
The Epidemiology of Entamoeba histolytica Infection and Its Associated Risk Factors among Domestic and Imported Patients in Taiwan during the 2011–2020 Period

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Policy
2.2. Data Source
2.3. Case Definition
2.4. Laboratory Examination
2.5. Surveillance of Environmental Factors
2.6. Statistical Analysis
3. Results
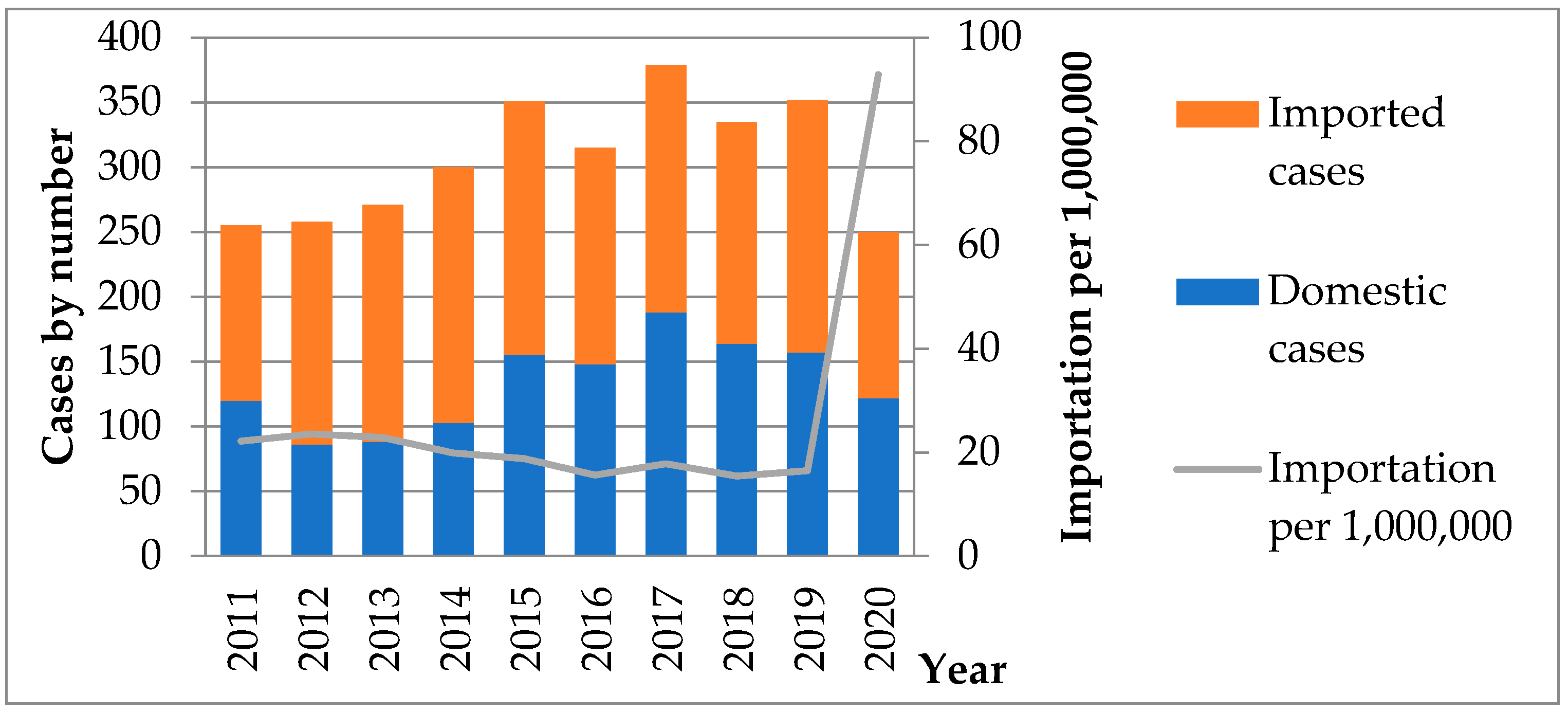
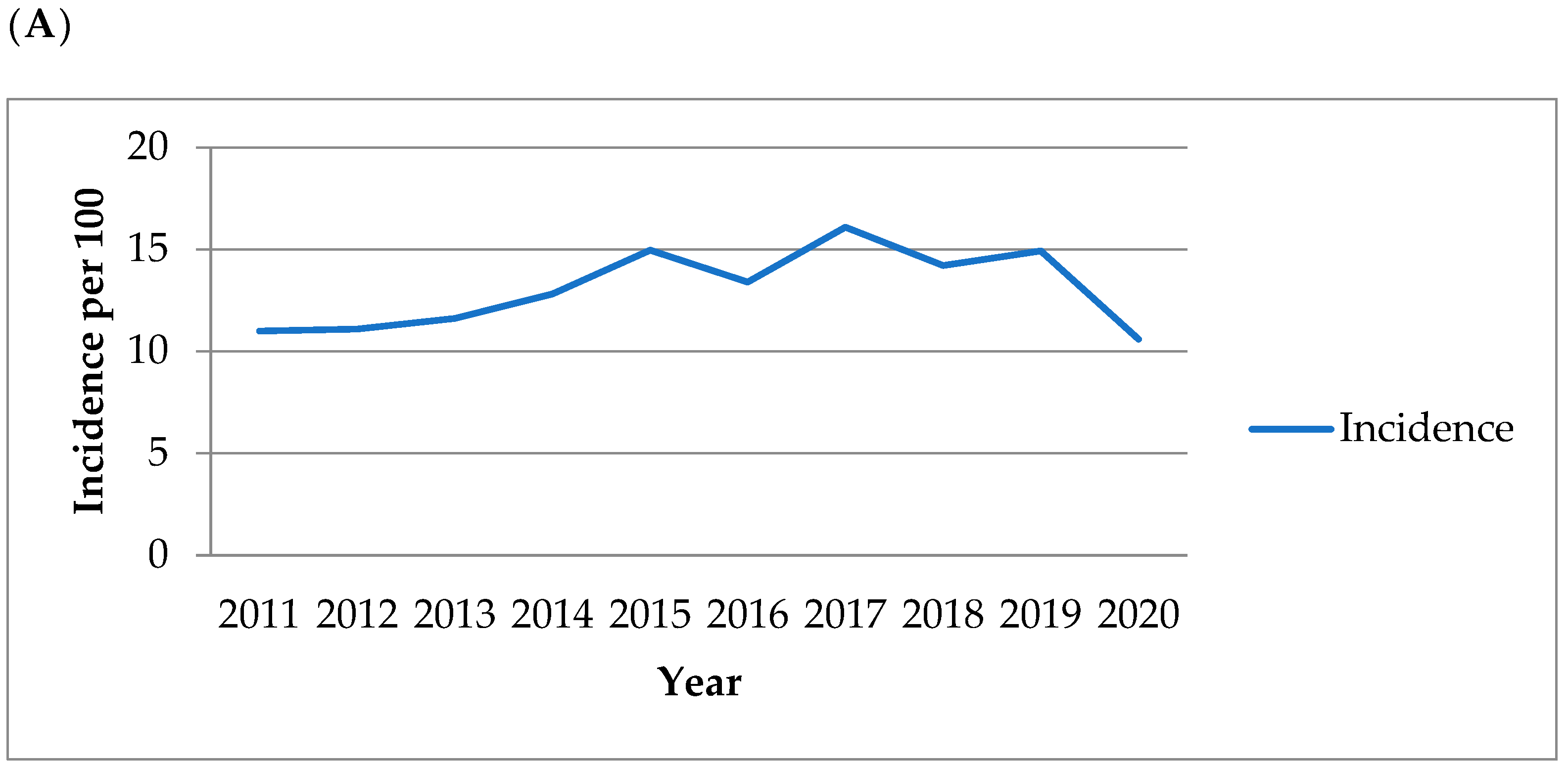
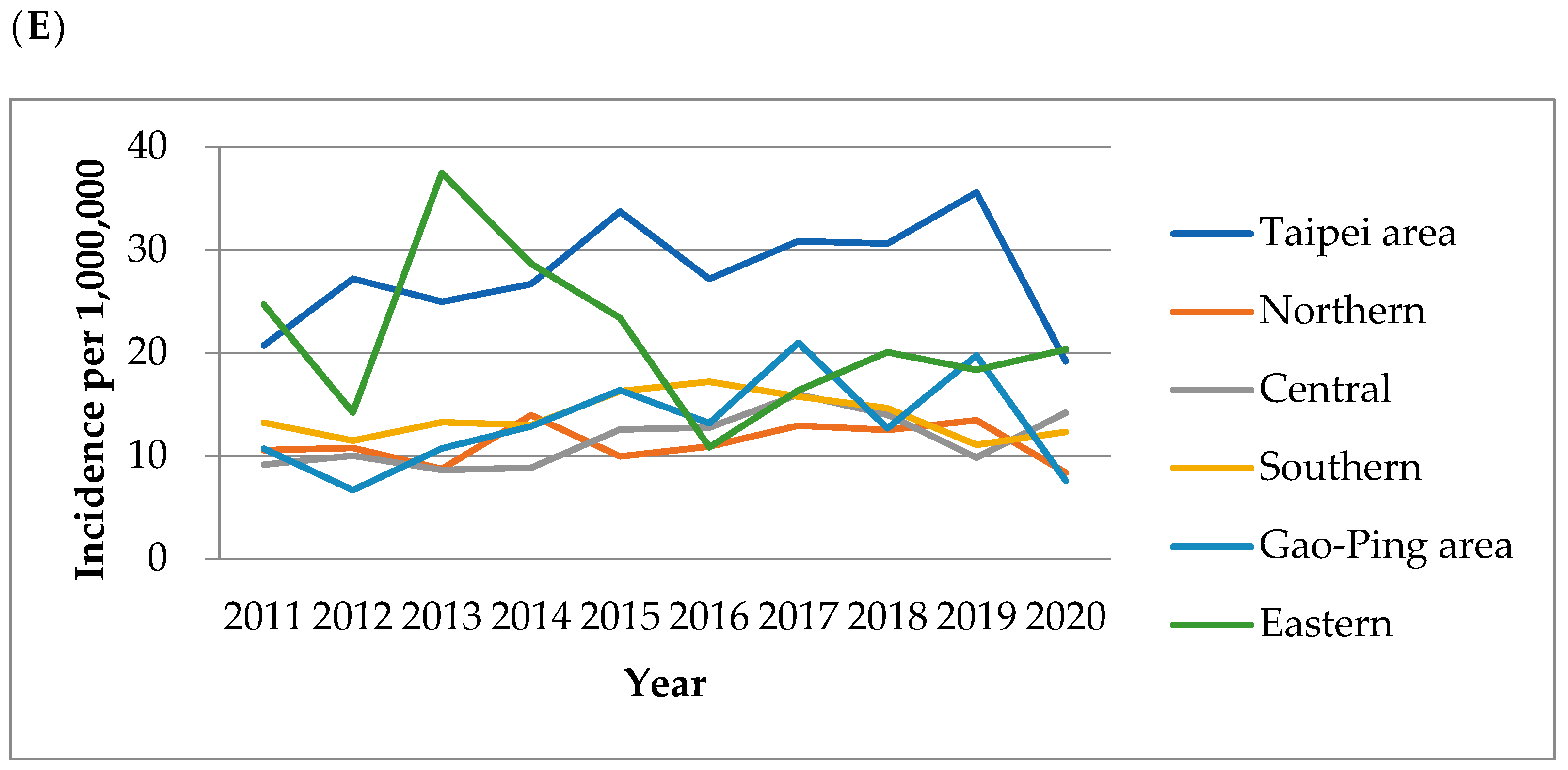
3.1. Surveillance
3.2. Outcome of Epidemiological Features
3.3. Outcome of Environmental Features
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Initiative for Vaccine Research: Parasitic Disease. Available online: http://www.who.into/vaccine_research/disease/sos_parasitic/en/index.html (accessed on 1 March 2022).
