
Obstructive Sleep Apnea Disrupts Glycemic Control in Obese Individuals
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Statistical Analysis
3. Results
3.1. Study Population
3.2. Comparison of Polysomnographic Sleep Parameters
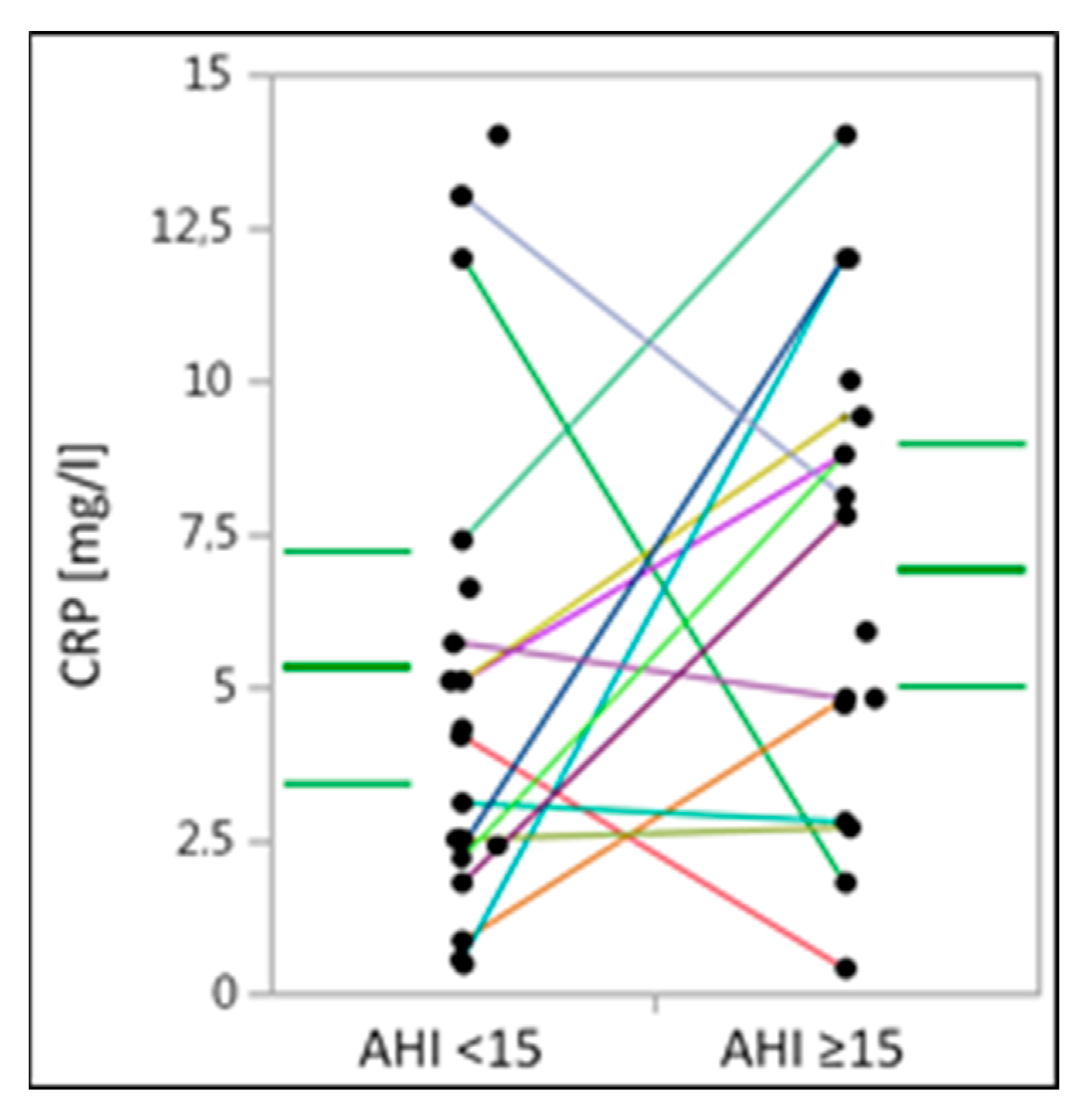
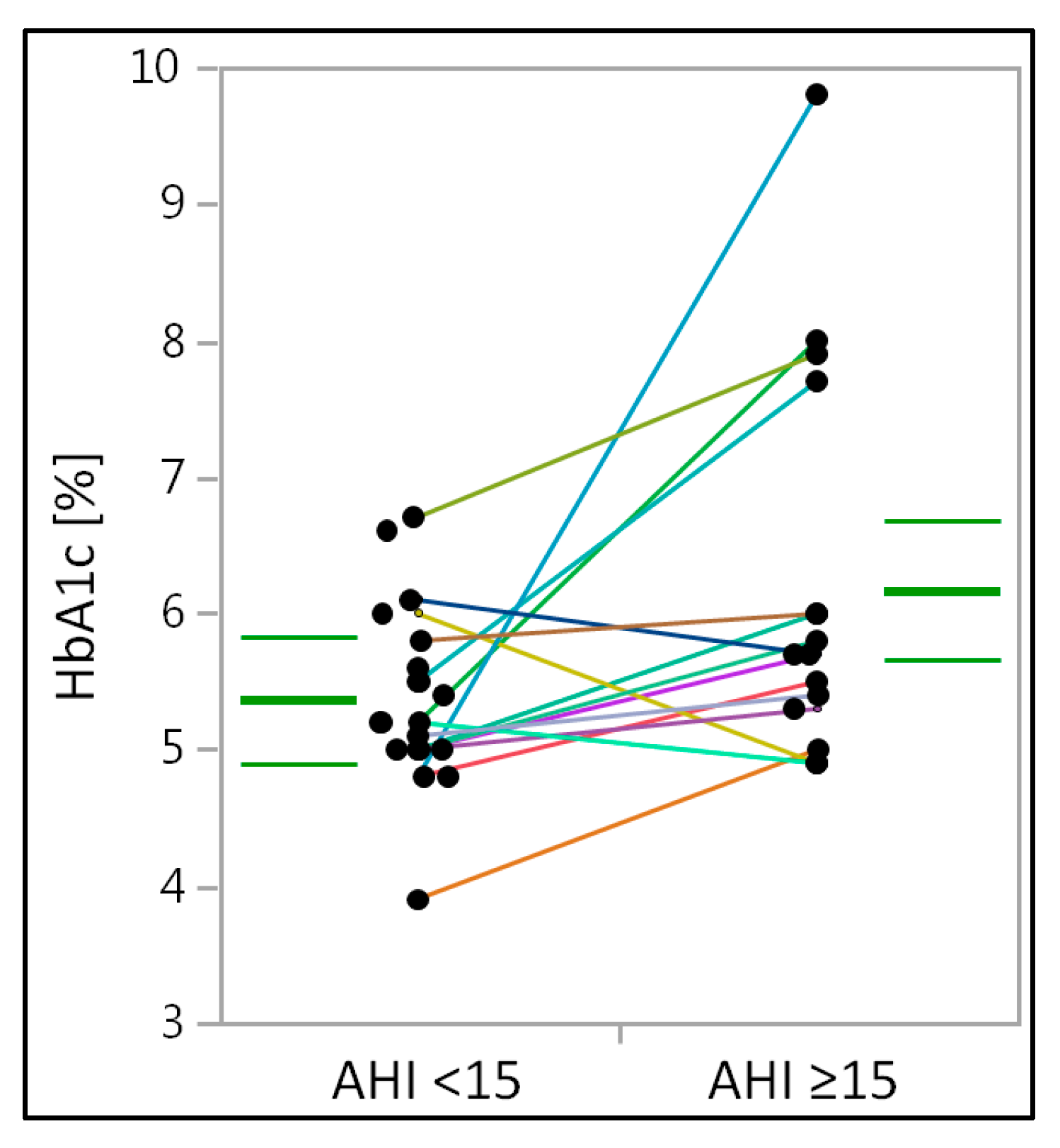
3.3. Analysis of C-Reactive Protein and Glycated Hemoglobin Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ho, M.L.; Brass, S.D. Obstructive sleep apnea. Neurol. Int. 2011, 3, e15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malhotra, A.; White, D.P. Obstructive sleep apnoea. Lancet 2002, 360, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Curtin, L.R.; McDowell, M.A.; Tabak, C.J.; Flegal, K.M. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA 2006, 295, 1549–1555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, A.B.; Foster, G.; Givelber, R.; Nieto, F.J.; Redline, S.; Young, T. Progression and regression of sleep-disordered breathing with changes in weight: The Sleep Heart Health Study. Arch. Intern. Med. 2005, 165, 2408–2413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peppard, P.E.; Young, T.; Palta, M.; Dempsey, J.; Skatrud, J. Longitudinal study of moderate weight change and sleep-disordered breathing. JAMA 2000, 284, 3015–3021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, T.; Peppard, P.E.; Taheri, S. Excess weight and sleep-disordered breathing. J. Appl. Physiol. 2005, 99, 1592–1599. [Google Scholar] [CrossRef] [PubMed]
- Lattimore, J.D.; Celermajer, D.S.; Wilcox, I. Obstructive sleep apnea and cardiovascular disease. J. Am. Coll. Cardiol. 2003, 41, 1429–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlatzer, C.; Schwarz, E.I.; Kohler, M. The effect of continuous positive airway pressure on metabolic variables in patients with obstructive sleep apnoea. Chronic Respir. Dis. 2014, 11, 41–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pamidi, S.; Tasali, E. Obstructive sleep apnea and type 2 diabetes: Is there a link? Front. Neurol. 2012, 3, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakhtoura, M.; Azar, S.T. Continuous positive airway pressure and type 2 diabetes mellitus. Diabetol. Metab. Syndr. 2012, 6, 176–179. [Google Scholar] [CrossRef] [PubMed]
