
Light Transmission of Various Aesthetic Posts at Different Depths and Its Effect on Push-Out Bond Strength, Microhardness of Luting Cement

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Microhardness and Push-Out Bond Strength Test
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
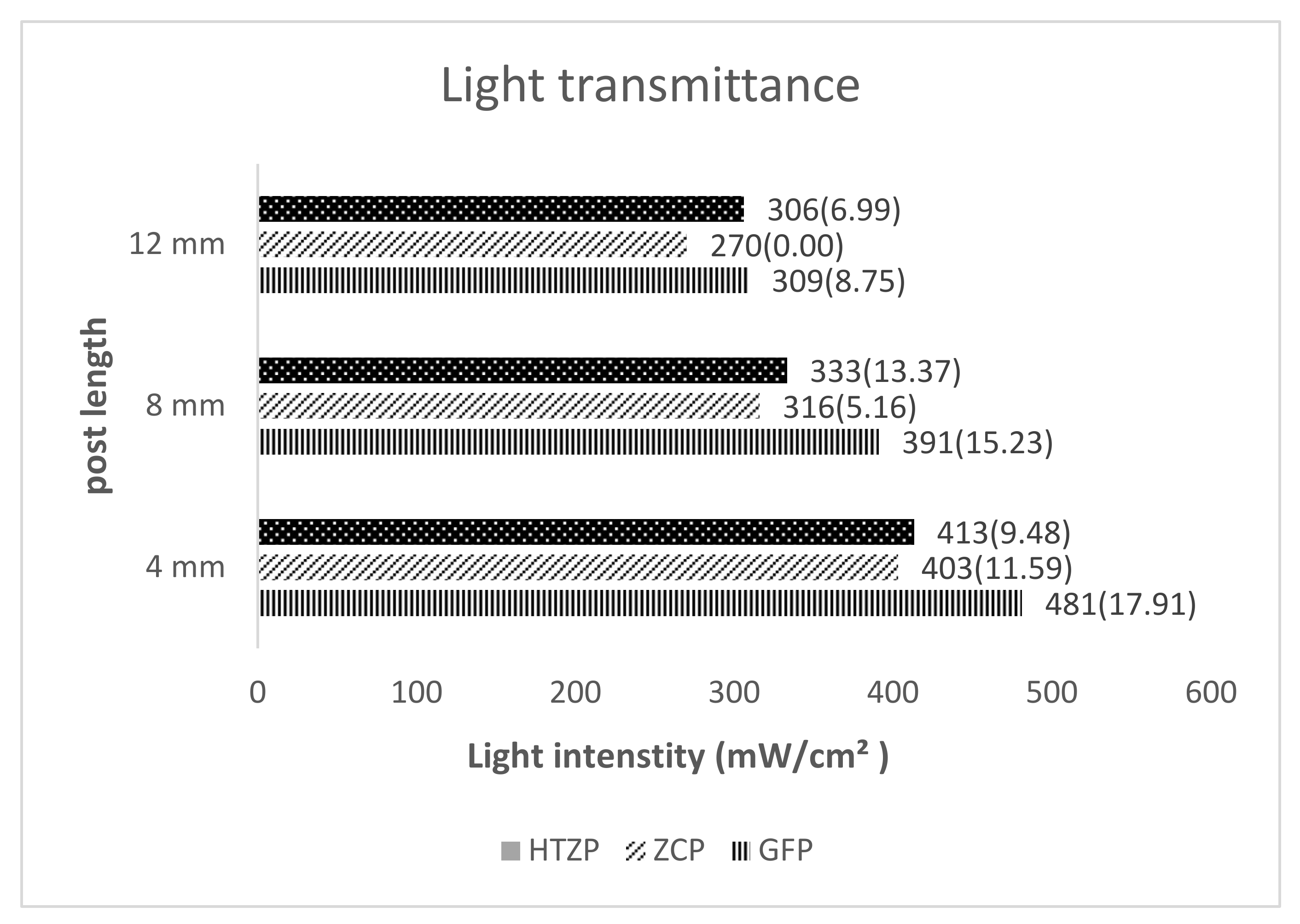
- The light intensity attenuation with increased depth was observed in all tested posts;
- The fiber-reinforced composite post showed the highest light transmission intensity at different lengths compared to the high translucent post and ceramic zirconia post;
- Microhardness of luting cement was consistently higher at cervical cross section across all the posts and recorded highest in the GFP post;
- Push-out bond strength was correlated with microhardness of luting cement; GFP post recorded the maximum strength at the cervical cross section.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arab, K.; Barasain, O.; Altaweel, A.; Alkhayyal, J.; Alshiha, L.; Barasain, R.; Alessa, R.; Alshaalan, H. Influence of social media on the decision to undergo a cosmetic procedure. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmood, R.N.; Anwar, A. Assessment of psychosocial impact of dental aesthetics and self perceived orthodontic treatment need in young adults. Pak. Oral Dent. J. 2014, 34. [Google Scholar]
- Zarone, F.; Di Mauro, M.I.; Ausiello, P.; Ruggiero, G.; Sorrentino, R. Current status on lithium disilicate and zirconia: A narrative review. BMC Oral Health 2019, 19, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes, G.C.; Baratieri, L.N.; de Andrada, M.A.; Maia, H.P. All-ceramic post, core, and crown: Technique and case report. J. Esthet. Restor. Dent. 2001, 13, 285. [Google Scholar] [CrossRef] [PubMed]
- Stewardson, D.A.; Shortall, A.C.; Marquis, P.M. The effect of the elastic modulus of endodontic posts on static load failure. Int. Endod. J. 2011, 44, 458–468. [Google Scholar] [CrossRef]
- Koutayas, S.O.; Kern, M. All-ceramic posts and cores: The state of the art. Quintessence Int. 1999, 30, 383–392. [Google Scholar]
- Santos, A.F.; Meira, J.B.; Tanaka, C.B.; Xavier, T.A.; Ballester, R.Y.; Lima, R.G.; Pfeifer, C.S.; Versluis, A. Can fiber posts increase root stresses and reduce fracture? J. Dent. Res. 2010, 89, 587–591. [Google Scholar] [CrossRef]
- Bouillaguet, S.; Troesch, S.; Wataha, J.C.; Krejci, I.; Meyer, J.M.; Pashley, D.H. Microtensile bond strength between adhesive cements and root canal dentin. Dent. Mater. 2003, 19, 199–205. [Google Scholar] [CrossRef] [Green Version]
- Shiratori, F.K.; do Valle, A.L.; Pegoraro, T.A.; Carvalho, R.M.; Pereira, J.R. Influence of technique and manipulation on self-adhesive resin cements used to cement intraradicular posts. J. Prosthet. Dent. 2013, 110, 56–60. [Google Scholar] [CrossRef]