- Petri, W.A., Jr.; Ravdin, H.J. Entamoeba species, including amebiasis. In Principles and Practice of Infectious Diseases, 7th ed.; Bennett, J.E., Mandell, G.L., Dolin, R., Eds.; Churchill Livingstone Elsevier: Philadelphia, PA, USA, 2010; pp. 3411–3425. [Google Scholar]
- Kow-Tong, C.; Chien-Jen, C.; Chiu, J.-P. A school waterborne outbreak involving both Shigella sonnei and Entamoeba histolytica. J. Environ. Health 2001, 64, 9. [Google Scholar]
- Petri, W.A., Jr.; Singh, U. Diagnosis and management of amebiasis. Clin. Infect. Dis. 1999, 29, 1117–1125. [Google Scholar] [CrossRef] [PubMed]
- Allason-Jones, E.; Mindel, A.; Sargeaunt, P.; Williams, P. Entamoeba histolytica as a commensal intestinal parasite in homosexual men. N. Engl. J. Med. 1986, 315, 353–356. [Google Scholar] [CrossRef] [PubMed]
- Haque, R.; Huston, C.D.; Hughes, M.; Houpt, E.; Petri, W.A., Jr. Amebiasis. N. Engl. J. Med. 2003, 348, 1565–1573. [Google Scholar] [CrossRef] [PubMed]
- Nagata, N.; Shimbo, T.; Akiyama, J.; Nakashima, R.; Nishimura, S.; Yada, T.; Watanabe, K.; Oka, S.; Uemura, N. Risk factors for intestinal invasive amebiasis in Japan, 2003–2009. Emerg. Infect. Dis. 2012, 18, 717. [Google Scholar] [CrossRef]
- Ximénez, C.; Morán, P.; Rojas, L.; Valadez, A.; Gómez, A. Reassessment of the epidemiology of amebiasis: State of the art. Infect. Genet. Evol. 2009, 9, 1023–1032. [Google Scholar] [CrossRef]
- Schuster, F.L.; Visvesvara, G.S. Amebae and ciliated protozoa as causal agents of waterborne zoonotic disease. Vet. Parasitol. 2004, 126, 91–120. [Google Scholar] [CrossRef]
- Centers for Disease Control. Taiwan. Entamoeba Histolytica infection. Available online: https://www.cdc.gov.tw/Disease/SubIndex/r0w7-NmfmIEmsJIcqyBe6A (accessed on 1 March 2022).
