

Long-Term Prognostic Value of Myocardial Viability by Myocardial Contrast Echocardiography in Patients after Acute Myocardial Infarction: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Study Collection and Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
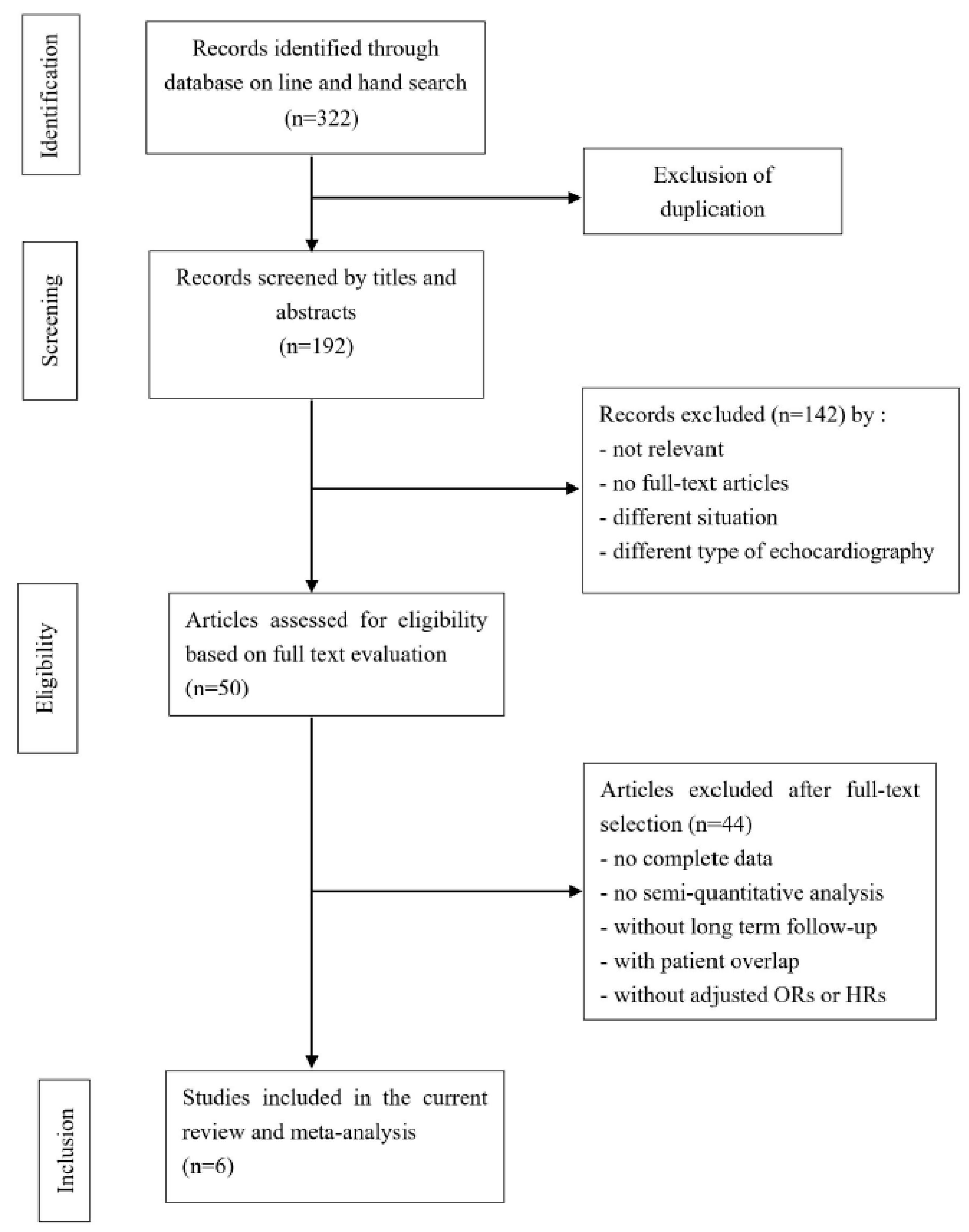
3.1. Systematic Review
3.2. Characteristics of MCE and Semiquantitative Systems
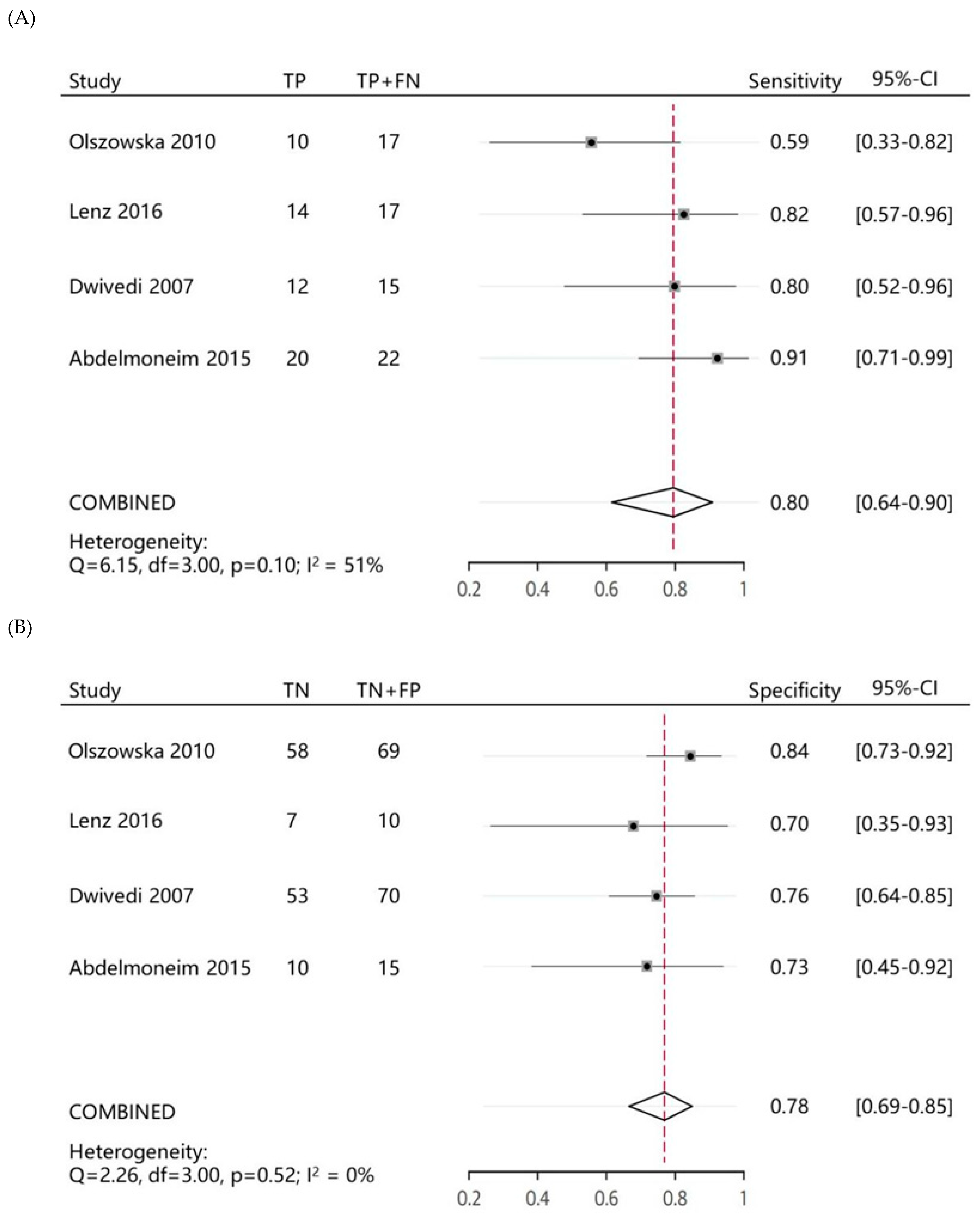
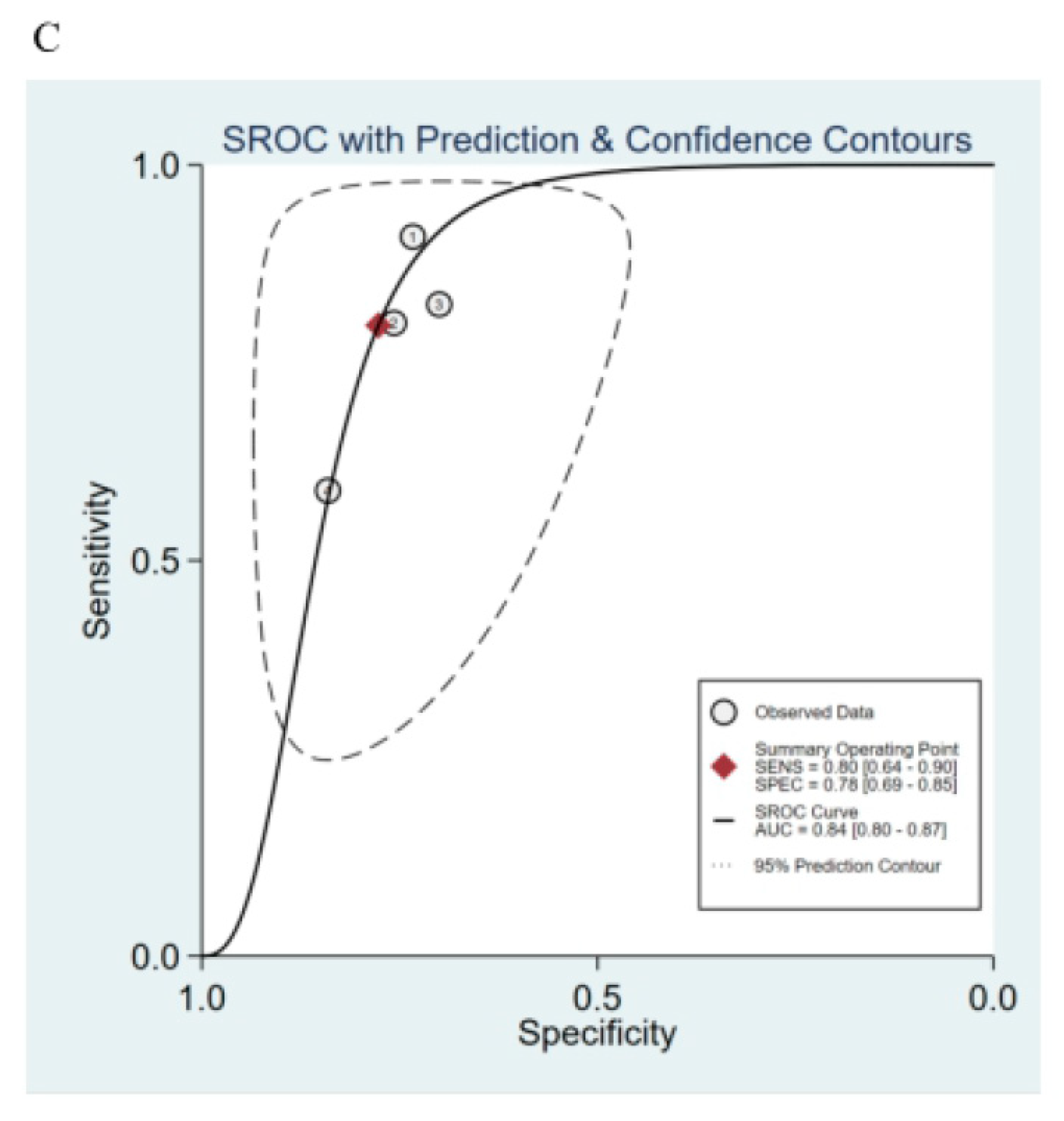
3.3. Ability of MCE Score Index to Predict MACE in Post-AMI Patients
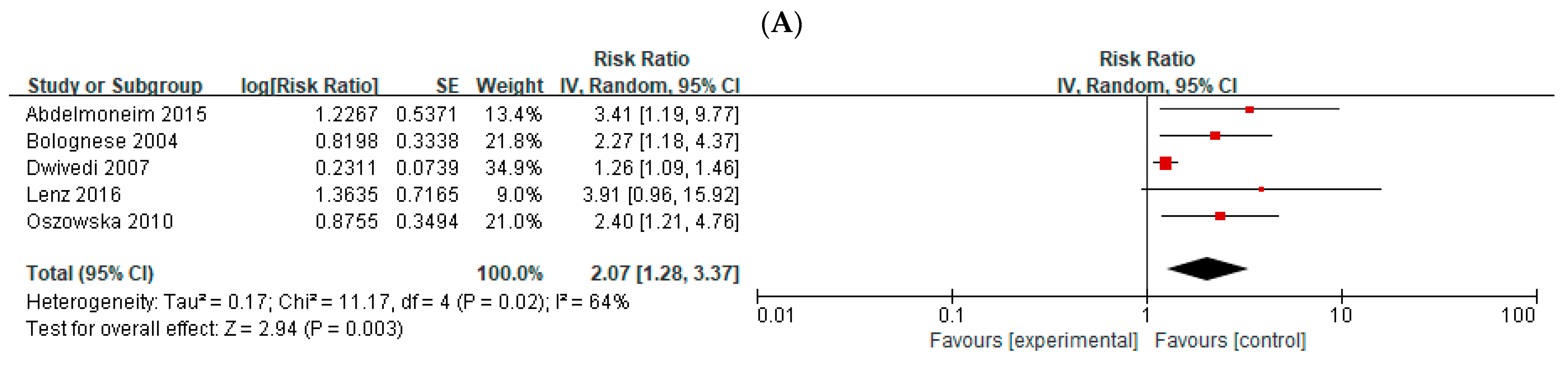
3.4. Total Cardiac Events in Post-AMI Patients
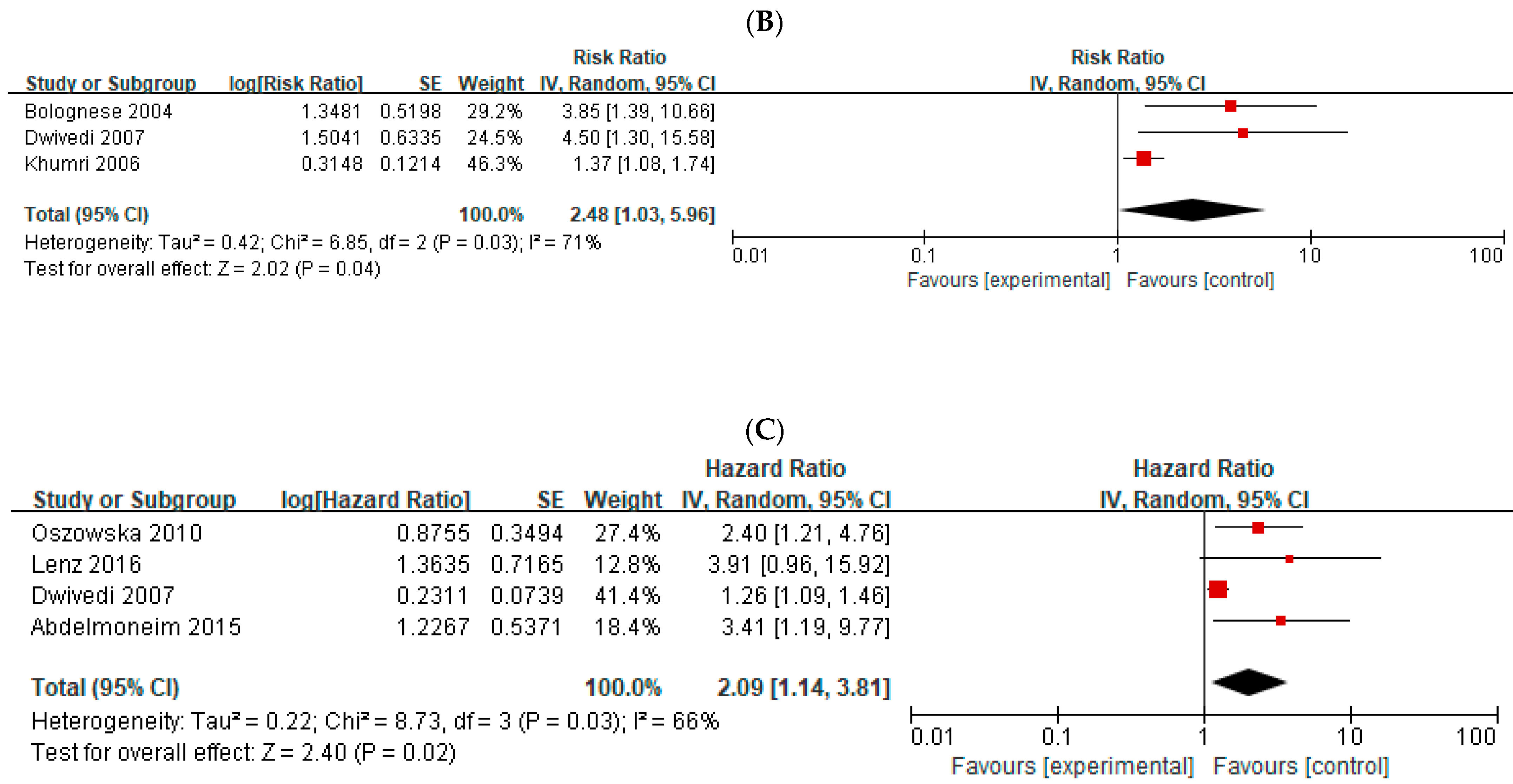
3.5. Cardiac Death in Post-AMI Patients
3.6. Sensitivity Analysis
3.7. Meta-Analysis of the Studies That Reported HRs for Total Cardiac Events
3.8. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roth, G.A.; Huffman, M.D.; Moran, A.E.; Feigin, V.; Mensah, G.A.; Naghavi, M.; Murray, C.J. Global and regional patterns in cardiovascular mortality from 1990 to 2013. Circulation 2015, 132, 1667–1678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajaj, A.; Sethi, A.; Rathor, P.; Suppogu, N.; Sethi, A. Acute Complications of Myocardial Infarction in the Current Era: Diagnosis and Management. J. Investig. Med. Off. Publ. Am. Fed. Clin. Res. 2015, 63, 844–855. [Google Scholar] [CrossRef] [PubMed]
