
Atrial Fibrillation and Dementia: Epidemiological Insights on an Undervalued Association

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
- -
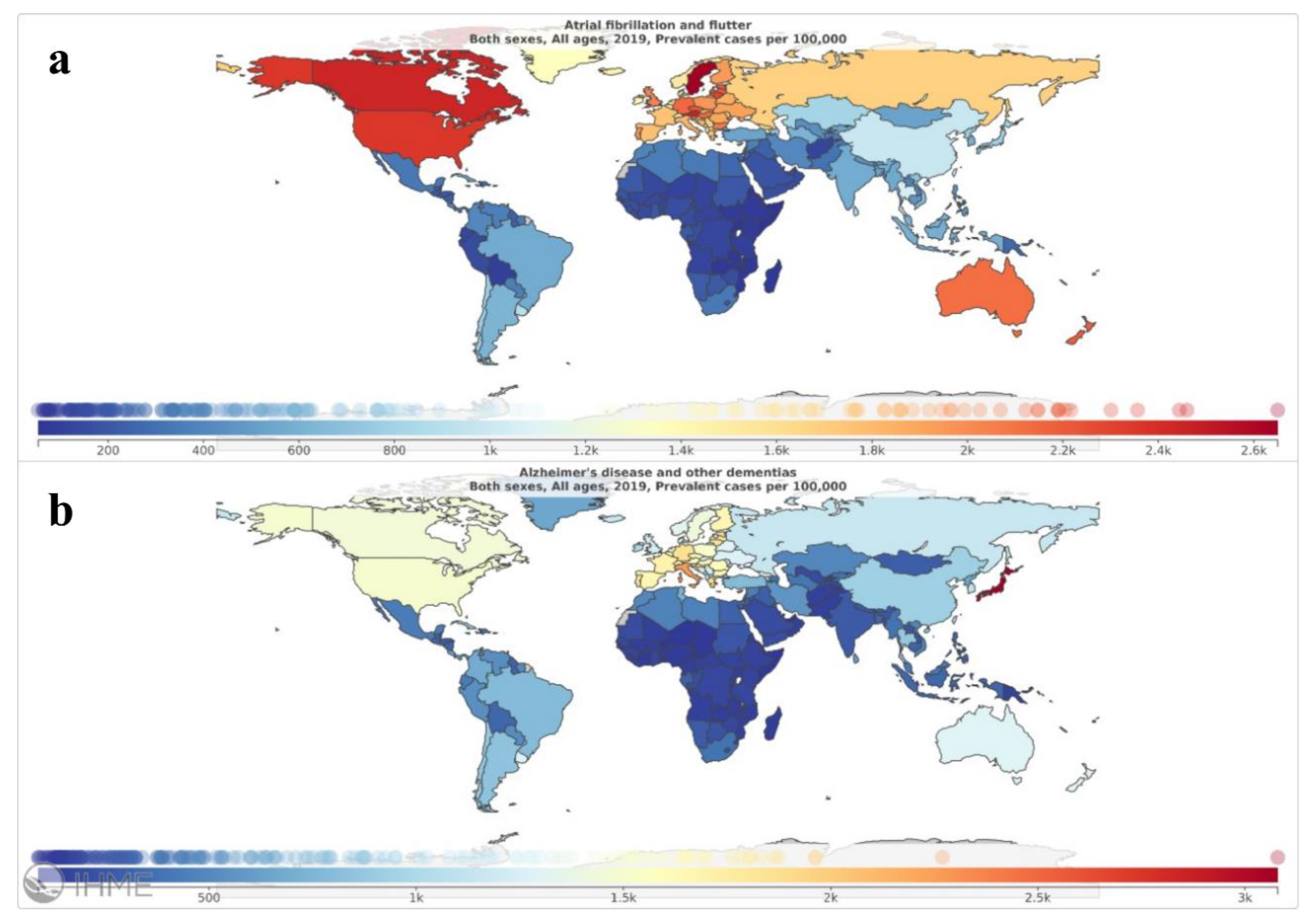
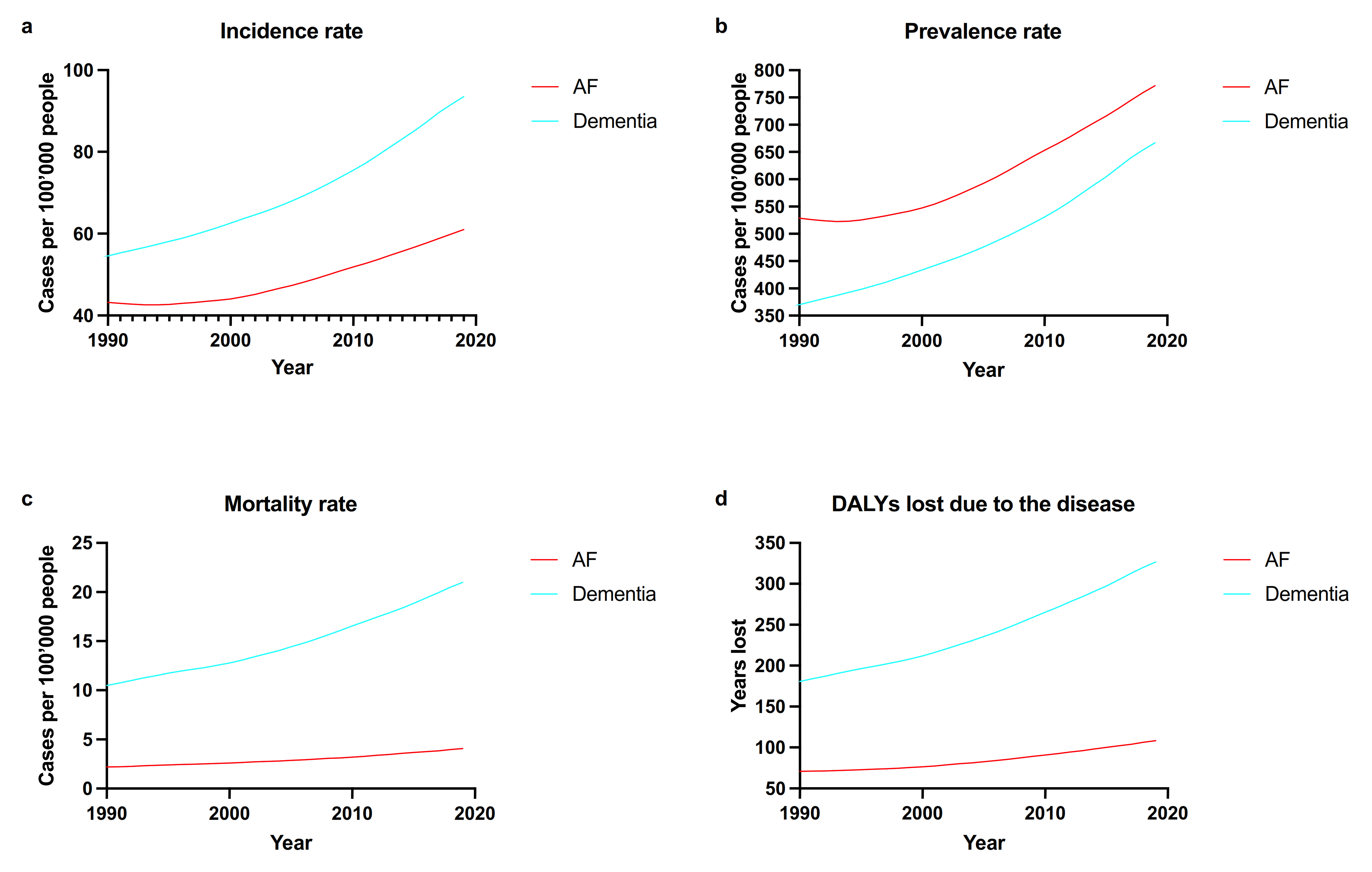
- Incidence rate: number of new cases diagnosed (per 100,000 people);
- -
- Prevalence rate: number of patients affected by the disease (per 100,000 people);
- -
- Mortality rate: number of deaths due to the specific disease (per 100,000 people);
- -
- Disability-adjusted life years (DALYs): sum of years lost due to premature death and years lived with disability (per 100,000 people)
- -
- “All-ages” (crude) and “age-standardized” estimates were reported for incidence and prevalence data. Concerning mortality rate, the “all-ages” (crude) estimate was reported, along with the percentage impact of the cause-specific mortality rate on the overall mortality rate in the population. Finally, regarding DALYs data, we reported the “all-ages” (crude) estimate, as well as the percentage of the cause-specific DALYs on the overall DALYs in the worldwide population. We only reported point estimates, whereas uncertainty interval can be found at GBD Results tool (http://ghdx.healthdata.org/gbd-results-tool, accessed on 12 November 2021). We also provide specific subgroup data pertaining to low and high socio-demographic index (SDI) countries, to assess potential difference in AF and dementia epidemiology according to different socio-demographic scenarios.
