
Assessment of Therapeutic Responses Using a Deep Neural Network Based on 18F-FDG PET and Blood Inflammatory Markers in Pyogenic Vertebral Osteomyelitis


Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
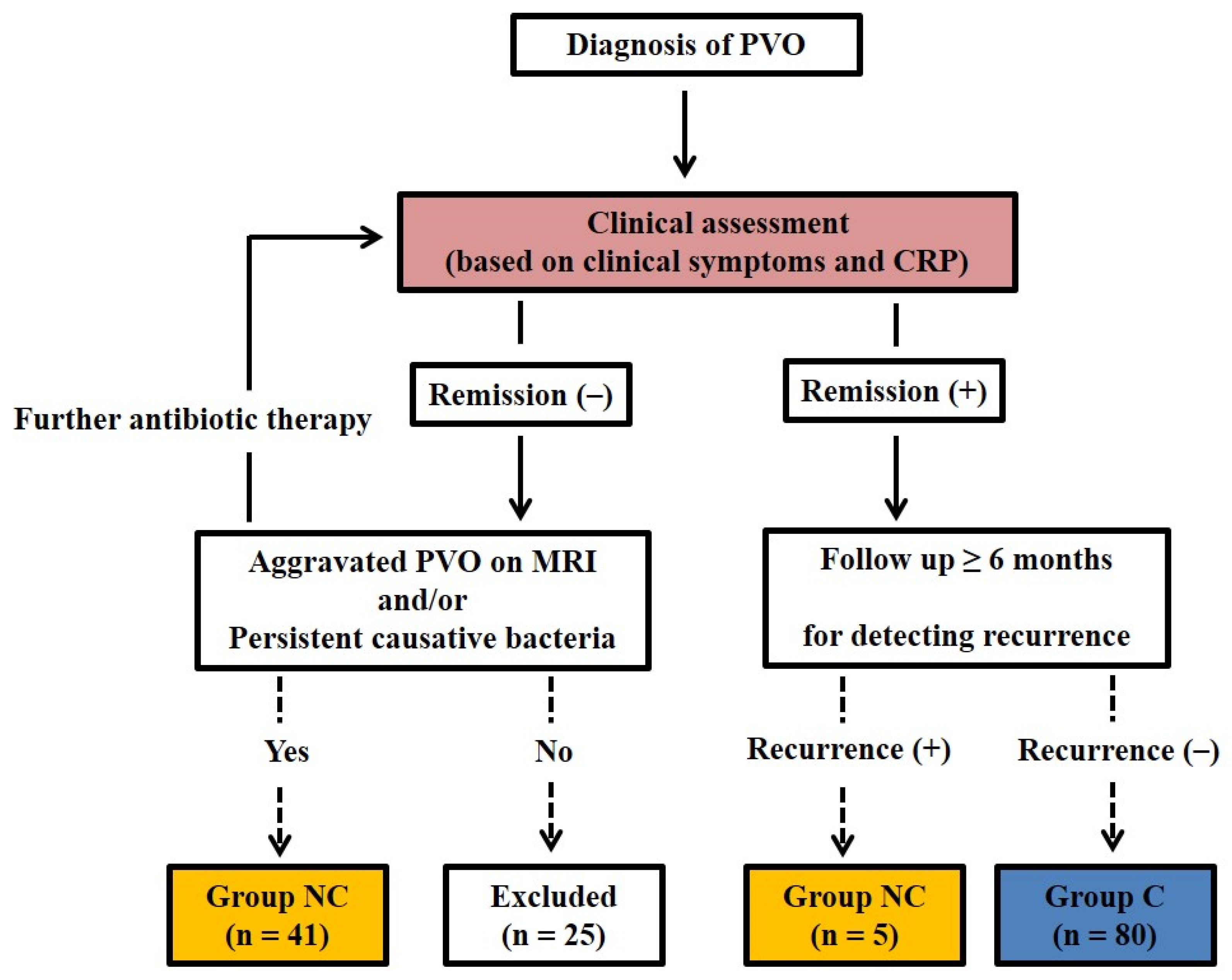
2.2. Clinical Assessment and Determining Therapeutic Response
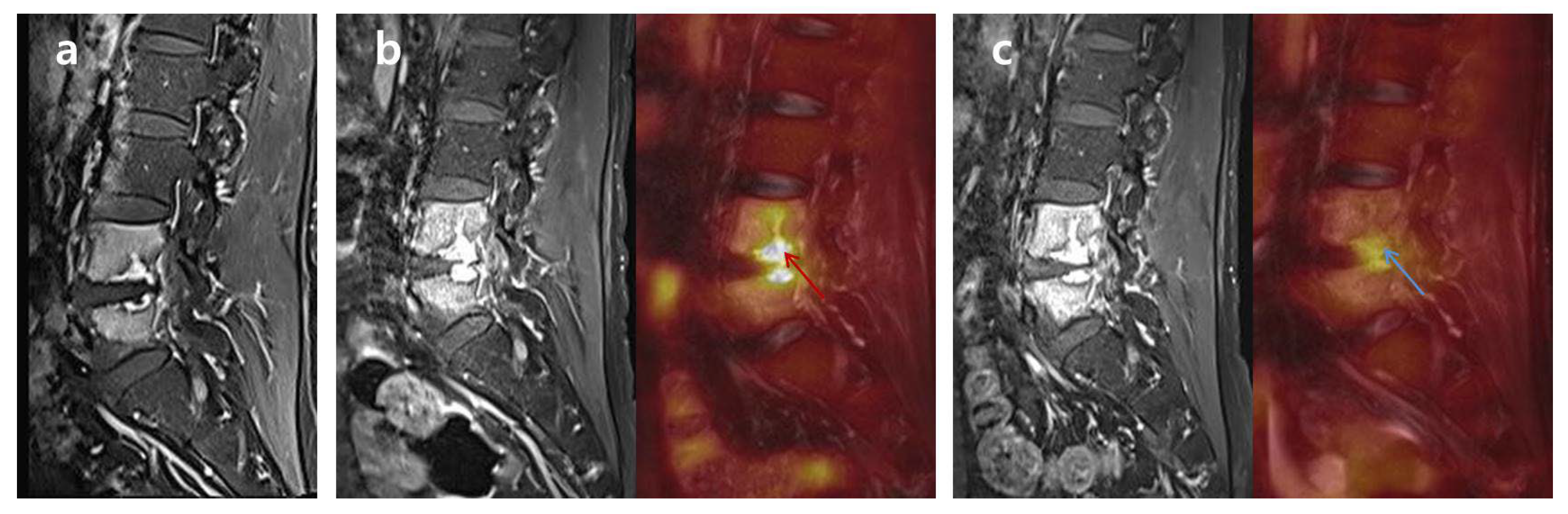
2.3. FDG-PET/MRI and Image Analysis
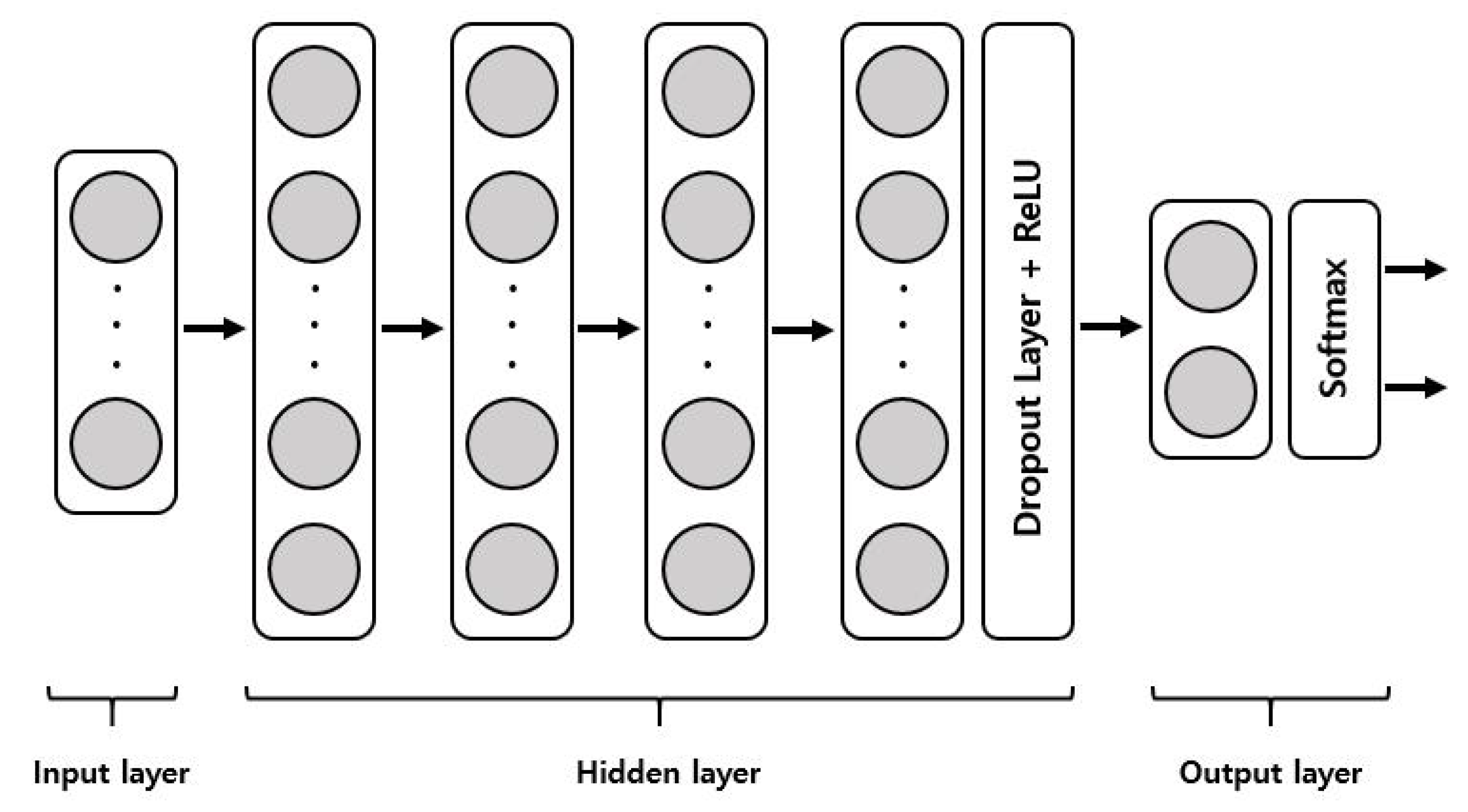
2.4. Deep Neural Network Model
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data
3.2. Causative Bacteria and Antibiotic Therapy
3.3. Clinical Assessment and Determination of Therapeutic Response
3.4. Development of DNN Model to Predict Remission of PVO
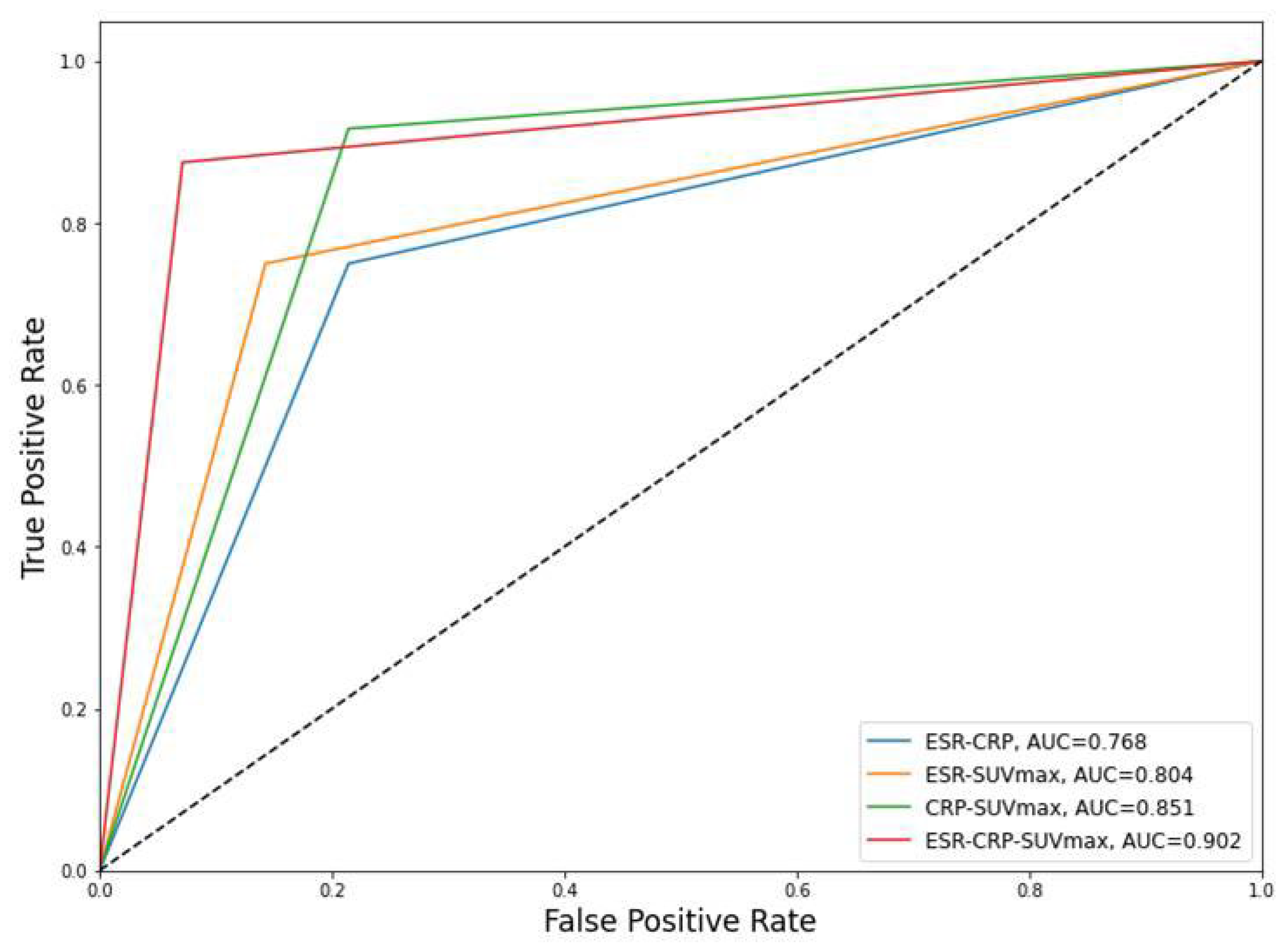
3.5. Performances of the DNN Models for Predicting the Remission of PVO
3.6. Incorrectly Predicted Cases in the DNN Model 4
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Colmenero, J.D.; Jiménez-Mejías, M.E.; Sanchez-Lora, F.J.; Reguera, J.M.; Palomino-Nicas, J.; Martos, F.; Garcia de las Heras, J.; Pachon, J. Pyogenic, tuberculous, and brucellar vertebral osteomyelitis: A descriptive and comparative study of 219 cases. Ann. Rheum. Dis. 1997, 56, 709–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berbari, E.F.; Kanj, S.S.; Kowalski, T.J.; Darouiche, R.O.; Widmer, A.F.; Schmitt, S.K.; Hendershot, E.F.; Holtom, P.D.; Huddleston, P.M.; Petermann, G.W.; et al. 2015 Infectious Diseases Society of America (IDSA) Clinical Practice Guidelines for the Diagnosis and Treatment of Native Vertebral Osteomyelitis in Adults. Clin. Infect. Dis. 2015, 61, e26–e46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perronne, C.; Saba, J.; Behloul, Z.; Salmon-Ceron, D.; Leport, C.; Vilde, J.L.; Kahn, M.F. Pyogenic and tuberculous spondylodiskitis (vertebral osteomyelitis) in 80 adult patients. Clin. Infect. Dis. 1994, 19, 746–750. [Google Scholar] [CrossRef] [PubMed]
