
Seroprevalence of Hepatitis E Virus Infection in Middle Eastern Countries: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Literature Search Strategy
2.2. Eligibility Criteria
2.3. Study Screening and Data Extraction
2.4. Quality Assessment
2.5. Data Synthesis and Statistical Analysis
3. Results
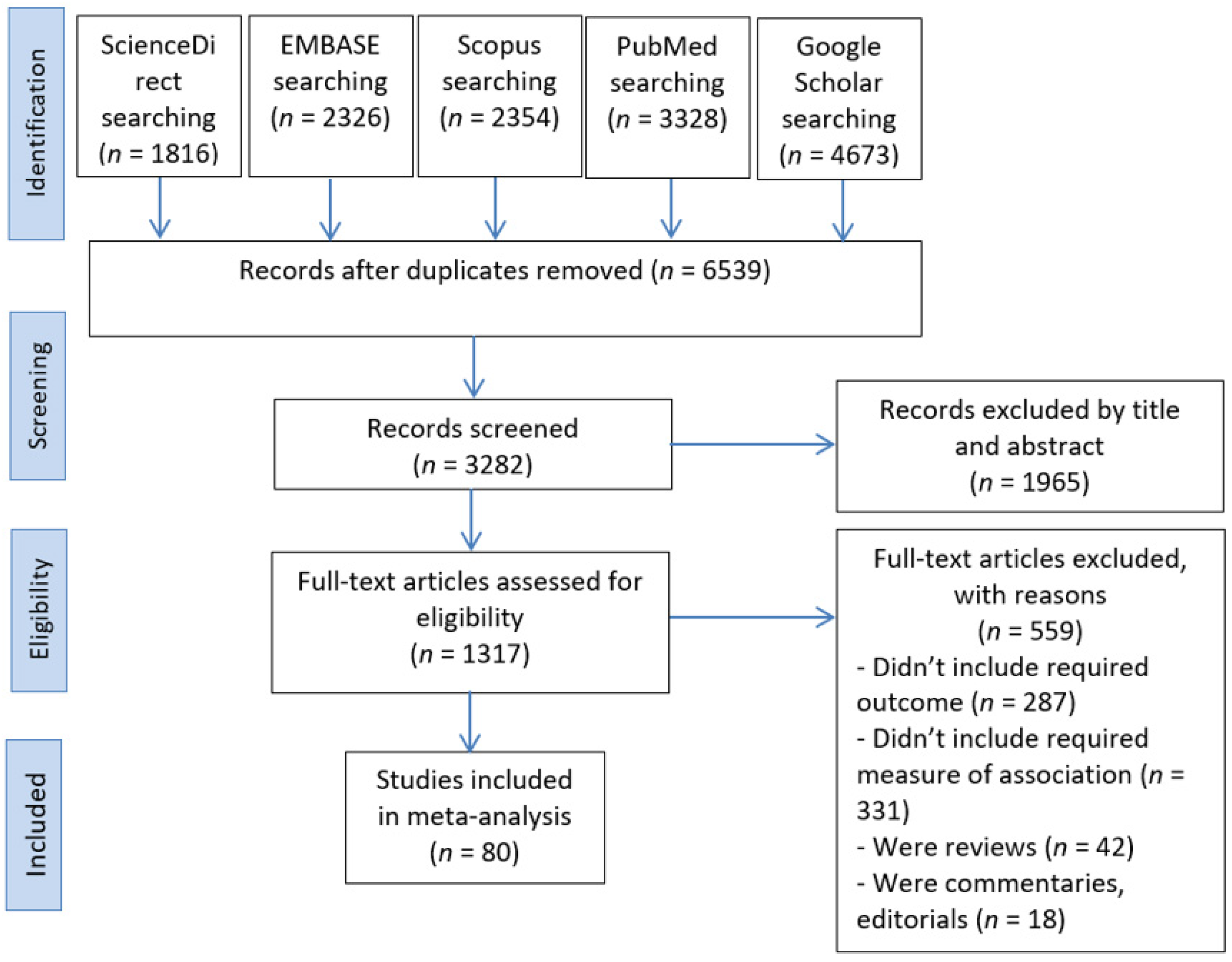
3.1. Search Outcomes
3.2. Characteristics of the Included Studies
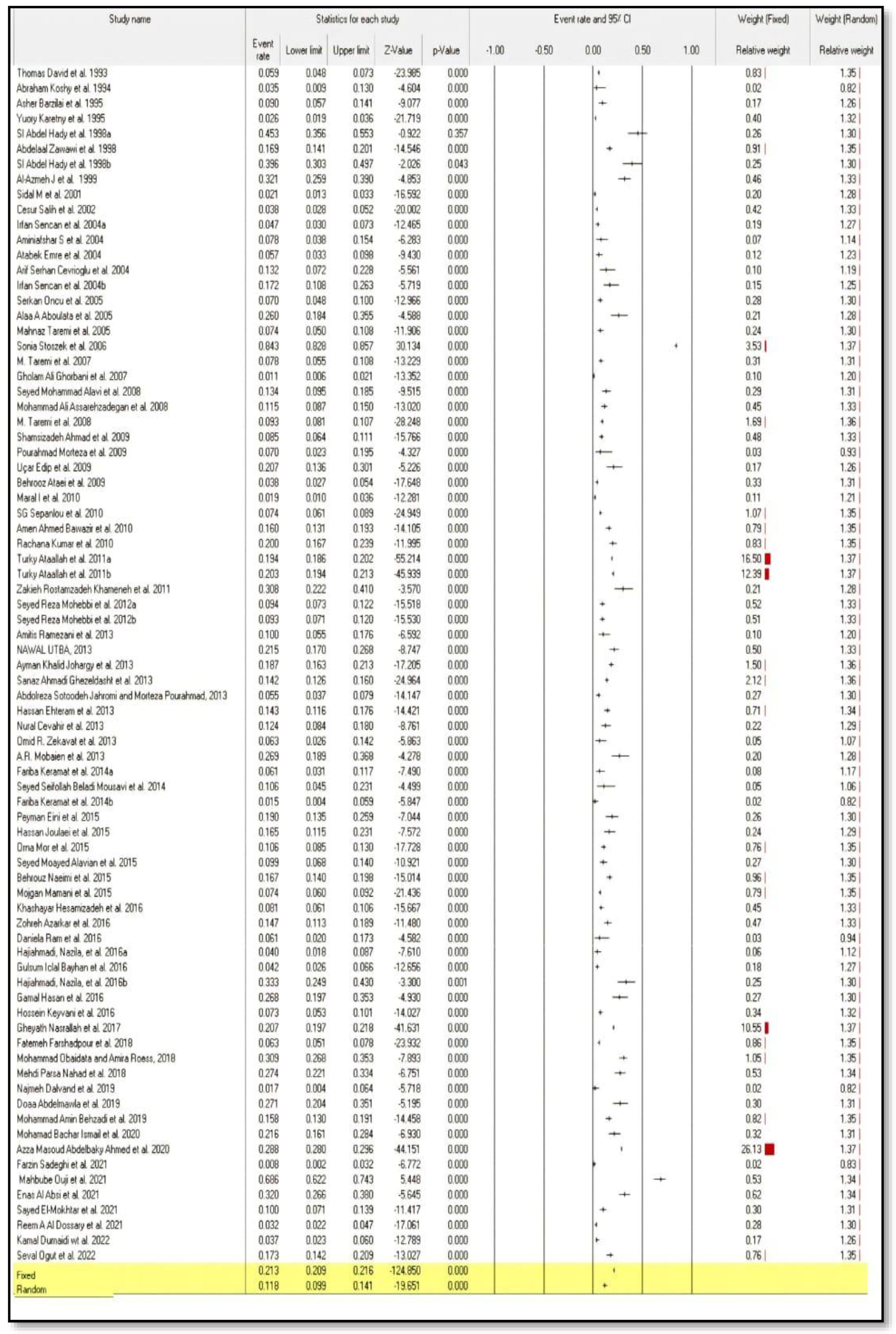
