
Opioid-Sparing Analgesia Impacts the Perioperative Anesthetic Management in Major Abdominal Surgery

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
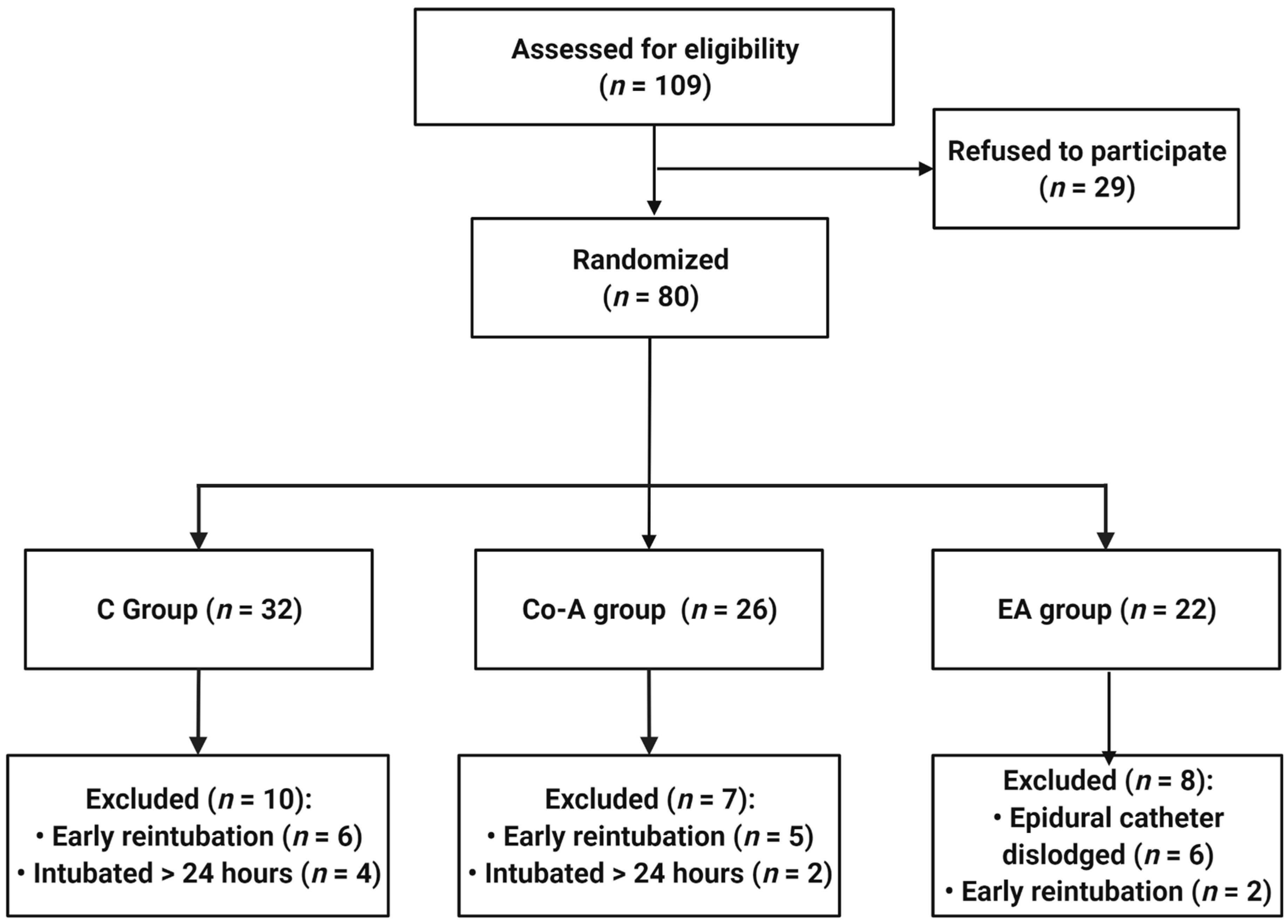
2.1. Study Design. Inclusion/Exclusion Criteria
2.2. Data Collection and Analysis
3. Results
3.1. Demographic Data
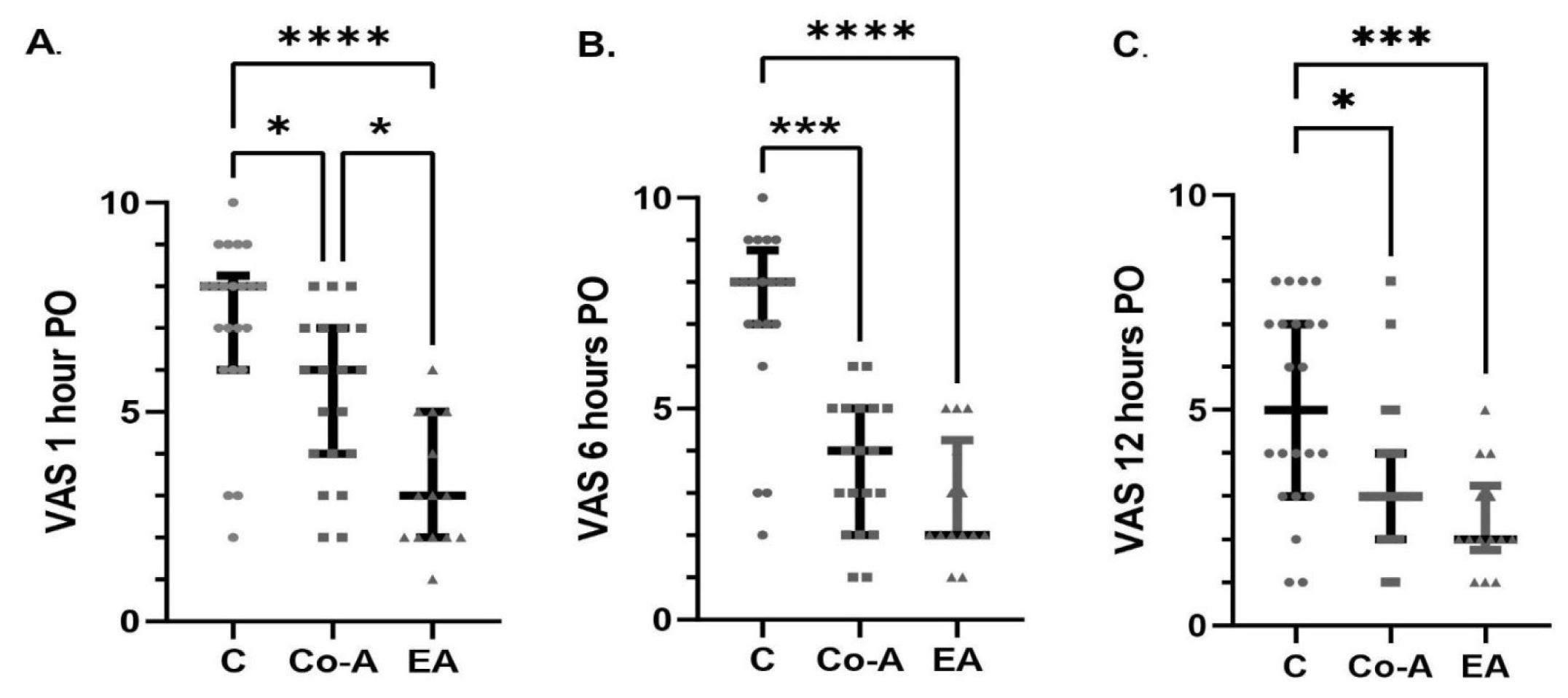
3.2. The Impact of Multimodal Analgesia Strategies on VAS Score
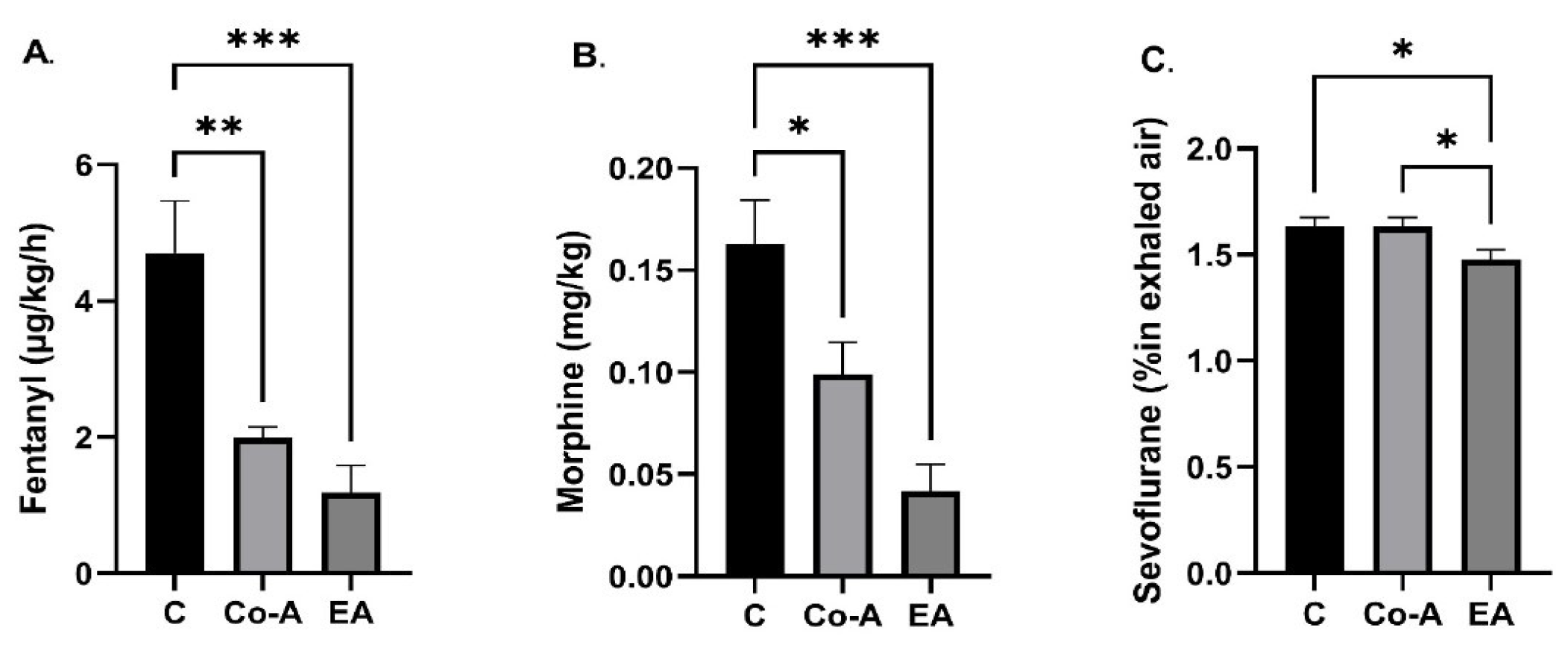
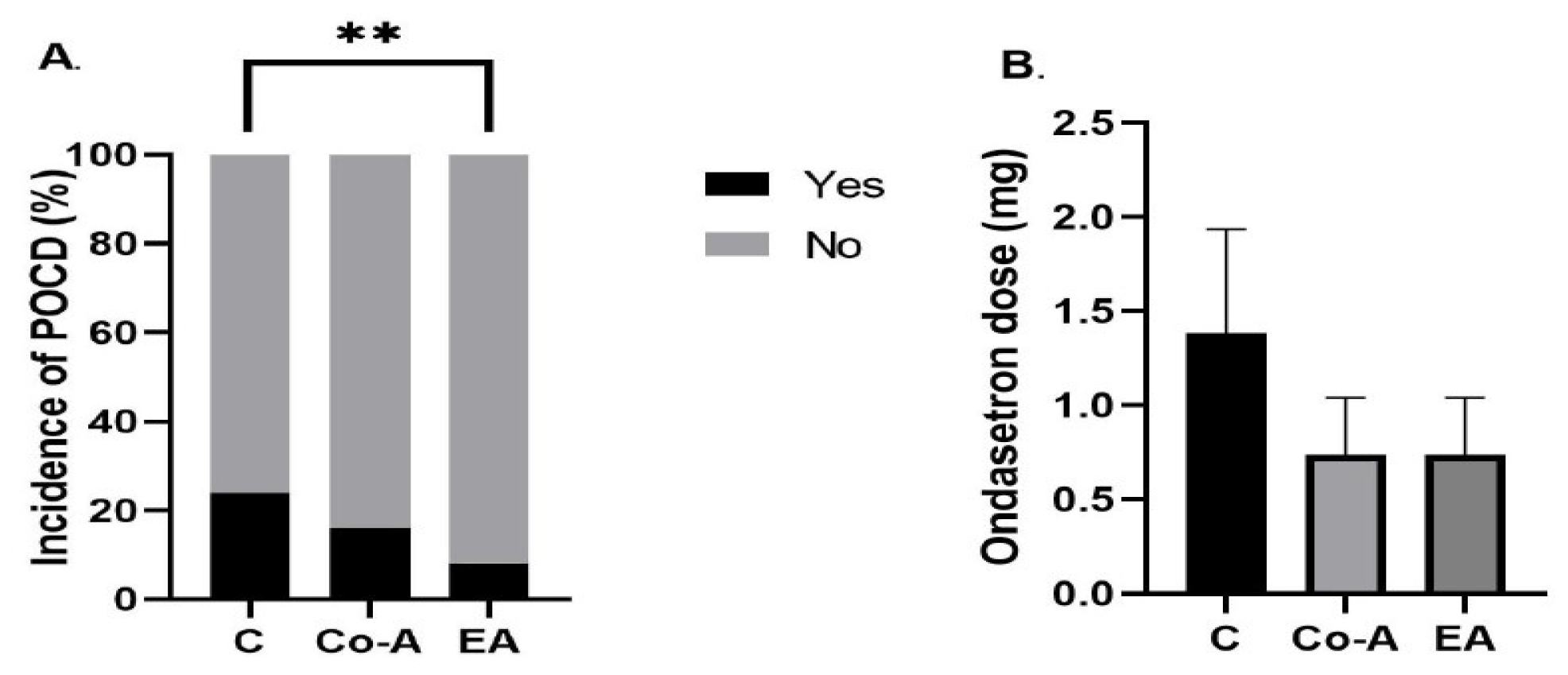
3.3. The Impact of Multimodal Analgesia Strategies on the Secondary Outcomes: The Total Intraoperative Fentanyl Dose, Total Postoperative Morphine Dose, Maximal Intraoperative Sevoflurane Concentration, the Incidence of POCD, and the Postoperative Dose of Ondansetron
4. Discussion
Study Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weiser, T.G.; Haynes, A.B.; Molina, G.; Lipsitz, S.; Esquivel, M.; Uribe-Leitz, T.; Fu, R.; Azad, T.; Chao, T.; Berry, T.; et al. Estimate of the global volume of surgery in 2012: An assessment supporting improved health outcomes. Lancet 2015, 385, S11. [Google Scholar] [CrossRef]
- Andrei, S.; Isac, S.; Carstea, M.; Martac, C.; Mihalcea, L.; Buzatu, C.; Ionescu, D.; Georgescu, D.E.; Droc, G. Isolated liver trauma: A clinical perspective in a non-emergency center for liver surgery. Exp. Ther. Med. 2022, 23, 1–5. [Google Scholar] [CrossRef]
- Botea, F.; Ionescu, M.; Braşoveanu, V.; Hrehoreţ, D.; Alexandrescu, S.; Grigorie, M.; Stanciulea, O.; Nicolaescu, D.; Tomescu, D.; Droc, G.; et al. Liver Resections in a High-Volume Center: From Standard Procedures to Extreme Surgery and Ultrasound-guided Resections. Chirurgia 2017, 112, 259–277. [Google Scholar] [CrossRef] [PubMed]
