
Oral Microbiome Using Colocasia antiquorum var. esculenta Extract Varnish in a Mouse Model with Oral Gavage of P. gingivalis ATCC 53978

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethanol Extract of CA
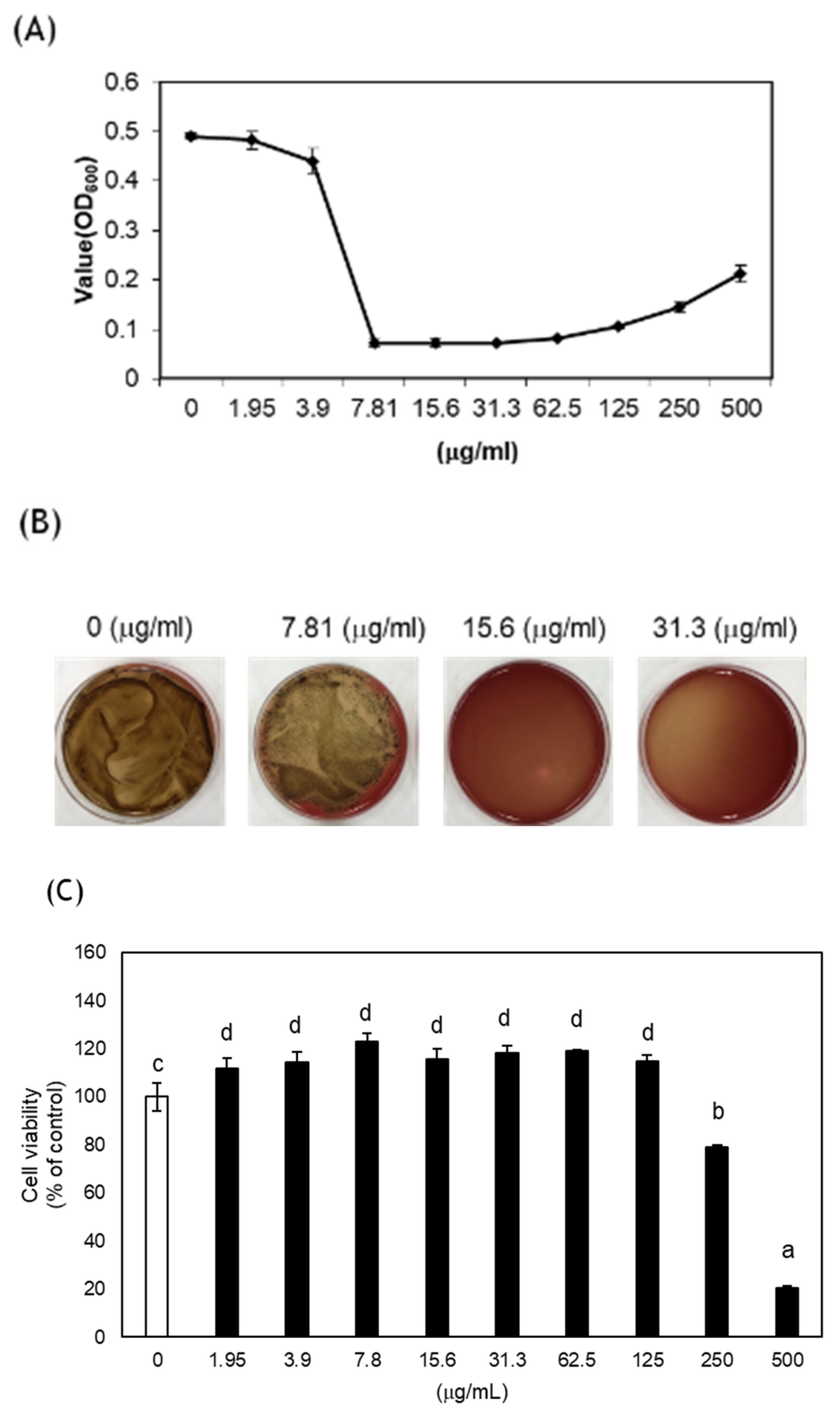
2.2. Antibacterial Assay
2.3. Cytotoxicity
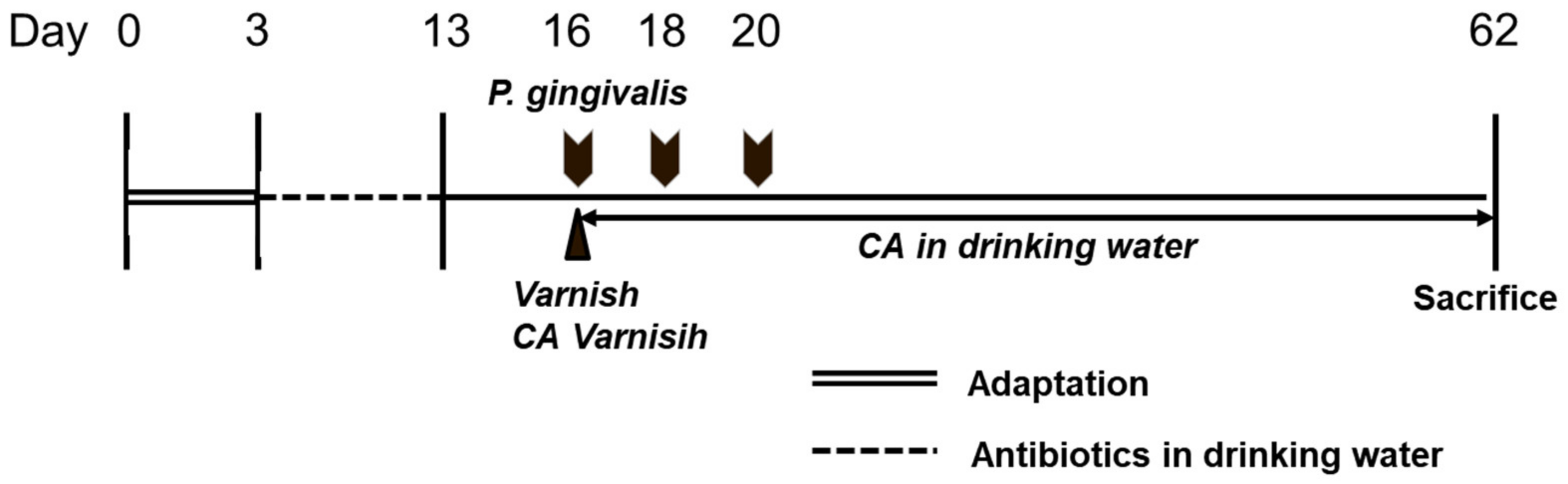
2.4. Oral Gavage of the P. gingivalis Mouse Model
- Group 1: Negative control (NC; no bacterial inoculation, no treatment)
- Group 2: Positive control (PC; bacterial inoculation, no treatment)
- Group 3: CA in drinking water (WCA; bacterial inoculation, 0.5% CA extract in drinking water)
- Group 4: Varnish (V; bacterial inoculation, varnish)
- Group 5: CA varnish (VCA; bacterial inoculation, varnish mixed with CA)
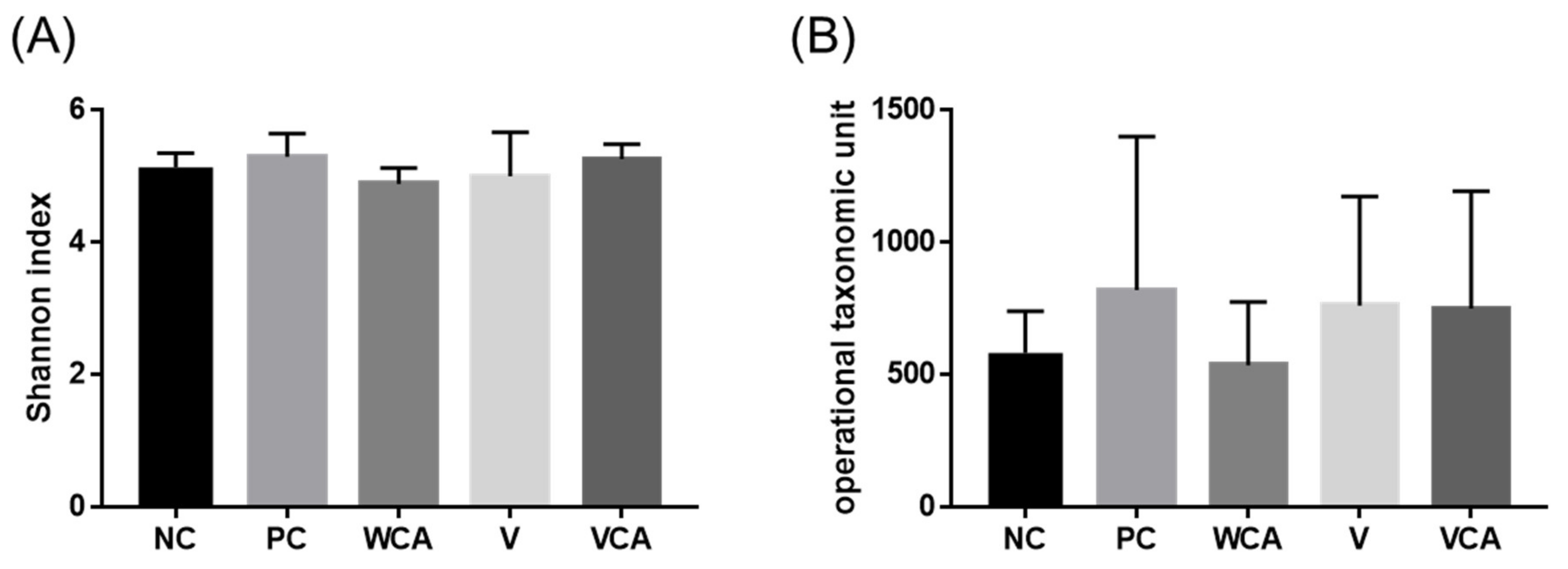
2.5. Oral Microbiome
2.6. mRNA Expression by Quantitative RT-PCR
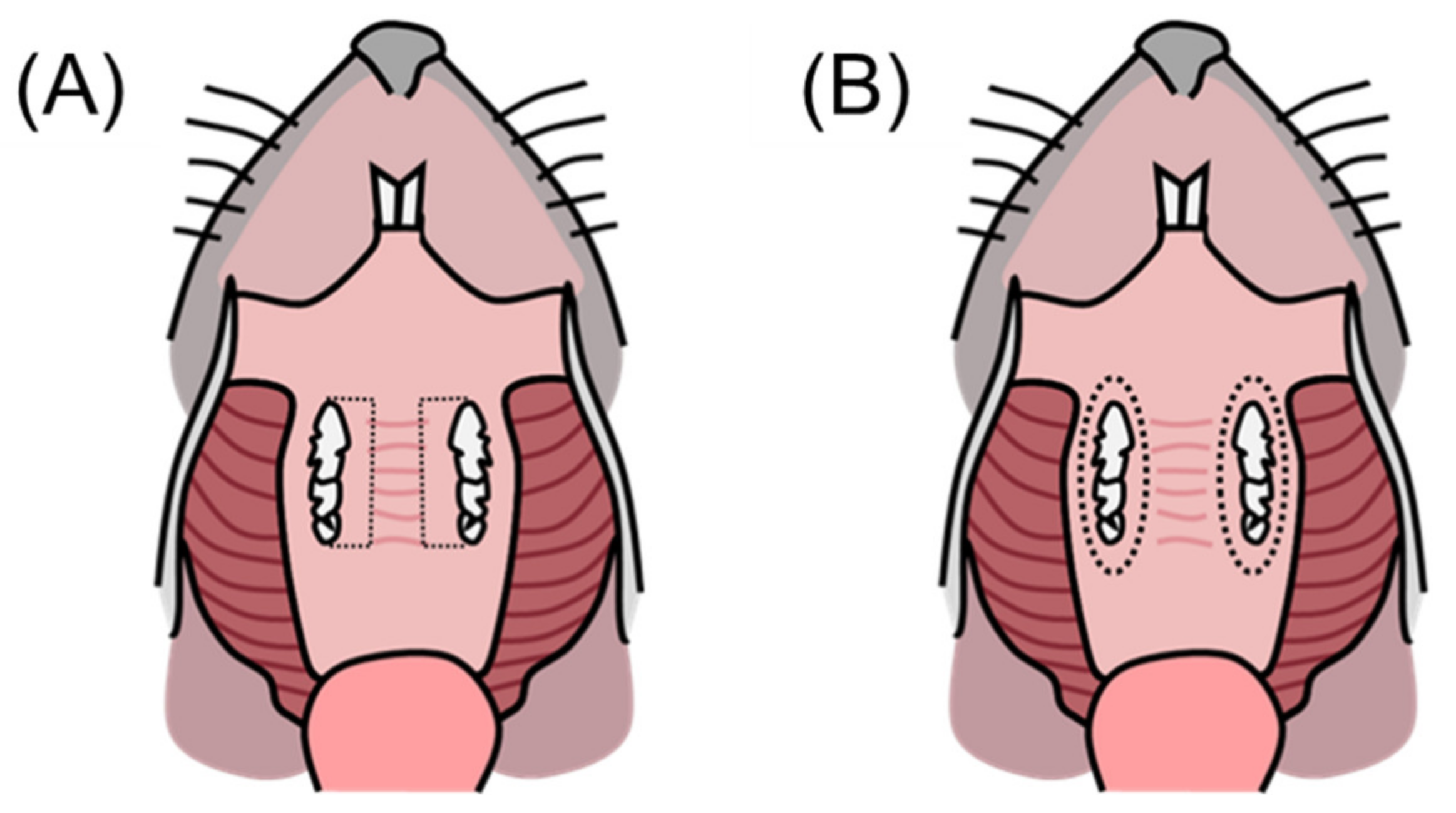
2.7. Alveolar Bone Loss
2.8. Statistical Analysis
3. Results
3.1. Antibacterial Effect and Cytotoxicity of CA
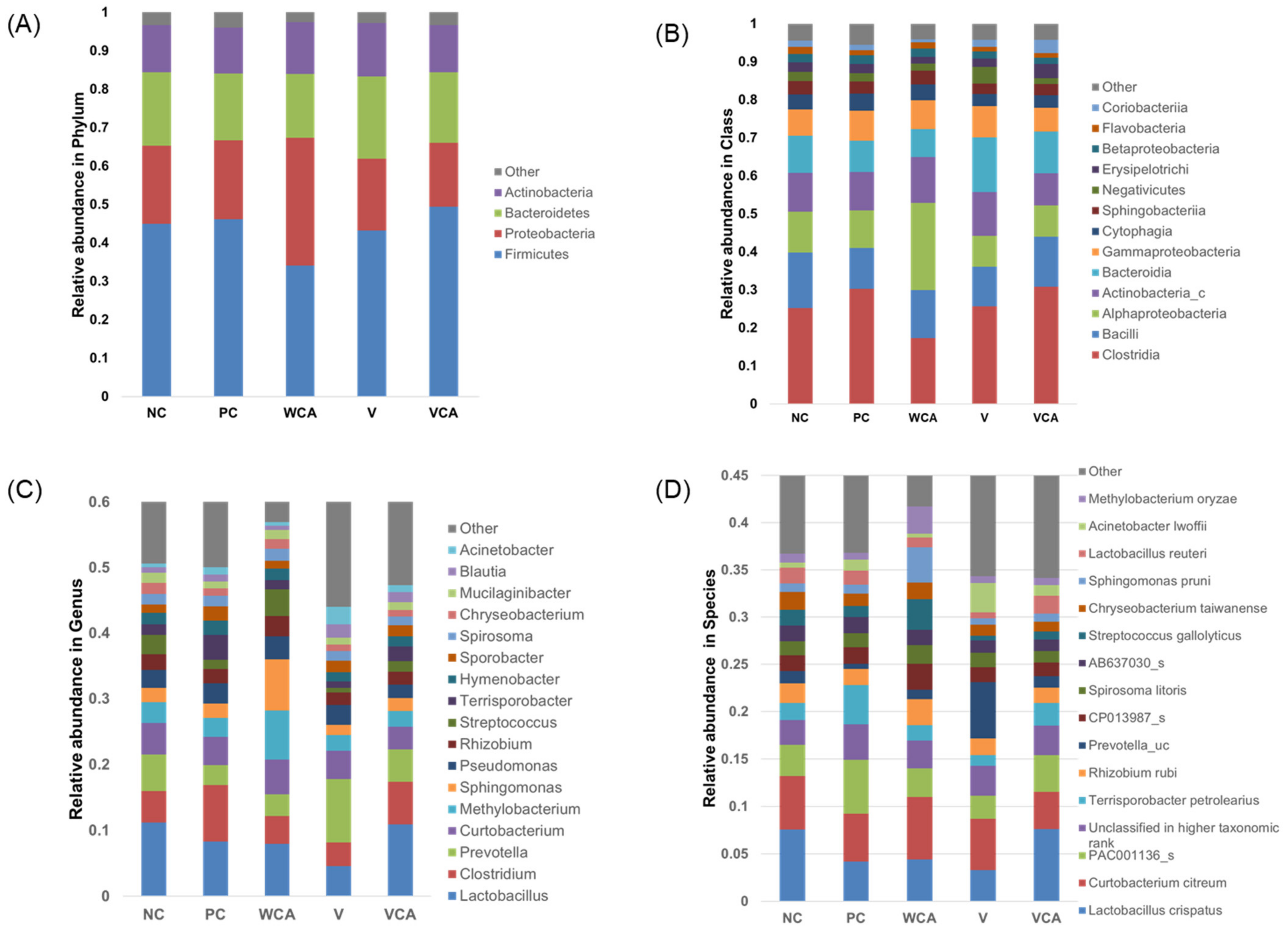
3.2. Oral Microbiome
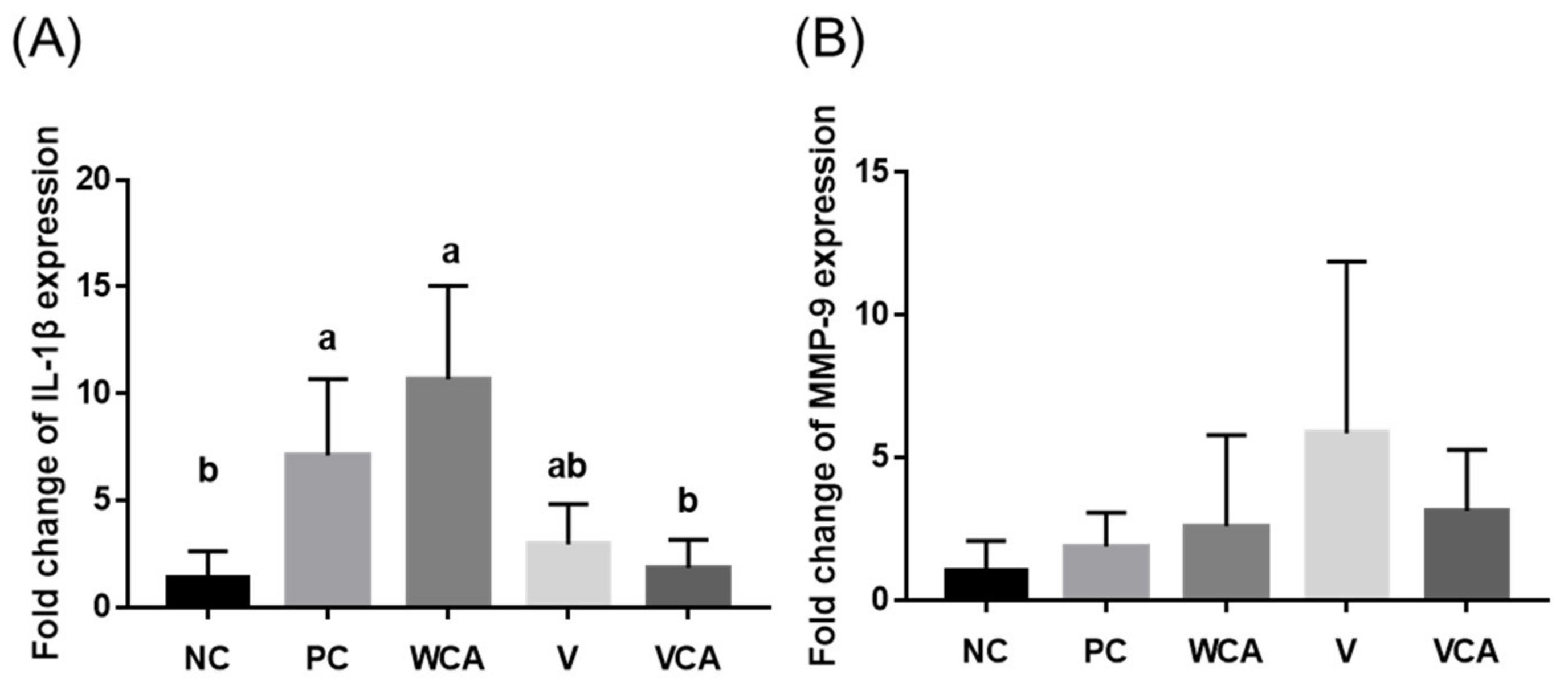
3.3. Anti-Inflammatory Effect
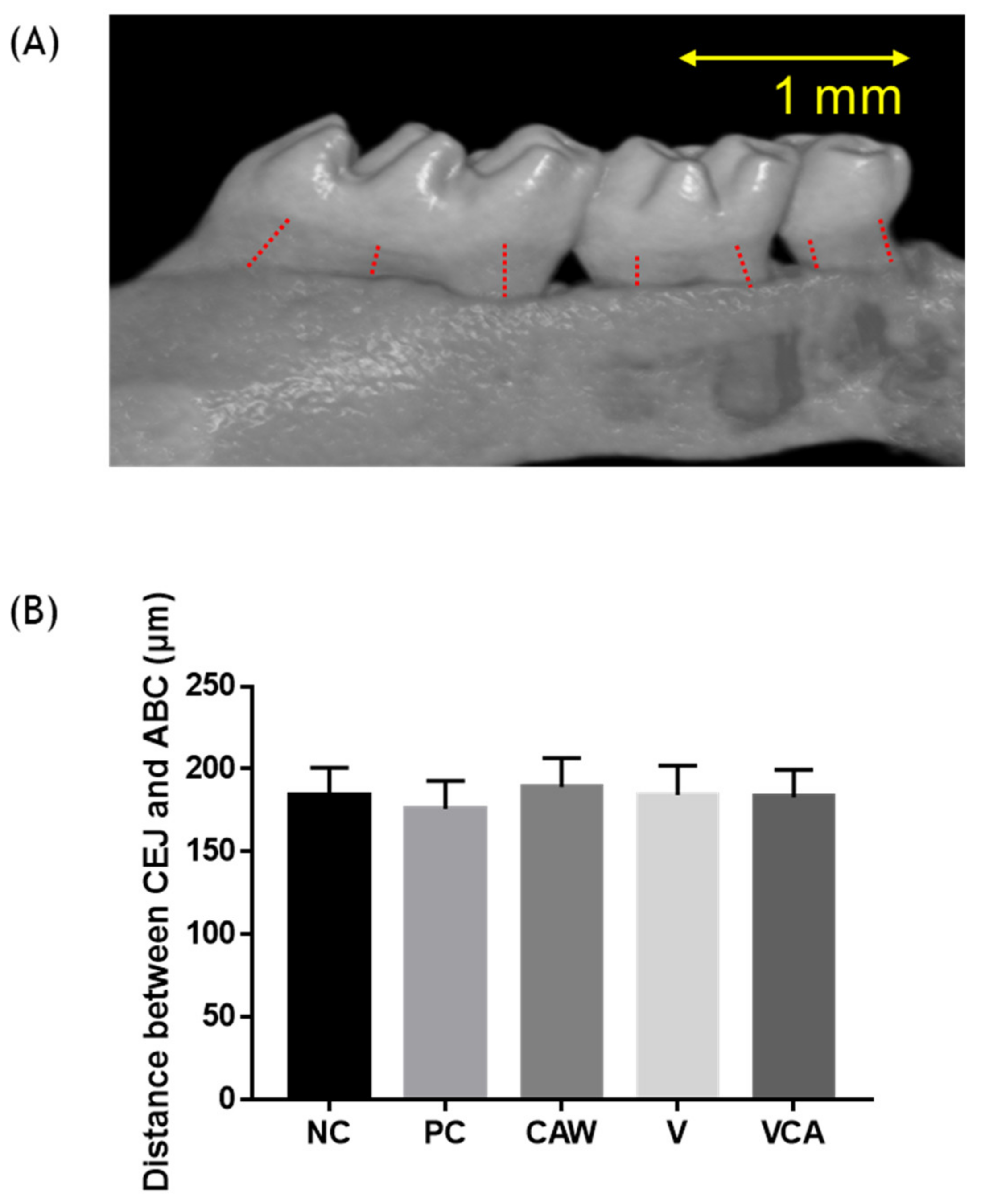
3.4. Alveolar Bone Loss
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kilian, M.; Chapple, I.L.C.; Hannig, M.; Marsh, P.D.; Meuric, V.; Pedersen, A.M.L.; Tonneti, M.S.; Wade, W.G.; Zaura, E. The oral microbiome—An update for oral healthcare professionals. Br. Dent. J. 2016, 221, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Daly, C.G.; Seymour, G.J.; Kieser, J.B. Bacterial endotoxin: A role in chronic inflammatory periodontal disease? J. Oral Pathol. Med. 1980, 9, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Ide, M.; Jagdev, D.; Coward, P.Y.; Crook, M.; Barclay, G.R.; Wilson, R.F. The Short-Term Effects of Treatment of Chronic Periodontitis on Circulating Levels of Endotoxin, C-Reactive Protein, Tumor Necrosis Factor-α, and Interleukin-6. J. Periodontol. 2004, 75, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Casarin, R.C.V.; Del Peloso, R.