
Paroxysmal Finger Hematoma—A Probable Vascular Disorder in Post-COVID-19 Condition: Two Clinical Case Presentations



Abstract
:1. Introduction
2. Materials and Methods
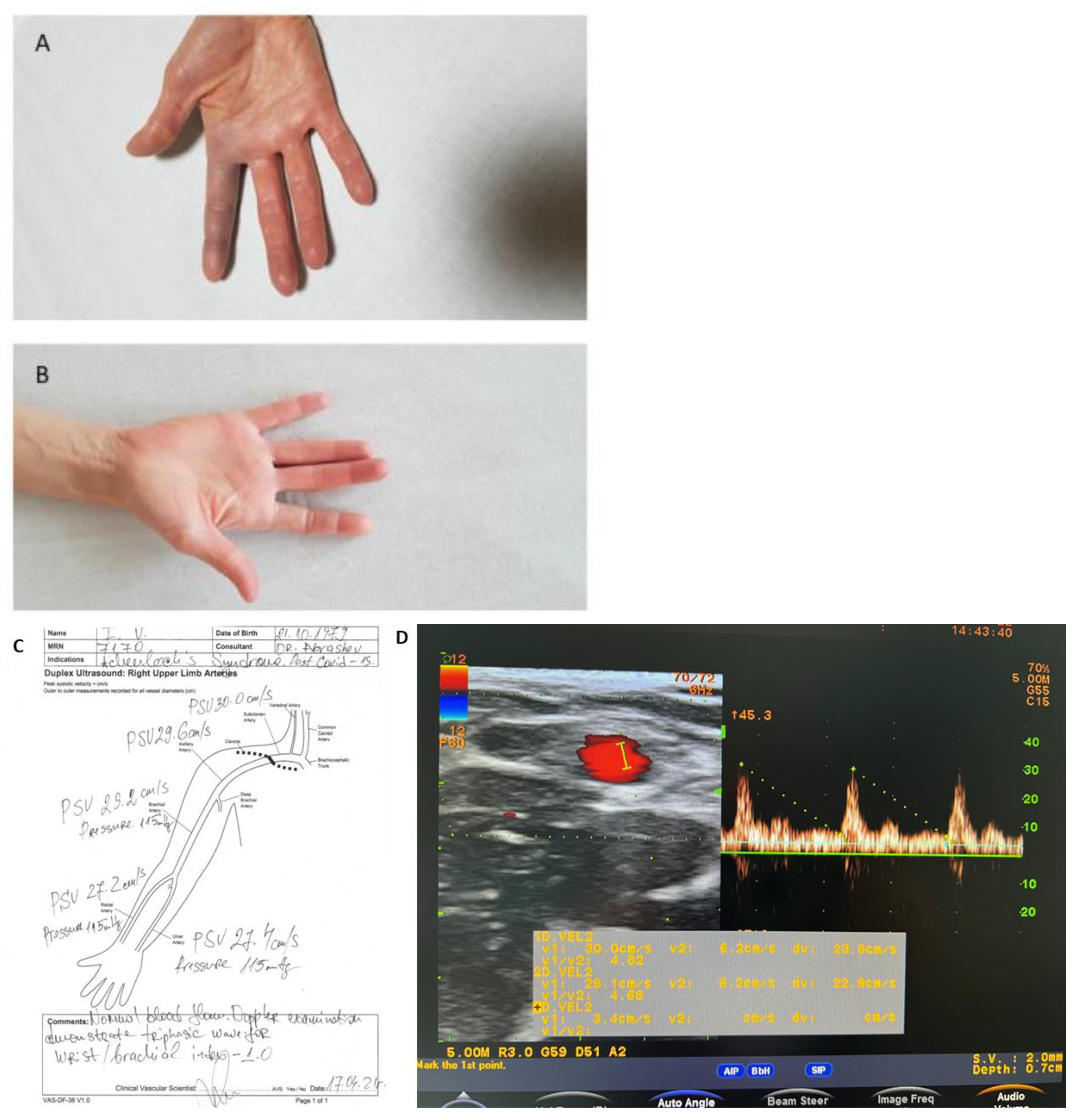
2.1. Case Report One
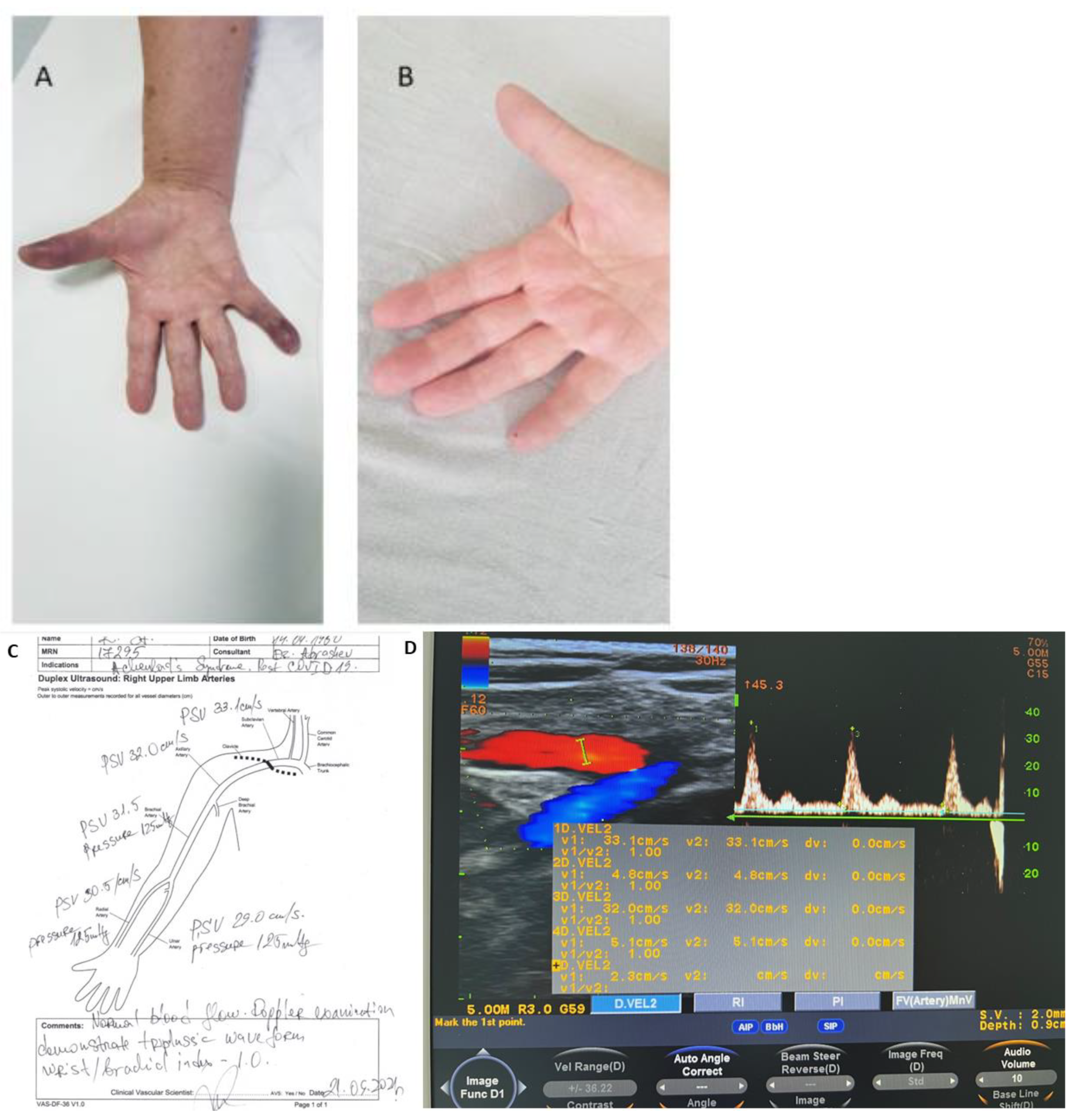
2.2. Case Report Two
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harnarayan, P.; Ramdass, M.J.; Islam, S.; Naraynsingh, V. Achenbach Syndrome Revisited: The Paroxysmal Finger Hematoma May Have a Genetic Link. Vasc. Health Risk Manag. 2021, 17, 809–816. [Google Scholar] [CrossRef] [PubMed]
- Godoy, A.; Tabares, A.H. Achenbach syndrome (paroxysmal finger hematoma). Vasc. Med. 2019, 24, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Ada, F.; Kasimzade, F. Analysis of 24 patients with Achenbach’s syndrome. World J. Clin. Cases 2019, 7, 1103–1110. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, H.; Uchida, H.A.; Okuyama, Y.; Wada, J. Acute idiopathic blue fingers: A young man with Achenbach’s syndrome. BMJ Case Rep. 2016, 2016, bcr2016214491. [Google Scholar] [CrossRef]
- Khaira, H.S.; Rittoo, D.; Vohra, R.K.; Smith, S.R. The non-ischaemic blue finger. Ann. R. Coll. Surg. Engl. 2001, 83, 154. [Google Scholar]
- Wang, X.; Sahu, K.K.; Cerny, J. Coagulopathy, endothelial dysfunction, thrombotic microangiopathy and complement activation: Potential role of complement system inhibition in COVID-19. J. Thromb. Thrombolysis 2021, 51, 657–662. [Google Scholar] [CrossRef]
- Al-Samkar, H.; Karp Leaf, R.S.; Dzik, W.H.; Carlson, J.C.; Fogerty, A.E.; Waheed, A.; Goodarzi, K.; Bendapudi, P.K.; Bornikova, L.; Gupta, S.; et al. COVID-19 and coagulation: Bleeding and thrombotic manifestations of SARS-CoV-2 infection. Blood 2020, 136, 489–500. [Google Scholar] [CrossRef]
- Fraissé, M.; Logre, E.; Pajot, O.; Mentec, H.; Plantefève, G.; Contou, D. Thrombotic and hemorrhagic events in critically ill COVID-19 patients: A French monocenter retrospective study. Crit. Care 2020, 24, 275. [Google Scholar] [CrossRef]