- Lin, F.-H.; Chen, B.-C.; Chou, Y.-C.; Hsieh, C.-J.; Yu, C.-P. Incidence and Risk Factors for Notifiable Typhoid and Paratyphoid in Taiwan during the Period 2011–2020. Healthcare 2021, 9, 1316. [Google Scholar] [CrossRef]
- Lin, F.-H.; Chou, Y.-C.; Chen, B.-C.; Lu, J.-C.; Liu, C.-J.; Hsieh, C.-J.; Yu, C.-P. An Increased Risk of School-Aged Children with Viral Infection among Diarrhea Clusters in Taiwan during 2011–2019. Children 2021, 8, 807. [Google Scholar] [CrossRef]
- Lin, F.-H.; Chou, Y.-C.; Chien, W.-C.; Chung, C.-H.; Hsieh, C.-J.; Yu, C.-P. The Most Common Location of Schools with Viral Upper Respiratory Tract Infection Clusters in Taiwan, 2011–2019. Children 2022, 9, 720. [Google Scholar] [CrossRef]
- Centers for Disease Control. Taiwan. Notifiable Infectious Disease Statistical System. Available online: http://nidss.cdc.gov.tw (accessed on 1 March 2022).
- Tan, H.-F.; Yeh, C.-Y.; Chang, H.-W.; Chang, C.-K.; Tseng, H.-F. Private doctors’ practices, knowledge, and attitude to reporting of communicable diseases: A national survey in Taiwan. BMC Infect. Dis. 2009, 9, 11. [Google Scholar] [CrossRef] [Green Version]
- Taiwan Centers for Disease Control. Amebiasis Daisnosis. 2021. Available online: https://www.cdc.gov.tw/File/Get/b36EzUCvXZQqL3BLMx8gMw (accessed on 1 March 2022).
- Leung, P.-O.; Chen, K.-H.; Chen, K.-L.; Tsai, Y.-T.; Liu, S.-Y.; Chen, K.-T. Epidemiological features of intestinal infection with Entamoeba histolytica in Taiwan, 2002–2010. Travel Med. Infect. Dis. 2014, 12, 673–679. [Google Scholar] [CrossRef] [PubMed]
- Garcia, L.S. Diagnostic Medical Parasitology; ASM Press: Washington, DC, USA, 2001. [Google Scholar]
- Israeli, E.; Talis, B.; Peled, N.; Snier, R.; El-On, J. Anti-amoebic antibody activity in patients, determined with antigens prepared from virulent parasites (indirect hemagglutination assay and enzyme-linked immunosorbent assay). IMAJ-RAMAT GAN 2007, 9, 663. [Google Scholar]
- Haque, R.; Petri, W.A., Jr. Diagnosis of amebiasis in Bangladesh. Arch. Med. Res. 2006, 37, 272–275. [Google Scholar] [CrossRef] [PubMed]
- Blessmann, J.; Buss, H.; Nu, P.A.T.; Dinh, B.T.; Ngo, Q.T.V.; Van, A.L.; Alla, M.D.A.; Jackson, T.F.; Ravdin, J.I.; Tannich, E. Real-time PCR for detection and differentiation of Entamoeba histolytica and Entamoeba dispar in fecal samples. J. Clin. Microbiol. 2002, 40, 4413–4417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonin, P.; Trudel, L. Detection and differentiation of Entamoeba histolytica and Entamoeba dispar isolates in clinical samples by PCR and enzyme-linked immunosorbent assay. J. Clin. Microbiol. 2003, 41, 237–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Environmental Protection Administration. Air Pollution Statistics. 2022. Available online: https://www.epa.gov.tw/eng/2C04F91E41A2000B (accessed on 1 March 2022).