- Jahn, C.; Gouveris, H.; Matthias, C. Systemic inflammation in patients with compromised upper airway anatomy and primary snoring or mild obstructive sleep apnea. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 3429–3433. [Google Scholar] [CrossRef] [PubMed]
- Tam, C.S.; Wong, M.; Tam, K.; Aouad, L.; Waters, K.A. The effect of acute intermittent hypercapnic hypoxia treatment on IL-6, TNF-alpha, and CRP levels in piglets. Sleep 2007, 30, 723–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korkmaz, M.; Korkmaz, H.; Küçüker, F.; Ayyıldız, S.N.; Çankaya, S. Evaluation of the association of sleep apnea-related systemic inflammation with CRP, ESR, and neutrophil-to-lymphocyte ratio. Med. Sci. Monit. 2015, 21, 477–481. [Google Scholar] [PubMed] [Green Version]
- Ruehland, W.R.; Rochford, P.D.; O’Donoghue, F.J.; Pierce, R.J.; Singh, P.; Thornton, A.T. The new AASM criteria for scoring hypopneas: Impact on the apnea hypopnea index. Sleep 2009, 32, 150–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jehan, S.; Zizi, F.; Pandi-Perumal, S.R.; Wall, S.; Auguste, E.; Myers, A.K.; Jean-Louis, G.; McFarlane, S.I. Obstructive Sleep Apnea and Obesity: Implications for Public Health. Sleep Med. Disord. 2017, 1, 19. [Google Scholar] [PubMed]
- Shelton, K.E.; Woodson, H.; Gay, S.; Suratt, P.M. Pharyngeal fat in obstructive sleep apnea. Am. Rev. Respir. Dis. 1993, 148, 462–466. [Google Scholar] [CrossRef] [PubMed]
- Schwab, R.J.; Pasirstein, M.; Pierson, R.; Mackley, A.; Hachadoorian, R.; Arens, R.; Maislin, G.; Pack, A.I. Identification of upper airway anatomic risk factors for obstructive sleep apnea with volumetric magnetic resonance imaging. Am. J. Respir. Crit. Care Med. 2003, 168, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Fleming, W.E.; Holty, J.C.; Bogan, R.K.; Hwang, D.; Ferouz-Colborn, A.S.; Budhiraja, R.; Redline, S.; Mensah-Osman, E.; Osman, N.I.; Li, Q.; et al. Use of blood biomarkers to screen for obstructive sleep apnea. Nat. Sci. Sleep 2018, 10, 159–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, S.; Wan, Y.; Xu, M.; Ming, J.; Xing, Y.; An, F.; Ji, Q. The