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart disease and stroke statistics—2019 update: A report from the American heart association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef] [PubMed]
- Atrial Fibrillation and Flutter—Level 3 Cause. Available online: https://www.thelancet.com/pb-assets/Lancet/gbd/summaries/diseases/atrial-fibrillation.pdf (accessed on 12 November 2021).
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s Disease and Other Dementias—Level 3 Cause. Available online: https://www.thelancet.com/pb-assets/Lancet/gbd/summaries/diseases/alzheimers-dementias.pdf (accessed on 12 November 2021).
- Ferri, C.P.; Prince, M.; Brayne, C.; Brodaty, H.; Fratiglioni, L.; Ganguli, M.; Hall, K.; Hasegawa, K.; Hendrie, H.; Huang, Y.; et al. Global prevalence of dementia: A Delphi consensus study. Lancet 2005, 366, 2112–2117. [Google Scholar] [CrossRef]
- Hurd, M.D.; Martorell, P.; Delavande, A.; Mullen, K.J.; Langa, K. Monetary Costs of Dementia in the United States. New Engl. J. Med. 2013, 368, 1326–1334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunch, T.J. Atrial Fibrillation and Dementia. Circulation 2020, 142, 618–620. [Google Scholar] [CrossRef] [PubMed]
- Anselmino, M.; Scarsoglio, S.; Saglietto, A.; Gaita, F.; Ridolfi, L. Transient cerebral hypoperfusion and hypertensive events during atrial fibrillation: A plausible mechanism for cognitive impairment. Sci. Rep. 2016, 6, 28635. [Google Scholar] [CrossRef]
- Saglietto, A.; Scarsoglio, S.; Ridolfi, L.; Gaita, F.; Anselmino, M. Higher ventricular rate during atrial fibrillation relates to increased cerebral hypoperfusions and hypertensive events. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saglietto, A.; Scarsoglio, S.; Canova, D.; Roatta, S.; Gianotto, N.; Piccotti, A.; Franzin, S.; Gaita, F.; de Ferrari, G.M.; Ridolfi, L.; et al. Increased beat-to-beat variability of cerebral microcirculatory perfusion during atrial fibrillation: A near-infrared spectroscopy study. EP Eur. 2021, 23, 1219–1226. [Google Scholar] [CrossRef]
- Chen, L.Y.; Lopez, F.L.; Gottesman, R.F.; Huxley, R.R.; Agarwal, S.K.; Loehr, L.; Mosley, T.; Alonso, A. Atrial fibrillation and cognitive decline-the role of subclinical cerebral infarcts. Stroke 2014, 45, 2568–2574. [Google Scholar] [CrossRef] [Green Version]
- Gaita, F.; Corsinovi, L.; Anselmino, M.; Raimondo, C.; Pianelli, M.; Toso, E.; Bergamasco, L.; Boffano, C.; Valentini, M.C.; Cesarani, F.; et al. Prevalence of Silent Cerebral Ischemia in Paroxysmal and Persistent Atrial Fibrillation and Correlation with Cognitive Function. J. Am. Coll. Cardiol. 2013, 62, 1990–1997. [Google Scholar] [CrossRef] [Green Version]