- Central Weather Bureau. Monthly Data. 2022. Available online: https://www.cwb.gov.tw/V8/C/C/Statistics/monthlydata.html (accessed on 1 March 2022).
- Gordis, L. The dynamics of disease transmission. In Epidemiology, 3rd ed.; Gordis, L., Ed.; Elsevier Inc.: Philadelphia, PA, USA, 2004. [Google Scholar]
- Stanley, S.L., Jr. Amoebiasis. Lancet 2003, 361, 1025–1034. [Google Scholar] [CrossRef]
- Hung, C.-C.; Deng, H.-Y.; Hsiao, W.-H.; Hsieh, S.-M.; Hsiao, C.-F.; Chen, M.-Y.; Chang, S.-C.; Su, K.-E. Invasive amebiasis as an emerging parasitic disease in patients with human immunodeficiency virus type 1 infection in Taiwan. Arch. Intern. Med. 2005, 165, 409–415. [Google Scholar] [CrossRef]
- Tengku, S.; Norhayati, M. Review Paper Public health and clinical importance of amoebiasis in Malaysia: A review. Trop. Biomed. 2011, 28, 194–222. [Google Scholar]
- Ximénez, C.; Cerritos, R.; Rojas, L.; Dolabella, S.; Morán, P.; Shibayama, M.; González, E.; Valadez, A.; Hernández, E.; Valenzuela, O. Human amebiasis: Breaking the paradigm? Int. J. Environ. Res. Public Health 2010, 7, 1105–1120. [Google Scholar] [CrossRef]
- World Tourism Organization. UNWTO Tourism Highlights. 2012 ed. Available online: http://mkt.unwto.org/en/publication/unwto-tourism-highlights-2012-edition (accessed on 1 March 2022).
- Steffen, R.; Rickenbach, M.; Wilhelm, U.; Helminger, A.; Schär, M. Health problems after travel to developing countries. J. Infect. Dis. 1987, 156, 84–91. [Google Scholar] [CrossRef] [Green Version]
- Harvey, K.; Esposito, D.H.; Han, P.; Kozarsky, P.; Freedman, D.O.; Plier, D.A.; Sotir, M.J. Surveillance for travel-related disease—GeoSentinel surveillance system, United States, 1997–2011. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2013, 62, 1–23. [Google Scholar]
- Diamond, L.S.; Clark, C.G. A Redescription of Entamoeba Histolytica Schaudinn, 1903 (Emended Walker, 1911) Separating it from Entamoeba Dispar Brumpt, 1925 1. J. Eukaryot. Microbiol. 1993, 40, 340–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herbinger, K.-H.; Fleischmann, E.; Weber, C.; Perona, P.; Löscher, T.; Bretzel, G. Epidemiological, clinical, and diagnostic data on intestinal infections with Entamoeba histolytica and Entamoeba dispar among returning travelers. Infection 2011, 39, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Foo, P.; Chan, Y.; See Too, W.C.; Tan, Z.N.; Wong, W.K.; Lalitha, P.; Lim, B.H. Development of a thermostabilized, one-step, nested, tetraplex PCR assay for simultaneous identification and differentiation of Entamoeba species, Entamoeba histolytica and Entamoeba dispar from stool samples. J. Med. Microbiol. 2012, 61, 1219–1225. [Google Scholar] [CrossRef] [Green Version]
- Ali, I.K.M.; Clark, C.G.; Petri, W.A., Jr. Molecular epidemiology of amebiasis. Infect. Genet. Evol. 2008, 8, 698–707. [Google Scholar] [CrossRef] [Green Version]
