attitudes and behavior regarding antibiotics use and misuse among adults in the community of Jordan. A pilot study. Saudi Pharm. J. 2012, 20, 125–133. [Google Scholar] [CrossRef] [Green Version]
- Karasneh, R.A.; Al-Azzam, S.I.; Ababneh, M.A.; Basheti, I.A.; Al-Azzeh, O.; Al Sharie, S.; Conway, B.R.; Aldeyab, M.A. Exploring Information Available to and Used by Physicians on Antibiotic Use and Antibiotic Resistance in Jordan. Antibiotics 2021, 10, 963. [Google Scholar] [CrossRef]
- Alsulaiman, S.A.; Rentner, T.L. The Use of the Health Belief Model to Assess U.S. College Students’ Perceptions of Covid-19 and Adherence to Preventive Measures. J. Public Health Res. 2021, 10, 2273. [Google Scholar] [CrossRef]
- Cohen, J. Monkeypox Outbreak Questions Intensify as Cases Soar. Available online: https://www.science.org/content/article/monkeypox-outbreak-questions-intensify-cases-soar (accessed on 1 June 2022).
- Kumar, S.; Preetha, G. Health promotion: An effective tool for global health. Indian J. Community Med. 2012, 37, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.; Leggat, P.A. Human Monkeypox: Current State of Knowledge and Implications for the Future. Trop. Med. Infect. Dis. 2016, 1, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cervantes, J. The Future of Infectious Diseases Education. Med. Sci. Educ. 2020, 30, 1783–1785. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. Phylogenetic Inference in the Epidemiologic and Evolutionary Investigation of HIV-1, HCV and HBV. Ph.D. Thesis, Lund University, Faculty of Medicine, Lund, Sweden, 13 September 2017. [Google Scholar]
- Engering, A.; Hogerwerf, L.; Slingenbergh, J. Pathogen-host-environment interplay and disease emergence. Emerg. Microbes Infect. 2013, 2, 1–7. [Google Scholar] [CrossRef]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S.; et al. Confidence in managing human monkeypox cases in Asia: A cross-sectional survey among general practitioners in Indonesia. Acta Trop. 2020, 206, 105450. [Google Scholar] [CrossRef]
- Ashcroft, J.; Byrne, M.H.V.; Brennan, P.A.; Davies, R.J. Preparing medical students for a pandemic: A systematic review of student disaster training programmes. Postgrad. Med. J. 2021, 97, 368. [Google Scholar] [CrossRef]
- Alper, S.; Bayrak, F.; Yilmaz, O. Psychological correlates of COVID-19 conspiracy beliefs and preventive measures: Evidence from Turkey. Curr. Psychol. 2021, 40, 5708–5717. [Google Scholar] [CrossRef]
- Cassese, E.C.; Farhart, C.E.; Miller, J.M. Gender Differences in COVID-19 Conspiracy Theory Beliefs. Politics Gend. 2020, 16, 1009–1018. [Google Scholar] [CrossRef]
- Earnshaw, V.A.; Eaton, L.A.; Kalichman, S.C.; Brousseau, N.M.; Hill, E.C.; Fox, A.B. COVID-19 conspiracy beliefs, health behaviors, and policy support. Transl. Behav. Med. 2020, 10, 850–856. [Google Scholar] [CrossRef]
- Oliver, J.E.; Wood, T. Medical conspiracy theories and health behaviors in the United States. JAMA Intern. Med. 2014, 174, 817–818. [Google Scholar] [CrossRef] [Green Version]
- Jolley, D.; Douglas, K.M. The effects of anti-vaccine conspiracy theories on vaccination intentions. PLoS ONE 2014, 9, e89177. [Google Scholar] [CrossRef] [PubMed]