- Abed, M.A.; Ali, R.M.; Abu Ras, M.M.; Hamdallah, F.O.; Khalil, A.A.; Moser, D.K. Symptoms of acute myocardial infarction: A correlational study of the discrepancy between patients’ expectations and experiences. Int. J. Nurs. Stud. 2015, 52, 1591–1599. [Google Scholar] [CrossRef] [PubMed]
- O’Gara, P.T.; Kushner, F.G.; Ascheim, D.D.; Casey, D.E., Jr.; Chung, M.K.; de Lemos, J.A.; Ettinger, S.M.; Fang, J.C.; Fesmire, F.M.; Franklin, B.A.; et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013, 61, e78–e140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amier, R.P.; Smulders, M.W.; van der Flier, W.M.; Bekkers, S.C.A.M.; Zweerink, A.; Allaart, C.P.; Demirkiran, A.; Roos, S.T.; Teunissen, P.F.A.; Appelman, Y.; et al. Long-Term Prognostic Implications of Previous Silent Myocardial Infarction in Patients Presenting With Acute Myocardial Infarction. JACC Cardiovasc. Imaging 2018, 11, 1773–1781. [Google Scholar] [CrossRef]
- Boateng, S.; Sanborn, T. Acute myocardial infarction. Dis. Mon. 2013, 59, 83–96. [Google Scholar] [CrossRef]