- Nadkarni, G.N.; Lala, A.; Bagiella, E.; Chang, H.L.; Moreno, P.R.; Pujadas, E.; Arvind, V.; Bose, S.; Charney, A.W.; Chen, M.D.; et al. Anticoagulation, bleeding, mortality, and pathology in hospitalized patients with COVID-19. J. Am. Coll. Cardiol. 2020, 76, 1815–1826. [Google Scholar] [CrossRef]
- Alharthy, A.; Faqihi, F.; Memish, Z.A.; Karakitsos, D. Fragile Endothelium and Brain Dysregulated Neurochemical Activity in COVID-19. ACS Chem. Neurosci. 2020, 11, 2159–2162. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H.; Levi, M.; Thachil, J. Coagulopathy in COVID-19. J. Thromb. Haemost. 2020, 18, 2103–2109. [Google Scholar] [CrossRef] [PubMed]
- Faggioli, P.M.; Mumoli, N.; Mazzone, A. Iloprost in COVID-19, The Rationale of Therapeutic Benefit. Front. Cardiovasc. Med. 2021, 8, 649499. [Google Scholar] [CrossRef] [PubMed]
- Chung, A.; Wildhirt, S.M.; Wang, S.; Koshal, A.; Radomski, M.W. Combined administration of nitric oxide gas and iloprost during cardiopulmonary bypass reduces platelet dysfunction: A pilot clinical study. J. Thorac. Cardiovasc. Surg. 2005, 129, 782–790. [Google Scholar] [CrossRef] [Green Version]
- Buffolo, F.; Monticone, S.; Camussi, G.; Aikawa, E. Role of Extracellular Vesicles in the Pathogenesis of Vascular Damage. Hypertension 2022, 79, 863–873. [Google Scholar] [CrossRef] [PubMed]
- Mulia, E.; Luke, K. Inhaled prostacyclin analogues in COVID-19 associated acute respiratory distress syndrome: Scientific rationale. Egypt. Heart J. 2021, 73, 82. [Google Scholar] [CrossRef]
- Carpentier, P.H.; Maricq, H.R.; Biro, C.; Jiguet, M.; Seinturier, C. Paroxysmal finger haematoma—A benign acrosyndrome occurring in middle-aged women. Vasa 2016, 45, 57–62. [Google Scholar] [CrossRef] [Green Version]
- Mills, J.L. Buerger’s disease: Current status. Vasc. Med. Rev. 1994, 2, 139–150. [Google Scholar] [CrossRef]
- Raveendran, A.V.; Jayadevan, R.; Sashidharan, S. Long COVID: An overview. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 869–875. [Google Scholar] [CrossRef]
