
Effects of High Intensity Interval Training Rehabilitation Protocol after an Acute Coronary Syndrome on Myocardial Work and Atrial Strain

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Study Protocol
2.3. Standard Doppler Transthoracic Echocardiography
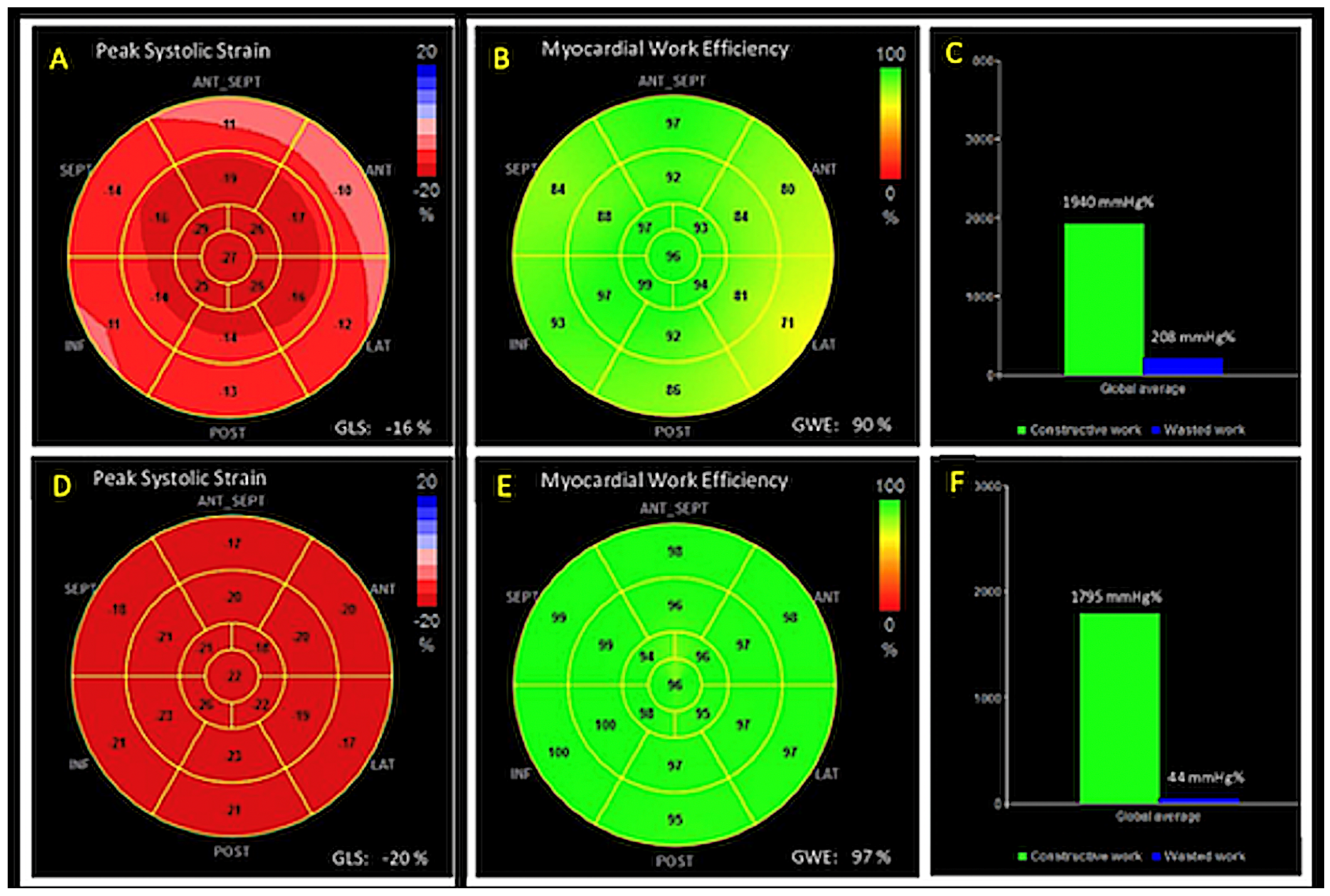
2.4. Two-Dimensional Speckle Tracking Echocardiography (2D-STE)
2.5. MW analysis
2.6. Cardiopulmonary Exercise Testing
2.7. Statistical Analysis
3. Results
Analysis of Intra and Inter-Observer Variability
4. Discussion
4.1. Effects of Cardiac Rehabilitation on Myocardial Function
4.2. Uniqueness of the Present Study
4.3. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ambrosetti, M.; Abreu, A.; Corra, U.; Davos, C.H.; Hansen, D.; Frederix, I.; Iliou, M.C.; Pedretti, R.F.; Schmid, J.P.; Vigorito, C.; et al. Secondary prevention through comprehensive cardiovascular rehabilitation: From knowledge to implementation. 2020 update. A position paper from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2021, 28, 460–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Andrea, A.; Sperlongano, S.; Pacileo, M.; Venturini, E.; Iannuzzo, G.; Gentile, M.; Sperlongano, R.; Vitale, G.; Maglione, M.; Cice, G.; et al. New Ultrasound Technologies for Ischemic Heart Disease Assessment and Monitoring in Cardiac Rehabilitation. J. Clin. Med. 2020, 9, 3131. [Google Scholar] [CrossRef]
- Trachsel, L.D.; David, L.P.; Gayda, M.; Henri, C.; Hayami, D.; Thorin-Trescases, N.; Thorin, E.; Blain, M.A.; Cossette, M.; Lalonge, J.; et al. The impact of high-intensity interval training on ventricular remodeling in patients with a recent acute myocardial infarction-A randomized training intervention pilot study. Clin. Cardiol. 2019, 42, 1222–1231. [Google Scholar] [CrossRef] [Green Version]