- Alexandrescu, S.; Diaconescu, A.; Zenaida, I.; Zlate, C.; Grigorie, R.; Hrehoret, D.; Brasoveanu, V.; Dima, S.; Botea, F.; Ionescu, M.; et al. Comparative Analysis between Simultaneous Resection and Staged Resection for Synchronous Colorectal Liver Metastases—A Single Center Experience on 300 Consecutive Patients. Chirurgia 2017, 112, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Balaceanu, A.; Diaconu, C.; Mateescu, D.; Stanica, A. Hepatocellular carcinoma with hepatic and pulmonary metastasis, inferior vena cava and left pulmonary artery thrombosis in a patient with asymptomatic hepatitis C. Case report. Med. Ultrason. 2010, 12, 345–348. [Google Scholar] [PubMed]
- Richebé, P.; Capdevila, X.; Rivat, C. Persistent Postsurgical Pain Pathophysiology and Preventative Pharmacologic Considerations. Anesthesiology 2018, 129, 590–607. [Google Scholar] [CrossRef] [PubMed]
- Gan, T.J. Poorly controlled postoperative pain: Prevalence, consequences, and prevention. J. Pain Res. 2017, 10, 2287–2298. [Google Scholar] [CrossRef] [Green Version]
- Chapman, C.R.; Vierck, C.J. The Transition of Acute Postoperative Pain to Chronic Pain: An Integrative Overview of Research on Mechanisms. J. Pain. 2017, 359, 1–38. [Google Scholar] [CrossRef]
- Wang, Y.; Sands, L.P.; Vaurio, L.; Mullen, E.A.; Leung, J.M. The effects of postoperative pain and its management on postoperative cognitive dysfunction. Am. J. Geriatr. Psychiatry 2007, 15, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Breivik, H.; Eisenberg, E.; O’Brien, T. The individual and societal burden of chronic pain in Europe: The case for strategic prioritisation and action to improve knowledge and availability of appropriate care. BMC Public Health 2013, 13, 1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soffin, E.M.; Lee, B.H.; Kumar, K.K.; Wu, C.L. The prescription opioid crisis: Role of the anesthesiologist in reducing opioid use and misuse. Br. J. Anaesth. 2019, 122, 198–208. [Google Scholar] [CrossRef] [PubMed]
- Anekar, A.A.; Cascella, M. WHO Analgesic Ladder. J. R. Coll. Physicians Edinb. 2021, 38, 284. [Google Scholar]