- Passos, S.P.; Souza, R.O.; Michida, S.M.; Zamboni, S.C.; Oliveira, S.H. Effects of cement-curing mode and light-curing unit on the bond durability of ceramic cemented to dentin. Braz. Oral Res. 2013, 27, 169–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lui, J.L. Depth of composite polymerization within simulated root canals using light-transmitting posts. Oper. Dent. 1994, 19, 165–168. [Google Scholar]
- Kumbuloglu, O.; Lassila, L.V.; User, A.; Vallittu, P.K. A study of the physical and chemical properties of four resin composite luting cements. Int. J. Prosthodont. 2004, 17, 357–363. [Google Scholar]
- Braga, R.R.; Cesar, P.F.; Gonzaga, C.C. Mechanical properties of resin cements with different activation modes. J. Oral Rehabil. 2002, 29, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Caughman, W.F.; Chan, D.C.; Rueggeberg, F.A. Curing potential of dual-polymerizable resin cements in simulated clinical situations. J. Prosthet. Dent. 2001, 85, 479–484. [Google Scholar] [CrossRef]
- Barfeie, A.; Thomas, M.B.; Watts, A.; Rees, J. Failure Mechanisms of Fibre Posts: A Literature Review. Eur. J. Prosthodont. Restor. Dent. 2015, 23, P115–P127. [Google Scholar] [PubMed]
- Cekic-Nagas, I.; Ergun, G.; Egilmez, F. Light transmittance of fiber posts following various surface treatments: A preliminary study. Eur. J. Dent. 2016, 10, 230–233. [Google Scholar] [CrossRef] [Green Version]
- Goracci, C.; Corciolani, G.; Vichi, A.; Ferrari, M. Light-transmitting ability of marketed fiber posts. J. Dent. Res. 2008, 87, 1122–1126. [Google Scholar] [CrossRef]
- Moazzami, S.M.; Kazemi, R.; Alami, M.; Attaran, E.; Mehhary, M.; Sarmad, M.; Shahrokh, H. Light conduction capability of different light-transmitting FRC posts. J. Dent. Mater. Tech. 2012, 1, 40–46. [Google Scholar]
- Vieira, C.; Bachmann, L.; Chaves, C.D.; Silva-Sousa, Y.T.; Da Silva, S.R.; Alfredo, E. Light transmission and bond strength of glass fiber posts submitted to different surface treatments. J. Prosthet. Dent. 2021, 125, 674.e1–674.e7. [Google Scholar] [CrossRef] [PubMed]
- Darwell, B.W. Materilas Science for Dentistry, 7th ed.; Woodhead Publishing: Sawston, UK, 2002; pp. 507–508, 510. [Google Scholar]
- Omidi, B.R.; Gosili, A.; Jaber-Ansari, M.; Mahdkhah, A. Intensity output and effectiveness of light curing units in dental offices. J. Clin. Exp. Dent. 2018, 10, e555. [Google Scholar] [CrossRef]
- Li, Q.; Lin, H.L.; Zheng, M.; Ozcan, M.; Yu, H. Minimum Radiant Exposure and Irradiance for Triggering Adequate Polymerization of a Photo-Polymerized Resin Cement. Materials 2021, 14, 2341. [Google Scholar] [CrossRef] [PubMed]