- Lehman, H.; Acho, R.; Hans, S.S. Achenbach syndrome as a rare cause of painful, blue finger. J. Vasc. Surg. Cases Innov. Tech. 2021, 7, 589–592. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Liu, P.P.; Blet, A.; Smyth, D.; Li, H. The science underlying COVID-19: Implications for the cardiovascular system. Circulation 2020, 142, 68–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goshua, G.; Pine, A.B.; Meizlish, M.L.; Chang, C.H.; Zhang, H.; Zhang, H.; Bahel, P.; Baluha, A.; Bar, N.; Bona, R.D.; et al. Endotheliopathy in COVID-19-associated coagulopathy: Evidence from a single-centre, cross-sectional study. Lancet Haematol. 2020, 7, e575–e582. [Google Scholar] [CrossRef]
- Østergaard, L. SARS CoV-2 related microvascular damage and symptoms during and after COVID-19: Consequences of capillary transit-time changes, tissue hypoxia and inflammation. Physiol. Rep. 2021, 9, e14726. [Google Scholar] [CrossRef]
- Ribeir, F.; Aveiro, M.; Leal, M.; Valente, T.; Jesus, G. An Acute Blue Finger: A Case of Achenbach’s Syndrome. Eur. J. Case Rep. Intern. Med. 2019, 6, 9. [Google Scholar] [CrossRef]
- Zhai, Z.; Li, C.; Chen, Y.; Gerotziafas, G.; Zhang, Z.; Wan, J.; Liu, P.; Elalamy, I.; Wang, C. Prevention and treatment of venous thromboembolism associated with coronavirus disease 2019 infection: A consensus statement before guidelines. Thromb. Haemost. 2020, 120, 937–948. [Google Scholar] [CrossRef] [PubMed]
- Willoughby, S.R.; Luu, L.J.; Cameron, J.D.; Nelson, A.J.; Schultz, C.D.; Worthley, S.G.; Worthley, M.I. Clopidogrel improves microvascular endothelial function in subjects with stable coronary artery disease. Heart Lung Circ. 2014, 23, 534–541. [Google Scholar] [CrossRef]
- Fodor, A.; Tiperciuc, B.; Login, C.; Orasan, O.H.; Lazar, A.L.; Buchman, C.; Hanghicel, P.; Sitar-Taut, A.; Suharoschi, R.; Vulturar, R.; et al. Endothelial Dysfunction, Inflammation, and Oxidative Stress in COVID-19—Mechanisms and Therapeutic Targets. Oxidative Med. Cell. Longev. 2021, 2021, 8671713. [Google Scholar] [CrossRef]