- Roberts, G.W.; Bekker, T.B.; Carlsen, H.H.; Moffatt, C.H.; Slattery, P.J.; McClure, A.F. Postoperative nausea and vomiting are strongly influenced by postoperative opioid use in a dose-related manner. Anesth. Analg. 2005, 101, 1343–1348. [Google Scholar] [CrossRef]
- Mulier, J.P. Perioperative opioids aggravate obstructive breathing in sleep apnea syndrome: Mechanisms and alternative anesthesia strategies. Curr. Opin. Anaesthesiol. 2016, 29, 129–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavand’homme, P.; Estebe, J.P. Opioid-free anesthesia: A different regard to anesthesia practice. Curr. Opin. Anaesthesiol. 2018, 31, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Helander, E.M.; Menard, B.L.; Harmon, C.M.; Homra, B.; Allain, A.; Bordelon, G.; Wyche, M.; Padnos, I.; Lavrova, A.; Kaye, A. Multimodal Analgesia, Current Concepts, and Acute Pain Considerations. Curr. Pain Headache Rep. 2017, 21, 3. [Google Scholar] [CrossRef] [PubMed]
- Seki, H.; Furumoto, K.; Sato, M.; Kagoya, A.; Hashimoto, H.; Sekiguchi, Y.; Nakatsuka, I. Effects of epidural anesthesia on postoperative nausea and vomiting in laparoscopic gynecological surgery: A randomized controlled trial. J. Anesth. 2018, 32, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Orhun, G.; Sungur, Z.; Koltka, K.; Savran Karadeniz, M.; Yavru, H.A.; Gürvit, H.; Şentürk, M. Comparison of epidural analgesia combined with general anesthesia and general anesthesia for postoperative cognitive dysfunction in elderly patients. Ulus Travma Acil Cerrahi Derg. 2020, 26, 30–36. [Google Scholar]
- Montes, A.; Roca, G.; Sabate, S.; Lao, J.; Navarro, N.; Cantillo, J.; Canet, J.; Ruiz, C.; Delgado, J.; Jimenez, L.; et al. Genetic and Clinical Factors Associated with Chronic Postsurgical Pain after Hernia Repair, Hysterectomy, and Thoracotomy: A Two-year Multicenter Cohort Study. Anesthesiology 2015, 122, 1123–1141. [Google Scholar] [CrossRef] [Green Version]
- Halaszynski, T. Influences of the Aging Process on Acute Perioperative Pain Management in Elderly and Cognitively Impaired Patients. Ochsner J. 2013, 13, 228–247. [Google Scholar] [PubMed]
