
Autologous Tooth Dentin Graft: A Retrospective Study in Humans

 and
and
Abstract
:1. Introduction
2. Materials and Methods:
2.1. Patients
- Aged ≥ 25 years and committed to participate in up to a 3-month follow-up.
- Upper and lower teeth with indications to be extracted.
- Human immunodeficiency virus infection.
- Presence of metabolic, endocrine, blood, neoplastic, or renal diseases.
- Alcoholism or drug abuse.
- Smoking >10 cigarettes per day.
- Any other conditions that might interfere with the analysis of the results.
- Previous bone grafting.
- History of irradiation therapy.
- Gum diseases.
- Bruxism/clenching.
- Inadequate oral hygiene.
- Lack of primary stability.
- Insufficient bone or any abnormality that would contraindicate implant placement.
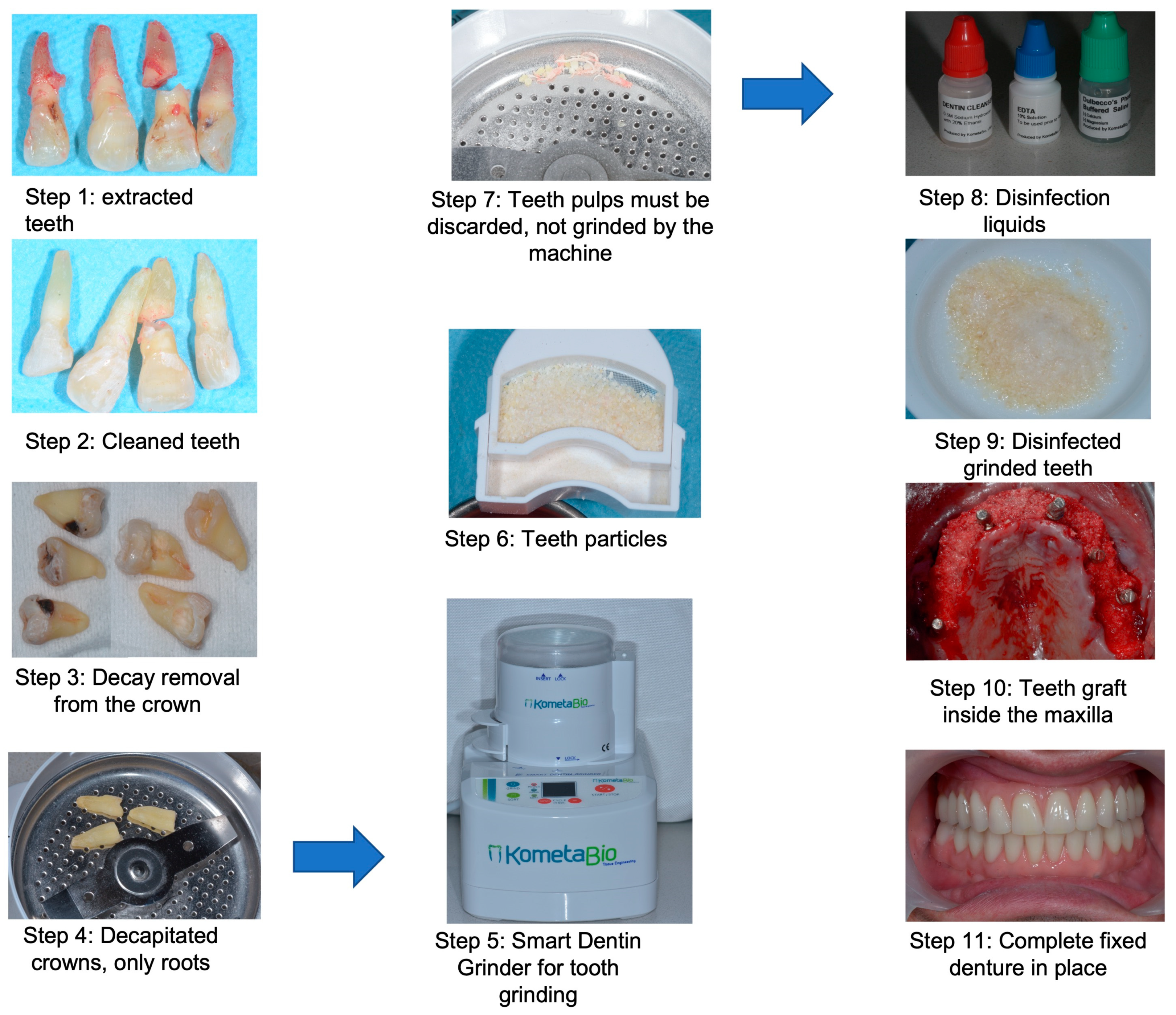
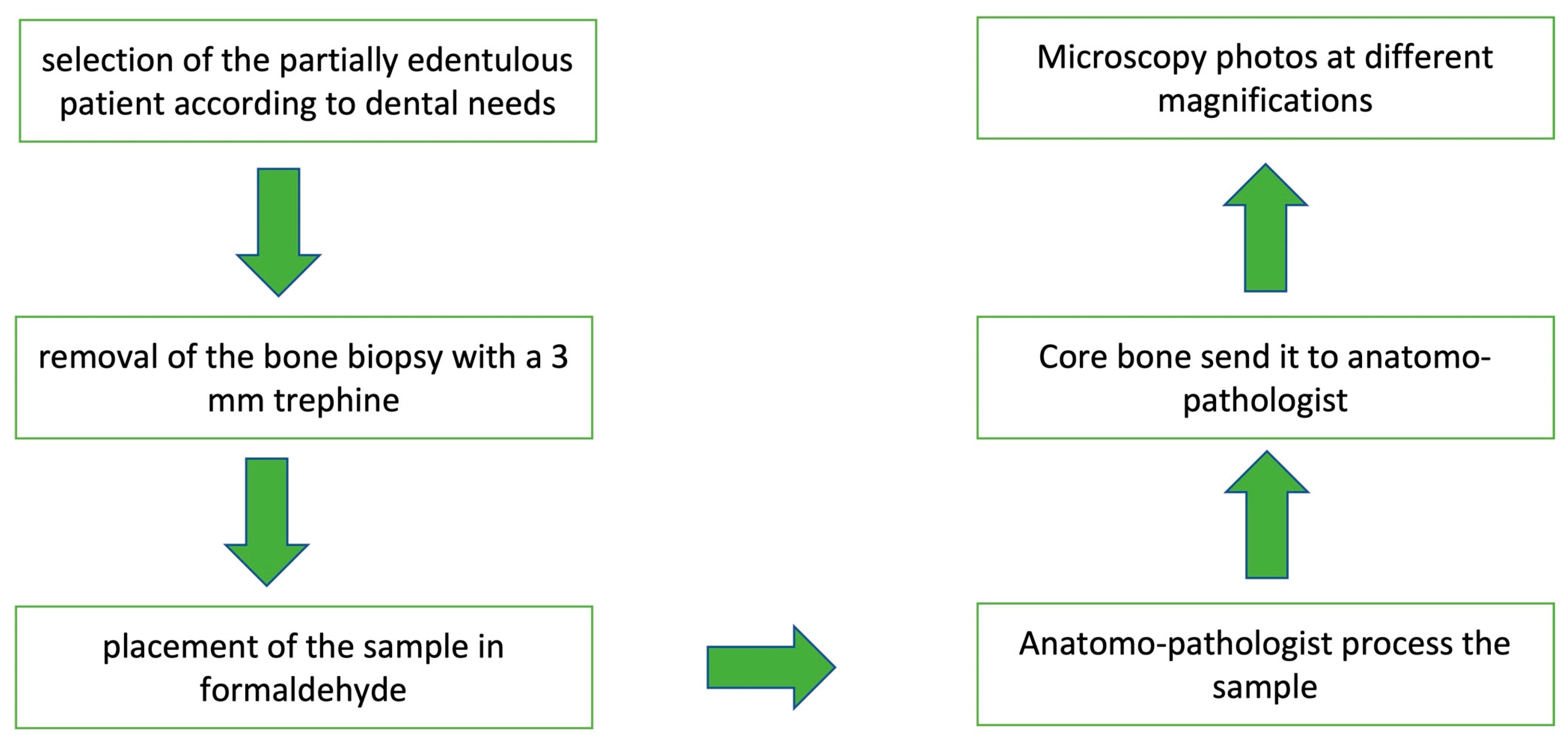
2.2. Histological Preparation
3. Results
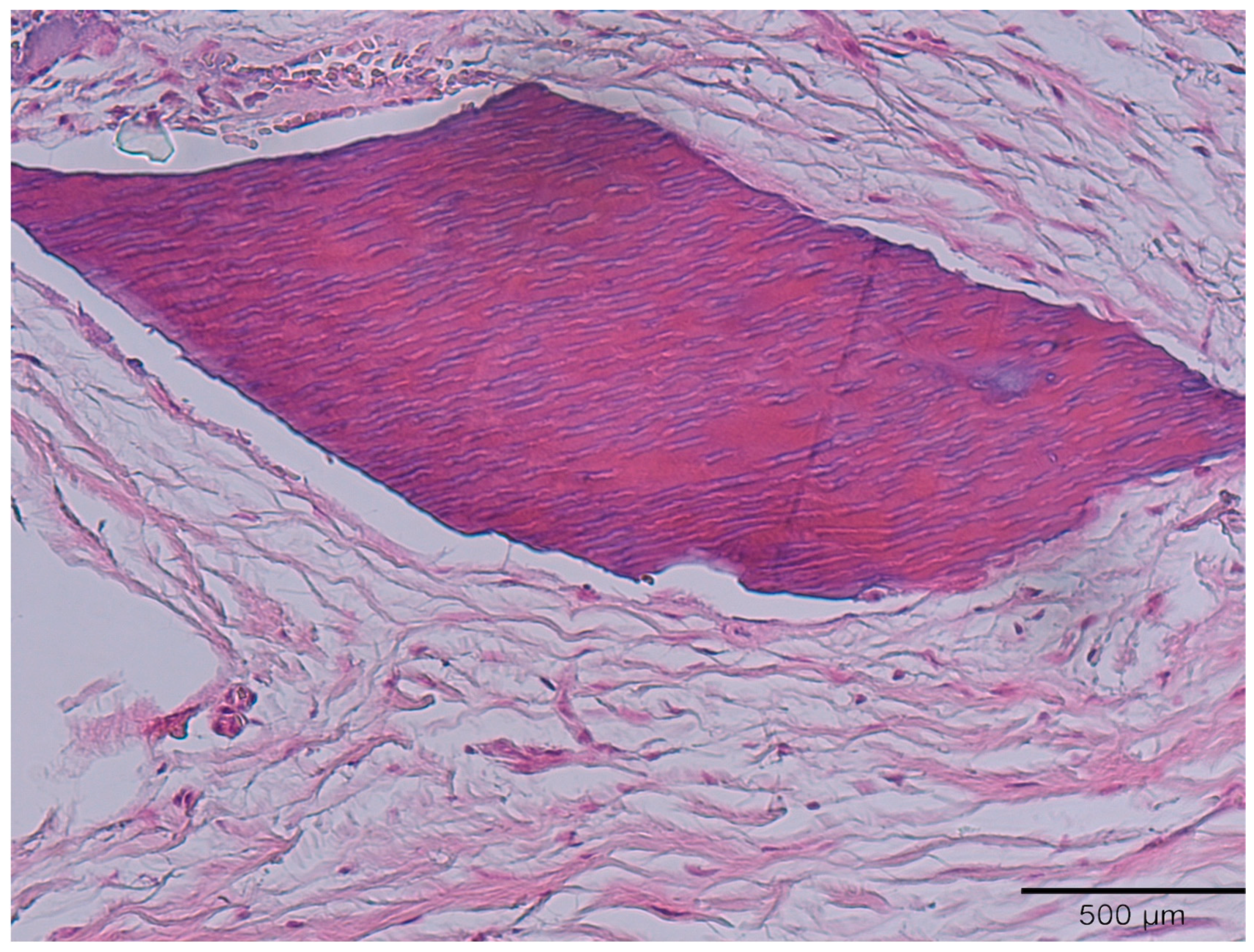
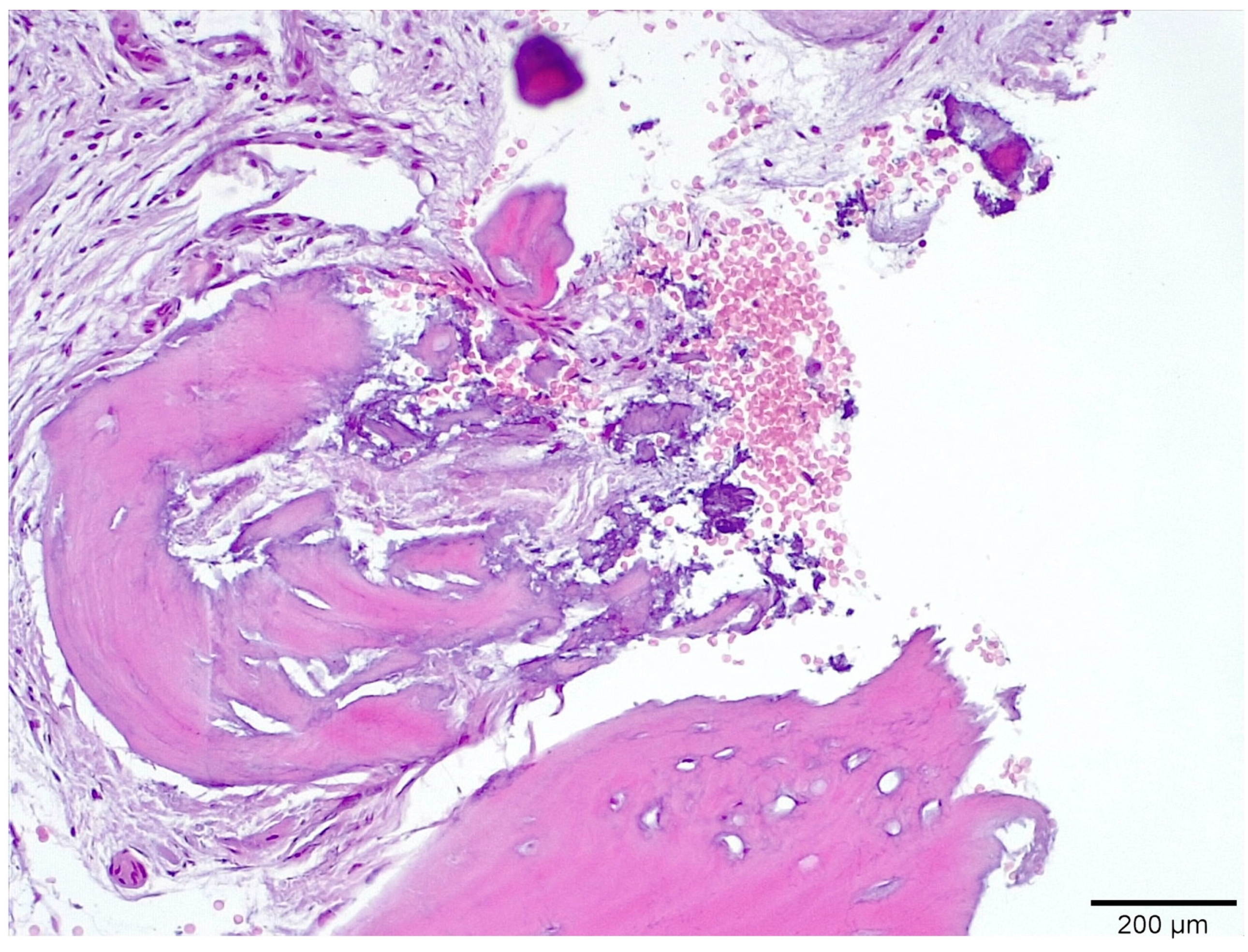
3.1. Histological Analysis Showed Signs of New Bone Formation at 60 Days