- Yu, G.J.; Koslowsky, I.L.; Riccio, S.A.; Chu, A.K.M.; Rabin, H.R.; Kloiber, R. Diagnostic challenges in pyogenic spinal infection: An expanded role for FDG-PET/CT. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 501–509. [Google Scholar] [CrossRef]
- Kim, J.; Kim, Y.S.; Peck, K.R.; Kim, E.S.; Cho, S.Y.; Ha, Y.E.; Kang, C.I.; Chung, D.R.; Song, J.H. Outcome of culture-negative pyogenic vertebral osteomyelitis: Comparison with microbiologically confirmed pyogenic vertebral osteomyelitis. Semin. Arthritis Rheum. 2014, 44, 246–252. [Google Scholar] [CrossRef]
- Zarghooni, K.; Rollinghoff, M.; Sobottke, R.; Eysel, P. Treatment of spondylodiscitis. Int. Orthop. 2012, 36, 405–411. [Google Scholar] [CrossRef] [Green Version]
- Bernard, L.; Dinh, A.; Ghout, I.; Simo, D.; Zeller, V.; Issartel, B.; Le Moing, V.; Belmatoug, N.; Lesprit, P.; Bru, J.P.; et al. Antibiotic treatment for 6 weeks versus 12 weeks in patients with pyogenic vertebral osteomyelitis: An open-label, non-inferiority, randomised, controlled trial. Lancet 2015, 385, 875–882. [Google Scholar] [CrossRef]
- Zimmerli, W. Clinical practice. Vertebral osteomyelitis. N. Engl. J. Med. 2010, 362, 1022–1029. [Google Scholar] [CrossRef]
- Zarrouk, V.; Feydy, A.; Salles, F.; Dufour, V.; Guigui, P.; Redondo, A.; Fantin, B. Imaging does not predict the clinical outcome of bacterial vertebral osteomyelitis. Rheumatology 2007, 46, 292–295. [Google Scholar] [CrossRef] [Green Version]