- Rueggeberg, F.A.; Caughman, W.F.; Curtis, J.W. Effect of light intensity and exposure duration on cure of resin composite. Oper. Dent. 1994, 19, 26–32. [Google Scholar] [PubMed]
- Anusavice, K.J.; Shen, C.; Rawls, H.R. Phillips’ Science of Dental Materials; Saunder: Philadelphia, PA, USA, 2012. [Google Scholar]
- Soares, C.J.; Mitsui, F.H.; Neto, F.H.; Marchi, G.M.; Martins, L.R. Radiodensity evaluation of seven root post systems. Am. J. Dent. 2005, 18, 57–60. [Google Scholar] [PubMed]
- Morgan, L.F.; da Cunha Peixoto, R.T.; de Castro Albuquerque, R.; Corrêa, M.F.; de Abreu Poletto, L.T.; Pinotti, M.B. Light transmission through a translucent fiber post. J. Endod. 2008, 34, 299–302. [Google Scholar] [CrossRef]
- McLaren, E.A.; Lawson, N.; Choi, J.; Kang, J.; Trujillo, C. New High-Translucent Cubic-Phase–Containing Zirconia: Clinical and Laboratory Considerations and the Effect of Air Abrasion on Strength. Compendium 2017, 38, 1–9. [Google Scholar]
- Zhang, Y.; Lawn, B.R. Novel zirconia materials in dentistry. J. Dent. Res. 2018, 97, 140–147. [Google Scholar] [CrossRef]
- Kim, H.K. Optical and Mechanical Properties of Highly Translucent Dental Zirconia. Materials 2020, 13, 3395. [Google Scholar] [CrossRef]
- Zhang, F.; Inokoshi, M.; Batuk, M.; Hadermann, J.; Naert, I.; Van Meerbeek, B.; Vleugels, J. Strength, toughness and aging stability of highly-translucent Y-TZP ceramics for dental restorations. Dent. Mater. 2016, 32, e327–e337. [Google Scholar] [CrossRef] [PubMed]
- Rueggeberg, F.A.; Caughman, W.F.; Curtis, J.W., Jr.; Davis, H.C. Factors affecting cure at depths within light-activated resin composites. Am. J. Dent. 1993, 6, 91–95. [Google Scholar]
- Yap, A.U. Effectiveness of polymerization in composite restoratives claiming bulk placement: Impact of cavity depth and exposure time. Oper. Dent. 2000, 25, 113–120. [Google Scholar]
- e Silva, A.L.; Arias, V.G.; Soares, L.E.; Martin, A.A.; Martins, L.R. Influence of fiber-post translucency on the degree of conversion of a dual-cured resin cement. J. Endod. 2007, 33, 303–305. [Google Scholar]
- Strassler, H.E.; Marchiori, R. Using Luscent Anchors to esthetically restore and reinforce flared root canals. Contemp. Esthet. Restorat. Pract. 2001, 86–88. [Google Scholar]
- Freedman, G.; Novak, I.M.; Serota, K.S.; Glassman, G.D. Intra-radicular rehabilitation: A clinical approach. Pract. Periodontics Aesthetic Dent. PPAD 1994, 6, 33–39. [Google Scholar]