- Ledowski, T. Objective monitoring of nociception: A review of current commercial solutions. Br. J. Anaesth. 2019, 123, e312–e321. [Google Scholar] [CrossRef] [PubMed]
- Fiore, J.F., Jr.; Olleik, G.; El-Kefraoui, C.; Verdolin, B.; Kouyoumdjian, A.; Alldrit, A.; Figueiredo, A.; Valanci, S.; Marquez-GdeV, J.; Schulz, M.; et al. Preventing opioid prescription after major surgery: A scoping review of opioid-free analgesia. Br. J. Anaesth. 2019, 123, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Bell, R.F.; Dahl, J.B.; Moore, R.A.; Kalso, E. Peri-operative ketamine for acute post-operative pain: A quantitative and qualitative systematic review (Cochrane review). Acta Anaesthesiol. Scand. 2005, 49, 1405–1428. [Google Scholar] [CrossRef] [PubMed]
- Zakine, J.; Samarcq, D.; Lorne, E.; Moubarak, M.; Montravers, P.; Beloucif, S.; Dupont, H. Postoperative ketamine administration decreases morphine consumption in major abdominal surgery: A prospective, randomized, double-blind, controlled study. Anesth. Analg. 2008, 106, 1856–1861. [Google Scholar] [CrossRef]
- De Kock, M.; Lavand’homme, P.; Waterloos, H. ‘Balanced analgesia’ in the perioperative period: Is there a place for ketamine? Pain 2001, 92, 373–380. [Google Scholar] [CrossRef]
- Katz, J.; Schmid, R.; Snijdelaar, D.G.; Coderre, T.J.; McCartney, C.J.L.; Wowk, A. Pre-emptive analgesia using intravenous fentanyl plus low-dose ketamine for radical prostatectomy under general anesthesia does not produce short-term or long-term reductions in pain or analgesic use. Pain 2004, 110, 707–718. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Echevarria, G.C.; Doan, L.; Ekasumara, N.; Calvino, S.; Chae, F.; Martinez, E.; Robinson, E.; Cuffet, G.; Franco, L. Effects of a single subanaesthetic dose of ketamine on pain and mood after laparoscopic bariatric surgery: A randomised double-blind placebo controlled study. Eur. J. Anaesthesiol. 2019, 36, 16–24. [Google Scholar] [CrossRef]