3.3. Overall Pooled Seroprevalence of Hepatitis E Virus Infection in Middle Eastern Countries
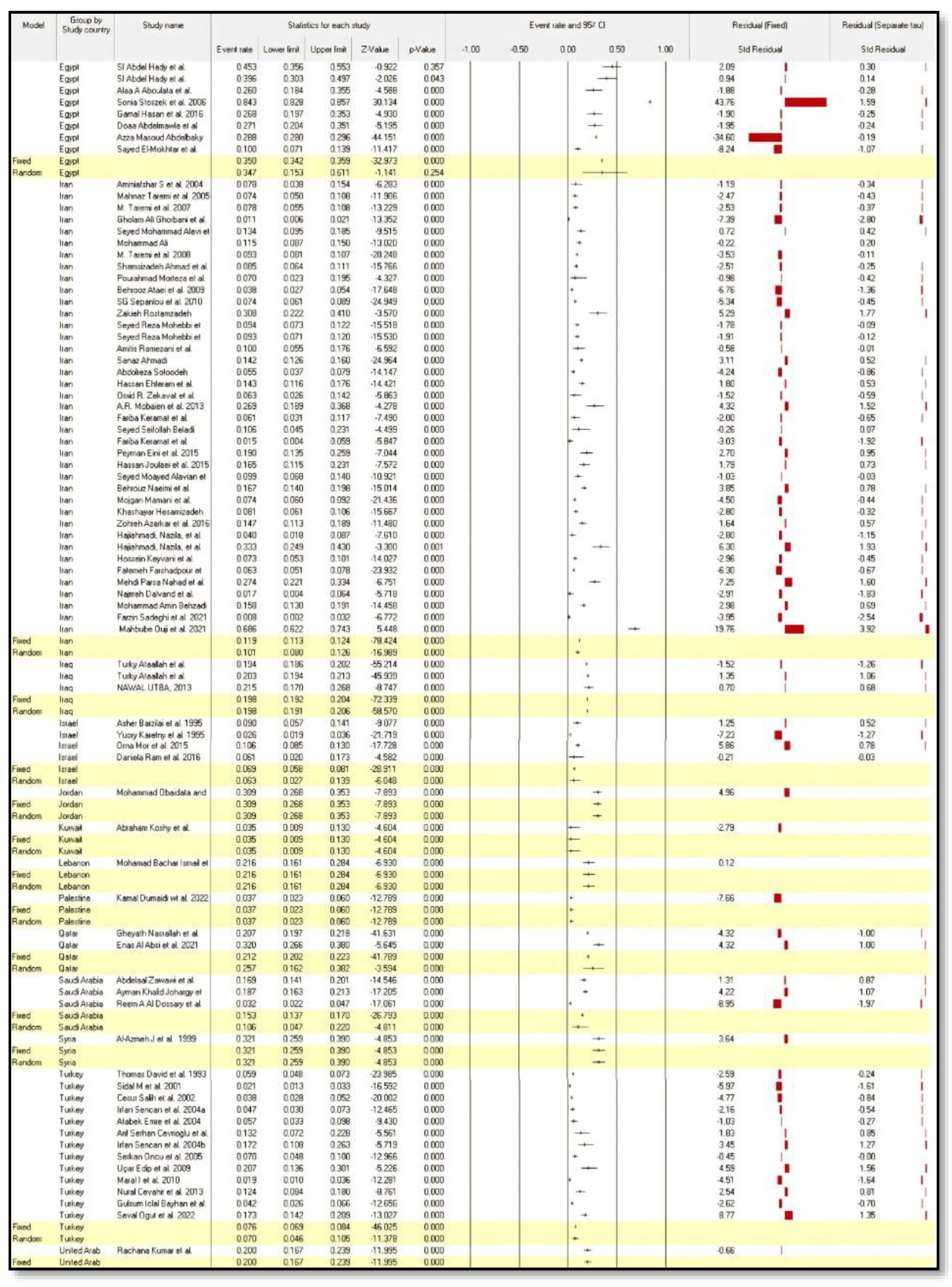
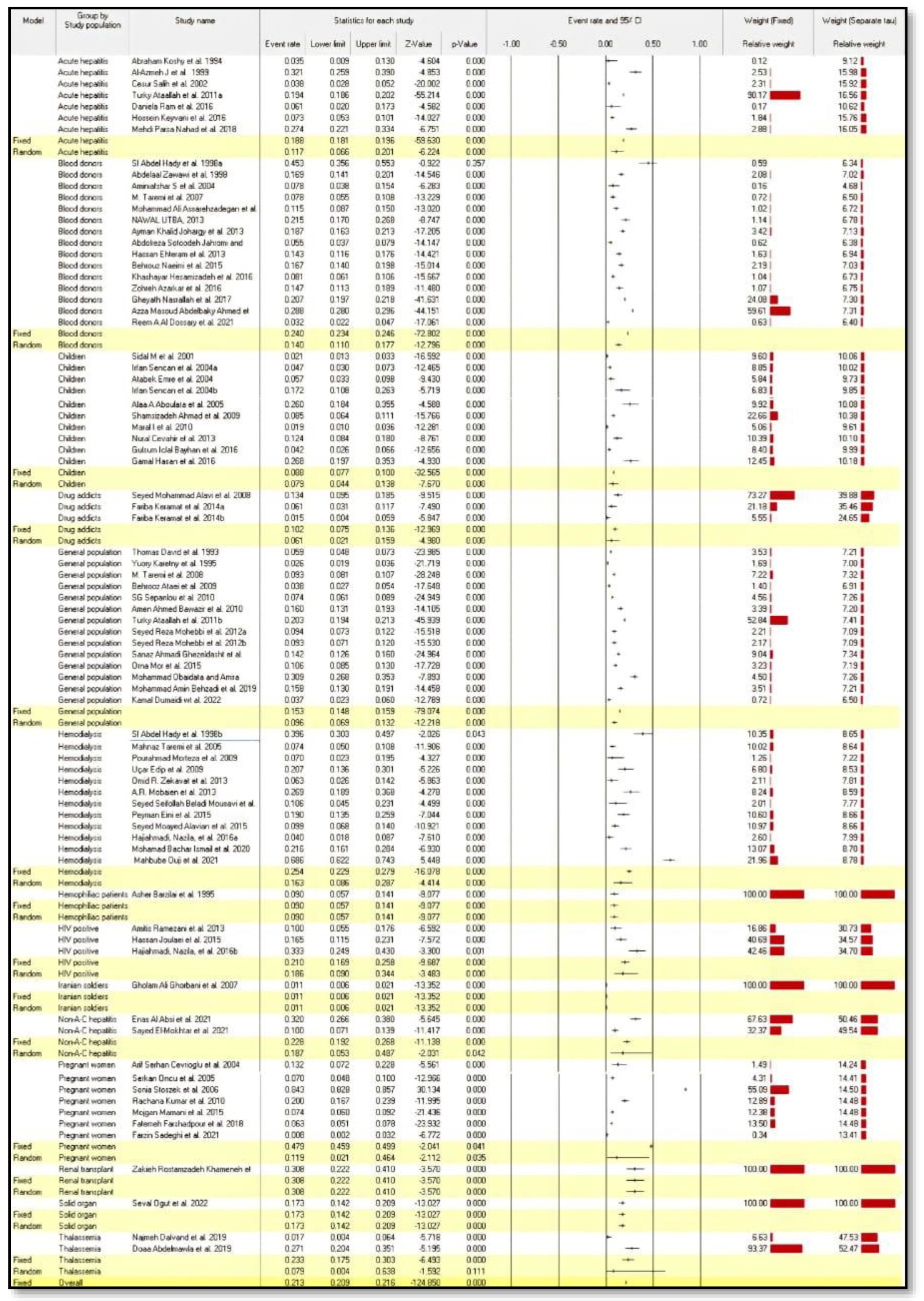
3.4. Subgroup Analysis
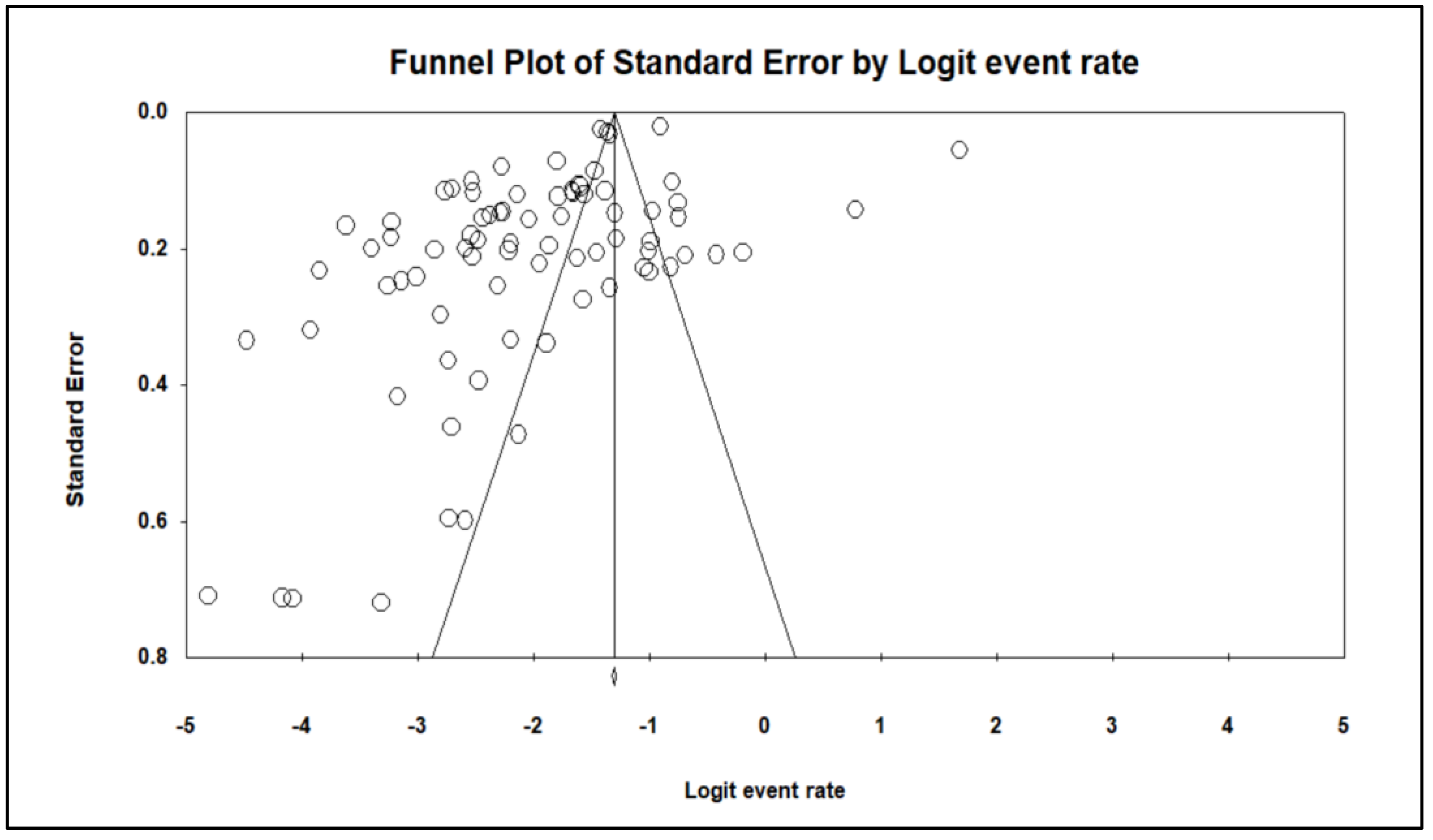
3.5. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Global Health Sector Strategy on Viral Hepatitis 2016–2021: Towards Ending Viral Hepatitis; World Health Organization: Geneva, Switzerland, 2016.