- Dobson, G.P. Wired to Doubt: Why People Fear Vaccines and Climate Change and Mistrust Science. Front. Med. 2022, 8, 809395. [Google Scholar] [CrossRef] [PubMed]
- Brainard, J.; Hunter, P.R. Misinformation making a disease outbreak worse: Outcomes compared for influenza, monkeypox, and norovirus. Simulation 2019, 96, 365–374. [Google Scholar] [CrossRef] [Green Version]
- Ajibo, H.T.; Obi-keguna, C.N.; Ugwuoke, P.J. Monkey Pox and Destabilization of Community Life in Nigeria: Implication for Social Work Practice. IOSR J. Humanit. Soc. Sci. 2018, 23, 79–84. [Google Scholar] [CrossRef]
- Muğaloğlu, E.Z.; Kaymaz, Z.; Mısır, M.E.; Laçin-Şimşek, C. Exploring the Role of Trust in Scientists to Explain Health-Related Behaviors in Response to the COVID-19 Pandemic. Sci. Educ. 2022, 1–29. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Fraihat, E.; Dababseh, D.; Yaseen, A.; Taim, D.; Zabadi, S.; Hamdan, A.A.; Hassona, Y.; Mahafzah, A.; Şahin, G.Ö. Dental students’ awareness and attitudes toward HPV-related oral cancer: A cross sectional study at the University of Jordan. BMC Oral Health 2019, 19, 171. [Google Scholar] [CrossRef] [Green Version]
- Abuhammad, S.; Muflih, S.; Alzoubi, K.H.; Gharaibeh, B. Nursing and PharmD Undergraduate Students’ Attitude Toward the “Do Not Resuscitate” Order for Children with Terminally Ill Diseases. J. Multidiscip. Healthc. 2021, 14, 425–434. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Group | Number (%) |
|---|---|---|
| Age in years (mean, SD 1) | 19.9 (1.4) | |
| Age | <21 years | 459 (74.6) |
| ≥21 years | 156 (25.4) | |
| Sex | Male | 183 (29.8) |
| Female | 432 (70.2) | |
| Place of residence | Amman (the capital) | 503 (81.8) |
| Outside Amman | 112 (18.2) | |
| School/Faculty | Medicine | 351 (57.1) |
| Dentistry | 191 (31.1) | |
| Nursing | 12 (2.0) | |
| Pharmacy | 23 (3.7) | |
| Laboratory Sciences | 31 (5.0) | |
| Rehabilitation | 7 (1.1) |
| Human Monkeypox Knowledge Item | Response | Age | p-Value, χ2 | Sex | p-Value, χ2 | ||
|---|---|---|---|---|---|---|---|
| <21 years | ≥21 years | Male | Female | ||||
| Monkeypox is prevalent in the Middle East * | Correct | 272 (59.3) | 98 (62.8) | 0.357, 2.061 | 109 (59.6) | 261 (60.4) | 0.769, 0.527 |
| Incorrect | 68 (14.8) | 16 (10.3) | 23 (12.6) | 61 (14.1) | |||
| Do not know | 119 (25.9) | 42 (26.9) | 51 (27.9) | 110 (25.5) | |||
| Monkeypox is prevalent in Western and Central Africa | Correct | 257 (56.0) | 104 (66.7) | 0.064, 5.497 | 91 (49.7) | 270 (62.5) | 0.001, 15.040 |
| Incorrect | 21 (4.6) | 5 (3.2) | 15 (8.2) | 11 (2.5) | |||
| Do not know | 181 (39.4) | 47 (30.1) | 77 (42.1) | 151 (35.0) | |||
| There is an outbreak of human monkeypox in the world | Correct | 238 (51.9) | 71 (45.5) | 0.121, 4.225 | 100 (54.6) | 209 (48.4) | 0.364, 2.023 |
| Incorrect | 150 (32.7) | 50 (32.1) | 54 (29.5) | 146 (33.8) | |||
| Do not know | 71 (15.5) | 35 (22.4) | 29 | 77 | |||
| Monkeypox is caused by a virus | Correct | 339 (73.9) | 136 (87.2) | 0.003, 11.781 | 143 (78.1) | 332 (76.9) | 0.897, 0.217 |
| Incorrect | 16 (3.5) | 3 (1.9) | 6 (3.3) | 13 (3.0) | |||
| Do not know | 104 (22.7) | 17 (10.9) | 34 (18.6) | 87 (20.1) | |||