- Carragee, E.J.; Kim, D.; van der Vlugt, T.; Vittum, D. The clinical use of erythrocyte sedimentation rate in pyogenic vertebral osteomyelitis. Spine 1997, 22, 2089–2093. [Google Scholar] [CrossRef]
- Jeon, I.; Kong, E. Application of Simultaneous 18F-FDG PET/MRI for Evaluating Residual Lesion in Pyogenic Spine Infection: A Case Report. Infect. Chemother. 2020, 52, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Nanni, C.; Boriani, L.; Salvadori, C.; Zamparini, E.; Rorato, G.; Ambrosini, V.; Gasbarrini, A.; Tumietto, F.; Cristini, F.; Scudeller, L.; et al. FDG PET/CT is useful for the interim evaluation of response to therapy in patients affected by haematogenous spondylodiscitis. Eur. J. Nucl. Mol. Imaging 2012, 39, 1538–1544. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Kim, I.J.; Suh, K.T.; Kim, Y.K.; Lee, J.S. Prediction of residual disease of spine infection using F-18 FDG PET/CT. Spine 2009, 34, 2424–2430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, I.; Kong, E.; Kim, S.W.; Cho, I.H.; Hong, C.P. Assessment of Therapeutic Response in Pyogenic Vertebral Osteomyelitis Using (18)F-FDG-PET/MRI. Diagnostics 2020, 10, 916. [Google Scholar] [CrossRef]
- Jeon, I.; Kong, E.; Yu, D.; Hong, C.P. Clinical and Radiological Analysis of Pyogenic Vertebral Osteomyelitis Immediately after Successful Antimicrobial Therapy: Considerations for Assessing Therapeutic Response. Diagnostics 2020, 10, 861. [Google Scholar] [CrossRef] [PubMed]
- Seong, I.; Kong, E.; Jeon, I. Clinical and Radiological Features Predicting Intervertebral Autofusion after Successful Antibiotic Therapy in Pyogenic Vertebral Osteomyelitis. Diagnostics 2021, 11, 1349. [Google Scholar] [CrossRef]