- Bracho Mora, Á.; Rivero de Rodríguez, Z.; Arraiz, N.; Villalobos, R.; Urdaneta, H. Detection of Entamoeba histolytica and Entamoeba dispar by PCR in children, less than five years of age with diarrhea, in Maracaibo, Venezuela: A preliminary study. Investig. Clínica 2013, 54, 373–381. [Google Scholar]
- Scheelbeek, P.F.; Dangour, A.D.; Jarmul, S.; Turner, G.; Sietsma, A.J.; Minx, J.C.; Callaghan, M.; Ajibade, I.; Austin, S.E.; Biesbroek, R. The effects on public health of climate change adaptation responses: A systematic review of evidence from low-and middle-income countries. Environ. Res. Lett. 2021, 16, 073001. [Google Scholar] [CrossRef]
- Duchenne-Moutien, R.A.; Neetoo, H. Climate Change and Emerging Food Safety Issues: A Review. J. Food Prot. 2021, 84, 1884–1897. [Google Scholar] [CrossRef]
- Zavala, G.A.; van Dulm, E.; Doak, C.M.; García, O.P.; Polman, K.; Campos-Ponce, M. Ascariasis, Amebiasis and Giardiasis in Mexican children: Distribution and geographical, environmental and socioeconomic risk factors. J. Parasit. Dis. 2020, 44, 829–836. [Google Scholar] [CrossRef]
- Doyle, T.J.; Glynn, M.K.; Groseclose, S.L. Completeness of notifiable infectious disease reporting in the United States: An analytical literature review. Am. J. Epidemiol. 2002, 155, 866–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Cases | Domestic Cases | Imported Cases | p | |||
|---|---|---|---|---|---|---|---|
| N = 3066, % | N = 1331, % | N = 1735, % | |||||
| Sex | |||||||
| Male | 1707 | 55.7 | 1085 | 81.5 | 622 | 35.9 | <0.001 |
| Female | 1359 | 44.3 | 246 | 18.5 | 1113 | 64.1 | |
| Age | |||||||
| <20 | 26 | 0.8 | 10 | 0.8 | 16 | 0.9 | <0.001 |
| 20–29 | 1075 | 35.1 | 283 | 21.3 | 792 | 45.6 | |
| 30–39 | 1185 | 38.6 | 450 | 33.8 | 735 | 42.4 | |
| 40–49 | 408 | 13.3 | 252 | 18.9 | 156 | 9.0 | |
| 50–59 | 186 | 6.1 | 164 | 12.3 | 22 | 1.3 | |
| ≥60 | 186 | 6.1 | 172 | 12.9 | 14 | 0.8 | |
| Season | |||||||
| Spring | 773 | 25.2 | 346 | 26.0 | 427 | 24.6 | 0.251 |
| Summer | 785 | 25.6 | 321 | 24.1 | 464 | 26.7 | |
| Fall | 808 | 26.4 | 345 | 25.9 | 463 | 26.7 | |
| Winter | 700 | 22.8 | 319 | 24.0 | 381 | 22.0 | |
| Residency | |||||||
| Taipei area | 1055 | 34.4 | 516 | 38.8 | 539 | 31.1 | <0.001 |
| Northern | 410 | 13.4 | 172 | 12.9 | 238 | 13.7 | |
| Central | 527 | 17.2 | 214 | 16.1 | 313 | 18.0 | |
| Southern | 466 | 15.2 | 157 | 11.8 | 309 | 17.8 | |
| Gao-Ping | 489 | 15.9 | 216 | 16.2 | 273 | 15.7 | |
| Eastern | 119 | 3.9 | 56 | 4.2 | 63 | 3.6 | |
| Variables | Year | p | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | ||
| Cases | |||||||||||
| Domestic | 120 | 86 | 88 | 103 | 155 | 148 | 188 | 164 | 157 | 122 | <0.001 |
| Imported | 135 | 172 | 183 | 197 | 196 | 167 | 191 | 171 | 195 | 128 | |
| Sex | |||||||||||
| Male | 151 | 112 | 139 | 155 | 187 | 175 | 239 | 197 | 194 | 158 | <0.001 |
| Female | 104 | 146 | 132 | 145 | 164 | 140 | 140 | 138 | 158 | 92 | |
| Age group | |||||||||||
| <20 | 1 | 3 | 4 | 2 | 2 | 2 | 1 | 0 | 7 | 4 | 0.003 |
| 20–29 | 101 | 86 | 107 | 100 | 136 | 124 | 112 | 114 | 120 | 75 | |
