1. Introduction
The state of oral health is determined by a complex of interactions between socioeconomic status, beliefs, behaviors [
1,
2], values [
3,
4], and oral health literacy [
5].
The term oral health values is defined as the importance the individual gives to self-care and to their trust in professional care [
4,
6]. The notion of oral health beliefs represents the individual perceptions of the ability to control the results of one’s own oral health [
7]. A positive perception of these abilities represents increased care priorities [
8]. Thus, knowledge and education contribute to this. Research shows that oral care education is associated with beliefs in the highest oral health level [
5,
9]. In terms of process, beliefs often have an intuitive and unreasonable character. Values require a process of reflection, of analysis. Awareness of one’s own values depends on knowledge, on oral health literacy—the degree to which individuals have the ability to understand basic oral health care information [
10].
For the evaluation of oral health beliefs, there are a series of instruments, such as those based on clearly established patterns (Health Beliefs Model), for example, the Oral Health Belief Questionnaire, which measures five types of beliefs regarding oral health: perceived seriousness, benefit from preventive practices, benefit of plaque control, effectiveness of dentists, and perceived importance [
11], validated in various contexts [
12,
13]; the Oral Health Behavior Questionnaire for Adolescents, which takes into account the adolescents’ beliefs about oral health behaviors [
14]; or tools that assess oral health knowledge, attitude, and behavior (for example, the KAB questionnaire), thus linking oral health literacy, oral health beliefs, and behaviors in a single tool [
15].
However, for the assessment of oral health values, the tools are reduced to a considerable extent. In the literature, it was considered that the Oral Health Impact Profile (OHIP-14), which considers the poor impact of oral health on the quality of life [
16], is a tool that measures oral health values [
17]. However, it is worth mentioning that oral health, in turn, depends on how much the individual values it. The first tool built on this approach, namely, what the patient values, is the Oral Health Values Scale (OHVS) [
4], which takes into account the variation of values and helps explain the differences in using oral care and treatments.
The OHVS is a multidimensional instrument built in 2021 whose purpose is to identify and measure the values of one’s oral health [
4]. Unlike other instruments that deal with oral health (OHIP-14 is focused on the quality of life) [
16] or the Hiroshima University-Dental Behavioral Inventory on oral self-care behavior (HU-dbi) [
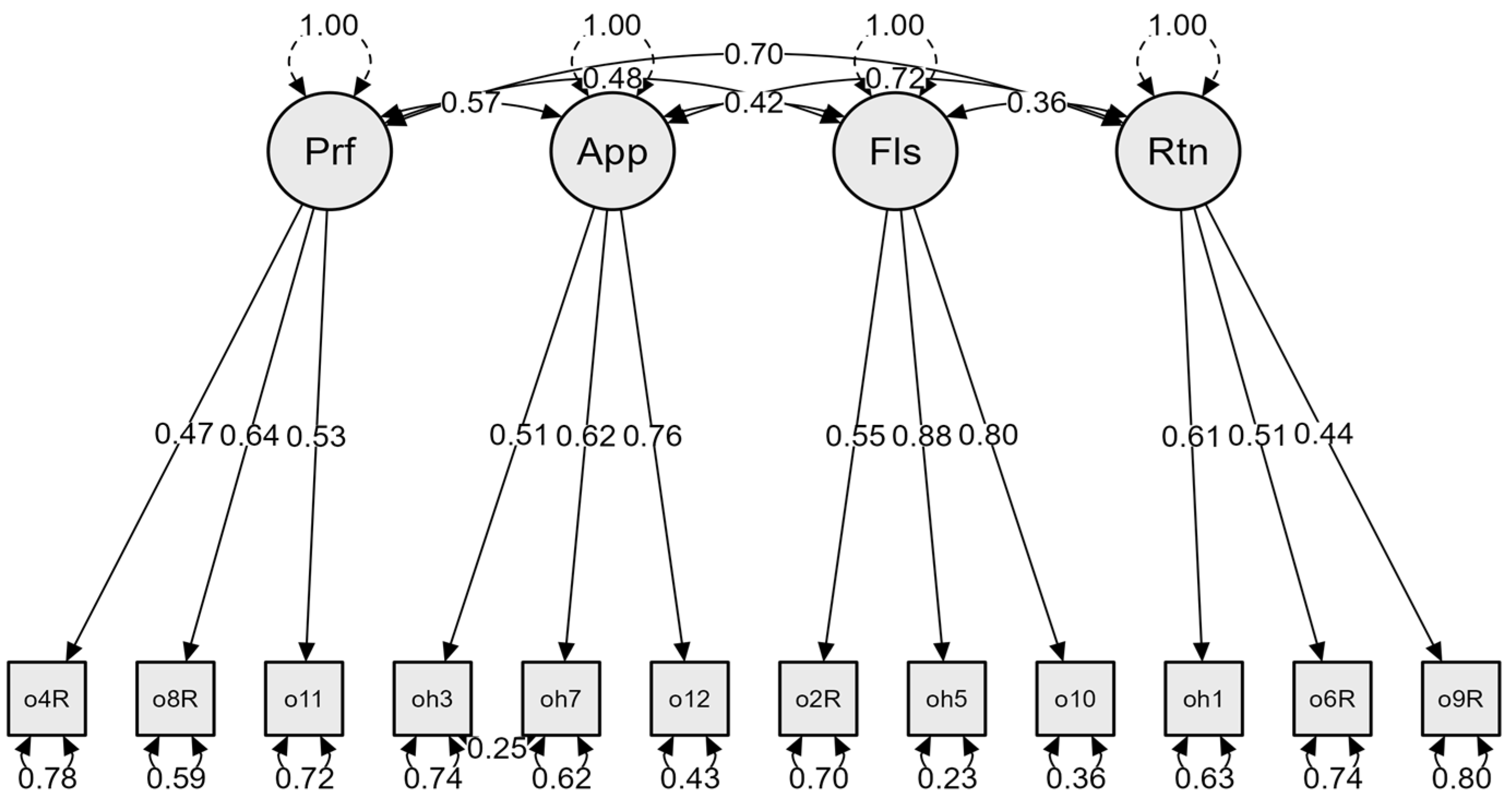
18], in the OHVS, the focus is on how much attention an individual pays to oral health care and on how much one invests in auxiliary oral health care. The validation of the scale was conducted in a case of American respondents. The scale is composed of twelve items, of which six are reversed, assessed on a continuum from 1—strongly disagree to 5—strongly agree. The total score of the scale is between 12 and 60 items. The items are distributed within four factors:
Professional dental care and the costs associated with it in terms of energy, time, and focus (e.g., Going to a dentist is not worth the cost to me).
Appearance and health aims to consider dentition as a source of pride and the evaluation of oral health as part of general health (e.g., My smile is an important part of my appearance).
Flossing as a result of consistent self-care behavior (e.g., Flossing my teeth every day is a high priority for me).
Retention of natural teeth reflects the values of oral health by means of the implications it has in one’s functioning and personal health (e.g., It is important to me to keep my natural teeth).