- Valliani, A.A.; Ranti, D.; Oermann, E.K. Deep Learning and Neurology: A Systematic Review. Neurol. Ther. 2019, 8, 351–365. [Google Scholar] [CrossRef] [Green Version]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Tranchevent, L.C.; Azuaje, F.; Rajapakse, J.C. A deep neural network approach to predicting clinical outcomes of neuroblastoma patients. BMC Med. Genomics 2019, 12, 178. [Google Scholar] [CrossRef] [Green Version]
- Jeon, I.; Yu, D.; Kong, E. Validity of Clinical Assessment Using Clinical Symptoms and C-Reactive Protein for Therapeutic Response in Pyogenic Vertebral Osteomyelitis: Analysis Based on (18)F-FDG-PET. Medicina 2021, 57, 809. [Google Scholar] [CrossRef]
- Yu, D.; Kim, S.W.; Jeon, I. Antimicrobial therapy and assessing therapeutic response in culture-negative pyogenic vertebral osteomyelitis: A retrospective comparative study with culture-positive pyogenic verterbal osteomyelitis. BMC Infect. Dis. 2020, 20, 939. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.H.; Smith, P.N.; Rao, N.; Donaldson, W.F. Serum C-reactive protein levels correlate with clinical response in patients treated with antibiotics for wound infections after spinal surgery. Spine J. 2006, 6, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.G.; Park, K.B.; Kang, D.H.; Hwang, S.H.; Jung, J.M.; Han, J.W. A clinical analysis of surgical treatment for spontaneous spinal infection. J. Korean Neurosurg. Soc. 2007, 42, 317–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zilkens, K.W.; Peters, K.M.; Schwanitz, B.M. New inflammation markers for early detection of spondylodiscitis. Eur. Spine J. 1992, 1, 152–155. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, T.J.; Berbari, E.F.; Huddleston, P.M.; Steckelberg, J.M.; Osmon, D.R. Do follow-up imaging examinations provide useful prognostic information in patients with spine infection? Clin. Infect. Dis. 2006, 43, 172–179. [Google Scholar] [CrossRef]
- Babouee Flury, B.; Elzi, L.; Kolbe, M.; Frei, R.; Weisser, M.; Schären, S.; Widmer, A.F.; Battegay, M. Is switching to an oral antibiotic regimen safe after 2 weeks of intravenous treatment for primary bacterial vertebral osteomyelitis? BMC Infect. Dis. 2014, 14, 226. [Google Scholar] [CrossRef] [Green Version]
- Yoon, S.H.; Chung, S.K.; Kim, K.J.; Kim, H.J.; Jin, Y.J.; Kim, H.B. Pyogenic vertebral osteomyelitis: Identification of microorganism and laboratory markers used to predict clinical outcome. Eur. Spine J. 2010, 19, 575–582. [Google Scholar] [CrossRef] [Green Version]
- Goldsmith, S.J.; Vallabhajosula, S. Clinically proven radiopharmaceuticals for infection imaging: Mechanisms and applications. Semin. Nucl. Med. 2009, 39, 2–10. [Google Scholar] [CrossRef]
- Bj0rksten, B.; Boquist, L. Histopathological aspects of chronic recurrent multifocal osteomyelitis. J. Bone Joint Surg. Br. 1980, 62, 376–380. [Google Scholar] [CrossRef] [Green Version]
- Signore, A.; Glaudemans, A.W. The molecular imaging approach to image infections and inflammation by nuclear medicine techniques. Ann. Nucl. Med. 2011, 25, 681–700. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Values |
|---|---|
| Age, years | 67.27 ± 11.18 (37–85) |
| Sex (Male/Female) | 47/27 |
| Cause of PVO | |
| Spontaneous | 30/74 (40.5%) |
| Procedure-related | 44/74 (59.5%) |
| Injection or acupuncture | 35/44 (79.5%) |
| Operation | 9/44 (20.5%) |