- Cai, H.; Harrison, D.G. Endothelial dysfunction in cardiovascular diseases: The role of oxidant stress. Circ. Res. 2000, 87, 840–844. [Google Scholar] [CrossRef] [Green Version]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Azarfar, A.; Beg, S. Achenbach Syndrome: A Case Series. Cureus 2022, 14, 22824. [Google Scholar] [CrossRef]
- Montiel, V.; Lobysheva, I.; Gérard, L.; Vermeersch, M.; Perez-Morga, D.; Castelein, T.; Mesland, J.B.; Hantson, P.; Collienne, C.; Gruson, D.; et al. Oxidative stress-induced endothelial dysfunction and decreased vascular nitric oxide in COVID-19 patients. EBioMedicine 2022, 77, 103893. [Google Scholar] [CrossRef] [PubMed]
- Helm, R.H. Achenbach syndrome: A report of three familial cases. J. Hand. Surg. Eur. 2022, 47, 214–215. [Google Scholar] [CrossRef]
- Silva Andrade, B.; Siqueira, S.; de Assis Soares, W.R.; de Souza Rangel, F.; Santos, N.O.; dos Santos Freitas, A.; Ribeiro da Silveira, P.; Tiwari, S.; Alzahrani, K.J.; Góes-Neto, A.; et al. Long-COVID and post-COVID health complications: An up-to-date review on clinical conditions and their possible molecular mechanisms. Viruses 2021, 13, 700. [Google Scholar] [CrossRef] [PubMed]
- Gu, S.X.; Tyagi, T.; Jain, K.; Gu, V.W.; Lee, S.H.; Hwa, J.M.; Kwan, J.M.; Krause, D.S.; Lee, A.I.; Halene, S.; et al. Thrombocytopathy and endotheliopathy: Crucial contributors to COVID-19 thromboinflammation. Nat. Rev. Cardiol. 2021, 18, 194–209. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Test | Result | Unit | Reference Range |
|---|---|---|---|
| Leukocytes, (WBC) | 6.9 | g/L | 3.5–10.5 |
| Lymphocytes, (LYM) | 30.3 | % | 20–48 |
| Neutrophils, (Neu) | 61.9 | % | 40–70 |
| Monocytes, (Mo) | 7.8 | % | 1–11 |
| Erythrocytes, (RBC) | 4.56 | ×1012/L | 3.7–5.3 |
| Hemoglobin, (HGB) | 139 | g/L | 120–160 |
| Hematocrit, (HCT) | 0.392 | L/L | 0.360–0.480 |