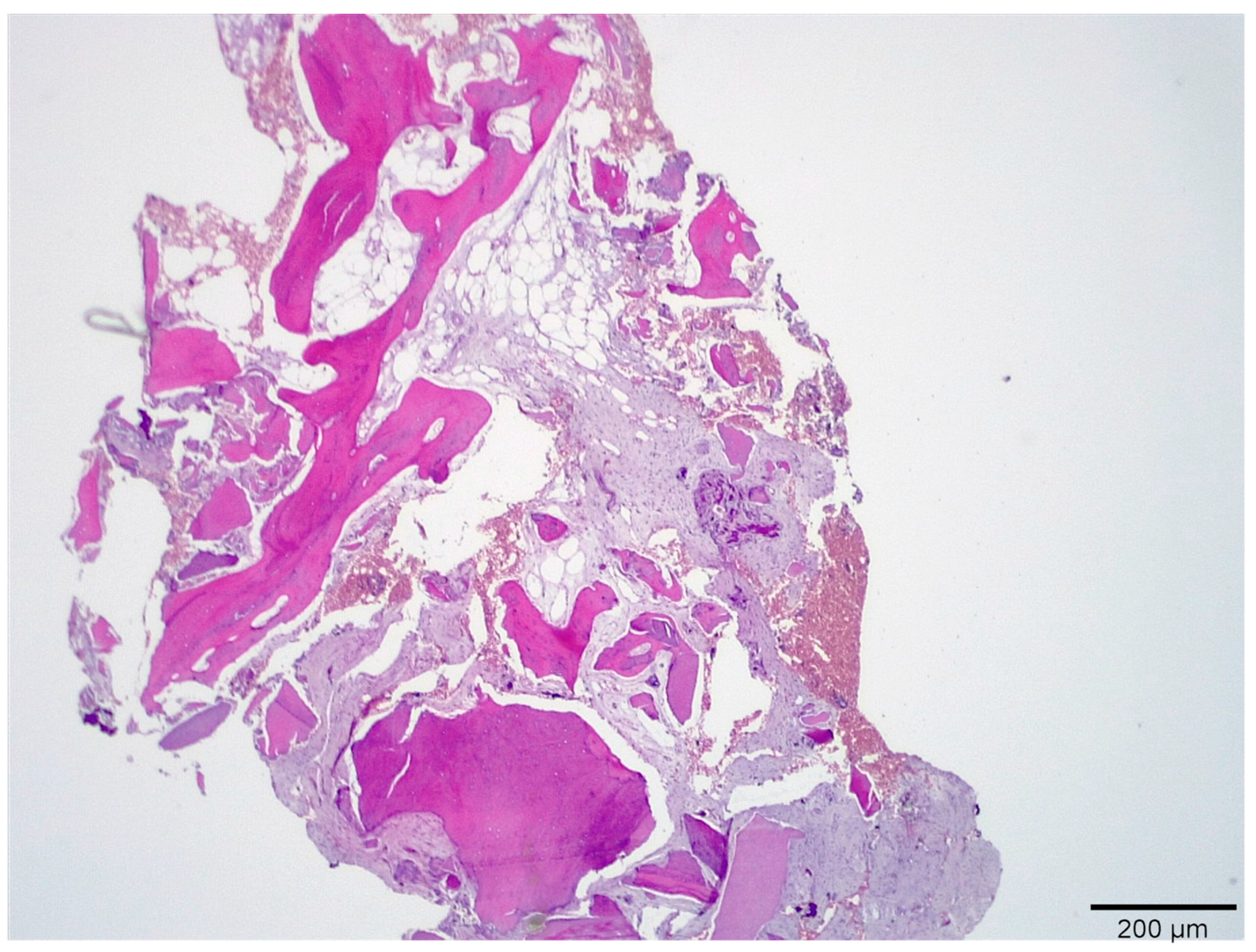
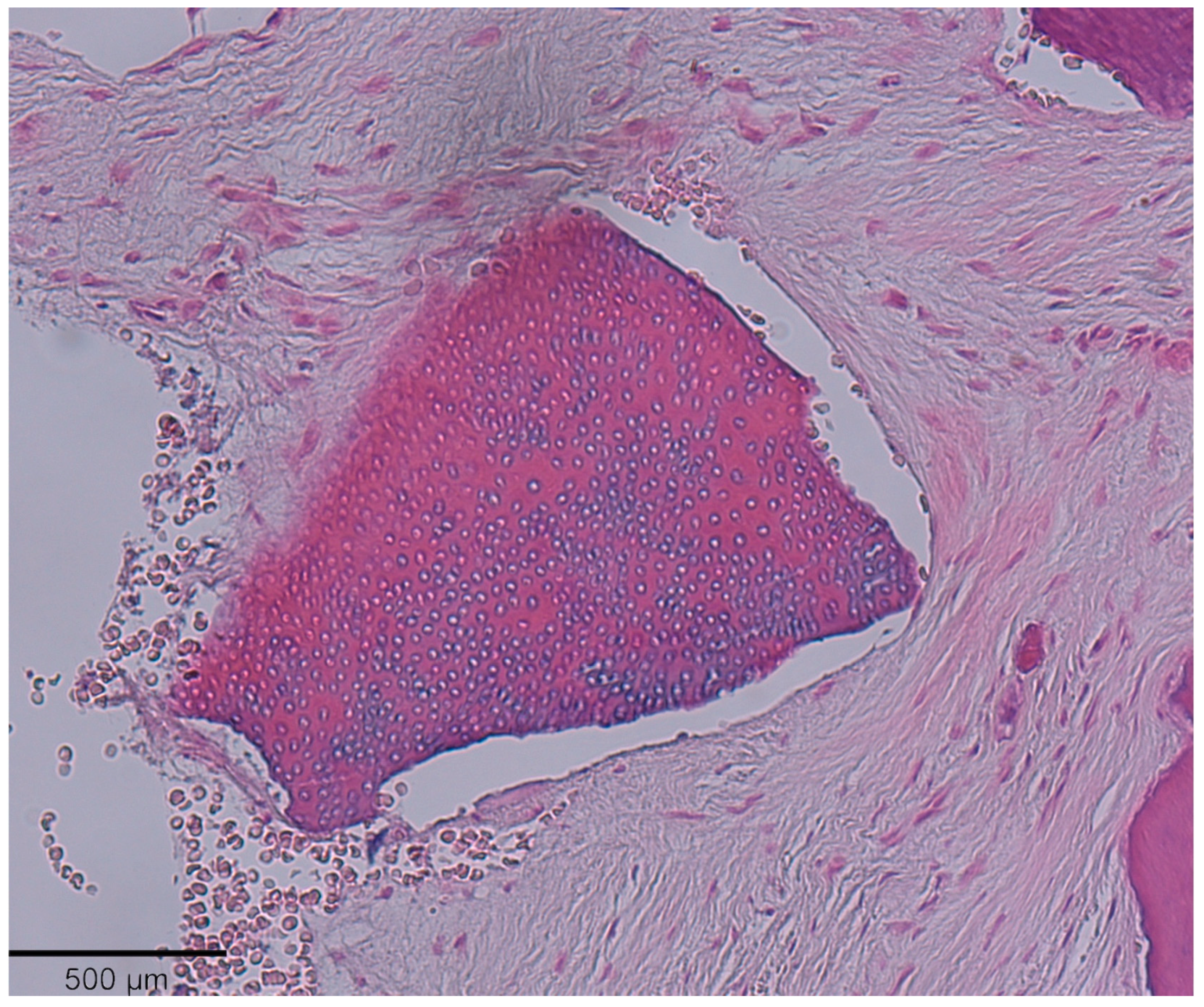
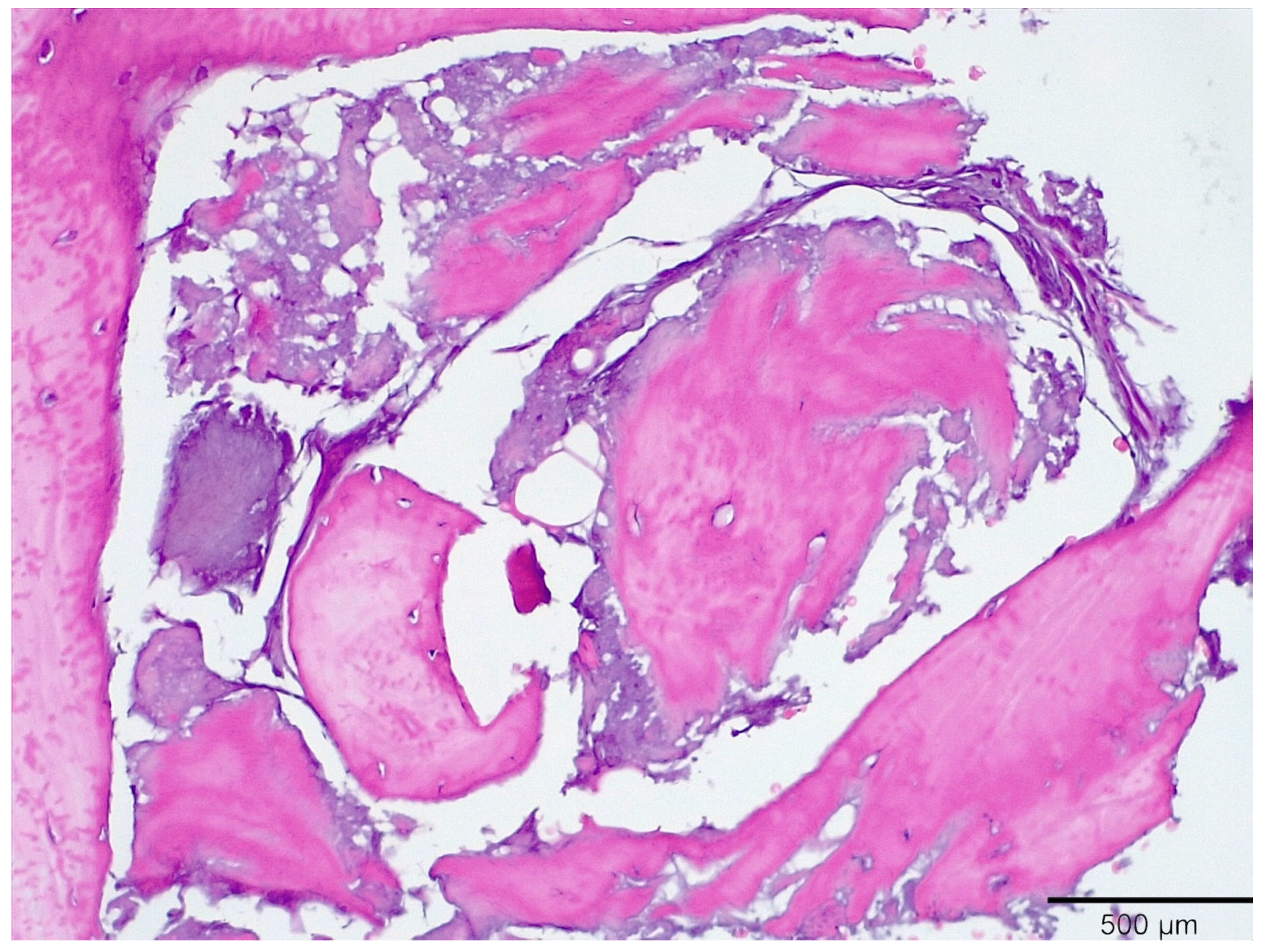
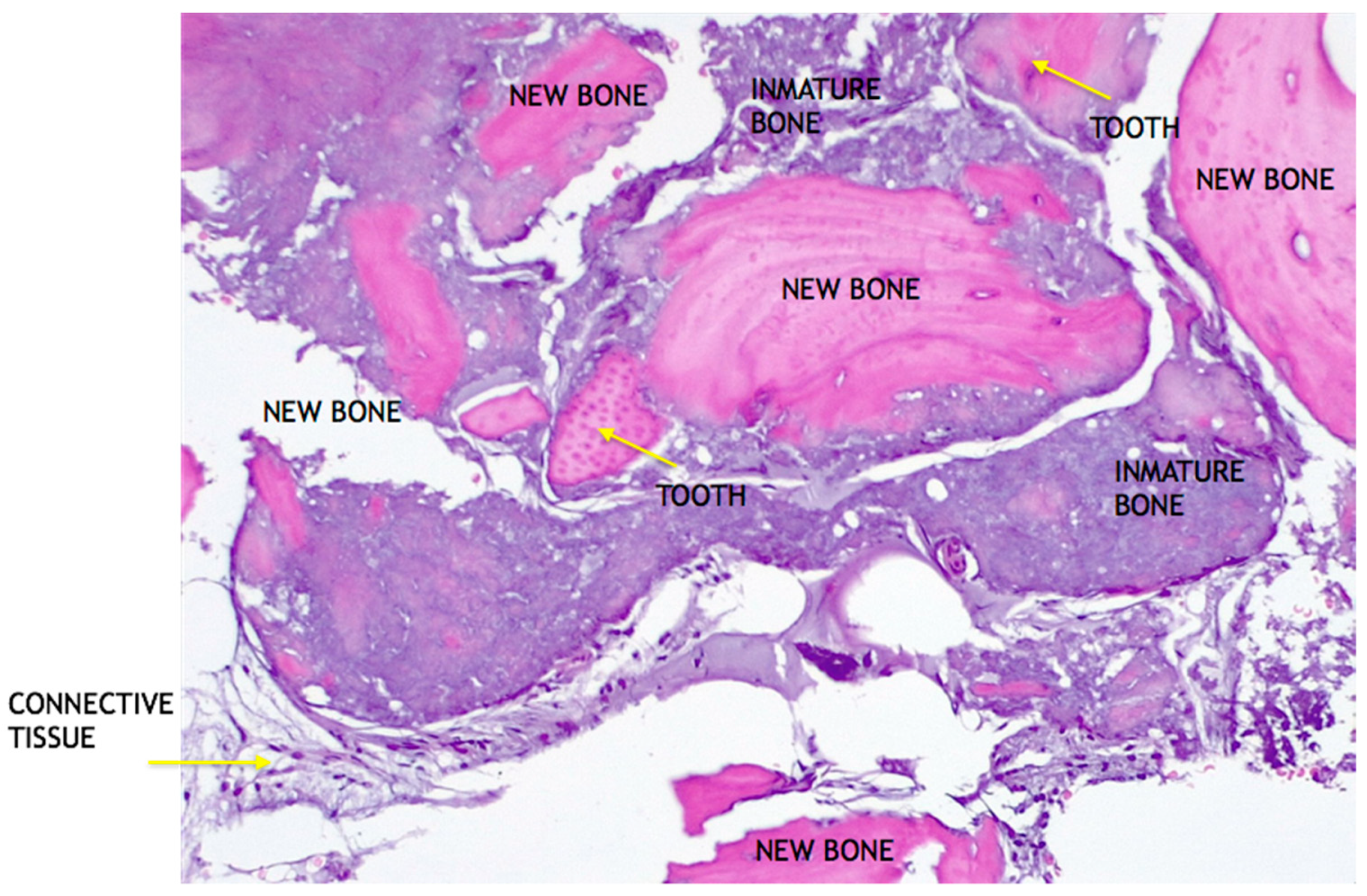
3.2. Histologic Data Obtained after Samples Analysis at 24 Months of Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bang, G.; Urist, M.R. Bone induction in excavation chambers in matrix of decalcified dentin. Arch. Surg. 1967, 94, 781–789. [Google Scholar] [CrossRef]
- Yeomans, J.D.; Urist, M.R. Bone induction by decalcified dentine implanted into oral, osseous and muscle tissues. Arch. Oral Biol. 1967, 12, 999–1008. [Google Scholar] [CrossRef]
- Huggins, C.B.; Urist, M.R. Dentin matrix transformation: Rapid induction of alkaline phosphatase and cartilage. Science 1970, 167, 896–898. [Google Scholar] [CrossRef] [PubMed]
- Bessho, K.; Tanaka, N.; Matsumoto, J.; Tagawa, T.; Murata, M. Human dentin-matrix-derived bone morphogenetic protein. J. Dent. Res. 1991, 70, 171–178. [Google Scholar] [CrossRef]
