
Prediction of Prognosis in Patients with Trauma by Using Machine Learning
 and
and
Abstract
:1. Introduction
2. Methods
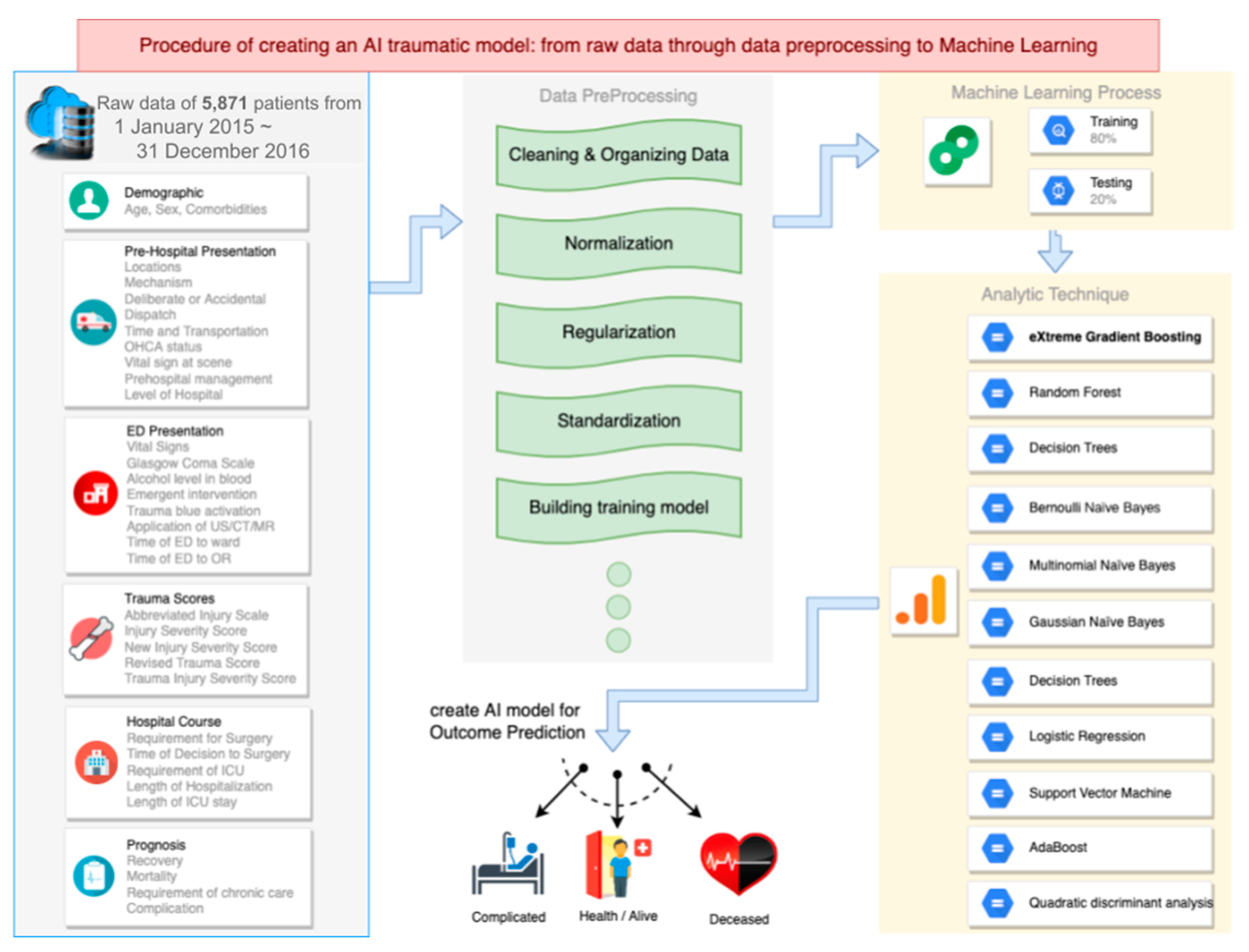
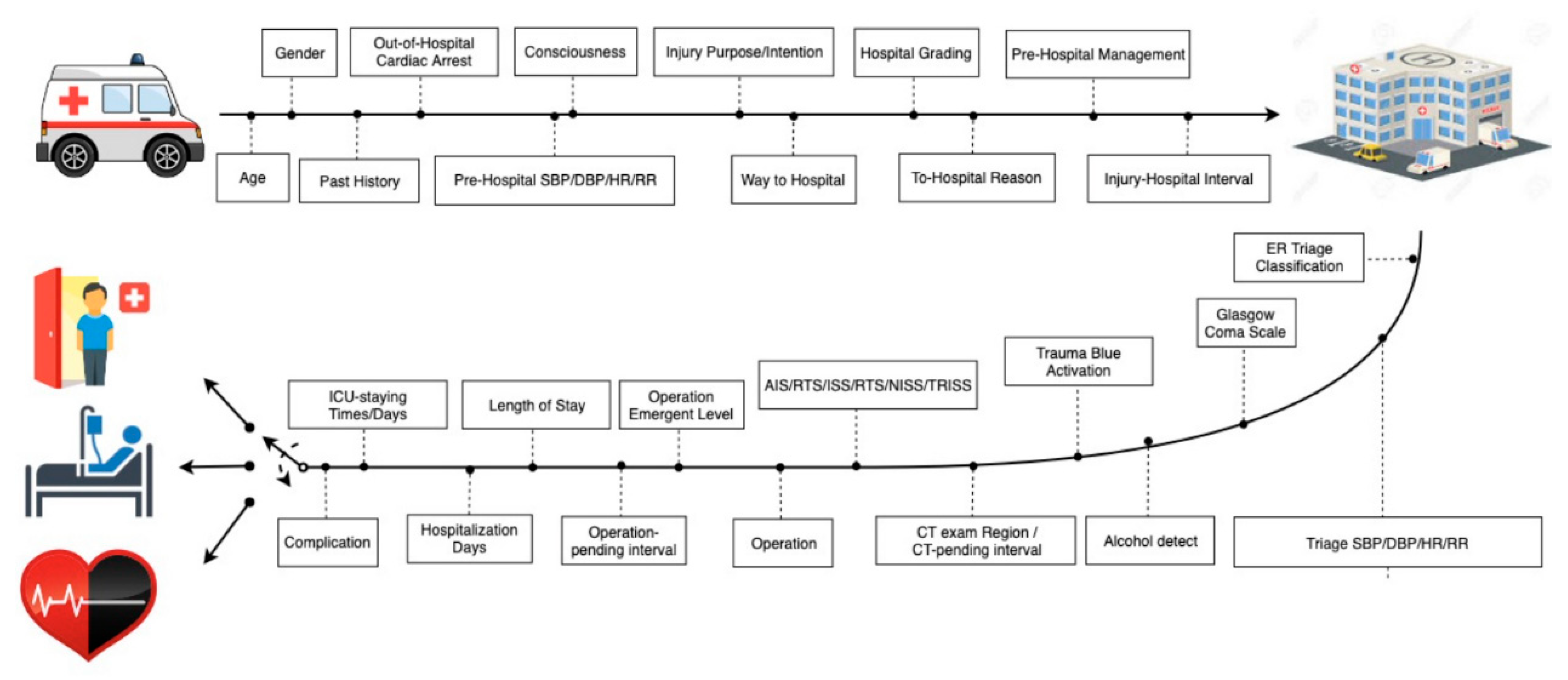
2.1. Dataset Management and ML Technique
2.2. ML Model Prototype
3. Results
3.1. Description of Dataset
3.2. Models
3.3. Complete Model and High-Ranking Features
3.4. Short-Term Model and High-Ranking Features
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. XGBoost
References
- Ministry of Health and Welfare: Statistics and Publications: Statistics: Cause of Death Statistics 2019. Available online: https://www.mohw.gov.tw/lp-4964-2.html (accessed on 1 May 2020).
- Centers for Disease Control and Prevention: Minority Health and Health Equity: Leading Causes of Death. 2017. Available online: https://www.cdc.gov/healthequity/lcod/index.htm (accessed on 1 May 2020).
- World Health Organization. Global Health Observatory Data: 2016 Update; World Health Organization Press: Geneva, Switzerland, 2020; Available online: https://www.who.int/gho/mortality_burden_disease/causes_death/top_10/en/ (accessed on 1 May 2020).