association between obstructive sleep apnea and metabolic syndrome: A systematic review and meta-analysis. BMC Pulm. Med. 2015, 15, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iiyori, N.; Alonso, L.C.; Li, J.; Sanders, M.H.; Garcia-Ocana, A.; O’Doherty, R.M.; Polotsky, V.Y.; O’Donnell, C.P. Intermittent hypoxia causes insulin resistance in lean mice independent of autonomic activity. Am. J. Respir. Crit. Care Med. 2007, 175, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Cignarelli, A.; Ciavarella, A.; Barbaro, M.; Kounaki, S.; Di Trani, A.; Falcone, V.A.; Quaranta, V.N.; Natalicchio, A.; Laviola, L.; Resta, O.; et al. Postprandial glucose and HbA1c are associated with severity of obstructive sleep apnoea in non-diabetic obese subjects. J. Endocrinol. Investig. 2021, 44, 2741–2748. [Google Scholar] [CrossRef] [PubMed]
- Kent, B.D.; Grote, L.; Bonsignore, M.R.; Saaresranta, T.; Verbraecken, J.; Lévy, P.; Sliwinski, P.; Tkacova, R.; Kvamme, J.A.; Fietze, I.; et al. European Sleep Apnoea Database collaborators. Sleep apnoea severity independently predicts glycaemic health in nondiabetic subjects: The ESADA study. Eur. Respir. J. 2014, 44, 130–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tasbakan, M.S.; Grote, L.; Hedner, J.; Kvamme, J.A.; Verbraecken, J.; McNicholas, W.T.; Roisman, G.; Tkacova, R.; Bonsignore, M.R.; Saaresranta, T.; et al. ESADA Collaborators. Positive airway pressure (PAP) treatment reduces glycated hemoglobin (HbA1c) levels in obstructive sleep apnea patients with concomitant weight loss: Longitudinal data from the ESADA. J Sleep Res. 2021, 30, e13331. [Google Scholar] [CrossRef] [PubMed]
- Bouloukaki, I.; Mermigkis, C.; Kallergis, E.M.; Moniaki, V.; Mauroudi, E.; Schiza, S.E. Obstructive sleep apnea syndrome and cardiovascular disease: The influence of C-reactive protein. World J. Exp. Med. 2015, 5, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Wei, P.; Qin, Y.; Wei, Y. Is C-reactive protein a marker of obstructive sleep apnea?: A meta-analysis. Medicine 2017, 96, e6850. [Google Scholar] [CrossRef] [PubMed]