| Mean corpuscular volume, (MCV) | 86.1 | fL | 80.0–96.0 |
| Mean corpuscular hemoglobin, (MCH) | 30.4 | pg | 27.0–33.0 |
| Red Cell Distribution Width, (RDW) | 15.1 | % | 11.2–14.7 |
| Platelet Count, (PLT) | 239 | ×109/L | 130–140 |
| Mean Platelet Volume, (MPV) | 7.3 | fL | 6.3–12,5 |
| Glucose | 5.64 | mmol/L | 3.6–6.1 |
| Creatinine | 60 | µmol/l | 65–127 |
| Uric acid | 201 | μmol/L | 142–340 |
| Erythrocyte Sedimentation Rate, (ESR) | 5 | mm/h | 0–39 |
| Total Bilirubin | 6.1 | µmol/L | <21 |
| Total protein, (TP) | 78.5 | g/L | 64.00–83.00 |
| Albumin | 47.1 | g/L | 35.00–52.00 |
| Aspartate Aminotransferase, (ASAT) | 20.4 | U/L | <40.00 |
| Alanine Aminotransferase, (ALAT) | 17.3 | U/L | <33.00 |
| Creatine Kinase, (CK) | 88 | U/l | <170.0 |
| C-reactive protein, (CRP) | 0.2 | mg/l | <5 |
| Factor V Leiden, (FVL) | Negative | PCR-RFLP | |
| Sodium levels, Na+ | 136 | mmol/L | 136.00–151.00 |
| Potassium levels, K+ | 4.1 | mmol/L | 3.50–5.60 |
| Rheumatoid Factor (RF) | 8 | IU/mL | <20 |
| Fibrinogen | 2.12 | g/L | 2–4 g/L |
| International Normalized Ratio (INR) | 0.94 | UI | 0.8–1.2 |
| Prothrombin time (PT) | 108.9 | % | 70–130 |
| Activated Partial Thromboplastin Time (APTT) | 31.1 | sec | 27.6–37.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abrashev, H.; Ananiev, J.; Georgieva, E. Paroxysmal Finger Hematoma—A Probable Vascular Disorder in Post-COVID-19 Condition: Two Clinical Case Presentations. Medicina 2022, 58, 915. https://doi.org/10.3390/medicina58070915
Abrashev H, Ananiev J, Georgieva E. Paroxysmal Finger Hematoma—A Probable Vascular Disorder in Post-COVID-19 Condition: Two Clinical Case Presentations. Medicina. 2022; 58(7):915. https://doi.org/10.3390/medicina58070915
Chicago/Turabian StyleAbrashev, Hristo, Julian Ananiev, and Ekaterina Georgieva. 2022. "Paroxysmal Finger Hematoma—A Probable Vascular Disorder in Post-COVID-19 Condition: Two Clinical Case Presentations" Medicina 58, no. 7: 915. https://doi.org/10.3390/medicina58070915