- Junejo, R.T.; Braz, I.D.; Lucas, S.; van Lieshout, J.J.; Lip, G.Y.; Fisher, J.P. Impaired Cerebrovascular Reactivity in Patients with Atrial Fibrillation. J. Am. Coll. Cardiol. 2019, 73, 1230–1232. [Google Scholar] [CrossRef] [PubMed]
- Conen, D.; Rodondi, N.; Müller, A.; Beer, J.H.; Ammann, P.; Moschovitis, G.; Auricchio, A.; Hayoz, D.; Kobza, R.; Shah, D.; et al. Relationships of Overt and Silent Brain Lesions with Cognitive Function in Patients With Atrial Fibrillation. J. Am. Coll. Cardiol. 2019, 73, 989–999. [Google Scholar] [CrossRef] [PubMed]
- Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Vos, T.; Lim, S.S.; Aynalem, Y.A.; Azari, S.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analy-sis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
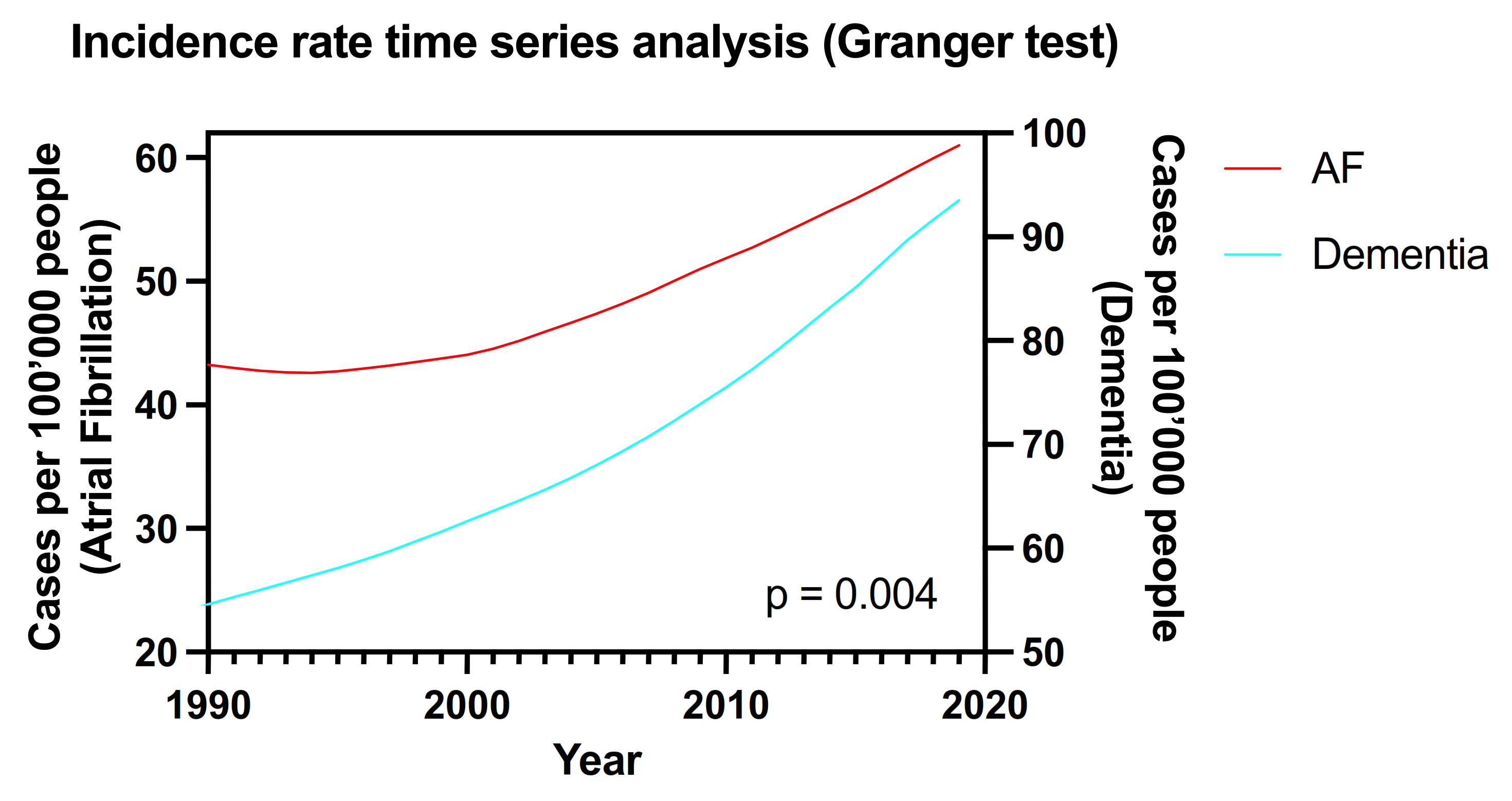
- Granger, C.W.J. Investigating Causal Relations by Econometric Models and Cross-spectral Methods. Econometrica 1969, 37, 424–438. [Google Scholar] [CrossRef]
- Zeileis, A.; Torsten, H. Diagnostic Checking in Regression Relationships. R News 2002, 2, 7–10. [Google Scholar]
- Ott, A.; Breteler, M.M.; de Bruyne, M.C.; van Harskamp, F.; Grobbee, D.E.; Hofman, A. Atrial Fibrillation and Dementia in a Population-Based Study. Stroke 1997, 28, 316–321. [Google Scholar] [CrossRef]
- Kottkamp, H. Fibrotic Atrial Cardiomyopathy: A Specific Disease/Syndrome Supplying Substrates for Atrial Fibrillation, Atrial Tachycardia, Sinus Node Disease, AV Node Disease, and Thromboembolic Complications. J. Cardiovasc. Electrophysiol. 2012, 23, 797–799. [Google Scholar] [CrossRef]
- Marrouche, N.F.; Wilber, D.; Hindricks, G.; Jais, P.; Akoum, N.; Marchlinski, F.; Kholmovski, E.; Burgon, N.; Hu, N.; Mont, L.; et al. Association of Atrial Tissue Fibrosis Identified by Delayed Enhancement MRI and Atrial Fibrillation Catheter Ablation. JAMA 2014, 311, 498–506. [Google Scholar] [CrossRef]
- Bayés-De-Luna, A.; Martínez-Sellés, M.; Elosua, R.; Bayes-Genis, A.; Mendieta, G.; Baranchuk, A.; Breithardt, G. Relation of Advanced Interatrial Block to Risk of Atrial Fibrillation and Stroke. Am. J. Cardiol. 2020, 125, 1745–1748. [Google Scholar] [CrossRef]
- Martínez-Sellés, M.; Elosua, R.; Ibarrola, M.; de Andrés, M.; Díez-Villanueva, P.; Bayes-Genis, A.; Baranchuk, A.; Bayés-De-Luna, A.; BAYES Registry Investigators. Advanced interatrial block and P-wave duration are associated with atrial fibrillation and stroke in older adults with heart disease: The BAYES registry. Europace 2020, 22, 1001–1008. [Google Scholar] [CrossRef]