É.; Mariano, F.S.; Nociti, F.H., Jr.; Casati, M.Z.; Gonçalves, R.B. Levels of Aggregatibacter actinomycetemcomitans, Porphyromonas gingivalis, Inflammatory Cytokines and Species-Specific Immunoglobulin G in Generalized Aggressive and Chronic Periodontitis. J. Periodontal. Res. 2010, 45, 635–642. [Google Scholar] [CrossRef]
- Rai, B.; Kharb, S.; Jain, R.; Anand, S.C. Biomarkers of periodontitis in oral fluids. J. Oral Sci. 2008, 50, 53–56. [Google Scholar] [CrossRef] [Green Version]
- De Araújo, R.F., Jr.; de Souza, T.O.; de Medeiros, C.A.X.; de Souza, L.B.; de Freitas, M.L.; de Lucena, H.F.; do Socorro Costa Feitosa Alves, M.; de Araújo, A.A. Carvedilol Decrease IL-1β and TNF-α, Inhibits MMP-2, MMP-9, COX-2, and RANKL Expression, and Up-Regulates OPG in a Rat Model of Periodontitis. PLoS ONE 2013, 8, e66391. [Google Scholar] [CrossRef]
- Cobb, C.M.; Sottosanti, J.S. A re-evaluation of scaling and root planing. J. Periodontol. 2021, 92, 1370–1378. [Google Scholar] [CrossRef]
- Buchanan, S.A.; Robertson, P.B. Calculus Removal by Scaling/Root Planing with and without Surgical Access. J. Periodontol. 1987, 58, 159–163. [Google Scholar] [CrossRef]
- Machtei, E.E.; Hirsh, I.; Falah, M.; Shoshani, E.; Avramoff, A.; Penhasi, A. Multiple applications of flurbiprofen and chlorhexidine chips in patients with chronic periodontitis: A randomized, double blind, parallel, 2-arms clinical trial. J. Clin. Periodontol. 2011, 38, 1037–1043. [Google Scholar] [CrossRef] [Green Version]
- Rainsford, K. Profile and mechanisms of gastrointestinal and other side effects of nonsteroidal anti-inflammatory drugs (NSAIDs). Am. J. Med. 1999, 107, 27–35. [Google Scholar] [CrossRef]
- Laleman, I.; Teughels, W. Novel natural product-based oral topical rinses and toothpastes to prevent periodontal diseases. Periodontology 2000, 84, 102–123. [Google Scholar] [CrossRef]