| Initial clinical features at diagnosis of PVO | |
| Fever (°C, >37.3) | 37/74 (50.0%) |
| Back pain | 72/74 (97.3%) |
| Radiculopathy | 39/74 (52.7%) |
| Weakness | 10/74 (13.5%) |
| Bowel and bladder symptoms | 4/74 (5.4%) |
| Extent of PVO, levels | 1.35 ± 0.53 (1–3) |
| Location of PVO | |
| Thoracic spine | 6/74 (8.1%) |
| Thoracic-lumbar spine | 3/74 (4.0%) |
| Lumbar-sacral spine | 65/74 (87.8%) |
| ESR (mm/h) | 67.68 ± 30.21 (6–120) |
| CRP (mg/L) | 9.84 ± 9.16 (0.03–33.8) |
| Duration of follow up, months # | 12.66 ± 8.81 (1–44) |
| Characteristics | Values |
|---|---|
| Identification of causative bacteria | 38/74 (51.4%) |
| Causative bacteria | |
| Gram-positive bacteria | 35/38 (92.1%) |
| Staphylococcus aureus | 18/35 (51.4%) |
| MSSA | 13/15 (60.0%) |
| MRSA | 5/15 (40.0%) |
| Coagulase-negative staphylococci | 6/35 (17.1%) |
| MRSE | 3/6 (50.0%) |
| Others | 3/6 (50.0%) |
| Streptococcus species | 7/35 (20.0%) |
| Enterococcus species | 4/35 (11.4%) |
| Gram-negative bacteria | 3/38 (7.9%) |
| Escherichia coli | 2/3 (66.7%) |
| Enterobacter species | 1/3 (33.3%) |
| Non | 36/74 (48.6%) |
| Routes of causative bacterial diagnosis | |
| Blood | 10/38 (26.3%) |
| PVO lesion | 19/38 (50.0%) |
| Blood and PVO lesion | 6/38 (15.8%) |
| Duration of parenteral antibiotics, days | 44.14 ± 16.70 (21–89) |
| Attributes | Group C (n = 80) | Group NC (n = 46) | Total (n = 126) |
|---|---|---|---|
| ESR * | 42.64 ± 27.76 (7–120) | 71.57 ± 31.36 (7–120) | 53.20 ± 32.20 (7–120) |
| CRP * | 0.80 ± 1.07 (0.02–5.93) | 3.01 ± 3.20 (0.11–15.75) | 1.61 ± 2.36 (0.02–15.75) |
| SUVmax * | 4.59 ± 2.15 (1.66–16.11) | 7.30 ± 2.14 (3.61–14.65) | 5.58 ± 2.51 (1.66–16.11) |