- Boersma, E. Does time matter? A pooled analysis of randomized clinical trials comparing primary percutaneous coronary intervention and in-hospital fibrinolysis in acute myocardial infarction patients. Eur. Heart J. 2006, 27, 779–788. [Google Scholar] [CrossRef] [Green Version]
- Janardhanan, R.; Swinburn, J.M.; Greaves, K.; Senior, R. Usefulness of myocardial contrast echocardiography using low-power continuous imaging early after acute myocardial infarction to predict late functional left ventricular recovery. Am. J. Cardiol. 2003, 92, 493–497. [Google Scholar] [CrossRef]
- Swinburn, J.; Lahiri, A.; Senior, R. Intravenous myocardial contrast echocardiography predicts recovery of dysynergic myocardium early after acute myocardial infarction. J. Am. Coll. Cardiol. 2001, 38, 19–25. [Google Scholar] [CrossRef] [Green Version]
- Janardhanan, R.; Moon, J.C.; Pennell, D.J.; Senior, R. Myocardial contrast echocardiography accurately reflects transmurality of myocardial necrosis and predicts contractile reserve after acute myocardial infarction. Am. Heart J. 2005, 149, 355–362. [Google Scholar] [CrossRef]
- Galiuto, L.; Garramone, B.; Scarà, A.; Rebuzzi, A.G.; Crea, F.; La Torre, G.; Funaro, S.; Madonna, M.; Fedele, F.; Agati, L.; et al. The extent of microvascular damage during myocardial contrast echocardiography is superior to other known indexes of post-infarct reperfusion in predicting left ventricular remodeling: Results of the multicenter AMICI study. J. Am. Coll. Cardiol. 2008, 51, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, G.; Janardhanan, R.; Hayat, S.A.; Lim, T.K.; Senior, R. Comparison between myocardial contrast echocardiography and (99m)technetium sestamibi single photon emission computed tomography determined myocardial viability in predicting hard cardiac events following acute myocardial infarction. Am. J. Cardiol. 2009, 104, 1184–1188. [Google Scholar] [CrossRef] [PubMed]
- Lenz, C.J.; Abdelmoneim, S.S.; Anavekar, N.S.; Foley, T.A.; Nhola, L.F.; Huang, R.; Oh, J.K.; Mulvagh, S.L. A comparison of infarct mass by cardiac magnetic resonance and real time myocardial perfusion echocardiography as predictors of major adverse cardiac events following reperfusion for ST elevation myocardial infarction. Echocardiography 2016, 33, 1539–1545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olszowska, M.; Kostkiewicz, M.; Podolec, P.; Rubis, P.; Tracz, W. Myocardial viability detected by myocardial contrast echocardiography—prognostic value in patients after myocardial infarction. Echocardiography 2010, 27, 430–434. [Google Scholar] [CrossRef]