The internal consistency reported on by the authors in the case of the sample of American subjects is good, both for each and every subscale (αs < 0.70) and for the entire instrument (α = 0.84). The association of the OHVS with instruments that evaluate constructs of oral health provided the evidence for concurrent and convergent validity. In the development and validation stages, the OHVS was associated with various instruments that measure the oral health impact profile (Oral Health Impact Profile-14—OHIP-14), distrust of dentist (Revised Dental Beliefs Survey—R-DBS), oral health literacy (Health Literacy in Dentistry Scale—HeLD and Comprehensive Measure of Oral Health Knowledge—CMOHK), oral self-care (Dental Neglect Scale—DNS and Importance of Oral Self-Care Behavior—IDB), and dental anxiety and fear (Dental Fear Survey—DFS and Index of Dental Anxiety and Fear—IDAF-4C) [
4]. A similar pattern of the OHVS relationship with the other instruments was observed in both stages. Thus, the OHVS negatively correlates with the quality of life related to oral health, dental fear, and distrust of dentist. It positively correlates with oral health literacy and oral self-care.
The purpose of the present research is to adapt and validate the Oral Health Values Scale (OHVS) into the Romanian language and test the factorial structure and the evaluation of the psychometrical properties of the scale.
The rationale for this approach was motivated by the fact that the OHVS is the first instrument of its kind in the assessment literature that deals with the evaluation of the values related to oral health and with the evaluation of the doctor–patient relationship. Secondly, we were motivated by the fact that researchers and clinicians need valid instruments regarding the concepts that are important within one’s culture and language for epidemiological studies and oral health education sessions in dental offices. These studies may put forth a profile of the population in various social environments with regard to their personal values concerning health, an important aspect given that the latter influences one’s lifestyle. One’s healthy behavior regarding one’s cariogenic diet, personal oral hygiene, and dental visits can be changed according to the values concerning health within programs meant to promote health in communities, with tailored oral health education messages.
Upon reading the study of its development and validation published in 2021, one can infer that the OHVS has good psychometric properties [
4]. However, in Romania, people do not go to the dentist as often as the people in other countries in the European Union do, although medical services in private practices are financially acceptable [
19,
20,
21]. In addition, 18% of a population of 5000 Romanians, investigated in 2021 by the National Inspectorate of Public Health, had not visited the dentist in the last 5 years [
22]; therefore, there could be differences with regard to the degree to which individuals invest in their oral health. Populations from different countries can have different perceptions on what good oral health means.
Hypotheses
Considering the available literature [
4], the authors propose the hypothesis that the four-factor OHVS is structurally valid as shown by confirmatory factorial analysis (CFA). In addition, the authors expect to obtain significant associations between the OHVS and the tests that measure other oral health constructs: Oral Health Impact Profile (OHIP-14), Dental Neglect Scale (DNS), Revised Dental Beliefs Survey (R-DBS), and general health literacy (GHL).
4. Discussion
The study focused on the translation of the OHVS and the assessment of its validity and reliability in the case of a Romanian adult population.