- Hannan, A.L.; Hing, W.; Simas, V.; Climstein, M.; Coombes, J.S.; Jayasinghe, R.; Byrnes, J.; Furness, J. High-intensity interval training versus moderate-intensity continuous training within cardiac rehabilitation: A systematic review and meta-analysis. Open Access J. Sports Med. 2018, 9, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Qin, Y.; Wu, X.; Wang, J.; Li, Y.; Ding, X.; Guo, D.; Jiang, Z.; Zhu, W.; Cai, Q.; Lu, X. Value of territorial work efficiency estimation in non-ST-segment-elevation acute coronary syndrome: A study with non-invasive left ventricular pressure-strain loops. Int. J. Cardiovasc. Imaging 2021, 37, 1255–1265. [Google Scholar] [CrossRef]
- Price, K.J.; Gordon, B.A.; Bird, S.R.; Benson, A.C. A review of guidelines for cardiac rehabilitation exercise programmes: Is there an international consensus? Eur. J. Prev. Cardiol. 2016, 23, 1715–1733. [Google Scholar] [CrossRef] [PubMed]
- Woodruffe, S.; Neubeck, L.; Clark, R.A.; Gray, K.; Ferry, C.; Finan, J.; Sanderson, S.; Briffa, T.G. Australian Cardiovascular Health and Rehabilitation Association (ACRA) core components of cardiovascular disease secondary prevention and cardiac rehabilitation 2014. Heart Lung Circ. 2015, 24, 430–441. [Google Scholar] [CrossRef] [PubMed]
- Mezzani, A.; Hamm, L.F.; Jones, A.M.; McBride, P.E.; Moholdt, T.; Stone, J.A.; Urhausen, A.; Williams, M.A. Aerobic exercise intensity assessment and prescription in cardiac rehabilitation: A joint position statement of the European Association for Cardiovascular Prevention and Rehabilitation, the American Association of Cardiovascular and Pulmonary Rehabilitation and the Canadian Association of Cardiac Rehabilitation. Eur. J. Prev. Cardiol. 2013, 20, 442–467. [Google Scholar] [PubMed]
- Zhang, X.; Xu, D.; Sun, G.; Jiang, Z.; Tian, J.; Shan, Q. Effects of high-intensity interval training in patients with coronary artery disease after percutaneous coronary intervention: A systematic review and meta-analysis. Nurs. Open 2021, 8, 1424–1435. [Google Scholar] [CrossRef] [PubMed]