- Roberts, H.W.; Leonard, D.L.; Vandewalle, K.S.; Cohen, M.E.; Charlton, D.G. The effect of a translucent post on resin composite depth of cure. Dent. Mater. 2004, 20, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Stylianou, A.; Burgess, J.O.; Liu, P.R.; Givan, D.A.; Lawson, N.C. Light-transmitting fiber optic posts: An in vitro evaluation. J. Prosthet. Dent. 2017, 117, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Kim, S.K.; Kim, K.H.; Kwon, T.Y. Degree of conversion of dual-cured resin cement light-cured through three fibre posts within human root canals: An ex vivo study. Int. Endod. J. 2009, 42, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Ferracane, J.L. Correlation between hardness and degree of conversion during the setting reaction of unfilled dental restorative resins. Dent. Mater. 1985, 1, 11–14. [Google Scholar] [CrossRef]
- Silva Junior, J.E.; Amaral, F.L.; França, F.M.; Turssi, C.P.; Basting, R.T. Influence of glass fiber post translucency on microhardness and dentin bond strength of resin cement at different root levels. J. Adhes. Sci. Technol. 2016, 30, 594–606. [Google Scholar] [CrossRef]
- Ceballos, L.; Garrido, M.A.; Fuentes, V.; Rodríguez, J. Mechanical characterization of resin cements used for luting fiber posts by nanoindentation. Dent. Mater. 2007, 23, 100–105. [Google Scholar] [CrossRef]
- Özcan, M.; Zambonι, S.; Valandro, F.; Bottιno, M.; Bagis, B. Microhardness of dual-polymerized resin cement around a translucent fiber post in the intraradicular environment. J. Conserv. Dent. JCD 2011, 14, 370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, V.J.; Chen, Y.M.; Yip, K.H.; Smales, R.J.; Meng, Q.F.; Chen, L. Effect of two fiber post types and two luting cement systems on regional post retention using the push-out test. Dent. Mater. 2008, 24, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Reges, R.V.; Moraes, R.R.; Correr, A.B.; Sinhoreti, M.A.; Correr-Sobrinho, L.; Piva, E.; Nouer, P.R. In-depth polymerization of dual-cured resin cement assessed by hardness. J. Biomater. Appl. 2008, 23, 85–96. [Google Scholar] [CrossRef]
- Moraes, R.R.; Boscato, N.; Jardim, P.S.; Schneider, L.F. Dual and self-curing potential of self-adhesive resin cements as thin films. Oper. Dent. 2011, 36, 635–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reginato, C.F.; Oliveira, A.S.; Kaizer, M.R.; Jardim, P.S.; Moraes, R.R. Polymerization efficiency through translucent and opaque fiber posts and bonding to root dentin. J. Prosthodont. Res. 2013, 57, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Szesz, A.; Cuadros-Sanchez, J.; Hass, V.; da Cruz, G.K.; Arrais, C.A.; Reis, A.; Loguercio, A.D. Influence of delivered radiant exposure values on bonding of fiber posts to root canals. J. Adhes. Dent. 2015, 17, 181–188. [Google Scholar] [PubMed]
- Dietschi, D.; Duc, O.; Krejci, I.; Sadan, A. Biomechanical considerations for the restoration of endodontically treated teeth: A systematic review of the literature-Part 1. Composition and micro-and macrostructure alterations. Quintessence Int. 2007, 38, 733–743. [Google Scholar]