- Rajeshwari, H.R.; Dhamecha, D.; Jagwani, S.; Rao, M.; Jadhav, K.; Shaikh, S.; Puzhankara, L.; Jalalpure, S. Local drug delivery systems in the management of periodontitis: A scientific review. J. Control Release 2019, 307, 393–409. [Google Scholar] [CrossRef]
- Kumar, M.; Bhardwaj, R. Wetting characteristics of Colocasia esculenta (Taro) leaf and a bioinspired surface thereof. Sci. Rep. 2020, 10, 935. [Google Scholar] [CrossRef]
- Simsek, S.; El Nehir, S. In vitro starch digestibility, estimated glycemic index and antioxidant potential of taro (Colocasia esculenta L. Schott) corm. Food Chem. 2015, 168, 257–261. [Google Scholar] [CrossRef]
- Yang, A.H.; Yeh, K.W. Molecular cloning, recombinant gene expression, and antifungal activity of cystatin from taro (Colocasia esculenta cv. Kaosiung no. 1). Planta 2005, 221, 493–501. [Google Scholar] [CrossRef]
- Moon, S.-H.; Ji, S.H.; Son, J.-L.; Shin, S.-J.; Oh, S.; Kim, S.H.; Bae, J.-M. Antibacterial, anti-inflammatory, and anti-osteoclastogenic activities of Colocasia antiquorum var. esculenta: Potential applications in preventing and treating periodontal diseases. Dent. Mater. J. 2020, 39, 1096–1102. [Google Scholar] [CrossRef]
- Abe, T.; Hajishengallis, G. Optimization of the ligature-induced periodontitis model in mice. J. Immunol. Methods 2013, 394, 49–54. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Lu, Z.; Zhang, X.; Yu, H.; Kirkwood, K.L.; Lopes-Virella, M.F.; Huang, Y. Metabolic Syndrome Exacerbates Inflammation and Bone Loss in Periodontitis. J. Dent. Res. 2015, 94, 362–370. [Google Scholar] [CrossRef] [Green Version]
- Cai, Y.; Chen, Z.; Liu, H.; Xuan, Y.; Wang, X.; Luan, Q. Green tea epigallocatechin-3-gallate alleviates Porphyromonas gingivalis-induced periodontitis in mice. Int. Immunopharmacol. 2015, 29, 839–845. [Google Scholar] [CrossRef]
- De Molon, R.S.; de Avila, E.D.; Cirelli, J.A. Host responses induced by different animal models of periodontal disease: A literature review. J. Investig. Clin. Dent. 2013, 4, 211–218. [Google Scholar] [CrossRef]