- Wita, K.; Filipecki, A.; Szydło, K.; Turski, M.; Tabor, Z.; Wróbel, W.; Elzbieciak, M.; Lelek, M.; Bochenek, T.; Trusz-Gluza, M. Prediction of long-term outcome after primary percutaneous coronary intervention for acute anterior myocardial infarction. Kardiol. Pol. 2010, 68, 393–400. [Google Scholar]
- Dwivedi, G.; Janardhanan, R.; Hayat, S.A.; Swinburn, J.M.; Senior, R. Prognostic value of myocardial viability detected by myocardial contrast echocardiography early after acute myocardial infarction. J. Am. Coll. Cardiol. 2007, 50, 327–334. [Google Scholar] [CrossRef] [Green Version]
- Abdelmoneim, S.S.; Martinez, M.W.; Mankad, S.V.; Bernier, M.; Dhoble, A.; Pellikka, P.A.; Chandrasekaran, K.; Oh, J.K.; Mulvagh, S.L. Resting qualitative and quantitative myocardial contrast echocardiography to predict cardiac events in patients with acute myocardial infarction and percutaneous revascularization. Heart Vessel. 2015, 30, 45–55. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.S.B.; O’Connell, D. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical.epidemiology/oxford.asp (accessed on 1 July 2016).