- WHO. Global Hepatitis Report 2017; World Health Organization: Geneva, Switzerland, 2017.
- Bigna, J.J.; Modiyinji, A.F.; Nansseu, J.R.; Amougou, M.A.; Nola, M.; Kenmoe, S.; Temfack, E.; Njouom, R. Burden of hepatitis E virus infection in pregnancy and maternofoetal outcomes: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2020, 20, 426. [Google Scholar] [CrossRef] [PubMed]
- Dalton, H.R.; Izopet, J. Transmission and epidemiology of hepatitis E virus genotype 3 and 4 infections. Cold Spring Harb. Perspect. Med. 2018, 8, a032144. [Google Scholar] [CrossRef] [PubMed]
- Izopet, J.; Lhomme, S.; Chapuy-Regaud, S.; Mansuy, J.-M.; Kamar, N.; Abravanel, F. HEV and transfusion-recipient risk. Transfus. Clin. Biol. 2017, 24, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.B.; Simmonds, P. Hepatitis E virus and fulminant hepatitis—A virus or host-specific pathology? Liver Int. 2015, 35, 1334–1340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirazo, S.; Ramos, N.; Mainardi, V.; Gerona, S.; Arbiza, J. Transmission, diagnosis, and management of hepatitis E: An update. Hepatic Med. Evid. Res. 2014, 6, 45. [Google Scholar] [CrossRef]
- Pérez-Gracia, M.T.; Suay, B.; Mateos-Lindemann, M.L. Hepatitis E: An emerging disease. Infect. Genet. Evol. 2014, 22, 40–59. [Google Scholar] [CrossRef]
- Fujiwara, S.; Yokokawa, Y.; Morino, K.; Hayasaka, K.; Kawabata, M.; Shimizu, T. Chronic hepatitis E: A review of the literature. J. Viral Hepat. 2014, 21, 78–89. [Google Scholar] [CrossRef]
- Aggarwal, R. Diagnosis of hepatitis E. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 24–33. [Google Scholar] [CrossRef]
- Alavian, S.M.; Rezaee-Zavareh, M.S. The Middle East and hepatitis C virus infection: Does it need special attention? Lancet Infect. Dis. 2016, 16, 1006–1007. [Google Scholar] [CrossRef] [Green Version]
- Tufenkeji, H. Hepatitis A shifting epidemiology in the Middle East and Africa. Vaccine 2000, 18, S65–S67. [Google Scholar] [CrossRef]
- Mahboobi, N.; Alavian, S.M. Hepatitis A in the Eastern Mediterranean region: A review on the prevalence. Scimetr 2014, 2, e87346. [Google Scholar] [CrossRef]
- Franco, E.; Bagnato, B.; Marino, M.G.; Meleleo, C.; Serino, L.; Zaratti, L. Hepatitis B: Epidemiology and prevention in developing countries. World J. Hepatol. 2012, 4, 74. [Google Scholar] [CrossRef] [PubMed]
- Rezaee-Zavareh, M.S.; Karimi-Sari, H.; Dolatimehr, F.; Alavian, S.M. Hepatitis A virus infection, vaccination and Iranian healthcare workers. Hepat. Mon. 2015, 15, e35238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NHLBI. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies; National Heart, Lung, and Blood Institute: Bethesda, MA, USA, 2014.
- NHLBI. National Institute of Health Study Quality Assessment Tool; National Heart, Lung, and Blood Institute: Bethesda, MA, USA, 2017.
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef]
- Thomas, D.L.; Quinn, T.; Mahley, R.; Palaoglu, K.E.; Badur, S. Epidemiology of hepatitis E virus infection in Turkey. Lancet 1993, 341, 1561–1562. [Google Scholar] [CrossRef]
- Koshy, A.; Richards, A.L.; Al-Mufti, S.; Grover, S.; Shabrawy, M.A.; Pacsa, A.; Al-Anezi, A.A.H.; Al-Nakib, B.; Burans, J.; Carl, M. Acute sporadic hepatitis E in Kuwait. J. Med. Virol. 1994, 42, 405–408. [Google Scholar] [CrossRef]
- Barzilai, A.; Schulman, S.; Karetnyi, Y.V.; Favorov, M.O.; Levin, E.; Mendelson, E.; Weiss, P.; Fields, H.A.; Varon, D.; Martinowitz, U. Hepatitis E virus infection in hemophiliacs. J. Med. Virol. 1995, 46, 153–156. [Google Scholar] [CrossRef]
- Karetnyi, Y.V.; Handsher, R.; Aboudy, Y.; Varsano, N.; Mendelson, E.; Weiss, P.; Levin, E.; Bar-Shani, S.; Schwartz, E.; Fields, H.A. Serological evidence for hepatitis E virus infection in Israel. J. Med. Virol. 1995, 45, 316–320. [Google Scholar] [CrossRef]
- Abdelaal, M.; Zawawi, T.; Al Sobhi, E.; Jeje, O.; Gilpin, C.; Kinsara, A.; Osoba, A.; Oni, G. Epidemiology of hepatitis E virus in male blood donors in Jeddah, Saudi Arabia. Ir. J. Med. Sci. 1998, 167, 94–96. [Google Scholar] [CrossRef]
- SI, A.H.; El-Din, M.S.; El-Din, M.E. A high hepatitis E virus (HEV) seroprevalence among unpaid blood donors and haemodialysis patients in Egypt. J. Egypt. Public Health Assoc. 1998, 73, 165–179. [Google Scholar]
- Al-Azmeh, J.; Frösner, G.; Darwish, Z.; Bashour, H.; Monem, F. Hepatitis E in Damascus, Syria. Infection 1999, 27, 221–223. [Google Scholar] [CrossRef] [PubMed]
- Sıdal, M.; Ünüvar, E.; Oğuz, F.; Cihan, C.; Önel, D.; Badur, S. Age-specific seroepidemiology of hepatitis A, B, and E infections among children in Istanbul, Turkey. Eur. J. Epidemiol. 2001, 17, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Colak, D.; Ogunc, D.; Gunseren, F.; Velipasaoglu, S.; Aktekin, M.; Gültekin, M. Seroprevalence of antibodies to hepatitis A and E viruses in pediatric age groups in Turkey. Acta Microbiol. Et Immunol. Hung. 2002, 49, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Cesur, S.; Akin, K.; Doğaroğlu, I.; Birengel, S.; Balik, I. Hepatitis A and hepatitis E seroprevalence in adults in the Ankara area. Mikrobiyoloji Bul. 2002, 36, 79–83. [Google Scholar]
- Cevrioglu, A.S.; Altindis, M.; Tanir, H.M.; Aksoy, F. Investigation of the incidence of hepatitis E virus among pregnant women in Turkey. J. Obstet. Gynaecol. Res. 2004, 30, 48–52. [Google Scholar] [CrossRef]
- Sencan, I.; Sahin, I.; Kaya, D.; Oksuz, S.; Yildirim, M. Assessment of HAV and HEV seroprevalence in children living in post-earthquake camps from Düzce, Turkey. Eur. J. Epidemiol. 2004, 19, 461–465. [Google Scholar] [CrossRef]
- Atabek, M.E.; Fýndýk, D.; Gulyuz, A.; Erkul, I. Prevalence of anti-HAV and anti-HEV antibodies in Konya, Turkey. Health Policy 2004, 67, 265–269. [Google Scholar] [CrossRef]
- Aminiafshar, S.; Alimagham, M.; Gachkar, L.; Yousefi, F.; Attarchi, Z. Anti hepatitis E virus seropositivity in a group of blood donors. Iran. J. Public Health 2004, 33, 53–56. [Google Scholar]
- Oncu, S.; Oncu, S.; Okyay, P.; Ertug, S.; Sakarya, S. Prevalence and risk factors for HEV infection in pregnant women. Med. Sci. Monit. 2006, 12, 39. [Google Scholar]