- Boyer, E.; Leroyer, P.; Malherbe, L.; Fong, S.B.; Loréal, O.; Bonnaure Mallet, M.; Meuric, V. Oral dysbiosis induced by Porphyromonas gingivalis is strain-dependent in mice. J. Oral Microbiol. 2020, 12, 1832837. [Google Scholar] [CrossRef]
- Oz, H.S.; Puleo, D.A. Animal Models for Periodontal Disease. J. Biomed. Biotechnol. 2011, 2011, 754857. [Google Scholar] [CrossRef] [Green Version]
- Berezow, A.B.; Darveau, R.P. Microbial shift and periodontitis. Periodontology 2000, 55, 36–47. [Google Scholar] [CrossRef]
- Mougeot, J.-L.C.; Stevens, C.B.; Cotton, S.L.; Morton, D.S.; Krishnan, K.; Brennan, M.T.; Paster, B.C.; Bahrani Mougeot, F.K. Concordance of HOMIM and HOMI NGS technologies in the microbiome analysis of clinical samples. J. Oral Microbiol. 2016, 8, 30379. [Google Scholar] [CrossRef] [Green Version]
- Dewhirst, F.E.; Chen, T.; Izard, J.; Paster, B.J.; Tanner, A.C.R.; Yu, W.-H.; Lakshmanan, A.; Wade, W.G. The Human Oral Microbiome. J. Bacteriol. 2010, 192, 5002–5017. [Google Scholar] [CrossRef] [Green Version]
- Costalonga, M.; Herzberg, M.C. The oral microbiome and the immunobiology of periodontal disease and caries. Immunol. Lett. 2014, 162, 22–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Healy, C.M.; Moran, G.P. The microbiome and oral cancer: More questions than answers. Oral Oncol. 2019, 89, 30–33. [Google Scholar] [CrossRef]
- Abusleme, L.; O’Gorman, H.; Dutzan, N.; Greenwell-Wild, T.; Moutsopoulos, N.M. Establishment and Stability of the Murine Oral Microbiome. J. Dent. Res. 2020, 99, 721–729. [Google Scholar] [CrossRef]
- Abusleme, L.; Hong, B.-Y.; Hoare, A.; Konkel, J.; Diaz, P.; Moutsopoulos, N. Oral Microbiome Characterization in Murine Models. Bio-Protocol 2017, 7, 139–148. [Google Scholar] [CrossRef] [Green Version]
- Vikrant Berde, C.; Salvi Sagar, P.; Kajarekar Kunal, V.; Joshi Suyoj, A.; Berde Vikrant, B. Insight into the Animal Models for Microbiome Studies. In Microbiome in Human Health Disease; Springer: Singapore, 2021; pp. 259–273. [Google Scholar] [CrossRef]