- Scharf, M.; Schmid, A.; Kemmler, W.; von Stengel, S.; May, M.S.; Wuest, W.; Achenbach, S.; Uder, M.; Lell, M.M. Myocardial adaptation to high-intensity (interval) training in previously untrained men with a longitudinal cardiovascular magnetic resonance imaging study (Running Study and Heart Trial). Circ. Cardiovasc. Imaging 2015, 8, e002566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weidemann, F.; Wacker, C.; Rauch, A.; Bauer, W.R.; Bijnens, B.; Sutherland, G.R.; Ertl, G.; Voelker, W.; Fidler, F.; Strotmann, J.M. Sequential changes of myocardial function during acute myocardial infarction, in the early and chronic phase after coronary intervention described by ultrasonic strain rate imaging. J. Am. Soc. Echocardiogr. 2006, 19, 839–847. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Mele, D.; Agricola, E.; Pezzullo, E.; Cameli, M.; Rossi, A.; Esposito, R.; Novo, G.; Mondillo, S.; Montisci, R.; et al. XStrain 4D analysis predicts left ventricular remodeling in patients with recent non-ST-segment elevation myocardial infarction. Int. J. Cardiol. 2016, 206, 107–109. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Cocchia, R.; Caso, P.; Riegler, L.; Scarafile, R.; Salerno, G.; Golia, E.; Di Salvo, G.; Calabro, P.; Bigazzi, M.C.; et al. Global longitudinal speckle-tracking strain is predictive of left ventricular remodeling after coronary angioplasty in patients with recent non-ST elevation myocardial infarction. Int. J. Cardiol. 2011, 153, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Antoni, M.L.; Mollema, S.A.; Atary, J.Z.; Borleffs, C.J.; Boersma, E.; van de Veire, N.R.; Holman, E.R.; van der Wall, E.E.; Schalij, M.J.; Bax, J.J. Time course of global left ventricular strain after acute myocardial infarction. Eur. Heart J. 2010, 31, 2006–2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGregor, G.; Stöhr, E.J.; Oxborough, D.; Kimani, P.; Shave, R. Effect of exercise training on left ventricular mechanics after acute myocardial infarction-an exploratory study. Ann Phys Rehabil Med. 2018, 61, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Angadi, S.S.; Jarrett, C.L.; Sherif, M.; Gaesser, G.A.; Mookadam, F. The effect of exercise training on biventricular myocardial strain in heart failure with preserved ejection fraction. ESC Heart Fail. 2017, 4, 