- Aboulata, A.A.; Ahmad, M.S.; Shaban, M.; Zayd, K.; AM, A.E.-M. Prevalence of hepatitis E virus in Egyptian children presented with minor hepatic disorders. Egypt. J. Immunol. 2005, 12, 71–76. [Google Scholar] [PubMed]
- Taremi, M.; Khoshbaten, M.; Gachkar, L.; EhsaniArdakani, M.; Zali, M. Hepatitis E virus infection in hemodialysis patients: A seroepidemiological survey in Iran. BMC Infect. Dis. 2005, 5, 36. [Google Scholar] [CrossRef] [Green Version]
- Stoszek, S.K.; Abdel-Hamid, M.; Saleh, D.a.A.; Kafrawy, S.E.; Narooz, S.; Hawash, Y.; Shebl, F.M.; El Daly, M.; Said, A.; Kassem, E. High prevalence of hepatitis E antibodies in pregnant Egyptian women. Trans. R. Soc. Trop. Med. Hyg. 2006, 100, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Taremi, M.; Gachkar, L.; MahmoudArabi, S.; Kheradpezhouh, M.; Khoshbaten, M. Prevalence of antibodies to hepatitis E virus among male blood donors in Tabriz, Islamic Republic of Iran. East. Mediterr. Health J. 2007, 13, 98–102. [Google Scholar] [PubMed]
- Ghorbani, G.A.; Alavian, S.-M.; Esfahani, A.A.; Assari, S. Seroepidemiology of hepatitis E virus in Iranian soldiers. Hepat. Mon. 2007, 7, 123–126. [Google Scholar]
- Alavi, S.M.; Ahmadi, F.; Ghasemirad, M.R. Seroepidemiological study of hepatitis E virus in drug addicts in Ahvaz, Southern Iran: 2005–2006. Hepat. Mon. 2008, 8, 263–266. [Google Scholar]
- Assarehzadegan, M.A.; Shakerinejad, G.; Amini, A.; Rezaee, S.R. Seroprevalence of hepatitis E virus in blood donors in Khuzestan Province, southwest Iran. Int. J. Infect. Dis. 2008, 12, 387–390. [Google Scholar] [CrossRef] [Green Version]
- Taremi, M.; Alizadeh, A.; Ardalan, A.; Ansari, S.; Zali, M. Seroprevalence of hepatitis E in Nahavand, Islamic Republic of Iran: A population-based study. East. Mediterr. Health J. 2008, 14, 157–162. [Google Scholar]
- Uçar, E.; Cetin, M.; Kuvandik, C.; Helvaci, M.R.; Güllü, M.; Hüzmeli, C. Hepatitis E virus seropositivity in hemodialysis patients in Hatay province, Turkey. Mikrobiyoloji Bul. 2009, 43, 299–302. [Google Scholar]
- Shamsizadeh, A.; Nikfar, R.; Makvandi, M.; Shamsizadeh, N. Seroprevalence of hepatitis E virus infection in children in the Southwest of Iran. Hepat. Mon. 2009, 9, 269–276. [Google Scholar]
- Ataei, B.; Nokhodian, Z.; Javadi, A.A.; Kassaian, N.; Shoaei, P.; Farajzadegan, Z.; Adibi, P. Hepatitis E virus in Isfahan Province: A population-based study. Int. J. Infect. Dis. 2009, 13, 67–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pourahmad, M.; Sotoudeh, J.A.; Nasiri, H. Brief Report: Hepatitis E virus infection in hemodialysis patients: A seroepidemiological survey in Jahrom, Southern Iran. Hepat. Mon. 2009, 9, 232–235. [Google Scholar]
- Maral, I.; Budakoglu, I.; Ceyhan, M.; Atak, A.; Bumin, M. Hepatitis E virus seroepidemiology and its change during 1 year in primary school students in Ankara, Turkey. Clin. Microbiol. Infect. 2010, 16, 831–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bawazir, A.A.; Hart, C.A.; Sallam, T.A.; Parry, C.M.; Beeching, N.J.; Cuevas, L.E. Seroepidemiology of hepatitis A and hepatitis E viruses in Aden, Yemen. Trans. R. Soc. Trop. Med. Hyg. 2010, 104, 801–805. [Google Scholar] [CrossRef]
- Kumar, R.M.; Uduman, S.; Rana, S.; Kochiyil, J.K.; Usmani, A.; Thomas, L. Sero-prevalence and mother-to-infant transmission of hepatitis E virus among pregnant women in the United Arab Emirates. Eur. J. Obstet. Gynecol. Reprod. Biol. 2001, 100, 9–15. [Google Scholar] [CrossRef]
- Sepanlou, S.G.; Rezvan, H.; Amini-Kafiabad, S.; Dayhim, M.; Merat, S. A population-based seroepidemiological study on hepatitis E virus in Iran. Middle East J. Dig. Dis. 2010, 2, 97. [Google Scholar]
- Turky, A.M.; Akram, W.; Al-Naaimi, A.S.; Omer, A.R.; Al-Rawi, J.R. Analysis of acute viral hepatitis (A and E) in Iraq. Glob. J. Health Sci. 2011, 3, 70. [Google Scholar] [CrossRef]
- Khameneh, Z.R.; Sepehrvand, N.; Masudi, S. Seroprevalence of hepatitis E among Iranian renal transplant recipients. Hepat. Mon. 2011, 11, 646. [Google Scholar] [CrossRef]
- Mohebbi, S.R.; Rostami Nejad, M.; Tahaei, S.M.E.; Pourhoseingholi, M.A.; Habibi, M.; Azimzadeh, P.; Naghoosi, H.; Karayiannis, P.; Zali, M.R. Seroepidemiology of hepatitis A and E virus infections in Tehran, Iran: A population based study. Trans. R. Soc. Trop. Med. Hyg. 2012, 106, 528–531. [Google Scholar] [CrossRef]
- Jahromi, A.S.; Pourahmad, M. Hepatitis E virus and serum level aminotransferases in blood donors. Rep. Biochem. Mol. Biol. 2013, 2, 48. [Google Scholar]
- Ghezeldasht, S.A.; Miri, R.; Hedayatimoghadam, M.; Shamsian, A.; Bidkhori, H.; Fathimoghadam, F.; Rezaee, S.A. Population movement and virus spreading: HEV spreading in a Pilgrimage city, Mashhad in northeast Iran; an example. Hepat. Mon. 2013, 13, e10255. [Google Scholar] [CrossRef] [PubMed]
- Cevahir, N.; Demir, M.; Bozkurt, A.I.; Ergin, A.; Kaleli, I. Seroprevalence of hepatitis e virus among primary school children. Pak. J. Med. Sci. 2013, 29, 629. [Google Scholar] [CrossRef] [PubMed]
- Ehteram, H.; Ramezani, A.; Eslamifar, A.; Sofian, M.; Banifazl, M.; Ghassemi, S.; Aghakhani, A.; Mashayekhi, P. Seroprevalence of Hepatitis E Virus infection among volunteer blood donors in central province of Iran in 2012. Iran. J. Microbiol. 2013, 5, 172. [Google Scholar] [PubMed]
- Zekavat, O.R.; Makarem, A.; Karami, M.Y.; Amanat, A.; Mohandes, M.; Habibagahi, M. Serological investigation for hepatitis E virus infection in the patients with chronic maintenance hemodialysis from southwest of Iran. Asian J. Transfus. Sci. 2013, 7, 21. [Google Scholar]
- Mobaien, A.; Mohammadi, R.; Sorouri, R.; Sadeghi, K. Hepatitis E virus seroprevalence in haemodialysis patients in Zanjan Province, Islamic Republic of Iran. East. Mediterr. Health J. 2013, 19, 608–612. [Google Scholar] [CrossRef]
- Johargy, A.K.; Mahomed, M.F.; Khan, M.M.; Kabrah, S. Anti hepatitis E virus seropositivity in a group of male blood donors in Makkah, Saudi Arabia. J. Pak. Med. Assoc. 2013, 63, 185–189. [Google Scholar]
- Utba, N.M. The prevalence of hepatitis E virus in Al-Sadr City-Baghdad. Clin. Lab. 2013, 59, 115–120. [Google Scholar] [CrossRef]
- Ramezani, A.; Velayati, A.A.; Khorami-Sarvestani, S.; Eslamifar, A.; Mohraz, M.; Banifazl, M.; Bidari-Zerehpoosh, F.; Yaghmaei, F.; McFarland, W.; Foroughi, M. Hepatitis E virus infection in patients infected with human immunodeficiency virus in an endemic area in Iran. Int. J. STD AIDS 2013, 24, 769–774. [Google Scholar] [CrossRef]