- Yin, L.; Wan, Y.-D.; Pan, X.-T.; Zhou, C.-Y.; Lin, N.; Ma, C.-T.; Yao, J.; Su, Z.; Wan, C.; Yu, W.-Y.; et al. Association Between Gut Bacterial Diversity and Mortality in Septic Shock Patients: A Cohort Study. Med. Sci. Monit. 2019, 25, 7376–7382. [Google Scholar] [CrossRef]
- Nguyen, N.-P.; Warnow, T.; Pop, M.; White, B. A perspective on 16S rRNA operational taxonomic unit clustering using sequence similarity. NPJ Biofilms Microbiomes 2016, 2, 16004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, P.J. Genetic control of the immune response in pathogenesis. J. Periodontol. 2005, 76, 2042–2046. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.-H.; Shin, S.-J.; Tae, H.-J.; Oh, S.-H.; Bae, J.-M. Effects of Colocasia antiquorum var. esculenta Extract In Vitro and In Vivo against Periodontal Disease. Medicina 2021, 57, 1054. [Google Scholar] [CrossRef]
- Jain, S.; Darveau, R.P. Contribution of Porphyromonas gingivalis lipopolysachharide to periodontitis. Periodontology 2000, 54, 53. [Google Scholar] [CrossRef] [Green Version]
- Dahlen, G.; Manji, F.; Baelum, V.; Fejerskov, O. Black pigmented Bacteroides species and Actinobacillus actinomycetemcomitans in subgingival plaque of adult Kenyans. J. Clin. Periodontol. 1989, 16, 305–310. [Google Scholar] [CrossRef]
- Lee, J.-Y.; Sojar, H.T.; Bedi, G.S.; Genco, R.J. Porphyromonas (Bacteroides) gingivalis fimbrillin: Size, amino-terminal sequence, and antigenic heterogeneity. Infect. Immun. 1991, 59, 383–389. [Google Scholar] [CrossRef] [Green Version]
- ISO10993-5; Biological Evaluation of Medical Devices—Part 5: Tests for In Vitro Cytotoxicity. International Organisation for Standardization: Geneva, Switzerland, 2009.
- Welch, M.J.L.; Ramírez-Puebla, S.T.; Borisy, G.G. Oral Microbiome Geography: Micron-Scale Habitat and Niche. Cell Host Microbe 2020, 28, 160–168. [Google Scholar] [CrossRef]
- Li, H.; Xiao, B.; Zhang, Y.; Xiao, S.; Luo, J.; Huang, W. Impact of maternal intrapartum antibiotics on the initial oral microbiome of neonates. Pediatr. Neonatol. 2019, 60, 654–661. [Google Scholar] [CrossRef] [Green Version]