- Kanbay, A.; Kaya, E.; Büyükoğlan, H.; Kaya, M.G.; Şimşek, Z.Ö.; Tutar, N.; Demir, R. Correlation between pentraxin-3 and endothelial dysfunction in obstructive sleep apnea syndrome. Ann. Thorac. Surg. 2015, 10, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Guilleminault, C.; Kirisoglu, C.; Ohayon, M.M. C-reactive protein and sleep-disordered breathing. Sleep 2004, 27, 1507–1511. [Google Scholar] [CrossRef] [PubMed]
- Gouveris, H.; Bahr, K.; Jahn, C.; Matthias, C.; Simon, P. The Apnea-Hypopnea Index Underestimates Systemic Inflammation in Women with Sleep-Disordered Breathing. J. Women’s Health 2018, 27, 920–926. [Google Scholar] [CrossRef] [PubMed]
- Rocchi, C.; Valentina, C.; Totaro, V.; Broggi, S.; Lattanzi, S.; Viticchi, G.; Falsetti, L.; Silvestrini, M.; Buratti, L. Inflammation markers in moderate and severe obstructive sleep apnea: The influence of sex. Sleep Breath. 2022. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Buratti, L.; Rocchi, C.; Totaro, V.; Broggi, S.; Lattanzi, S.; Viticchi, G.; Falsetti, L.; Silvestrini, M. Sex-Related Differences in Polygraphic Parameters in a Population of Patients with Obstructive Sleep Apnea Syndrome. CNS Neurol. Disord. Drug Targets 2022, 21, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Masa, J.F.; Pépin, J.L.; Borel, J.C.; Mokhlesi, B.; Murphy, P.B.; Sánchez-Quiroga, M.Á. Obesity hypoventilation syndrome. Eur. Respir. Rev. 2019, 28, 180097. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| AHI < 15 | AHI ≥ 15 | Between Group Comparison (p-Value) | |
|---|---|---|---|
| Number of individuals | 23 | 23 | |
| Male participants (%) | 7 (30) | 7 (30) | |
| Female participants (%) | 16 (70) | 16 (70) | |
| Age, in years (± SD) | 42.57 ± 11.44 | 43.43 ± 11.96 | 0.214 |
| BMI, in kg/m2 (± SD) | 37.35 ± 3.88 | 37.87 ± 4.74 | 0.532 |
| Hypertension (n (%)) | 10 (43) | 8 (35) | |
| Diabetes mellitus (n (%)) | 2 (9) | 2 (9) | |
| Insulin intake (n(%)) | 0 (0) | 0 (0) | |
| Metformin intake (n (%)) | 3 (13) | 2 (9) | |
| Pulmonary disorders (n (%)) | 2 (9) | 2 (9) | |
| Hypothyroidism (n (%)) | 4 (17) | 6 (25) | |
| Levothyroxine intake (n (%)) | 5 (22) | 6 (25) | |
| Number of non-smokers (%) | 16 (70) | 15 (65) | |
| Number of active smokers (%) | 7 (30) | 8 (35) |