- Keramat, F.; Mamani, M.; Samadi, M.; Mohammadnezhad, S.; Eini, P.; Moradi, A. Seroprevalence of hepatitis E Virus among injection drug users and non-injection drug users in Hamadan, west of Iran. Avicenna J. Clin. Microbiol. Infect. 2014, 1, 22343. [Google Scholar] [CrossRef] [Green Version]
- Mousavi, S.S.B.; Motemednia, F.; Mousavi, M.B. Epidemiology of hepatitis e virus infection in patients on chronic hemodialysis. Jundishapur J. Microbiol. 2014, 7, e6993. [Google Scholar]
- Eini, P.; Mamani, M.; Javani, M. Seroprevalence of hepatitis e among hemodialysis patients: A report from Hamadan, Iran. Hepat. Mon. 2015, 15, e26260. [Google Scholar] [CrossRef] [Green Version]
- Mor, O.; Bassal, R.; Michaeli, M.; Wax, M.; Ram, D.; Cohen-Ezra, O.; Cohen, D.; Mendelson, E.; Ben-Ari, Z.; Shohat, T. Prevalence of hepatitis E virus antibodies, Israel, 2009–2010. Emerg. Infect. Dis. 2015, 21, 692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mamani, M.; Zamani, M.; Hashemi, S.H.; Keramat, F. Seroprevalence of antibodies to hepatitis E virus among pregnant women. Avicenna J. Clin. Microbiol. Infect. 2015, 2, 25339. [Google Scholar] [CrossRef]
- Alavian, S.M.; Ataei, B.; Ebrahimi, A.; Pirhaji, O.; Azad, R.; Olya, B.; Ataei, A.M. Anti-hepatitis E antibody in hemodialysis patients in Isfahan, Iran: Prevalence and risk factors. Hepat. Mon. 2015, 15, e23633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joulaei, H.; Rudgari, O.; Motazedian, N.; Gorji-Makhsous, S. Hepatitis E virus seroprevalence in HIV positive individuals in Shiraz, Southern Iran. Iran. J. Microbiol. 2015, 7, 103–108. [Google Scholar]
- Naeimi, B.; Kalimani, F.M.; Pourfatolah, A.A.; Azimzadeh, M.; Mankhian, A.; Akbarzadeh, S.; Hajiani, G.; Kooshesh, F.; Khamisipour, G. Hepatitis E Virus seroprevalence among blood donors in Bushehr, South of Iran. Hepat. Mon. 2015, 15, e29219. [Google Scholar] [CrossRef] [Green Version]
- Ram, D.; Manor, Y.; Gozlan, Y.; Schwartz, E.; Ben-Ari, Z.; Mendelson, E.; Mor, O. Hepatitis E virus genotype 3 in sewage and genotype 1 in acute hepatitis cases, Israel. Am. J. Trop. Med. Hyg. 2016, 95, 216–220. [Google Scholar] [CrossRef] [Green Version]
- Keyvani, H.; Shamabadi, M.S.; Najafifard, S.; Hajibeigi, B.; Fallahian, F.; Alavian, S.-M. Seroprevalence of anti-HEV and HEV RNA among volunteer blood donors and patients with Hepatitis B and C in Iran. Bangladesh Liver J. 2009, 1, 34–37. [Google Scholar] [CrossRef]
- Hajiahmadi, N.; Moradi, A.; Vakili, M.A.; Javid, N.; Kelishadi, M.; Bazouri, M.; Tabarraei, A. Hepatitis E virus Seroprevalence and viremia in hemodialysis and HIV infected patients in Iran. Iran. J. Virol. 2016, 10, 12–17. [Google Scholar] [CrossRef]
- Hesamizadeh, K.; Sharafi, H.; Keyvani, H.; Alavian, S.M.; Shabankareh, A.N.-T.; Olyaie, R.S.; Keshvari, M. Hepatitis A virus and hepatitis E virus seroprevalence among blood donors in Tehran, Iran. Hepat. Mon. 2016, 16, e32215. [Google Scholar] [CrossRef] [Green Version]
- Azarkar, Z.; Miri, M.R.; Arjmand, S. Investigating the seroprevalence of hepatitis E among blood donors referring to blood donation centers in Birjand county in Iran. Mod. Care J. 2016, 13, e9456. [Google Scholar] [CrossRef] [Green Version]
- Hasan, G.; Assiri, A.; Marzuuk, N.; Daef, E.; Abdelwahab, S.; Ahmed, A.; Mohamad, I.; Al-Eyadhy, A.; Alhaboob, A.; Temsah, M.-H. Incidence and characteristics of hepatitis E virus infection in children in Assiut, Upper Egypt. J. Int. Med. Res. 2016, 44, 1115–1122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayhan, G.İ.; Demiören, K.; Güdücüoğlu, H. Epidemiology of hepatitis E virus in children in the province of Van, Turkey. Turk. Arch. Pediatrics 2016, 51, 148. [Google Scholar] [CrossRef] [PubMed]
- Nasrallah, G.K.; Al Absi, E.S.; Ghandour, R.; Ali, N.H.; Taleb, S.; Hedaya, L.; Ali, F.; Huwaidy, M.; Husseini, A. Seroprevalence of hepatitis E virus among blood donors in Qatar (2013–2016). Transfusion 2017, 57, 1801–1807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obaidat, M.M.; Roess, A.A. Seroprevalence and risk factors of Hepatitis E infection in Jordan’s population: First report. Int. J. Infect. Dis. 2018, 66, 121–125. [Google Scholar] [CrossRef] [Green Version]
- Farshadpour, F.; Taherkhani, R.; Ravanbod, M.R.; Eghbali, S.S.; Taherkhani, S.; Mahdavi, E. Prevalence, risk factors and molecular evaluation of hepatitis E virus infection among pregnant women resident in the northern shores of Persian Gulf, Iran. PLoS ONE 2018, 13, e0191090. [Google Scholar] [CrossRef] [Green Version]
- Parsa Nahad, M.; Bavi, A.; Zandi, M.; Nejati, M.; Rabie Rudsari, M.; Dehghani, M.A.; Kiani, H.; Ramezani, A.; Khosravi Seftejani, S.; Omidi, N. Seroprevalence of Hepatitis E Virus Infection among Patients with Acute Hepatitis Symptoms in Ahvaz, Iran. Int. J. Med. Lab. 2018, 5, 11–18. [Google Scholar]
- Dalvand, N.; Dalvand, A.; Sharifi, Z.; Hosseini, S.M. Prevalence of hepatitis E virus in thalassemia patients with hepatitis C in Tehran, Iran. Iran. J. Microbiol. 2019, 11, 535. [Google Scholar] [CrossRef]
- Behzadi, M.A.; Leyva-Grado, V.H.; Namayandeh, M.; Ziyaeyan, A.; Feyznezhad, R.; Dorzaban, H.; Jamalidoust, M.; Ziyaeyan, M. Seroprevalence of viral hepatitis A, B, C, D and E viruses in the Hormozgan province southern Iran. BMC Infect. Dis. 2019, 19, 1027. [Google Scholar] [CrossRef]
- Abdelmawla, D.; Moemen, D.; Darwish, A.; Mowafy, W. Hepatitis E virus prevalence in Egyptian children with transfusion-dependent thalassemia. Braz. J. Infect. Dis. 2019, 23, 40–44. [Google Scholar] [CrossRef]