- Bescos, R.; Ashworth, A.; Cutler, C.; Brookes, Z.L.; Belfield, L.; Rodiles, A.; Casas-Agustench, P.; Farnham, G.; Liddle, L.; Burleigh, M.; et al. Effects of Chlorhexidine mouthwash on the oral microbiome. Sci. Rep. 2020, 10, 5254. [Google Scholar] [CrossRef] [Green Version]
- Willis, J.R.; Gabaldon, T. The human oral microbiome in health and disease: From sequences to ecosystems. Microorganisms 2020, 8, 308. [Google Scholar] [CrossRef] [Green Version]
- Booth, V.; Downes, J.; Van den Berg, J.; Wade, W.G. Gram-positive anaerobic bacilli in human periodontal disease. J. Periodontal Res. 2004, 39, 213–220. [Google Scholar] [CrossRef]
- Koll-Klais, P.; Mandar, R.; Leibur, E.; Marcotte, H.; Hammarstrom, L.; Mikelsaar, M. Oral lactobacilli in chronic periodontitis and periodontal health: Species composition and antimicrobial activity. Oral Microbiol. Immunol. 2005, 20, 354–361. [Google Scholar] [CrossRef]
- Liu, T.-H.; Tsai, T.-Y.; Pan, T.-M. The Anti-Periodontitis Effects of Ethanol Extract Prepared Using Lactobacillus paracasei subsp. paracasei NTU 101. Nutrients 2018, 10, 472. [Google Scholar] [CrossRef] [Green Version]
- Taguchi, C.; Arikawa, K.; Saitou, M.; Uchiyama, T.; Watanabe, I.; Tobita, K.; Kobayashi, R.; Ochiai, T.; Nasu, I. Orally Ingested Lactobacillus crispatus KT-11 Inhibits Porphyromonas gingivalis infected Alveolar Bone Resorption. Int. J. Oral-Med. Sci. 2015, 13, 102–109. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Ju, J.; Rigney, T.; Tribble, G. Porphyromonas gingivalis infection increases osteoclastic bone resorption and osteoblastic bone formation in a periodontitis mouse model. BMC Oral Health 2014, 14, 89. [Google Scholar] [CrossRef] [Green Version]
- Toyama, T.; Todoki, K.; Takahashi, Y.; Watanabe, K.; Takahashi, S.S.; Sugiyama, S.; Lee, M.-C.-I.; Hamada, N. Inhibitory effects of Jixueteng on P. gingivalis-induced bone loss and osteoclast differentiation. Arch. Oral Biol. 2012, 57, 1529–1536. [Google Scholar] [CrossRef]