| DNN Models | Sensitivity | Specificity | PPV | NPV | Accuracy | AUC |
|---|---|---|---|---|---|---|
| DNN model 1 (ESR and CRP) | 75% | 78.6% | 85.7% | 64.7% | 76.3% | 0.768 [0.625–0.910] |
| DNN model 2 (ESR and SUVmax) | 75% | 85.7% | 90% | 66.7% | 79% | 0.804 [0.674–0.933] |
| DNN model 3 (CRP and SUVmax) | 91.7% | 78.6% | 88% | 84.6% | 86.8% | 0.851 [0.726–0.976] |
| DNN model 4 (ESR, CRP, and SUVmax) | 87.5% | 92.7% | 95.5% | 81.3% | 89.5% | 0.902 [0.804–0.999] |
| Number of Case | ESR | CRP | SUVmax | Prediction of DNN Model 4 | Actual Result |
|---|---|---|---|---|---|
| # 33 | 79 | 5.104 | 6.38 | Non-cured | Cured |
| # 45 | 25 | 0.537 | 7.79 | Non-cured | Cured |
| # 107 | 97 | 3.222 | 6.2 | Non-cured | Cured |
| # 126 | 7 | 0.149 | 4.6 | Cured | Non-cured |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, H.; Kong, E.; Yu, D.; Choi, G.S.; Jeon, I. Assessment of Therapeutic Responses Using a Deep Neural Network Based on 18F-FDG PET and Blood Inflammatory Markers in Pyogenic Vertebral Osteomyelitis. Medicina 2022, 58, 1693. https://doi.org/10.3390/medicina58111693
Shin H, Kong E, Yu D, Choi GS, Jeon I. Assessment of Therapeutic Responses Using a Deep Neural Network Based on 18F-FDG PET and Blood Inflammatory Markers in Pyogenic Vertebral Osteomyelitis. Medicina. 2022; 58(11):1693. https://doi.org/10.3390/medicina58111693
Chicago/Turabian StyleShin, Hyunkwang, Eunjung Kong, Dongwoo Yu, Gyu Sang Choi, and Ikchan Jeon. 2022. "Assessment of Therapeutic Responses Using a Deep Neural Network Based on 18F-FDG PET and Blood Inflammatory Markers in Pyogenic Vertebral Osteomyelitis" Medicina 58, no. 11: 1693. https://doi.org/10.3390/medicina58111693