- Ismail, M.B.; Al Kassaa, I.; El Safadi, D.; Al Omari, S.; Mallat, H.; Dabboussi, F.; Hamze, M. Prevalence of anti-hepatitis E virus IgG antibodies in sera from hemodialysis patients in Tripoli, Lebanon. PLoS ONE 2020, 15, e0233256. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.M.A.; Temerk, H.A.; Galal, H.R.; Bazeed, S.E.S.; Sultan, S. The seropervelance of infectious hepatitis viruses (HBV, HCV and HEV) among blood donors and their correlation to risk factors in Qena governorate, Upper Egypt. Virusdisease 2020, 31, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Ouji, M.; Taherkhani, R.; Farshadpour, F. High prevalence of hepatitis E among regular hemodialysis patients in South of Iran. Int. J. Artif. Organs 2021, 44, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, F.; Golchob, Z.; Javadian, M.; Barary, M.; Sabbagh, P.; Ebrahimpour, S.; Bayani, M. Seroprevalence of hepatitis A and hepatitis E viruses among pregnant women in Northern Iran. Infect. Dis. Obstet. Gynecol. 2021, 2021, 5130586. [Google Scholar] [CrossRef] [PubMed]
- Al Dossary, R.A.; Alnafie, A.N.; Aljaroodi, S.A.; Rahman, J.U.; Hunasemarada, B.C.; Alkharsah, K.R. Prevalence of Hepatitis E Virus Infection Among Blood Donors in the Eastern Province of Saudi Arabia. J. Multidiscip. Healthc. 2021, 14, 2381. [Google Scholar] [CrossRef]
- Sayed, I.M.; El-Mokhtar, M.A.; Mahmoud, M.A.R.; Elkhawaga, A.A.; Gaber, S.; Seddek, N.H.; Abdel-Wahid, L.; Ashmawy, A.M.; Alkareemy, E.A.R. Clinical outcomes and prevalence of Hepatitis E Virus (HEV) among non-AC hepatitis patients in egypt. Infect. Drug Resist. 2021, 14, 59. [Google Scholar] [CrossRef]
- Al Absi, E.S.; Al-Sadeq, D.W.; Khalili, M.; Younes, N.; Al-Dewik, N.; Abdelghany, S.K.; Abouzid, S.S.; Al Thani, A.A.; Yassine, H.M.; Coyle, P.V. The prevalence of HEV among non-AC hepatitis in Qatar and efficiency of serological markers for the diagnosis of hepatitis E. BMC Gastroenterol. 2021, 21, 266. [Google Scholar] [CrossRef]
- Dumaidi, K.; Abudamous, A.M.; Abu-Helu, R.; Al-Jawabreh, H.; Dumaidi, Y.; Al-Jawabreh, A. First Report of the HEV Seroprevalence and the Risk Factor Assessment in the West Bank, Palestine, during the Period of 2015–2017. Can. J. Infect. Dis. Med. Microbiol. 2022, 2022, 4935811. [Google Scholar] [CrossRef]
- Öğüt, S.; Sayıner, A.A.; Otlu, B.; Bozdayı, G.; Zeytinoğlu, A.; Aksaray, S.; Çolak, D.; Gökahmetoğlu, S.; Aysın, M. Hepatitis E Infection in Solid Organ Transplant Recipients in Turkey. Turk. J. Gastroenterol. Off. J. Turk. Soc. Gastroenterol. 2022, 33, 68–73. [Google Scholar] [CrossRef]
- Farshadpour, F.; Taherkhani, S.; Taherkhani, R. Hepatitis E virus infection during pregnancy: The overlooked cause of maternal and fetal mortality. Infect. Disord. Drug Targets 2019, 19, 334–336. [Google Scholar] [CrossRef]
- Ahmad, T.; Hui, J.; Musa, T.H.; Behzadifar, M.; Baig, M. Seroprevalence of hepatitis E virus infection in pregnant women: A systematic review and meta-analysis. Ann. Saudi Med. 2020, 40, 136–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.-H.; Nelson, K.E.; Panzner, U.; Kasture, Y.; Labrique, A.B.; Wierzba, T.F. A systematic review of the epidemiology of hepatitis E virus in Africa. BMC Infect. Dis. 2014, 14, 308. [Google Scholar] [CrossRef] [PubMed]
- Hartl, J.; Otto, B.; Madden, R.G.; Webb, G.; Woolson, K.L.; Kriston, L.; Vettorazzi, E.; Lohse, A.W.; Dalton, H.R.; Pischke, S. Hepatitis E seroprevalence in Europe: A meta-analysis. Viruses 2016, 8, 211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tengan, F.M.; Figueiredo, G.M.; Nunes, A.K.; Manchiero, C.; Dantas, B.P.; Magri, M.C.; Prata, T.V.; Nascimento, M.; Mazza, C.C.; Abdala, E. Seroprevalence of hepatitis E in adults in Brazil: A systematic review and meta-analysis. Infect. Dis. Poverty 2019, 8, 3. [Google Scholar] [CrossRef]
- Petrović, T.; Lupulović, D.; de Oya, N.J.; Vojvodić, S.; Blázquez, A.-B.; Escribano-Romero, E.; Martín-Acebes, M.A.; Potkonjak, A.; Milošević, V.; Lazić, S. Prevalence of hepatitis E virus (HEV) antibodies in Serbian blood donors. J. Infect. Dev. Ctries. 2014, 8, 1322–1327. [Google Scholar] [CrossRef] [Green Version]
- Alvarado-Esquivel, C.; Sánchez-Anguiano, L.F.; Hernández-Tinoco, J. Hepatitis E virus exposure in pregnant women in rural Durango, Mexico. Ann. Hepatol. 2015, 13, 510–517. [Google Scholar] [CrossRef]
- Khaskheli, M.-N.; Baloch, S.; Sheeba, A.; Baloch, S. Hepatitis E–A preventable health issue–Endangering pregnant women’s life and foetal outcomes. J. Pak. Med. Assoc. 2015, 65, 655–659. [Google Scholar]
- Elduma, A.H.; Osman, W.M. Dengue and hepatitis E virus infection in pregnant women in Eastern Sudan, a challenge for diagnosis in an endemic area. Pan Afr. Med. J. 2014, 19, 391. [Google Scholar] [CrossRef]
- Stoszek, S.K.; Engle, R.E.; Abdel-Hamid, M.; Mikhail, N.; Abdel-Aziz, F.; Medhat, A.; Fix, A.D.; Emerson, S.U.; Purcell, R.H.; Strickland, G.T. Hepatitis E antibody seroconversion without disease in highly endemic rural Egyptian communities. Trans. R. Soc. Trop. Med. Hyg. 2006, 100, 89–94. [Google Scholar] [CrossRef]
- Shata, M.T.; Daef, E.A.; Zaki, M.E.; Abdelwahab, S.F.; Marzuuk, N.M.; Sobhy, M.; Rafaat, M.; Abdelbaki, L.; Nafeh, M.A.; Hashem, M. Protective role of humoral immune responses during an outbreak of hepatitis E in Egypt. Trans. R. Soc. Trop. Med. Hyg. 2012, 106, 613–618. [Google Scholar] [CrossRef]
- Hartl, J.; Wehmeyer, M.H.; Pischke, S. Acute hepatitis E: Two sides of the same coin. Viruses 2016, 8, 299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krain, L.J.; Atwell, J.E.; Nelson, K.E.; Labrique, A.B. Fetal and neonatal health consequences of vertically transmitted hepatitis E virus infection. Am. J. Trop. Med. Hyg. 2014, 90, 365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First-Author Name | Publication Year | Study Sample | Study Country | Sampling Year | Study Population | Type of Study | Participant Age (Range) | Study City | Male (%) | Female (%) | Prevalence (%) | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Thomas David | 1993 | 1350 | Turkey | 1990–1992 | General population | Cross-sectional | 18–65 years | Istanbul, Ayvalik, Aydin, Trabzon region, and Adana | 50.2 | 49.8 | 5·9 | [20] |
| Abraham Koshy | 1994 | 57 | Kuwait | 1992 | Acute viral hepatitis patients | Cross-sectional | 19–46 years | Kuwait | 88 | 12 | 4 | [21] |
| Asher Barzilai | 1995 | 188 | Israel | NM | Hemophiliac patients | Cross-sectional | 2–75 years | Tel Aviv | 98.9 | 1.1 | 9 | [22] |
| Yuory Karetny | 1995 | 1416 | Israel | 1988–1993 | General population | Cross-sectional | 1–66 years | West Bank and central region of Israel | NM | NM | 2.6 | [23] |