356–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malfatto, G.; Revera, M.; Branzi, G.; Ciambellotti, F.; Giglio, A.; Blengino, S.; Oldani, M.; Facchini, C.; Parati, G.; Facchini, M. A brief period of intensive cardiac rehabilitation improves global longitudinal strain and diastolic function after a first uncomplicated myocardial infarction. Acta Cardiol. 2017, 72, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Lustosa, R.P.; van der Bijl, P.; El Mahdiui, M.; Montero-Cabezas, J.M.; Kostyukevich, M.V.; Ajmone Marsan, N.; Bax, J.J.; Delgado, V. Noninvasive Myocardial Work Indices 3 Months after ST-Segment Elevation Myocardial Infarction: Prevalence and Characteristics of Patients with Postinfarction Cardiac Remodeling. J. Am. Soc. Echocardiogr. 2020, 33, 1172–1179. [Google Scholar] [CrossRef] [PubMed]
- Meimoun, P.; Abdani, S.; Stracchi, V.; Elmkies, F.; Boulanger, J.; Botoro, T.; Zemir, H.; Clerc, J. Usefulness of Noninvasive Myocardial Work to Predict Left Ventricular Recovery and Acute Complications after Acute Anterior Myocardial Infarction Treated by Percutaneous Coronary Intervention. J. Am. Soc. Echocardiogr. 2020, 33, 1180–1190. [Google Scholar] [CrossRef] [PubMed]



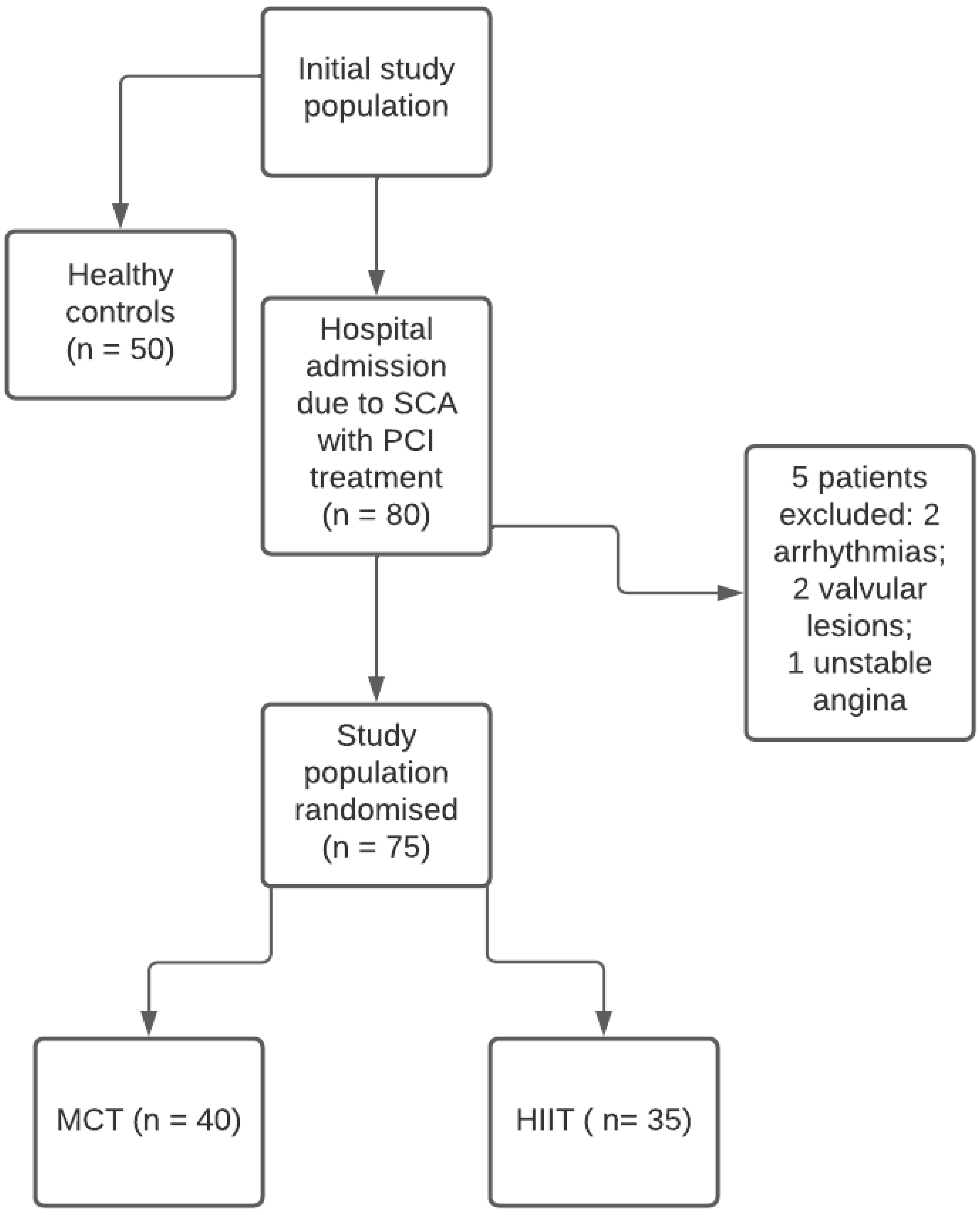{kind=link}
{kind=link}
| Variable | Ischemic Patients (n = 75) | Controls (n = 50) | p-Value |
|---|---|---|---|
| Male sex (%) | 43 (57.5) | 30 (60) | NS |
| Age (years) | 62.3 ± 8.3 | 59.3 ± 15.4 | NS |
| BSA (m2) | 1.87 ± 0.17 | 1.85 ± 0.15 | NS |
| BMI (kg/m2) | 27.9 ± 3.6 | 25.2 ± 3.4 | NS |
| Systolic blood pressure (mmHg) | 133.5 ± 6.4 | 125.4 ± 5.8 | <0.01 |
| Diastolic blood pressure (mmHg) | 85.4 ± 12.2 | 78.3 ± 9.2 | <0.05 |
| Heart rate (b/m) | 78.4 ± 12.3 | 76.4 ± 11.4 | NS |
| Arterial hypertension (%) | 19 (25.5) | - | - |
| Diabetes mellitus (%) | 31 (41.2) | - | - |
| Smoking or history of smoking (%) | 33 (44.4) | - | - |
| Hyperlipidemia (%) | 42 (56.6) | - | - |
| Beta-blockers (%) | 65 (86.4) | - | - |
| ACE inhibitors or ARB (%) | 58 (77.3) | - | - |
| Aldosterone receptor antagonists (%) | 14 (18.5) | - | - |