The OHVS authors concluded that the relevant values for oral health comprise four factors with implications on aspect and functionality: Professional dental care, Appearance, Flossing, and Retention of the natural teeth. The correlations between the OHVS and other measures of oral health constructs and oral health behaviors in the development and validation samples provided evidence on the convergent and competing validity. Under such conditions, the OHVS seems a useful and promising measure in epidemiologic and behavioral dental research [
4].
Based on these considerations, for the cross-cultural validation of the OHVS, the authors resorted to a factorial structure analysis through CFA and selected the best-known tools in the oral health field, some already validated by the Romanian population, out of which some can be seen in the validation of the English version of the OHVS, as it has already been shown above: OHIP-14, R-DBS, DNS, GHL. After making sure that the social desirability did not affect the completion of the instruments, we proceeded to the CFA.
The confirmatory factorial analysis supported the structure of the four-factor scale and the integral presence of all 12 items. The CFA showed that the scale has good fit indices, and all the items have a loading factor over 0.40. Considering the replication of the four-factor structure of the scale and the good value of the goodness-of-fit indices, it was considered that the findings of the present study are in line with those obtained in the validation of the English version [
4].
The comparison of the average scores of the subscales obtained in the current study with those obtained on the American sample [
4] showed a hierarchy similar to the latter: Appearance and Retention of teeth had the highest values, followed by Professional dental care and, finally, Flossing, which suggests similar values regardless of the cultural model.
As for internal consistency, evidence was found for the general scale and for two subscales, Appearance and Flossing, which had good internal consistency, while the subscales Professional dental care and Retention of natural teeth had reduced consistency. This could be due to the fact that the subscales had a small number of items, three. On the other hand, as the literature explains, Cronbach´s α internal consistency coefficients are influenced by how many items a scale has [
46]. When the number of items is below 10, the Cronbach’s α values are quite low [
47]. Therefore, for a scale of three items, the value of coefficients is expected to be a moderate one.
As expected, the OHVS significantly correlates with all the instruments within the study that measure aspects related to oral health. The convergent validity proved that the OHVS and its subscales are negatively associated with the disbelief in dental services (R-DBS) and with negative oral health impacts (OHIP-14), although the subscale Appearance is poorly related, suggesting no convergence, and positively associated with oral self-care (DNS) and general health literacy expressed through the ability to understand and read medical materials (GHL). The findings are consistent with those of the OHVS development study [
4]. Unlike the original study [
4], in the present research, weak and moderate correlations were obtained between the OHVS and the other instruments used for convergent validity.
The correlations between the four factors of the OHVS showed that the latter are associated, but they measure different concepts. The highest correlation was between Appearance and Retention of teeth. A comparison with the original study in which the OHVS was developed and validated showed a similar result [
4]. The discriminant validity was certified by the Fornell–Larcker criterion [
40]. The values of the square root of the indicator AVE were higher than the inter-construct correlation coefficients for all factors.
The construct validity of the scale was also verified by the gender effect. The literature shows that women have more dental anxiety [
48]; therefore, they frequent more dental care practices [
49], and they have positive attitudes towards dental hygiene [
50,
51,
52,
53]. In addition to using dental floss more than men do, women trust the efficiency of the latter [
54,
55]. This pattern was noticeable in the present sample as well. As for gender differences, the results confirm prior data in the literature that show that women invest more in professional care and aspect, and they believe in the efficiency of flossing. The result is consistent with that of other pieces of research. For example, it is demonstrated that, while both men and women have the same level of knowledge about oral health, they do not have the same attitudes and behaviors. Women invest more in their aspect and beauty than men do; therefore, they tend to take better care of their teeth, to follow the doctors’ instructions, and to show up on time for appointments [
54].
Research carried out on samples of Romanian subjects showed the fact that women take more measures with regard to their oral health precisely because they care more about oral health [
8]. For women, their smile is a critical reason for which they resort to oral health services [
56].
5. Limitations
Several limitations are worth mentioning. Although the data come from a relatively large sample, the latter is still a probabilistic one, which can make the results less representative. Secondly, although the age range greatly varies (the age bracket is 18 and 75), there is still a large number of young students (18–29 years old—58% and 30–35 years old—8%). The limitation provides the opportunity for further research, since subsequent studies could take into consideration the validation of the scale on specific populations, such as teenagers, emerging adults, elderly people, etc. In addition, there is a high number of women in the sample, which means that the results are relevant for this gender. The gender disproportion may be due to the receptivity of the female population in completing questionnaires that improve self-knowledge. Of course, this aspect limits the generalization of the results. Another possible limitation is related to the fact that the data regarding the frequency of visits to the dentist were not collected. Last, but not least, another aspect related to the sample comes from the level of education of the participants, who are mostly people with higher education. Clearly, this percentage of people with higher education does not reflect the actual situation in Romania.
Thus, there is the need for future research on samples that are equally distributed concerning gender and education level in order to have a more accurate validation of the Romanian version of the OHVS. Despite these limitations, the proof regarding the construct validity of the OHVS is a starting point for subsequent research regarding the examination of the OHVS properties. In this sense, in order to better understand the quality of the items and of the information provided by the OHVS, the authors consider that it is important to carry out subsequent research that should use the item response theory (IRT) analysis.


 ,
, 


{kind=link}