| Abdelaal Zawawi | 1998 | 593 | Saudi Arabia | 1995 | Male blood donors | Cross-sectional | 15–60 years | Jeddah | 100 | 0 | 16.9 | [24] |
| SI Abdel Hady | 1998 | 95 | Egypt | NM | Blood donors | Cross-sectional | NM | NM | NM | NM | 45.2 | [25] |
| SI Abdel Hady | 1998 | 96 | Egypt | NM | Hemodialysis patients | Cross-sectional | NM | NM | NM | NM | 39.6 | [25] |
| Al-Azmeh J | 1999 | 193 | Syria | 1995–1998 | Acute hepatitis patients | Hospital-based | 12–70 years | Damascus | 52.4 | 47.6 | 31.9 | [26] |
| Sıdal M | 2001 | 909 | Turkey | 1997–1998 | Children | Cross-sectional | Six months–15 years | Istanbul | NM | NM | 2.1 | [27] |
| Colak D | 2002 | 338 | Turkey | 1996–1997 | Pediatric age groups | Cross-sectional | 1–11 years | Antalya | NM | NM | 0.89 | [28] |
| Cesur Salih | 2002 | 1046 | Turkey | 2000–2001 | Adults | Cross-sectional | 15–75 years | Ankara | NM | NM | 3.8 | [29] |
| Arif Serhan Cevrioglu | 2004 | 76 | Turkey | 2000–2002 | Pregnant women | Cross-sectional | 19–42 years | Afyon | 0 | 100 | 12.6 | [30] |
| Irfan Sencan | 2004 | 383 | Turkey | 1999 | Children | Cross-sectional | 2–15 years | Du¨zce | 51.7 | 48.3 | 4.7 | [31] |
| Atabek Emre | 2004 | 210 | Turkey | 2001–2002 | Children | Cross-sectional | 1–18 years | Konya | 49 | 51 | 5.5 | [32] |
| Aminiafshar S | 2004 | 90 | Iran | 2003–2004 | Blood donors | Cross-sectional | 40–49 years | Tehran | 80.2 | 19.8 | 7.8 | [33] |
| Irfan Sencan | 2004 | 93 | Turkey | 1999 | Children | Cross-sectional | 2–15 years | Golyaka | 37.6 | 62.4 | 17.2 | [31] |
| Serkan Oncu | 2005 | 386 | Turkey | NM | Pregnant women | Cross-sectional | 18–32 years | Aydin | 0 | 100 | 7 | [34] |
| Alaa A Aboulata | 2005 | 100 | Egypt | 2004–2005 | Children presenting with minor hepatic disorders | Cross-sectional | 1–10 years | Cairo | NM | NM | 26 | [35] |
| Mahnaz Taremi | 2005 | 324 | Iran | 2004 | Hemodialysis patients | Cross-sectional | 18–80 years | Tabriz | 59 | 41 | 7.4 | [36] |
| Sonia Stoszek | 2006 | 2428 | Egypt | 1997–2003 | Pregnant women | Cross-sectional | 18–40 years | Nile Delta | NM | NM | 84.3 | [37] |
| M. Taremi | 2007 | 399 | Iran | 2004 | Male blood donors | Cross-sectional | 20–60 years | Tabriz | 100 | 0 | 7.8 | [38] |
| Gholam Ali Ghorbani | 2007 | 800 | Iran | 2006 | Soldiers | Cross-sectional | 17–23 years | Tehran | 100 | 0 | 1.1 | [39] |
| Seyed Mohammad Alavi | 2008 | 224 | Iran | 2005–2006 | Drug addicts | Cross-sectional | 18–54 years | Ahvaz | 100 | 0 | 13.5 | [40] |
| Mohammad Ali Assarehzadegan | 2008 | 400 | Iran | 2005 | Blood donors | Cross-sectional | 18–60 years | Khuzestan | 65 | 35 | 11.5 | [41] |
| M. Taremi | 2008 | 1824 | Iran | 2003 | General population | Cross-sectional | 6–80 years | Nahavand | NM | NM | 9.3 | [42] |
| Uçar Edip | 2009 | 92 | Turkey | NM | Hemodialysis patients | Cross-sectional | 22–71 years | Hatay | 58.7 | 41.3 | 20.6 | [43] |
| Shamsizadeh Ahmad | 2009 | 566 | Iran | 2006–2007 | Children | Cross-sectional | 6–15 years | Southwestern Iran | 45.4 | 54.6 | 8.5 | [44] |
| Behrooz Ataei | 2009 | 816 | Iran | 2005 | General population | Cross-sectional | 6–60 years | Isfahan | 47.5 | 52.5 | 3.8 | [45] |
| Pourahmad Morteza | 2009 | 43 | Iran | 2007 | Hemodialysis patients | Cross-sectional | NM | Jahrom | 67.4 | 32.6 | 7 | [46] |
| Maral I | 2010 | 515 | Turkey | 2003–2005 | Primary school children | Cross-sectional | 6–13 years | Ankara | 52.7 | 47.3 | 1.9 | [47] |
| Amen Ahmed Bawazir | 2010 | 538 | Yemen | 2005 | General population | Cross-sectional | one month–79 years | Aden | 52 | 48 | 16 | [48] |
| Rachana Kumar | 2010 | 469 | United Arab Emirates | NM | Pregnant women | Cohort | NM | Al Ain | 0 | 100 | 20 | [49] |
| SG Sepanlou | 2010 | 1423 | Iran | 2009 | General population | Cross-sectional | NM | Tehran and Golestan | NM | NM | 7.4 | [50] |
| Turky Ataallah | 2011 | 9610 | Iraq | 2005–2006 | Acute viral hepatitis | Cross-sectional | 1–60 years | Baghdad | 49.5 | 50.5 | 19.4 | [51] |
| Turky Ataallah | 2011 | 6972 | Iraq | 2005–2006 | General population | Cross-sectional | 1–60 years | Baghdad | 48.8 | 51.2 | 20.3 | [51] |
| Zakieh Rostamzadeh Khameneh | 2011 | 91 | Iran | NM | Renal transplant recipients | Cross-sectional | 6–65 years | Urmia | 67 | 33 | 30.8 | [52] |
| Seyed Reza Mohebbi | 2012 | 551 | Iran | 2006–2007 | General population | Cross-sectional | 1–83 years | Tehran | 36.3 | 63.7 | 9.4 | [53] |
| Seyed Reza Mohebbi | 2012 | 551 | Iran | 2006–2007 | General population | Cross-sectional | 1–83 years | Tehran | 50 | 50 | 9.3 | [53] |
| Abdolreza Sotoodeh Jahromi | 2013 | 477 | Iran | 2009 | Blood donors | Cross-sectional | 17–59 years | Jahrom | 447 | 30 | 5.4 | [54] |
| Sanaz Ahmadi Ghezeldasht | 2013 | 1582 | Iran | 2012 | General population | Cross-sectional | 1–90 years | Mashhad | 45.4 | 54.6 | 14.2 | [55] |
| Nural Cevahir | 2013 | 185 | Turkey | NM | Primary school children | Cross-sectional | 7–14 years | Denizli | 50.3 | 49.7 | 12.4 | [56] |
| Hassan Ehteram | 2013 | 530 | Iran | 2012 | Blood donors | Cross-sectional | 31–50 years | Central province | 91.9 | 8.1 | 14.3 | [57] |
| Omid Zekavat | 2013 | 80 | Iran | 2010 | Patients with chronic maintenance hemodialysis | Cross-sectional | 26–80 years | Southwestern Iran | 63.7 | 63.3 | 6.3 | [58] |
| A.R. Mobaien | 2013 | 93 | Iran | 2011 | Hemodialysis patients | Cross-sectional | 16–88 years | Tehran | 52.7 | 47.3 | 26.9 | [59] |
| Ayman Khalid Johargy | 2013 | 900 | Saudi Arabia | 2009 | Male blood donors | Cross-sectional | 18–66 years | Makkah | 100 | 0 | 18.7 | [60] |
| Nawal Utba | 2013 | 270 | Iraq | NM | Blood donors and cleaning workers | Cross-sectional | 18–60 years | Baghdad | 67 | 33 | 21.5 | [61] |
| Amitis Ramezani | 2013 | 100 | Iran | 2012 | HIV-positive individuals | Cross-sectional | 34–43 years | Tehran | 71 | 29 | 10 | [62] |
| Fariba Keramat | 2014 | 131 | Iran | 2011–2012 | Injection drug users | Cross-sectional | 22–70 years | Hamadan | 99.2 | 0.8 | 6.1 | [63] |
| Fariba Keramat | 2014 | 131 | Iran | 2011–2012 | Non-injection drug users | Cross-sectional | 20–45 years | Hamadan | 99.2 | 0.8 | 1.5 | [63] |
| Seyed Seifollah Beladi Mousavi | 2014 | 47 | Iran | NM | Hemodialysis patients | Cross-sectional | 20–80 years | Ahvaz | 57.4 | 42.6 | 10.6 | [64] |