| Antiplatelet agents/oral anticoagulants (%) | 75 (100) | - | - |
| Diuretics (%) | 27 (35.8) | - | - |
| Variable | Ischemic Patients | Controls | p-Value |
|---|---|---|---|
| Ischemic Patients (n = 75) | Controls (n = 50) | ||
| IVSd (mm) | 11.8 ± 2.8 | 8.1 ± 2.3 | <0.01 |
| PWd (mm) | 10.8 ± 1.6 | 7.7 ± 2.1 | <0.01 |
| LVEDD (mm) | 53.3 ± 4.2 | 48.4 ± 5.6 | <0.01 |
| LVESD (mm) | 47.4 ± 5.2 | 34.6 ± 4.8 | <0.01 |
| LV mass index (g/m2) | 142.5 ± 22.3 | 80.5 ± 14.4 | <0.0001 |
| LVEDV index (mL/m2) | 69.4 ± 11.4 | 60.6 ± 8.3 | <0.01 |
| LVESV index (mL/m2) | 37.5 ± 12.3 | 24.5 ± 9.9 | <0.001 |
| Biplane LVEF (%) | 47.1 ± 6.1 | 56.3 ± 5.5 | <0.0001 |
| LV GLS (%) | −12.8 ± 2.8 | −21.4 ± 4.4 | <0.0001 |
| Myocardial Work Efficiency (%) | 82.1 ± 3.3 | 94.4 ± 4.1 | <0.001 |
| Myocardial Wasted Work (%) | 17.9 ± 4.4 | 5.8 ± 3.8 | <0.0001 |
| Mitral E velocity (m/s) | 0.9 ± 0.6 | 0.8 ± 0.4 | NS |
| Mitral A velocity (m/s) | 0.7 ± 0.4 | 0.7 ± 0.3 | NS |
| E/A ratio | 1.3 ± 0.4 | 1.1 ± 0.4 | NS |
| Mitral septal E’ velocity (m/s) | 0.13 ± 0.05 | 0.16 ± 0.05 | <0.01 |
| Mitral lateral E’ velocity (m/s) | 0.14 ± 0.04 | 0.18 ± 0.03 | <0.01 |
| E/e’ratio | 9.9 ± 3.1 | 4.9 ± 2.8 | <0.001 |
| Aortic root diameter (mm) | 34.3 ± 4.8 | 30.2 ± 3.2 | <0.01 |
| LAVI (mL/m2) | 33.4 ± 4.1 | 28.3 ± 5.1 | <0.01 |
| LA Strain (%) | 43.3 ± 4.1 | 53.8 ± 5.1 | <0.001 |
| PASP (mmHg) | 37.5 ± 7.8 | 21.3 ± 2.9 | <0.001 |
| TAPSE (mm) | 18.5 ± 3.3 | 24.5 ± 3.8 | <0.01 |
| Tricuspid S’ velocity (cm/s) | 11.3 ± 2.2 | 14.4 ± 3.1 | <0.01 |
| B-lines (median and IQR) | 1.45 (0–35) | 0.70 (0–25) | <0.001 |
| Variable | Baseline | After Rehabilitation | p-Value |
|---|---|---|---|
| Ischemic Patients (n = 75) | |||
| Baseline | After Rehabilitation | ||
| IVSd (mm) | 11.8 ± 2.8 | 10.9 ± 2.3 | NS |
| PWd (mm) | 10.8 ± 1.6 | 10.2 ± 2.1 | NS |
| LVEDD (mm) | 53.3 ± 4.2 | 54.4 ± 6.6 | NS |
| LVESD (mm) | 47.4 ± 5.2 | 41.6 ± 5.8 | <0.01 |
| LV mass index (g/m2) | 142.5 ± 22.3 | 136.5 ± 13.4 | NS |
| LVEDV index (mL/m2) | 69.4 ± 11.4 | 70.6 ± 8.3 | NS |