- Kim, D.; You, S.; So, S.; Lee, J.; Yook, S.; Jang, D.P.; Kim, I.Y.; Park, E.; Cho, K.; Cha, W.C.; et al. A data-driven artificial intelligence model for remote triage in the prehospital environment. PLoS ONE 2018, 13, e0206006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muisyo, T.; Bernardo, E.O.; Camazine, M.; Colvin, R.; Thomas, K.A.; Borgman, M.A.; Spinella, P.C. Mortality prediction in pediatric trauma. J. Pediatric Surg. 2019, 54, 1613–1616. [Google Scholar] [CrossRef] [PubMed]
- Kuo, P.J.; Wu, S.C.; Chien, P.C.; Rau, C.S.; Chen, Y.C.; Hsieh, H.Y.; Hsieh, C.H. Derivation and validation of different machine-learning models in mortality prediction of trauma in motorcycle riders: A cross-sectional retrospective study in southern Taiwan. BMJ Open 2018, 8, e018252. [Google Scholar] [CrossRef] [PubMed]
- Harvin, J.A.; Green, C.E.; Pedroza, C.; Tyson, J.E.; Moore, L.J.; Wade, C.E.; Holcomb, J.B.; Kao, L.S. Using Machine Learning to Identify Change in Surgical Decision Making in Current Use of Damage Control Laparotomy. J. Am. Coll. Surg. 2019, 228, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Rau, C.S.; Kuo, P.J.; Chien, P.C.; Huang, C.Y.; Hsieh, H.Y.; Hsieh, C.H. Mortality prediction in patients with isolated moderate and severe traumatic brain injury using machine learning models. PLoS ONE. 2018, 13, e0207192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahab, L.; Jiang, H.A. Comparative study on machine learning based algorithms for prediction of motorcycle crash severity. PLoS ONE 2019, 14, e0214966. [Google Scholar]
- Christie, S.A.; Conroy, A.S.; Callcut, R.A.; Hubbard, A.E.; Cohen, M.J. Dynamic multi-outcome prediction after injury: Applying adaptive machine learning for precision medicine in trauma. PLoS ONE 2019, 14, e0213836. [Google Scholar] [CrossRef] [PubMed]
- Cobb, A.N.; Daungjaiboon, W.; Brownlee, S.A.; Baldea, A.J.; Sanford, A.P.; Mosier, M.M.; Kuo, P.C. Seeing the forest beyond the trees: Predicting survival in burn patients with machine learning. Am. J. Surg. 2018, 215, 411–416. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Müller, A.; Nothman, J.; Louppe, G.; et al. Scikit-learn algorithm cheat-sheet: Machine learning in Python. JMLR 2011, 12, 2825–2830. [Google Scholar]
- Hasan, K.; Alam, A.; Das, D.; Hossain, E.; Hasan, M. Diabetes prediction using ensembling of different machine learning classifiers. IEEE Access 2020, 8, 76516–76531. [Google Scholar] [CrossRef]
- Parreco, J.; Hidalgo, A.; Parks, J.J.; Kozol, R.; Rattan, R. Using artificial intelligence to predict prolonged mechanical ventilation and tracheostomy placement. J. Surg. Res. 2018, 228, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Sefrioui, I.; Amadini, R.; Mauro, J.; El Fallahi, A.; Gabbrielli, M. Survival prediction of trauma patients: A study on US National Trauma Data Bank. Eur. J Trauma Emerg. Surg. 2017, 43, 805–822. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.J.; Yen, Z.S.; Tsai, J.C.H.; Chen, L.C.; Lin, S.J.; Sang, Y.Y.; Chen, J.C.; TTAS National Working Group. Validation of the Taiwan triage and acuity scale: A new computerised five-level triage system. Emerg Med J. 2011, 28, 1026–1031. [Google Scholar] [CrossRef] [PubMed]
- Fortuny, E.J.; Martens, D.; Provost, F. Predictive Modeling with Big Data: Is Bigger Really Better? Big Data 2014, 1, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Hale, A.T.; Stonko, D.P.; Lim, J.; Guillamondegui, O.D.; Shannon, C.N.; Patel, M.B. Using an artificial neural network to predict traumatic brain injury. J. Neurosurg. Pediatrics 2018, 23, 219–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, C.-C.; Liu, H.-T.; Rau, C.-S.; Hsu, S.-Y.; Hsieh, H.-Y.; Hsieh, C.