- Kranke, P.; Jokinen, J.; Pace, N.L.; Schnabel, A.; Hollmann, M.; Hahnenkamp, K.; Eberhart, L.; Poepping, D.; Weibel, S. Continuous intravenous perioperative lidocaine infusion for postoperative pain and recovery. Cochrane Database Syst. Rev. 2015, 7, CD009642. [Google Scholar] [CrossRef]
- Tauzin-Fin, P.; Bernard, O.; Sesay, M.; Biais, M.; Richebe, P.; Quinart, A.; Revel, P.; Sztark, F. Benefits of intravenous lidocaine on post-operative pain and acute rehabilitation after laparoscopic nephrectomy. J. Anaesthesiol. Clin. Pharmacol. 2014, 30, 366–372. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, G.S., Jr.; Fitzgerald, P.; Streicher, L.F.; Marcus, R.J.; McCarthy, R.J. Systemic lidocaine to improve postoperative quality of recovery after ambulatory laparoscopic surgery. Anesth. Analg. 2012, 115, 262–267. [Google Scholar] [CrossRef] [Green Version]
- Vigneault, L.; Turgeon, A.F.; Côté, D.; Lauzier, F.; Zarychanski, R.; Moore, L.; McIntyre, L.A.; Nicole, P.C.; Fergusson, D.A. Perioperative intravenous lidocaine infusion for postoperative pain control: A meta-analysis of randomized controlled trials. Can. J. Anaesth. 2011, 58, 22–37. [Google Scholar] [CrossRef] [PubMed]
- Groudine, S.B.; Fisher, H.A.; Kaufman, R.P., Jr.; Patel, M.K.; Wilkins, L.J.; Mehta, S.A.; Lumb, P.D. Intravenous lidocaine speeds the return of bowel function, decreases postoperative pain, and shortens hospital stay in patients undergoing radical retropubic prostatectomy. Anesth. Analg. 1998, 86, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Ghimire, A.; Subedi, A.; Bhattarai, B.; Sah, B.P. The effect of intraoperative lidocaine infusion on opioid consumption and pain after totally extraperitoneal laparoscopic inguinal hernioplasty: A randomized controlled trial. BMC Anesthesiol. 2020, 20, 137. [Google Scholar] [CrossRef] [PubMed]
- Xie, C.; Wang, Q.; Huai, D. Intravenous Infusion of Lidocaine Can Accelerate Postoperative Early Recovery in Patients Undergoing Surgery for Obstructive Sleep Apnea. Med. Sci. Monit. 2021, 27, e926990. [Google Scholar] [CrossRef]