- Martínez-Sellés, M.; Martínez-Larrú, M.E.; Ibarrola, M.; Santos, A.; Díez-Villanueva, P.; Bayés-Genis, A.; Baranchuk, A.; Bayés-De-Luna, A.; Elosua, R. Interatrial block and cognitive impairment in the BAYES prospective registry. Int. J. Cardiol. 2020, 321, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Saglietto, A.; Matta, M.; Gaita, F.; Jacobs, V.; Bunch, T.J.; Anselmino, M. Stroke-independent contribution of atrial fibrillation to dementia: A meta-analysis. Open Hear. 2019, 6, e000984. [Google Scholar] [CrossRef]
- Kwok, C.S.; Loke, Y.K.; Hale, R.; Potter, J.F.; Myint, P.K. Atrial fibrillation and incidence of dementia: A systematic review and meta-analysis. Neurology 2011, 76, 914–922. [Google Scholar] [CrossRef] [PubMed]
- Bruijn, R.F.A.G.D.; Ikram, M.A. Cardiovascular risk factors and future risk of Alzheimer’s disease. BMC Med. 2014, 12, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Silva, R.M.F.L.; Miranda, C.M.; Liu, T.; Tse, G.; Roever, L. Atrial Fibrillation and Risk of Dementia: Epidemiology, Mechanisms, and Effect of Anticoagulation. Front. Neurosci. 2019, 13, 18. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.; Lip, G.Y.; Apostolakis, S. Inflammation in Atrial Fibrillation. J. Am. Coll. Cardiol. 2012, 60, 2263–2270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaur, C.; Ling, E. Blood Brain Barrier in Hypoxic-Ischemic Conditions. Curr. Neurovascular Res. 2008, 5, 71–81. [Google Scholar] [CrossRef]
- Engelhardt, S.; Patkar, S.; Ogunshola, O. Cell-specific blood-brain barrier regulation in health and disease: A focus on hypoxia. J. Cereb. Blood Flow Metab. 2014, 171, 1210–1230. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.E.; Farr, S.A. The role of amyloid-beta in the regulation of memory. Biochem. Pharmacol. 2014, 88, 479–485. [Google Scholar] [CrossRef]
- Ovbiagele, B.; Saver, J.L.; Sanossian, N.; Salamon, N.; Villablanca, P.; Alger, J.R.; Razinia, T.; Kim, O.; Liebeskind, D.S. Predictors of Cerebral Microbleeds in Acute Ischemic Stroke and TIA Patients. Cerebrovasc. Dis. 2006, 22, 378–383. [Google Scholar] [CrossRef]
- Van Norden, A.G.; Berg, H.A.V.D.; de Laat, K.F.; Gons, R.A.; van Dijk, E.J.; de Leeuw, F.-E. Frontal and Temporal Microbleeds Are Related to Cognitive Function: The Radboud University Nijmegen Diffusion Tensor and Magnetic Resonance Cohort (RUN DMC) Study. Stroke 2011, 42, 3382–3386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Upshaw, C.B. Hemodynamic Changes After Cardioversion of Chronic Atrial Fibrillation. Arch. Intern. Med. 1997, 157, 1070–1076. [Google Scholar] [CrossRef]