-H. Motorcycle-related hospitalization of adolescents in a Level I trauma center in southern Taiwan: A cross-sectional study. BMC Pediatrics 2015, 15, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, S.E.; Decker, A.; Hubbard, A.; Callcut, R.A.; Fox, E.E.; Del Junco, D.J.; Holcomb, J.B.; Rahbar, M.H.; Wade, C.E.; Schreiber, M.A.; et al. Statistical Machines for Trauma Hospital Outcomes Research: Application to the PRospective, Observational, Multi-Center Major Trauma Transfusion (PROMMTT) Study. PLoS ONE 2015, 10, e0136438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christie, S.A.; Hubbard, A.E.; Callcut, R.A.; Hameed, M.; Dissak-Delon, F.N.; Mekolo, D.; Saidou, A.; Mefire, A.C.; Nsongoo, P.; Dicker, R.A. Machine learning without borders? An adaptable tool to optimize mortality prediction in diverse clinical settings. J Trauma Acute Care Surg. 2018, 85, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.T.; Salinas, J. Machine learning for predicting outcomes in trauma. Shock 2017, 48, 504–510. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | |
| Geriatric patients (>55 years) | 43.8% |
| Non-geriatric adults | 50.1% |
| Pediatric patients (<15 years) | 6.1% |
| Sex | |
| Male | 57.9% |
| Female | 42.1% |
| Transport type | |
| By Emergency Medical Services | 51% |
| By patient’s family or friends | 29.1% |
| Transfer from other hospitals | 19.9% |
| Triage | 2.4 ± 0.6 (mean ± SD) |
| I | 7.9% |
| II | 44.8% |
| III | 47.3% |
| Hospital stays | |
| <7 days | 66.7% |
| 7–30 days | 28.9% |
| >30 days | 4.4% |
| Requirement for intensive care | 17.3% |
| Requirement for surgery | 69.6% |
| Abbreviated Injury Scale ≥ 3 | |
| extremities | 24.4% |
| head | 21.4% |
| chest | 8.5% |
| abdomen | 3.2% |
| face | 0.6% |
| external | 0.6% |
| Major trauma (ISS >15) | 20.7% |
| Trauma scores | (mean ± SD) |
| Injury severity score (ISS) | 9.7 ± 8.8 |
| New injury severity score | 11.7 ± 10.5 |
| Revised trauma score | 7.6560 ± 0.7414 |
| Trauma injury severity score | 0.9543 ± 0.1267 |
| Complete Model | Short-Term Model | |
|---|---|---|
| Recovery | 86% | 89% |
| Chronic Care | 30% | 25% |
| Mortality | 67% | 41% |
| Complication | 80% | |
| High-ranking features | ||
| 1 | Trauma injury severity score | Trauma injury severity score |
| 2 | Abbreviated injury scale of head | Abbreviated injury scale of head |
| 3 | Dispatch of emergency medical service | Dispatch of emergency medical service |
| 4 | Triage | time from injury sites to the hospital |
| 5 | New injury severity score | New injury severity score |
| 6 | Time from injury sites to the hospital | Glasgow Coma Scale in ED |
| 7 | Requirement for intensive care | Triage |
| 8 | Length of hospital stay | transportation from injury sites to the hospital |
| 9 | Glasgow Coma Scale in ED | Gender |
| 10 | Prehospital managements by emergency medical technicians | Prehospital managements by emergency medical technicians |
| 11 | Revised trauma score | Level of transferred hospital |
| 12 | Prehospital consciousness | Time from surgical decision to surgery |
| 13 | Transportation from injury sites to the hospital | Deliberate or accidental injury |
| 14 | Comorbidity | Comorbidity |
| 15 | Deliberate or accidental injury | Age |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.-C.; Hsu, C.-C.; Lin, T.-C.; Chiang, H.-F.; Horng, G.-J.; Chen, K.-T. Prediction of Prognosis in Patients with Trauma by Using Machine Learning. Medicina 2022, 58, 1379. https://doi.org/10.3390/medicina58101379
Lee K-C, Hsu C-C, Lin T-C, Chiang H-F, Horng G-J, Chen K-T. Prediction of Prognosis in Patients with Trauma by Using Machine Learning. Medicina. 2022; 58(10):1379. https://doi.org/10.3390/medicina58101379
Chicago/Turabian StyleLee, Kuo-Chang, Chien-Chin Hsu, Tzu-Chieh Lin, Hsiu-Fen Chiang, Gwo-Jiun Horng, and Kuo-Tai Chen. 2022. "Prediction of Prognosis in Patients with Trauma by Using Machine Learning" Medicina 58, no. 10: 1379. https://doi.org/10.3390/medicina58101379