- Grady, M.V.; Mascha, E.; Sessler, D.I.; Kurz, A. The effect of perioperative intravenous lidocaine and ketamine on recovery after abdominal hysterectomy. Anesth. Analg. 2012, 115, 1078–1084. [Google Scholar] [CrossRef]
- Dholakia, U.; Clark-Price, S.C.; Keating, S.C.J.; Stern, A.W. Anesthetic effects and body weight changes associated with ketamine-xylazine-lidocaine administered to CD-1 mice. PLoS ONE 2017, 12, e0184911. [Google Scholar] [CrossRef] [Green Version]
- Kaka, U.; Hui Cheng, C.; Meng, G.Y.; Fakurazi, S.; Kaka, A.; Behan, A.A.; Ebrahimi, M. Electroencephalographic changes associated with antinociceptive actions of lidocaine, ketamine, meloxicam, and morphine administration in minimally anaesthetized dogs. Biomed. Res. Int. 2015, 305367. [Google Scholar] [CrossRef]
- El Sayed Moawad, H.; Mokbel, E.M. Postoperative analgesia after major abdominal surgery: Fentanyl–bupivacaine patient controlled epidural analgesia versus fentanyl patient controlled intravenous analgesia Egypt. J. Anaesth. 2019, 30, 393–397. [Google Scholar] [CrossRef] [Green Version]
- Panousis, P.; Heller, A.R.; Koch, T.; Litz, R.J. Epidural ropivacaine concentrations for intraoperative analgesia during major upper abdominal surgery: A prospective, randomized, double-blinded, placebo-controlled study. Anesth. Analg. 2009, 108, 1971–1976. [Google Scholar] [CrossRef] [PubMed]
- Queiroz-Williams, P.; Doherty, T.J.; da Cunha, A.F.; Leonardi, C. Effects of ketamine and lidocaine in combination on the sevoflurane minimum alveolar concentration in alpacas. Can. J. Vet. Res. 2016, 80, 141–145. [Google Scholar] [PubMed]