- Nampo, T.; Watahiki, J.; Enomoto, A.; Taguchi, T.; Ono, M.; Nakano, H.; Yamamoto, G.; Irie, T.; Tachikawa, T.; Maki, K. A new method for alveolar bone repair using extracted teeth for the graft material. J. Periodontol. 2010, 81, 1264–1272. [Google Scholar] [CrossRef]
- Ike, M.; Urist, M.R. Recycled dentin root matrix for a carrier of recombinant human bone morphogenetic protein. J. Oral Implantol. 1998, 24, 124–132. [Google Scholar] [CrossRef]
- Bakhshalian, N.; Hooshmand, S.; Campbell, S.C.; Kim, J.S.; Brummel-Smith, K.; Arjmandi, B.H. Biocompatibility and microstructural analysis of osteopromotive property of allogenic demineralized dentin matrix. Int. J. Oral Maxillofac. Implants 2013, 28, 1655–1662. [Google Scholar] [CrossRef]
- Kim, Y.-K.; Kim, S.-G.; Byeon, J.-H.; Lee, H.-J.; Um, I.-U.; Lim, S.-C.; Kim, S.-Y. Development of a novel bone grafting material using autogenous teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, 496–503. [Google Scholar] [CrossRef]
- Andersson, L. Dentin xenografts to experimental bone defects in rabbit tibia are ankylosed and undergo osseous replacement. Dent. Traumatol. 2010, 26, 398–402. [Google Scholar] [CrossRef]
- Gual-Vaqués, P.; Polis-Yanes, C.; Estrugo-Devesa, A.; Ayuso-Montero, R.; Mari-Roig, A.; Lopez-Lopez, J. Autogenous teeth used for bone grafting: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2018, 23, e112–e119. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L.; Ballester-Montilla, A.; De Aza, P.N.; Fernández-Domínguez, M.; Alexandre Gehrke, S.; Cegarra-Del Pino, P.; Mahesh, L.; Pelegrine, A.A.; Aragoneses, J.M.; Maté-Sánchez de Val, J. Particulated, Extracted Human Teeth Characterization by SEM–EDX Evaluation as a Biomaterial for Socket Preservation: An in vitro Study. Materials 2019, 12, 380. [Google Scholar] [CrossRef] [Green Version]
- Calvo-Guirado, J.L.; Cegarra Del Pino, P.; Sapoznikov, L.; Delgado Ruiz, R.A.; Fernández-Domínguez, M.; Gehrke, S.A. A new procedure for processing extracted teeth for immediate grafting in post-extraction sockets. An experimental study in American Fox Hound dogs. Ann. Anat. 2018, 217, 14–23. [Google Scholar] [CrossRef]