- Baker, P.J.; Evans, R.T.; Roopenian, D.C. Oral infection with Porphyromonas gingivalis and induced alveolar bone loss in immunocompetent and severe combined immunodeficient mice. Arch. Oral Biol. 1994, 39, 1035–1040. [Google Scholar] [CrossRef]
- Baker, P.J.; Dixon, M.; Roopenian, D.C. Genetic control of susceptibility to Porphyromonas gingivalis-induced alveolar bone loss in mice. Infect. Immun. 2000, 68, 5864–5868. [Google Scholar] [CrossRef] [Green Version]
- Polak, D.; Wilensky, A.; Shapira, L.; Halabi, A.; Goldstein, D.; Weiss, E.I.; Houri-Haddad, Y. Mouse model of experimental periodontitis induced by Porphyromonas gingivalis/Fusobacterium nucleatum infection: Bone loss and host response. J. Clin. Periodontol. 2009, 36, 406–410. [Google Scholar] [CrossRef]
- Daep, C.A.; Novak, E.A.; Lamont, R.J.; Demuth, D.R. Structural Dissection and In Vivo Effectiveness of a Peptide Inhibitor of Porphyromonas gingivalis Adherence to Streptococcus gordonii. Infect. Immun. 2011, 79, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Baker, P.J.; Dixon, M.; Evans, R.T.; Roopenian, D.C. Heterogeneity of Porphyromonas gingivalis strains in the induction of alveolar bone loss in mice. Oral Microbiol. Immunol. 2000, 15, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Bostanci, N.; Belibasakis, G.N. Porphyromonas gingivalis: An invasive and evasive opportunistic oral pathogen. FEMS Microbiol. Lett. 2012, 333, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’aiuto, F.; Parkar, M.; Brett, P.M.; Ready, D.; Tonetti, M.S. Gene polymorphisms in pro-inflammatory cytokines are associated with systemic inflammation in patients with severe periodontal infections. Cytokine 2004, 28, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Hernandez Rios, M.; Sorsa, T.; Obregon, F.; Tervahartiala, T.; Valenzuela, M.A.; Pozo, P.; Dutzan, N.; Lesaffre, E.; Molas, M.; Gamonal, J. Proteolytic roles of matrix metalloproteinase (MMP) 13 during progression of chronic periodontitis: Initial evidence for MMP 13/MMP 9 activation cascade. J. Clin. Periodontol. 2009, 36, 1011–1017. [Google Scholar] [CrossRef]