| 30–39 | 84 | 105 | 100 | 127 | 130 | 127 | 145 | 134 | 127 | 106 | |
| 40–49 | 30 | 27 | 44 | 44 | 45 | 33 | 57 | 50 | 46 | 32 | |
| 50–59 | 17 | 20 | 9 | 17 | 19 | 11 | 37 | 19 | 25 | 12 | |
| ≥60 | 22 | 17 | 7 | 10 | 19 | 18 | 27 | 18 | 27 | 21 | |
| Season | |||||||||||
| Spring | 69 | 67 | 70 | 66 | 94 | 72 | 92 | 87 | 91 | 65 | 0.467 |
| Summer | 53 | 73 | 84 | 76 | 91 | 93 | 100 | 78 | 78 | 59 | |
| Fall | 72 | 62 | 61 | 93 | 85 | 82 | 90 | 102 | 94 | 67 | |
| Winter | 61 | 56 | 56 | 65 | 81 | 68 | 97 | 68 | 89 | 59 | |
| Residency | |||||||||||
| Taipei area | 78 | 103 | 95 | 102 | 129 | 104 | 118 | 117 | 136 | 73 | <0.001 |
| Northern area | 37 | 38 | 31 | 50 | 36 | 40 | 48 | 47 | 51 | 32 | |
| Central area | 41 | 45 | 39 | 40 | 57 | 58 | 73 | 64 | 45 | 65 | |
| Southern area | 45 | 39 | 45 | 44 | 55 | 58 | 53 | 49 | 37 | 41 | |
| Kao-Ping area | 40 | 25 | 40 | 48 | 61 | 49 | 78 | 47 | 73 | 28 | |
| Eastern area | 14 | 8 | 21 | 16 | 13 | 6 | 9 | 11 | 10 | 11 | |
| Variables | Season | p | |||
|---|---|---|---|---|---|
| Spring | Summer | Fall | Winter | ||
| Sex | |||||
| Male | 441 | 423 | 442 | 401 | 0.448 |
| Female | 332 | 362 | 366 | 299 | |
| Age group | |||||
| <20 | 5 | 4 | 9 | 8 | 0.737 |
| 20–29 | 285 | 274 | 282 | 234 | |
| 30–39 | 298 | 297 | 315 | 275 | |
| 40–49 | 89 | 110 | 108 | 101 | |
| 50–59 | 43 | 55 | 51 | 37 | |
| ≥60 | 53 | 45 | 43 | 45 | |
| Residency | |||||
| Taipei area | 257 | 271 | 270 | 257 | 0.163 |
| Northern | 98 | 109 | 119 | 84 | |
| Central | 129 | 137 | 136 | 125 | |
| Southern | 148 | 99 | 117 | 102 | |
| Kao-Ping | 112 | 138 | 136 | 103 | |
| Eastern | 29 | 31 | 30 | 29 | |
| Variables | Region of Residence | p | |||||
|---|---|---|---|---|---|---|---|
| Taipei Area | Northern Area | Central Area | Southern Area | Kao-Ping Area | Eastern Area | ||
| Sex | |||||||
| Male | 569 | 215 | 322 | 225 | 310 | 66 | <0.001 |
| Female | 486 | 195 | 205 | 241 | 179 | 53 | |
| Age group | |||||||
| <20 | 6 | 3 | 8 | 3 | 4 | 2 | <0.001 |
| 20–29 | 316 | 168 | 203 | 195 | 164 | 29 | |
| 30–39 | 416 | 165 | 220 | 170 | 171 | 43 | |
| 40–49 | 181 | 47 | 46 | 33 | 82 | 19 | |
| 50–59 | 75 | 14 | 21 | 29 | 37 | 10 | |
| ≥60 | 61 | 13 | 29 | 36 | 31 | 16 | |
| Variables | Sex | p | |
|---|---|---|---|
| Male | Female | ||
| Age group | |||
| <20 | 19 | 7 | <0.001 |
| 20–29 | 532 | 543 a | |
| 30–39 | 595 | 590 b | |
| 40–49 | 266 c | 142 | |
| 50–59 | 162 d | 24 | |
| ≥60 | 133 e | 53 | |
| Country | Year | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | |
| Asia (N = 1716) | ||||||||||
| China | 7 | 5 | 6 | 3 | 4 | 3 | 2 | 4 | 6 | |
| Korea | 1 | 1 | 1 | |||||||
| Japan | 1 | 1 | 2 | 1 | ||||||
| Philippines | 8 | 19 | 12 | 22 | 20 | 17 | 30 | 18 | 24 | 13 |
| Indonesia | 106 | 141 | 153 | 164 | 159 | 127 | 148 | 122 | 155 | 110 |
| Vietnam | 6 | 2 | 5 | 3 | 6 | 6 | 4 | 13 | 4 | 2 |
| Myanmar | 1 | 1 | 1 | 1 | 1 | |||||
| Cambodia | 1 | 2 | 1 | 1 | ||||||
| Malaysia | 1 | 1 | ||||||||
| Thailand | 3 | 3 | 4 | 1 | 2 | 4 | 3 | 4 | 1 | |