| Human-to-human transmission of monkeypox occurs easily * | Correct | 170 (37.0) | 59 (37.8) | 0.430, 1.690 | 75 (41.0) | 154 (35.6) | 0.141, 3.914 |
| Incorrect | 136 (29.6) | 53 (34.0) | 46 (25.1) | 143 (33.1) | |||
| Do not know | 153 (33.3) | 44 (28.2) | 62 (33.9) | 135 (31.3) | |||
| Monkeypox and smallpox have similar signs and symptoms | Correct | 254 (55.3) | 107 (68.6) | <0.001, 16.076 | 98 (53.6) | 263 (60.9) | 0.189, 3.334 |
| Incorrect | 29 (6.3) | 16 (10.3) | 17 (9.3) | 28 (6.5) | |||
| Do not know | 176 (38.3) | 33 (21.2) | 68 (37.2) | 141 (32.6) | |||
| Skin rash is one of the signs or symptoms of human monkeypox | Correct | 359 (78.2) | 138 (88.5) | 0.019, 7.941 | 140 (76.5) | 357 (82.6) | 0.210, 3.122 |
| Incorrect | 9 (2.0) | 2 (1.3) | 4 (2.2) | 7 (1.6) | |||
| Do not know | 91 (19.8) | 16 (10.3) | 39 (21.3) | 68 (15.7) | |||
| Pustule is one of the signs or symptoms of human monkeypox | Correct | 347 (75.6) | 133 (85.3) | 0.041, 6.384 | 144 (78.7) | 336 (77.8) | 0.473, 1.499 |
| Incorrect | 22 (4.8) | 4 (2.6) | 5 (2.7) | 21 (4.9) | |||
| Do not know | 90 (19.6) | 19 (12.2) | 34 (18.6) | 75 (17.4) | |||
| Antibiotics are used to treat human monkeypox * | Correct | 174 (37.9) | 88 (56.4) | <0.001, 17.084 | 81 (44.3) | 181 (41.9) | 0.653, 0.853 |
| Incorrect | 84 (18.3) | 16 (10.3) | 26 (14.2) | 74 (17.1) | |||
| Do not know | 201 (43.8) | 52 (33.3) | 76 (41.5) | 177 (41.0) | |||
| Diarrhea is one of the signs or symptoms of human monkeypox * | Correct | 45 (9.8) | 24 (15.4) | 0.158, 3.692 | 14 (7.7) | 55 (12.7) | 0.047, 6.127 |
| Incorrect | 63 (13.7) | 19 (12.2) | 19 (10.4) | 63 (14.6) | |||
| Do not know | 351 (76.5) | 113 (72.4) | 150 (82.0) | 314 (72.7) | |||
| Vaccination is available to prevent human monkeypox | Correct | 109 (23.7) | 52 (33.3) | <0.001, 15.938 | 52 (28.4) | 109 (25.2) | 0.430, 1.689 |
| Incorrect | 167 (36.4) | 69 (44.2) | 73 (39.9) | 163 (37.7) | |||
| Do not know | 183 (39.9) | 35 (22.4) | 58 (31.7) | 160 (37.0) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sallam, M.; Al-Mahzoum, K.; Dardas, L.A.; Al-Tammemi, A.B.; Al-Majali, L.; Al-Naimat, H.; Jardaneh, L.; AlHadidi, F.; Al-Salahat, K.; Al-Ajlouni, E.; et al. Knowledge of Human Monkeypox and Its Relation to Conspiracy Beliefs among Students in Jordanian Health Schools: Filling the Knowledge Gap on Emerging Zoonotic Viruses. Medicina 2022, 58, 924. https://doi.org/10.3390/medicina58070924
Sallam M, Al-Mahzoum K, Dardas LA, Al-Tammemi AB, Al-Majali L, Al-Naimat H, Jardaneh L, AlHadidi F, Al-Salahat K, Al-Ajlouni E, et al. Knowledge of Human Monkeypox and Its Relation to Conspiracy Beliefs among Students in Jordanian Health Schools: Filling the Knowledge Gap on Emerging Zoonotic Viruses. Medicina. 2022; 58(7):924. https://doi.org/10.3390/medicina58070924
Chicago/Turabian StyleSallam, Malik, Kholoud Al-Mahzoum, Latefa Ali Dardas, Ala’a B. Al-Tammemi, Laith Al-Majali, Hala Al-Naimat, Laila Jardaneh, Farah AlHadidi, Khaled Al-Salahat, Eyad Al-Ajlouni, and et al. 2022. "Knowledge of Human Monkeypox and Its Relation to Conspiracy Beliefs among Students in Jordanian Health Schools: Filling the Knowledge Gap on Emerging Zoonotic Viruses" Medicina 58, no. 7: 924. https://doi.org/10.3390/medicina58070924