- Hayden, J.A.; Côté, P.; Bombardier, C. Evaluation of the quality of prognosis studies in systematic reviews. Ann. Intern. Med. 2006, 144, 427–437. [Google Scholar] [CrossRef]
- Bolognese, L.; Carrabba, N.; Parodi, G.; Santoro, G.M.; Buonamici, P.; Cerisano, G.; Antoniucci, D. Impact of microvascular dysfunction on left ventricular remodeling and long-term clinical outcome after primary coronary angioplasty for acute myocardial infarction. Circulation 2004, 109, 1121–1126. [Google Scholar] [CrossRef]
- Khumri, T.M.; Nayyar, S.; Idupulapati, M.; Magalski, A.; Stoner, C.N.; Kusnetzky, L.L.; Kosiborod, M.; Spertus, J.A.; Main, M.L. Usefulness of myocardial contrast echocardiography in predicting late mortality in patients with anterior wall acute myocardial infarction. Am. J. Cardiol. 2006, 98, 1150–1155. [Google Scholar] [CrossRef] [PubMed]
- Allman, K.C.; Shaw, L.J.; Hachamovitch, R.; Udelson, J.E. Myocardial viability testing and impact of revascularization on prognosis in patients with coronary artery disease and left ventricular dysfunction: A meta-analysis. J. Am. Coll. Cardiol. 2002, 39, 1151–1158. [Google Scholar] [CrossRef] [Green Version]
- Pradhan, J.; Senior, R. Assessment of myocardial viability by myocardial contrast echocardiography: Current perspectives. Curr. Opin. Cardiol. 2019, 34, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Kaul, S.; Jayaweera, A.R. Coronary and myocardial blood volumes: Noninvasive tools to assess the coronary microcirculation? Circulation 1997, 96, 719–724. [Google Scholar]
- Wei, K.; Jayaweera, A.R.; Firoozan, S.; Linka, A.; Skyba, D.M.; Kaul, S. Basis for detection of stenosis using venous administration of microbubbles during myocardial contrast echocardiography: Bolus or continuous infusion? J. Am. Coll. Cardiol. 1998, 32, 252–260. [Google Scholar] [CrossRef] [Green Version]
- Senior, R.; Becher, H.; Monaghan, M.; Agati, L.; Zamorano, J.; Vanoverschelde, J.L.; Nihoyannopoulos, P.; Edvardsen, T.; Lancellotti, P. Clinical practice of contrast echocardiography: Recommendation by the European Association of Cardiovascular Imaging (EACVI). Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1205–1205af. [Google Scholar] [CrossRef]
- Montisci, R.; Chen, L.; Ruscazio, M.; Colonna, P.; Cadeddu, C.; Caiati, C.; Montisci, M.; Meloni, L.; Iliceto, S. Non-invasive coronary flow reserve is correlated with microvascular integrity and myocardial viability after primary angioplasty in acute myocardial infarction. Heart 2006, 92, 1113–1118. [Google Scholar] [CrossRef] [Green Version]
- Shah, B.; Khattar, R.; Senior, R. The hibernating myocardium: Current concepts, diagnostic dilemmas, and clinical challenges in the post-STICH era. Eur. Heart J. 2013, 34, 1323–1336. [Google Scholar] [CrossRef] [Green Version]
- Hickman, M.; Janardhanan, R.; Dwivedi, G.; Burden, L.; Senior, R. Clinical significance of perfusion techniques utilising different physiological mechanisms to detect myocardial viability: A comparative study with myocardial contrast echocardiography and single photon emission computed tomography. Int. J. Cardiol. 2007, 114, 139–140. [Google Scholar] [CrossRef]
- Biagini, E.; van Geuns, R.J.; Baks, T.; Boersma, E.; Rizzello, V.; Galema, T.W.; de Feyter, P.J.; ten Cate, F.J. Comparison between contrast echocardiography and magnetic resonance imaging to predict improvement of myocardial function after primary coronary intervention. Am. J. Cardiol. 2006, 97, 361–366. [Google Scholar] [CrossRef]
- Trindade, M.L.; Caldas, M.A.; Tsutsui, J.M.; Rosario, M.A.; Rochitte, C.E.; Nicolau, J.C.; Ramires, J.A.; Mathias, W., Jr. Determination of size and transmural extent of acute myocardial infarction by real-time myocardial perfusion echocardiography: A comparison with magnetic resonance imaging. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2007, 20, 126–135. [Google Scholar]