| AHI < 15 | AHI ≥ 15 | Between Group Comparison (p-Value) | |
|---|---|---|---|
| AHI (n/hour) | 7.5 (5.5–12.5) | 41.5 (25.7–71.8) | <0.001 |
| Apnea index (n/hour) | 1 (0.3–2.5) | 11.3 (5.7–35.1) | <0.001 |
| Hypopnea index (n/hour) | 6.2 (4.3–8.7) | 23.2 (17–29.6) | <0.001 |
| Snoring index (n/hour) | 114 (10–350) | 425.2 (233–700.6) | 0.010 |
| Oxygen desaturation index (n/hour) | 9 (5.7–13) | 40.9 (25.5–72.7) | <0.001 |
| Oxygen desaturation in REM (n) | 16 (6–25) | 49 (24–78) | <0.001 |
| Average oxygen desaturation (%) | 95 (94–95) | 92 (91–94) | <0.001 |
| t90 (%) | 0.3 (0.1–1.9) | 8.4 (3–22.6) | <0.001 |
| PLM (n) | 19 (4–40) | 128 (24–211) | 0.014 |
| TST (min) | 387.12 ± 41.39 | 369.85 ± 43.18 | 0.312 |
| N3 sleep (%) | 19.99 ± 9.82 | 16.1 ± 9.13 | 0.39 |
| REM sleep (%) | 15.23 ± 7.62 | 13.73 ± 6.38 | 0.746 |
| REM AHI (n/hour) | 17.6 (12.8–30.4) | 56 (40–78) | <0.001 |
| Arousal index (n/hour) | 10.2 (8.5–11.8) | 23.6 (13.7–33.8) | <0.001 |
| Respiratory arousal index (n/hour) | 3.9 (2.6–7.7) | 13.3 (10.5–21.8) | <0.001 |
| AHI in supine position (n/hour) | 10.1 (6.1–22) | 62.7 (35.6–79) | <0.001 |
| AHI < 15 | AHI ≥ 15 | Between Group Comparison (p-Value) | |
|---|---|---|---|
| CRP (mg/L) | 4.25 (2.25–7.2) | 7.8 (3.75–9.7) | 0.186 |
| HbA1c (%) | 5.2 (5–5.75) | 5.8 (5.35–6.85) | 0.016 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seifen, C.; Pordzik, J.; Ludwig, K.; Bahr, K.; Schupp, C.; Matthias, C.; Simon, P.; Gouveris, H. Obstructive Sleep Apnea Disrupts Glycemic Control in Obese Individuals. Medicina 2022, 58, 1602. https://doi.org/10.3390/medicina58111602
Seifen C, Pordzik J, Ludwig K, Bahr K, Schupp C, Matthias C, Simon P, Gouveris H. Obstructive Sleep Apnea Disrupts Glycemic Control in Obese Individuals. Medicina. 2022; 58(11):1602. https://doi.org/10.3390/medicina58111602
Chicago/Turabian StyleSeifen, Christopher, Johannes Pordzik, Katharina Ludwig, Katharina Bahr, Cornelia Schupp, Christoph Matthias, Perikles Simon, and Haralampos Gouveris. 2022. "Obstructive Sleep Apnea Disrupts Glycemic Control in Obese Individuals" Medicina 58, no. 11: 1602. https://doi.org/10.3390/medicina58111602