- Quitero, M.F.; Garone-Netto, N.; de Freitas, P.M.; de Cerqueira Luz, M.A. Effect of post translucency on bond strength of different resin luting agents to root dentin. J. Prosthet. Dent. 2014, 111, 35–41. [Google Scholar] [CrossRef]
- Mjör, I.A.; Nordahl, I. The density and branching of dentinal tubules in human teeth. Arch. Oral Biol. 1996, 41, 401–412. [Google Scholar] [CrossRef]
- Tamura, Y.; Tsubota, K.; Otsuka, E.; Endo, H.; Takubo, C.; Miyazaki, M.; Latta, M.A. Dentin bonding: Influence of bonded surface area and crosshead speed on bond strength. Dent. Mater. J. 2011, 30, 206–211. [Google Scholar] [CrossRef] [Green Version]
- Sano, H.; Shono, T.; Sonoda, H.; Takatsu, T.; Ciucchi, B.; Carvalho, R.; Pashley, D.H. Relationship between surface area for adhesion and tensile bond strength—evaluation of a micro-tensile bond test. Dent. Mater. 1994, 10, 236–240. [Google Scholar] [CrossRef]
- Akgungor, G.; Akkayan, B. Influence of dentin bonding agents and polymerization modes on the bond strength between translucent fiber posts and three dentin regions within a post space. J. Prosthet. Dent. 2006, 95, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Alshammary, F.; Karobari, M.I.; Assiry, A.A.; Marya, A.; Shaikh, G.M.; Siddiqui, A.A.; Alam, M.K. Effect of Nd: YAG, Er, Cr: YSGG Laser Irradiation, and Adjunctive Photodynamic Therapy on Push-Out Bond Strength of Zirconia Posts to Radicular Dentin. BioMed Res. Int. 2021, 2021, 5523242. [Google Scholar] [CrossRef] [PubMed]
- Allabban, M.N.; Youssef, S.A.; Nejri, A.A.; Qudaih, M.A. Evaluation of Bond Strength of Aesthetic Type of Posts at Different Regions of Root Canal after Application of Adhesive Resin Cement. Open Access Maced. J. Med. Sci. 2019, 7, 2167–2172. [Google Scholar] [CrossRef] [PubMed] [Green Version]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haralur, S.B.; Alasmari, T.A.; Alasmari, M.H.; Hakami, H.M. Light Transmission of Various Aesthetic Posts at Different Depths and Its Effect on Push-Out Bond Strength, Microhardness of Luting Cement. Medicina 2022, 58, 75. https://doi.org/10.3390/medicina58010075
Haralur SB, Alasmari TA, Alasmari MH, Hakami HM. Light Transmission of Various Aesthetic Posts at Different Depths and Its Effect on Push-Out Bond Strength, Microhardness of Luting Cement. Medicina. 2022; 58(1):75. https://doi.org/10.3390/medicina58010075
Chicago/Turabian StyleHaralur, Satheesh B., Turki Abdullah Alasmari, Mohammed Hussin Alasmari, and Hafiz Mohammed Hakami. 2022. "Light Transmission of Various Aesthetic Posts at Different Depths and Its Effect on Push-Out Bond Strength, Microhardness of Luting Cement" Medicina 58, no. 1: 75. https://doi.org/10.3390/medicina58010075