| LVESV index (mL/m2) | 37.5 ± 12.3 | 33.5 ± 9.6 | <0.01 |
| Biplane LVEF (%) | 47.1 ± 6.1 | 52.3 ± 5.5 | <0.01 |
| LV GLS (%) | −12.8 ± 2.8 | −16.4 ± 4.3 | <0.001 |
| Myocardial Work Efficiency (%) | 82.1 ± 3.3 | 89.4 ± 4.1 | < 0.001 |
| Myocardial Wasted Work (%) | 17.9 ± 4.4 | 10.6 ± 3.3 | <0.0001 |
| Mitral E velocity (m/s) | 0.9 ± 0.6 | 0.7 ± 0.4 | NS |
| Mitral A velocity (m/s) | 0.7 ± 0.4 | 0.9 ± 0.3 | NS |
| E/A ratio | 1.3 ± 0.4 | 0.7 ± 0.5 | <0.01 |
| Mitral septal E’ velocity (m/s) | 0.13 ± 0.05 | 0.15 ± 0.05 | <0.01 |
| Mitral lateral E’ velocity (m/s) | 0.14 ± 0.04 | 0.17 ± 0.03 | <0.01 |
| E/e’ratio | 9.9 ± 3.1 | 4.4 ± 2.8 | <0.001 |
| Aortic root diameter (mm) | 34.3 ± 4.8 | 34.2 ± 3.2 | NS |
| LAVI (mL/m2) | 33.4 ± 4.1 | 30.3.3 ± 5.1 | <0.01 |
| LA Strain (%) | 43.3 ± 4.1 | 47.3 ± 5.4 | <0.01 |
| PASP (mmHg) | 37.5 ± 7.8 | 30.3 ± 2.9 | <0.01 |
| TAPSE (mm) | 18.5 ± 3.3 | 19.5 ± 3.8 | NS |
| Tricuspid S’ velocity (cm/s) | 11.3 ± 2.2 | 12.4 ± 3.1 | NS |
| B-lines (median and IQR) | 1.45 (0–35) | 0.90 (0–25) | <0.001 |
| Variable | HIIT | MCT | p-Value |
|---|---|---|---|
| HIIT (35 pts) | MCT (40 pts) | ||
| IVSd (mm) | 10.5 ± 2.9 | 11.1 ± 2.3 | NS |
| PWd (mm) | 10.2 ± 1.6 | 10.1 ± 2.1 | NS |
| LVEDD (mm) | 53.9 ± 4.2 | 54.8 ± 6.6 | NS |
| LVESD (mm) | 40.4 ± 6.2 | 43.6 ± 5.6 | <0.05 |
| LV mass index (g/m2) | 133.5 ± 22.5 | 137.5 ± 12.4 | NS |
| LVEDV index (mL/m2) | 68.6 ± 11.2 | 71.2 ± 7.3 | NS |
| LVESV index (mL/m2) | 31.5 ± 11.3 | 35.6 ± 8.6 | <0.01 |
| Biplane LVEF (%) | 53.1 ± 6.4 | 52.3 ± 5.4 | <0.01 |
| LV GLS (%) | −17.8 ± 3.8 | −15.4 ± 4.3 | <0.01 |
| Myocardial Work Efficiency (%) | 91.1 ± 3.3 | 87.4 ± 4.1 | <0.01 |
| Myocardial Wasted Work (%) | 9.9 ± 4.4 | 12.6 ± 3.3 | <0.01 |
| Mitral E velocity (m/s) | 0.8 ± 0.6 | 0.7 ± 0.4 | NS |
| Mitral A velocity (m/s) | 0.9 ± 0.4 | 0.8 ± 0.3 | NS |
| E/A ratio | 0.88 ± 0.4 | 0.87.1 ± 0.5 | NS |
| Mitral septal E’ velocity (m/s) | 0.16 ± 0.05 | 0.14 ± 0.05 | <0.01 |
| Mitral lateral E’ velocity (m/s) | 0.18 ± 0.04 | 0.15 ± 0.03 | <0.01 |
| E/e’ratio | 3.4 ± 3.1 | 6.4 ± 2.8 | <0.01 |