| Maldives | 1 | |||||||||
| India | 2 | 2 | 4 | 1 | 1 | 1 | ||||
| Oceania (N = 5) | ||||||||||
| Australia | 1 | 1 | ||||||||
| Giribas | 1 | |||||||||
| Tuvalu | 2 | |||||||||
| America (N = 3) | ||||||||||
| USA | 1 | |||||||||
| Panama | 1 | |||||||||
| Colombia | 1 | |||||||||
| Europe (N = 2) | ||||||||||
| U. K. | 1 | |||||||||
| France | 1 | |||||||||
| Miss. Data (N = 9) | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 4 | 0 | 0 |
| Country of Destination | No. Cases | No. of Air Passengers (100,000) | RR |
|---|---|---|---|
| China | 40 | 271.8 | Reference |
| Vietnam | 51 | 21.7 | 16.0 |
| Thailand | 25 | 18.2 | 9.3 |
| Philippines | 183 | 20.5 | 60.7 |
| Indonesia | 1385 | 17.3 | 544.0 |
| India | 11 | 2.9 | 25.8 |
| Variables | Year * | |||||
|---|---|---|---|---|---|---|
| Overall | 2011 | 2013 | 2014 | 2015 | 2018 | |
| Male | 6 | 1 | 1 | 1 | 2 | 1 |
| <20 | - | - | - | - | - | - |
| 20–44 | 2 | - | - | 1- | 1 | - |
| 45–64 | 2 | 1 | 1 | - | - | - |
| ≥65 | 2 | - | - | - | 1 | 1 |
| Female | 2 | 1 | - | - | 1 | - |
| <20 | - | - | - | - | - | - |
| 20–44 | - | - | - | - | - | - |
| 45–64 | 1 | 1 | - | - | - | - |
| ≥65 | 1 | - | - | - | 1 | - |
| Variables | Non-Standardization Coefficient | p | |
|---|---|---|---|
| B Value | Standard Error | ||
| TSP (μg/m3) | −0.099 | 0.087 | 0.259 |
| PM 2.5 (μg/m3) | −0.320 | 0.279 | 0.254 |
| SO2 (ppb) | 0.607 | 1.761 | 0.731 |
| CO (ppm) | −63.818 | 36.994 | 0.088 |
| NO2 (ppb) | 2.569 | 1.074 | 0.019 |
| O3 (ppb) | 0.294 | 0.109 | 0.008 |
| Variables | Non-Standardization Coefficient | p | |
|---|---|---|---|
| B Value | Standard Error | ||
| Temperature (°C) | 1.096 | 0.542 | 0.046 |
| Precipitation (mm) | 0.001 | 0.010 | 0.890 |
| Relative humidity (%) | −0.524 | 0.392 | 0.184 |
| Mean Pressure (hPa) | 0.349 | 0.451 | 0.441 |
| Number of Days with Precipitation ≥0.1 mm (day) | 0.137 | 0.519 | 0.792 |
| Sunshine Duration (hr) | −0.038 | 0.041 | 0.353 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, F.-H.; Chen, B.-C.; Chou, Y.-C.; Chien, W.-C.; Chung, C.-H.; Hsieh, C.-J.; Yu, C.-P. The Epidemiology of Entamoeba histolytica Infection and Its Associated Risk Factors among Domestic and Imported Patients in Taiwan during the 2011–2020 Period. Medicina 2022, 58, 820. https://doi.org/10.3390/medicina58060820
Lin F-H, Chen B-C, Chou Y-C, Chien W-C, Chung C-H, Hsieh C-J, Yu C-P. The Epidemiology of Entamoeba histolytica Infection and Its Associated Risk Factors among Domestic and Imported Patients in Taiwan during the 2011–2020 Period. Medicina. 2022; 58(6):820. https://doi.org/10.3390/medicina58060820
Chicago/Turabian StyleLin, Fu-Huang, Bao-Chung Chen, Yu-Ching Chou, Wu-Chien Chien, Chi-Hsiang Chung, Chi-Jeng Hsieh, and Chia-Peng Yu. 2022. "The Epidemiology of Entamoeba histolytica Infection and Its Associated Risk Factors among Domestic and Imported Patients in Taiwan during the 2011–2020 Period" Medicina 58, no. 6: 820. https://doi.org/10.3390/medicina58060820