- Lombardo, A.; Rizzello, V.; Galiuto, L.; Natale, L.; Giordano, A.; Rebuzzi, A.; Loperfido, F.; Crea, F.; Maseri, A. Assessment of resting perfusion defects in patients with acute myocardial infarction: Comparison of myocardial contrast echocardiography, combined first-pass/delayed contrast-enhanced magnetic resonance imaging and 99mTC-sestamibi SPECT. Int. J. Cardiovasc. Imaging 2006, 22, 417–428. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A.; Hollenberg, S.M.; et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation 2011, 124, e574–e651. [Google Scholar] [PubMed]
- Yanamala, C.M.; Bundhun, P.K.; Ahmed, A. Comparing mortality between fibrinolysis and primary percutaneous coronary intervention in patients with acute myocardial infarction: A systematic review and meta-analysis of 27 randomized-controlled trials including 11,429 patients. Coron. Artery Dis. 2017, 28, 315–325. [Google Scholar] [CrossRef]
- Aversano, T.; Aversano, L.T.; Passamani, E.; Knatterud, G.L.; Terrin, M.L.; Williams, D.O.; Forman, S.A.; Atlantic Cardiovascular Patient Outcomes Research Team (C-PORT). Thrombolytic therapy vs. primary percutaneous coronary intervention for myocardial infarction in patients presenting to hospitals without on-site cardiac surgery: A randomized controlled trial. JAMA 2002, 287, 1943–1951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silber, S.; Albertsson, P.; Avilés, F.F.; Camici, P.G.; Colombo, A.; Hamm, C.; Jørgensen, E.; Marco, J.; Nordrehaug, J.E.; Ruzyllo, W.; et al. Guidelines for percutaneous coronary interventions. The Task Force for Percutaneous Coronary Interventions of the European Society of Cardiology. Eur. Heart J. 2005, 26, 804–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Loon, R.B.; Veen, G.; Baur, L.H.; Twisk, J.W.; van Rossum, A.C. Long-term follow-up of the viability guided angioplasty after acute myocardial infarction (VIAMI) trial. Int. J. Cardiol. 2015, 186, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Cheng, R.C.; Li, X. Microvascular dysfunction in remote myocardium predict left ventricular remodelling in acute infarction. Heart 2013, 3, A175–A176. [Google Scholar] [CrossRef]
- Cheng, R.; Wei, G.; Yu, L.; Su, Z.; Wei, L.; Bai, X.; Tian, J.; Li, X. Coronary flow reserve in the remote myocardium predicts left ventricular remodeling following acute myocardial infarction. Yonsei Med. J. 2014, 55, 904–911. [Google Scholar] [CrossRef] [Green Version]
- Cheng, R.; Zhu, X.; Li, Y.; Bai, X.; Xue, L.; Wei, L. Coronary flow reserve in non-infarcted myocardium predicts long-term clinical outcomes in patients undergoing percutaneous coronary intervention. Yonsei Med. J. 2018, 59, 252–257. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Patients (n) | Age (Years) Mean ± SD | Men (%) | DM (%) | HT (%) | Smoker | Hyperlipidemia | Family History of CAD | Follow-Up Years, ms |
|---|---|---|---|---|---|---|---|---|---|---|
| Bolognese et al. [21] | 2004 | 124 | 62 ± 10 | 84 | 10 | 36 | 43 | 27 | N/A | mean 46 ± 32 |
| Khumri et al. [22] | 2006 | 167 | 61.6 ± 14.7 | 61.1 | 18.0 | 56.9 | 57 | 34.1 | N/A | mean 39 |
| Dwivedi et al. [16] | 2007 | 95 | 61 ± 10.8 | 75.8 | 26 | 32 | 42 | 44 | 27 | mean 46 ± 16 |
| Olszowska et al. [14] | 2010 | 86 | 58.4 ± 11.2 | 79.1 | 26 | 60 | 44 | 77 | 36 | mean 34 (range, 14–37) |
| Abdelmoneim et al. [17] | 2015 | 37 | 64 ± 14 | 73.0 | 27 | 73 | 65 | 86 | 146 | mean 14 ± 7 (median 17) |
| Lenz et al. [13] | 2016 | 27 | 62 ± 13 | 70.4 | 29.6 | 74.1 | 70.4 | 85.2 | 55.6 | mean 42 ± 31 (median 54) |
| Pooled | 536 | |||||||||
| Study | Inclusion | Exclusion | Treatment | Primary Endpoints | ||||||
| Bolognese et al. [21] | (1) first AMI (2) successful primary PTCA within 6 h of the onset of symptoms or between 6 and 24 h if there was evidence of continuing ischemia | (1) IRA diameter stenosis 70% or inability to identify IRA, (2) HF or cardiogenic shock in the first week after infarction, (3) postinfarction angina, (4) significant other cardiac disease, (5) life-limiting noncardiac disease. | 100% PTCA | MACE, including cardiac death, NFMI, hospitalization for congestive HF and combined events | ||||||
| Khumri et al. [22] | (1) recent myocardial necrosis, (2) wall motion abnormalities, (3) coronary angiography before MCE. | (1) Patients with previous anterior wall AMI; (2) technically difficult to perform MCE | medical therapy | (1) all-cause mortality (2) a combined end point of mortality or heart failure | ||||||