- De La Torre, J.C. Cardiovascular Risk Factors Promote Brain Hypoperfusion Leading to Cognitive Decline and Dementia. Cardiovasc. Psychiatry Neurol. 2012, 2012, 1–15. [Google Scholar] [CrossRef]
- Lavy, S.; Stern, S.; Melamed, E.; Cooper, G.; Keren, A.; Levy, P. Effect of chronic atrial fibrillation on regional cerebral blood flow. Stroke 1980, 11, 35–38. [Google Scholar] [CrossRef] [Green Version]
- Gardarsdottir, M.; Sigurdsson, S.; Aspelund, T.; Rokita, H.; Launer, L.J.; Gudnason, V.; Arnar, D.O. Atrial fibrilla-tion is asso-ciated with decreased total cerebral blood flow and brain perfusion. Europace 2018, 20, 1252–1258. [Google Scholar] [CrossRef] [PubMed]
- Packer, D.L.; Mark, D.B.; Robb, R.A.; Monahan, K.H.; Bahnson, T.D.; Poole, J.E.; Noseworthy, P.A.; Rosenberg, Y.D.; Jeffries, N.; Mitchell, L.B.; et al. Effect of Catheter Ablation vs Antiarrhythmic Drug Therapy on Mortality, Stroke, Bleeding, and Cardiac Arrest Among Patients with Atrial Fibrillation. JAMA J. Am. Med. Assoc. 2019, 55902, 1261–1274. [Google Scholar] [CrossRef]
- Kim, D.; Yang, P.-S.; Sung, J.-H.; Jang, E.; Yu, H.T.; Kim, T.-H.; Uhm, J.-S.; Kim, J.-Y.; Pak, H.-N.; Lee, M.-H.; et al. Less dementia after catheter ablation for atrial fibrillation: A nationwide cohort study. Eur. Hear. J. 2020, 41, 4483–4493. [Google Scholar] [CrossRef]
- Hsieh, Y.-C.; Chen, Y.-Y.; Chien, K.-L.; Chung, F.-P.; Lo, L.-W.; Chang, S.-L.; Chao, T.-F.; Hu, Y.-F.; Lin, C.-Y.; Tuan, T.-C.; et al. Catheter ablation of atrial fibrillation reduces the risk of dementia and hospitalization during a very long-term follow-up. Int. J. Cardiol. 2020, 304, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Jin, M.-N.; Kim, T.-H.; Kang, K.-W.; Yu, H.T.; Uhm, J.-S.; Joung, B.; Lee, M.-H.; Kim, E.; Pak, H.-N. Atrial Fibrillation Catheter Ablation Improves 1-Year Follow-Up Cognitive Function, Especially in Patients with Impaired Cognitive Function. Circ. Arrhythm. Electrophysiol. 2019, 12, e007197. [Google Scholar] [CrossRef]
- Bunch, T.J.; Bair, T.L.; Crandall, B.G.; Cutler, M.J.; Day, J.D.; Graves, K.G.; Jacobs, V.; Mallender, C.; Osborn, J.S.; Weiss, J.P.; et al. Stroke and dementia risk in patients with and without atrial fibrillation and carotid arterial disease. Hear. Rhythm 2020, 17, 20–26. [Google Scholar] [CrossRef]