| Peyman Eini | 2015 | 153 | Iran | 2010 | Hemodialysis patients | Cross-sectional | 10–70 years | Hamadan | 54.2 | 45.8 | 19.2 | [65] |
| Orna Mor | 2015 | 729 | Israel | 2009–2010 | General population | Cross-sectional | 10–75 years | Tel-Aviv | 54 | 46 | 10.6 | [66] |
| Mojgan Mamani | 2015 | 1050 | Iran | 2010–2012 | Pregnant women | Prospective cross-sectional | 14–49 years | Hamadan | 0 | 100 | 7.4 | [67] |
| Seyed Moayed Alavian | 2015 | 274 | Iran | 2012 | Hemodialysis patients | Cross-sectional | 21–80 years | Isfahan | 52.9 | 47.1 | 9.9 | [68] |
| Hassan Joulaei | 2015 | 158 | Iran | 2012–2013 | HIV-positive individuals | Cross-sectional | 1–60 years | Shiraz | 76.9 | 23.1 | 16.4 | [69] |
| Behrouz Naeimi | 2015 | 628 | Iran | 2013 | Blood donors | Cross-sectional | 19–65 years | Bushehr | 95.2 | 4.8 | 16.7 | [70] |
| Daniela Ram | 2016 | 49 | Israel | 2013–2015 | Acute hepatitis patients | Cross-sectional | NM | Haifa, Tel Aviv, Beer Sheva | NM | NM | 6.1 | [71] |
| Hossein Keyvani | 2016 | 200 | Iran | NM | Blood donors | Cross-sectional | 20–61 years | Tehran | 58.2 | 41.8 | 4.5 | [72] |
| Hossein Keyvani | 2016 | 100 | Iran | NM | Patients with hepatitis C | Cross-sectional | 20–61 years | Tehran | 58.2 | 41.8 | 7 | [72] |
| Hossein Keyvani | 2016 | 150 | Iran | NM | Patients with hepatitis B | Cross-sectional | 20–61 years | Tehran | 58.2 | 41.8 | 11.3 | [72] |
| Hajiahmadi Nazila | 2016 | 149 | Iran | NM | Hemodialysis patients | Cross-sectional | 15–90 years | Golestan | 49 | 51 | 4 | [73] |
| Hajiahmadi Nazila | 2016 | 102 | Iran | NM | HIV-infected patients | Cross-sectional | 17–54 years | Golestan | 68.6 | 31.4 | 33.3 | [73] |
| Khashayar Hesamizadeh | 2016 | 559 | Iran | 2014 | Blood donors | Cross-sectional | 18–37 years | Tehran | 95.9 | 4.1 | 8.1 | [74] |
| Zohreh Azarkar | 2016 | 340 | Iran | 2013–2014 | Blood donors | Cross-sectional | 20–40 years | Birjand | 93.8 | 2.2 | 14.7 | [75] |
| Gamal Hasan | 2016 | 123 | Egypt | 2007–2008 | Children | Multicenter prospective | 2–18 years | Assiut | 59.3 | 40.7 | 26.8 | [76] |
| Gülsüm İclal Bayhan | 2016 | 408 | Turkey | 2014 | Children | Cross-sectional | 2 months-18 years | Van | 43.9 | 56.1 | 4.2 | [77] |
| Gheyath Nasrallah | 2017 | 5854 | Qatar | 2013–2016 | Blood donors | Cross-sectional | 15–80 years | Al Doha | 97.4 | 2.6 | 20.7 | [78] |
| Mohammad Obaidata | 2018 | 450 | Jordan | 2015–2016 | Patients who visit healthcare clinics for routine care | Cross-sectional | 20–80 years | Eight governorates | 45.1 | 54.9 | 30.9 | [79] |
| Fatemeh Farshadpour | 2018 | 1331 | Iran | 2016–2017 | Pregnant women | Cross-sectional | 14–45 years | Bushehr | 0 | 100 | 6.3 | [80] |
| Mehdi Parsa Nahad | 2018 | 241 | Iran | 2013–2016 | Acute viral hepatitis patients | Cross-sectional | 10–80 years | Ahvaz | 51.9 | 48.1 | 27.4 | [81] |
| Najmeh Dalvand | 2019 | 120 | Iran | 2019 | Thalassemia-positive patients | Cross-sectional | 17–45 years | Tehran | 35 | 65 | 1.67 | [82] |
| Mohammad Amin Behzadi | 2019 | 562 | Iran | 2016–2017 | Healthy individuals | Cross-sectional | 1–86 years | Hormozgan | 29.2 | 70.8 | 15.8 | [83] |
| Doaa Abdelmawla | 2019 | 140 | Egypt | 2016 | Children with transfusion-dependent thalassemia | Cross-sectional | 2–6 years | Mansoura | 47.1 | 52.9 | 27.15 | [84] |
| Mohamad Bachar Ismail | 2020 | 171 | Lebanon | 2016 | Hemodialysis patients | Cross-sectional | 23–82 years | Tripoli | 43.8 | 56.2 | 21.63 | [85] |
| Azza Masoud Abdelbaky Ahmed | 2020 | 11,604 | Egypt | 2013–2014 | Blood donors | Cross-sectional | 18–60 years | Qena | 88.2 | 11.8 | 28.8 | [86] |
| Mahbube Ouji | 2021 | 226 | Iran | NM | Hemodialysis patients | Cross-sectional | 23–87 years | Bushehr, Borazjan, and Genaveh | 56.2 | 43.8 | 68.6 | [87] |
| Farzin Sadeghi | 2021 | 247 | Iran | 2020 | Pregnant women | Cross-sectional | 17–42 years | Northern Iran | 0 | 100 | 0.8 | [88] |
| Reem A Al Dossary | 2021 | 806 | Saudi Arabia | 2020 | Blood donors | Cross-sectional | 18–85 years | Eastern province | 94.9 | 5.1 | 3.2 | [89] |
| Sayed El-Mokhtar | 2021 | 300 | Egypt | 2016–2018 | Non-A-C hepatitis patients | Cross-sectional | 40–60 years | Assiut | 53 | 47 | 10 | [90] |
| Enas Al Absi | 2021 | 259 | Qatar | 2017–2019 | Non-A-C hepatitis patients | Cross-sectional | 6–98 years | Al Doha | 61.4 | 83.6 | 32.1 | [91] |
| Kamal Dumaidi | 2022 | 432 | Palestine | 2015–2017 | General population | Cross-sectional | 1–86 years | West Bank and Jerusalem | 49.3 | 50.7 | 3.7 | [92] |
| Seval Öğüt | 2022 | 485 | Turkey | NM | Solid organ recipients | Cross-sectional | 1–80 years | Izmir | 64.7 | 35.3 | 17.3 | [93] |
| Model | Effect Size and 95% Confidence Interval | Test of Null (2-Tail) | Heterogeneity | Tau-Squared | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model | Number of Studies | Point of Estimate | Lower Limit | Upper Limit | Z-Value | p-Value | Q-Value | df (Q) | p-Value | I Squared | Tau Squared | Standard Error | Variance | Tau |
| Fixed | 80 | 0.213 | 0.216 | 0.293 | −124.850 | 0.000 | 6154.911 | 79 | 0.000 | 98.733 | 0.763 | 0.372 | 0.138 | 0.874 |
| Random | 80 | 0.118 | 0.141 | 0.253 | −19.651 | 0.000 | ||||||||
| Kendall’s S Statistic (P-Q) | 6154.911 |
| Kendall’s tau without continuity correction | |
| Tau | 0.7633 |
| z-value for tau | −124.850 |
| p-value (1-tailed) | 0.001 |
| p-value (2-tailed) | 0.001 |
| Kendall’s tau with continuity correction | |
| Tau | 0.8737 |
| z-value for tau | −19.65 |
| p-value (1-tailed) | 0.001 |
| p-value (2-tailed) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qashqari, F.S. Seroprevalence of Hepatitis E Virus Infection in Middle Eastern Countries: A Systematic Review and Meta-Analysis. Medicina 2022, 58, 905. https://doi.org/10.3390/medicina58070905
Qashqari FS. Seroprevalence of Hepatitis E Virus Infection in Middle Eastern Countries: A Systematic Review and Meta-Analysis. Medicina. 2022; 58(7):905. https://doi.org/10.3390/medicina58070905
Chicago/Turabian StyleQashqari, Fadi S. 2022. "Seroprevalence of Hepatitis E Virus Infection in Middle Eastern Countries: A Systematic Review and Meta-Analysis" Medicina 58, no. 7: 905. https://doi.org/10.3390/medicina58070905