| Dwivedi et al. [16] | Patients shortly after their first presentation with AMI. | N/A | 68% revascularization; 87% thrombolysis | (1) Cardiac death; (2) Cardiac death or NFMI | ||||||
| Olszowska et al. [14] | Patients underwent PCI within 12 h of an anterior AMI. | Hemodynamically unstable patients | 100% PCI | (1) Cardiac death (2) Other cardiac events: NFMI, recurrent angina with TLR or repeat hospitalization for congestive HF | ||||||
| Abdelmoneim et al. [17] | Patients with evidence of STEMI. | N/A | 84% coronary intervention 5% fibrinolytic therapy only | Any cardiac events including hard events (all-cause mortality; NFMI) | ||||||
| Lenz et al. [13] | Patents with STEMI and TIMI III flow | N/A | 85.2% coronary intervention | Any cardiac events: (1) hard events (all-cause mortality; NFMI) (2) soft events (development of typical angina; hospitalization for arrhythmias, chest pain, unstable angina or to rule out MI; cardiac revascularization; and/or development of HF) | ||||||
| Study | The Number of Cardiac Events (n) | Multivariable RR | ||
|---|---|---|---|---|
| Total Cardiac Events | Cardiac Deaths | Total Cardiac Events | Cardiac Death | |
| Bolognese L et al. [21] | 14 | 9 | OR, 2.27; 95% CI, 1.18–4.35, p = 0.01 | OR, 3.85; 95% CI, 1.39–11.1, p = 0.01 |
| Khumri TM et al. [22] | N/A | 18 | N/A | OR, 4.5; 95% CI, 1.3–15.4, p = 0.02 |
| Dwivedi et al. [16] | 15 | 8 | HR, 1.26; 95% CI,1.09–1.44; p = 0.002 | HR,1.37; 95% CI,1.08–1.75; p = 0.01 |
| Olszowska et al. [14] | 17 | 4 | HR, 2.4; 95% CI, 1.21–2.6; p = 0.02 | |
| Abdelmoneim et al. [17] | 22 | 4 | HR, 3.41; 95% CI,1.19–12.27; p = 0.020 | |
| Lenz et al. [13] | 23 | 6 | HR, 3.91; 95% CI,0.96–21.8; p = 0.057 | |
| Study | Characteristics of MCE | Semiquantitative System | |||
|---|---|---|---|---|---|
| No. of Segments | Contrast Agents | Time to Perform MCE | Definition of Semiquantitative Parameters | Semiquantitative Scoring System | |
| Bolognese et al. [21] | 16 | iopamidol | shortly after PTCA | adding contrast scores of all segments and dividing by the total number of evaluable segments. | homogenous contrast perfusion = 2; partial/patchy contrast perfusion = 1; absent contrast perfusion = 0. |
| Khumri et al. [22] | 16 | Optison and Definity | a mean of 2 days (range 0 to 11) after AMI | a sum of the values for all interpretable segments divided by the number of segments analyzed | homogenous contrast perfusion = 1; partial/patchy contrast perfusion = 2; absent contrast perfusion = 3. |
| Dwivedi et al. [16] | 16 | 40 patients, Optison; 55 patients, Sonovue | within 7 ± 2 days after AMI | Same as Dwivedi et al. [16] | Same as Khumri TM et al. [22] |
| Olszowska et al. [14] | 16 | Optison | within 5 ± 2 days after PCI | Same as Dwivedi et al. [16] | Same as Khumri TM et al. [22] |
| Abdelmoneim et al. [17] | 17 | Definity | within a mean (SD) of 29.3 (21) h of the CA | Same as Dwivedi et al. [16] | Same as Khumri TM et al. [22] |
| Lenz et al. [13] | 17 | Definity | within 1.04 ± 0.8 days after catheterization | Same as Dwivedi et al. [16] | homogenous contrast perfusion = 0; partial/patchy contrast perfusion = 1; absent contrast perfusion = 2. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Yang, M.; Yang, Z.; Ye, L.; Luo, H.; Guo, Y. Long-Term Prognostic Value of Myocardial Viability by Myocardial Contrast Echocardiography in Patients after Acute Myocardial Infarction: A Systematic Review and Meta-Analysis. Medicina 2022, 58, 1429. https://doi.org/10.3390/medicina58101429
Wang J, Yang M, Yang Z, Ye L, Luo H, Guo Y. Long-Term Prognostic Value of Myocardial Viability by Myocardial Contrast Echocardiography in Patients after Acute Myocardial Infarction: A Systematic Review and Meta-Analysis. Medicina. 2022; 58(10):1429. https://doi.org/10.3390/medicina58101429
Chicago/Turabian StyleWang, Jingxin, Mengxi Yang, Zhi Yang, Lu Ye, Hong Luo, and Yingkun Guo. 2022. "Long-Term Prognostic Value of Myocardial Viability by Myocardial Contrast Echocardiography in Patients after Acute Myocardial Infarction: A Systematic Review and Meta-Analysis" Medicina 58, no. 10: 1429. https://doi.org/10.3390/medicina58101429