- Bunch, T.J.; Crandall, B.G.; Weiss, J.P.; May, H.; Bair, T.L.; Osborn, J.S.; Anderson, J.L.; Muhlestein, J.B.; Horne, B.D.; Lappe, D.L.; et al. Patients Treated with Catheter Ablation for Atrial Fibrillation Have Long-Term Rates of Death, Stroke, and Dementia Similar to Patients Without Atrial Fibrillation. J. Cardiovasc. Electrophysiol. 2011, 22, 839–845. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measure | Crude Estimate (Per 100,000 Individuals) | Age-Standardized Estimate (Per 100,000 Individuals) | Percentage on Total Deaths or DALYs |
|---|---|---|---|
| AF | |||
| Incidence rate | 61.01 | 57.09 | NA |
| Prevalence rate | 771.51 | 743.47 | NA |
| Mortality rate | 4.08 | 4.38 | 0.56% |
| DALYs | 108.48 | 107.13 | 0.33% |
| Dementia | |||
| Incidence rate | 93.52 | 94.99 | NA |
| Prevalence rate | 667.20 | 682.48 | NA |
| Mortality rate | 20.98 | 22.92 | 2.87% |
| DALYs | 326.68 | 338.64 | 1.00% |
| Measure | Crude Estimate (Per 100,000 Individuals) | Age-Standardized Estimate (Per 100,000 Individuals) | Percentage on Total Deaths or DALYs |
|---|---|---|---|
| AF | |||
| Incidence rate | |||
| Low SDI | 18.37 | 41.97 | NA |
| High SDI | 121.89 | 69.22 | NA |
| Prevalence rate | |||
| Low SDI | 199.58 | 514.20 | NA |
| High SDI | 1733.59 | 895.72 | NA |
| Mortality rate | |||
| Low SDI | 1.17 | 4.30 | 0.17% |
| High SDI | 10.85 | 4.61 | 1.24% |
| DALYs | |||
| Low SDI | 32.86 | 91.91 | 0.07% |
| High SDI | 248.40 | 122.64 | 0.84% |
| Dementia | |||
| Incidence rate | |||
| Low SDI | 24.23 | 76.97 | NA |
| High SDI | 219.65 | 100.57 | NA |
| Prevalence rate | |||
| Low SDI | 161.94 | 514.75 | NA |
| High SDI | 1598.23 | 721.43 | NA |
| Mortality rate | |||
| Low SDI | 5.50 | 23.03 | 0.80% |
| High SDI | 55.58 | 22.66 | 6.3% |
| DALYs | |||
| Low SDI | 93.13 | 315.76 | 0.20% |
| High SDI | 755.44 | 332.40 | 2.56% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saglietto, A.; Ballatore, A.; Xhakupi, H.; De Ferrari, G.M.; Anselmino, M. Atrial Fibrillation and Dementia: Epidemiological Insights on an Undervalued Association. Medicina 2022, 58, 361. https://doi.org/10.3390/medicina58030361
Saglietto A, Ballatore A, Xhakupi H, De Ferrari GM, Anselmino M. Atrial Fibrillation and Dementia: Epidemiological Insights on an Undervalued Association. Medicina. 2022; 58(3):361. https://doi.org/10.3390/medicina58030361
Chicago/Turabian StyleSaglietto, Andrea, Andrea Ballatore, Henri Xhakupi, Gaetano Maria De Ferrari, and Matteo Anselmino. 2022. "Atrial Fibrillation and Dementia: Epidemiological Insights on an Undervalued Association" Medicina 58, no. 3: 361. https://doi.org/10.3390/medicina58030361