- Graves, D. Cytokines That Promote Periodontal Tissue Destruction. J. Periodontol. 2008, 79, 1585–1591. [Google Scholar] [CrossRef] [Green Version]
- Lo Giudice, R.; Militi, A.; Nicita, F.; Bruno, G.; Tamà, C.; Lo Giudice, F.; Puleio, F.; Calapai, F.; Mannucci, C. Correlation between Oral Hygiene and IL-6 in Children. Dent. J. 2020, 8, 91. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primers | Forward | Reverse |
|---|---|---|
| GAPDH | AGGTTGTCTCCTGCGACTTCA | CTGTTGCTGTAGCCGTATTCATTG |
| IL-β | CTATACCTGTCCTGTGTAATGAAAGA | TCTGCTTGTGAGGTGCTGATGTA |
| MMP-9 | CCCTGGAACTCACACGACATC | GTCCACCTGGTTCACCTCATG |
| NC | PC | WCA | V | VCA | ||
|---|---|---|---|---|---|---|
| Phyla | Spirochaetes | 0.724 (0.488) | 1.438 (1.550) | 0.628 (0.428) | 0.555 (0.478) | 0.930 (1.031) |
| Class | Bacilli | 14.554 (8.278) | 10.784 (2.647) | 12.632 (7.476) | 10.409 (6.532) | 13.187 (6.558) |
| Genus | Lactobacillus | 11.206 (8.017) | 8.333 (2.527) | 7.986 (3.252) | 4.592 (2.774) | 10.912 (6.546) |
| Species | Lactobacillus crispatus | 6.529 (4.981) | 3.585 (1.580) | 3.539 (2.593) | 2.648 (1.689) | 6.632 (4.537) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, S.-J.; Moon, S.-H.; Kim, H.-J.; Oh, S.-H.; Bae, J.-M. Oral Microbiome Using Colocasia antiquorum var. esculenta Extract Varnish in a Mouse Model with Oral Gavage of P. gingivalis ATCC 53978. Medicina 2022, 58, 506. https://doi.org/10.3390/medicina58040506
Shin S-J, Moon S-H, Kim H-J, Oh S-H, Bae J-M. Oral Microbiome Using Colocasia antiquorum var. esculenta Extract Varnish in a Mouse Model with Oral Gavage of P. gingivalis ATCC 53978. Medicina. 2022; 58(4):506. https://doi.org/10.3390/medicina58040506
Chicago/Turabian StyleShin, Seong-Jin, Seong-Hee Moon, Hyun-Jin Kim, Seung-Han Oh, and Ji-Myung Bae. 2022. "Oral Microbiome Using Colocasia antiquorum var. esculenta Extract Varnish in a Mouse Model with Oral Gavage of P. gingivalis ATCC 53978" Medicina 58, no. 4: 506. https://doi.org/10.3390/medicina58040506