- Ramírez Fernández, M.P.; Gehrke, S.A.; Pérez Albacete Martinez, C.; Calvo Guirado, J.L.; de Aza, P.N. SEM-EDX Study of the Degradation Process of Two xenograft Materials Used in Sinus Lift Procedures. Materials 2017, 10, 542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esposito, M.; Grusovin, M.G.; Kwan, S.; Worthington, H.V.; Coulthard, P. Interventions for replacing missing teeth: Bone augmentation techniques for dental implant treatment. Cochrane Database Syst. Rev. 2008, 3, CD003607. [Google Scholar]
- Kim, Y.K.; Kim, S.G.; Yun, P.Y.; Yeo, I.S.; Jin, S.C.; Oh, J.S.; Kim, H.-J.; Yu, S.-K.; Lee, S.-Y.; Kim, J.-S.; et al. Autogenous teeth used for bone grafting: A comparison with traditional grafting materials. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, e39–e45. [Google Scholar] [CrossRef]
- Kim, Y.K.; Lee, J.; Kim, K.W.; Um, I.W.; Murata, M.; Ito, K. Analysis of Organic Components and Osteoinductivity in Autogenous Tooth Bone Graft Material. J. Korean Assoc. Maxillofac. Plast. Reconstr. Surg. 2013, 35, 353–359. [Google Scholar] [CrossRef] [Green Version]
- Horowitz, R.; Holtzclaw, D.; Rosen, P.S. A review on alveolar ridge preservation following tooth extraction. J. Evid. Based Dent. Pract. 2012, 12, 149–160. [Google Scholar] [CrossRef]
- Akazawa, T.; Murata, M.; Hino, J.; Nakamura, K.; Tazaki, J.; Kikuchi, M.; Arisue, M. Materials design and application of demineralized dentin/apatite composite granules derived from human teeth. Arch. Bioceram. Res. 2007, 7, 25–28. [Google Scholar]
- Kim, S.G.; Kim, H.K.; Lim, S.C. Combined implantation of particulate dentin, plaster of Paris, and a bone xenograft (Bio-Oss) for bone regeneration in rats. J. Craniomaxillofac. Surg. 2001, 29, 282–288. [Google Scholar]