- Barak, M.; Ben-Shlomo, I.; Katz, Y. Changes in effective and lethal doses of intravenous anesthetics and lidocaine when used in combination in mice. J. Basic Clin. Physiol. Pharmacol. 2001, 12, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Nakhli, M.S.; Kahloul, M.; Guizani, T.; Zedini, C.; Chaouch, A.; Naija, W. Intravenous lidocaine as adjuvant to general anesthesia in renal surgery. Libyan J. Med. 2018, 13, 1433418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jørgensen, H.; Wetterslev, J.; Møiniche, S.; Dahl, J.B. Epidural local anaesthetics versus opioid-based analgesic regimens on postoperative gastrointestinal paralysis, PONV and pain after abdominal surgery. Cochrane Database Syst. Rev. 2000, 4, CD001893. [Google Scholar]
- Rüsch, D.; Eberhart, L.H.; Wallenborn, J.; Kranke, P. Nausea and vomiting after surgery under general anesthesia: An evidence-based review concerning risk assessment, prevention, and treatment. Dtsch. Arztebl. Int. 2010, 107, 733–741. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control (n = 22) | Co-A (n = 19) | EA (n = 14) | |
|---|---|---|---|
| Poor social status (%) | 36.36 | 40.76 | 60 |
| Female gender (%) | 40.9 | 47.39 | 76.92 |
| Mean age (years) | 52.27 | 61.2 | 69.53 |
| Oncologic surgery (%) | 72.72 | 63.15 | 92.3 |
| Neurological condition (%) | 22.72 | 5.26 | 15.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jipa, M.; Isac, S.; Klimko, A.; Simion-Cotorogea, M.; Martac, C.; Cobilinschi, C.; Droc, G. Opioid-Sparing Analgesia Impacts the Perioperative Anesthetic Management in Major Abdominal Surgery. Medicina 2022, 58, 487. https://doi.org/10.3390/medicina58040487
Jipa M, Isac S, Klimko A, Simion-Cotorogea M, Martac C, Cobilinschi C, Droc G. Opioid-Sparing Analgesia Impacts the Perioperative Anesthetic Management in Major Abdominal Surgery. Medicina. 2022; 58(4):487. https://doi.org/10.3390/medicina58040487
Chicago/Turabian StyleJipa, Miruna, Sebastian Isac, Artsiom Klimko, Mihail Simion-Cotorogea, Cristina Martac, Cristian Cobilinschi, and Gabriela Droc. 2022. "Opioid-Sparing Analgesia Impacts the Perioperative Anesthetic Management in Major Abdominal Surgery" Medicina 58, no. 4: 487. https://doi.org/10.3390/medicina58040487