| Aortic root diameter (mm) | 34.2 ± 3.8 | 34.2 ± 3.1 | NS |
| LAVI (mL/m2) | 29.4 ± 3.8 | 32.3 ± 4.1 | <0.01 |
| LA Strain (%) | 49.2 ± 3.9 | 43.6 ± 4.1 | <0.01 |
| PASP (mmHg) | 28.5 ± 7.8 | 33.3 ± 2.9 | <0.01 |
| TAPSE (mm) | 19.5 ± 3.3 | 19.2 ± 3.7 | NS |
| Tricuspid S’ velocity (cm/s) | 12.7 ± 2.2 | 12.2 ± 3.1 | NS |
| B-lines (median and IQR) | 0.87 (0–27) | 0.91 (1–25) | NS |
| Variable | R | p Value | |
|---|---|---|---|
| LV EF | VO2 Peak | 0.21 | NS |
| LV E/e’ during ESE | −0.31 | <0.05 | |
| B lines during ESE | −0.2 | NS | |
| LV GLS | VO2 Peak | −0.40 | <0.01 |
| LV E/e’ during ESE | 0.33 | <0.05 | |
| B lines during ESE | 0.23 | NS | |
| LA Strain | VO2 Peak | 0.36 | <0.01 |
| LV E/e’ during ESE | −0.36 | <0.01 | |
| B lines during ESE | −0.28 | <0.05 | |
| LV MWE | VO2 Peak | 0.52 | <0.001 |
| LV E/e’ during ESE | −0.49 | <0.001 | |
| B lines during ESE | −0.39 | <0.01 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Andrea, A.; Carbone, A.; Ilardi, F.; Pacileo, M.; Savarese, C.; Sperlongano, S.; Di Maio, M.; Giallauria, F.; Russo, V.; Bossone, E.; et al. Effects of High Intensity Interval Training Rehabilitation Protocol after an Acute Coronary Syndrome on Myocardial Work and Atrial Strain. Medicina 2022, 58, 453. https://doi.org/10.3390/medicina58030453
D’Andrea A, Carbone A, Ilardi F, Pacileo M, Savarese C, Sperlongano S, Di Maio M, Giallauria F, Russo V, Bossone E, et al. Effects of High Intensity Interval Training Rehabilitation Protocol after an Acute Coronary Syndrome on Myocardial Work and Atrial Strain. Medicina. 2022; 58(3):453. https://doi.org/10.3390/medicina58030453
Chicago/Turabian StyleD’Andrea, Antonello, Andreina Carbone, Federica Ilardi, Mario Pacileo, Cristina Savarese, Simona Sperlongano, Marco Di Maio, Francesco Giallauria, Vincenzo Russo, Eduardo Bossone, and et al. 2022. "Effects of High Intensity Interval Training Rehabilitation Protocol after an Acute Coronary Syndrome on Myocardial Work and Atrial Strain" Medicina 58, no. 3: 453. https://doi.org/10.3390/medicina58030453