- Kim, S.Y.; Kim, S.G.; Lim, S.C.; Bae, C.S. Effects on bone formation in ovariectomized rats after implantation of tooth ash and plaster of Paris mixture. J. Oral Maxillofac. Surg. 2004, 62, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Lindhe, J.; Cecchinato, D.; Donati, M.; Tomasi, C.; Liljenberg, B. Ridge preservation with the use of deproteinized bovine bone mineral. Clin. Oral Implants Res. 2013, 25, 786–790. [Google Scholar] [CrossRef]
- Sperling, I.; Itzkowitz, D.; Kaufman, A.; Binderman, I. A new treatment of heterotransplanted teeth to prevent progression of root resorption. Dent. Traumatol. 1986, 2, 117–120. [Google Scholar] [CrossRef]
- Andersson, L.; Bodin, I.; Sörensen, S. Progression of root resorption following replantation of human teeth after extended extraoral storage. Dent. Traumatol. 1989, 5, 38–47. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L. Temporary implants and particulate dentin graft protecting traditional implants in severe periodontal patient: A case report. Indian J. Dent. Sci. 2021, 13, 201–204. [Google Scholar]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 3 | 6 | 12 | 24 | |
|---|---|---|---|---|
| New bone | 16.3 ± 1.98 | 41.1 ± 0.76 | 54.5 ± 0.24 | 59.4 ± 1.23 * |
| Residual Graft | 37.1 ± 0.34 | 30.0 ± 0.45 | 21.3 ± 0.88 | 15.6 ± 086 |
| Connective tissue | 46.6 ± 0.11 | 29.9 ± 0.56 | 24.2 ± 0.32 | 25.0 ± 0.44 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cervera-Maillo, J.M.; Morales-Schwarz, D.; Morales-Melendez, H.; Mahesh, L.; Calvo-Guirado, J.L. Autologous Tooth Dentin Graft: A Retrospective Study in Humans. Medicina 2022, 58, 56. https://doi.org/10.3390/medicina58010056
Cervera-Maillo JM, Morales-Schwarz D, Morales-Melendez H, Mahesh L, Calvo-Guirado JL. Autologous Tooth Dentin Graft: A Retrospective Study in Humans. Medicina. 2022; 58(1):56. https://doi.org/10.3390/medicina58010056
Chicago/Turabian StyleCervera-Maillo, José Manuel, David Morales-Schwarz, Hilde Morales-Melendez, Lanka Mahesh, and José Luis Calvo-Guirado. 2022. "Autologous Tooth Dentin Graft: A Retrospective Study in Humans" Medicina 58, no. 1: 56. https://doi.org/10.3390/medicina58010056