
Effects of Acupuncture on Cardiac Remodeling in Patients with Persistent Atrial Fibrillation: Results of a Randomized, Placebo-Controlled, Patient- and Assessor-Blinded Pilot Trial and Its Implications for Future Research

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Randomization and Blinding
2.3. Participants
2.4. EC Protocol
2.5. Outcomes
2.5.1. Primary Outcome
2.5.2. Secondary Outcome
2.6. Intervention
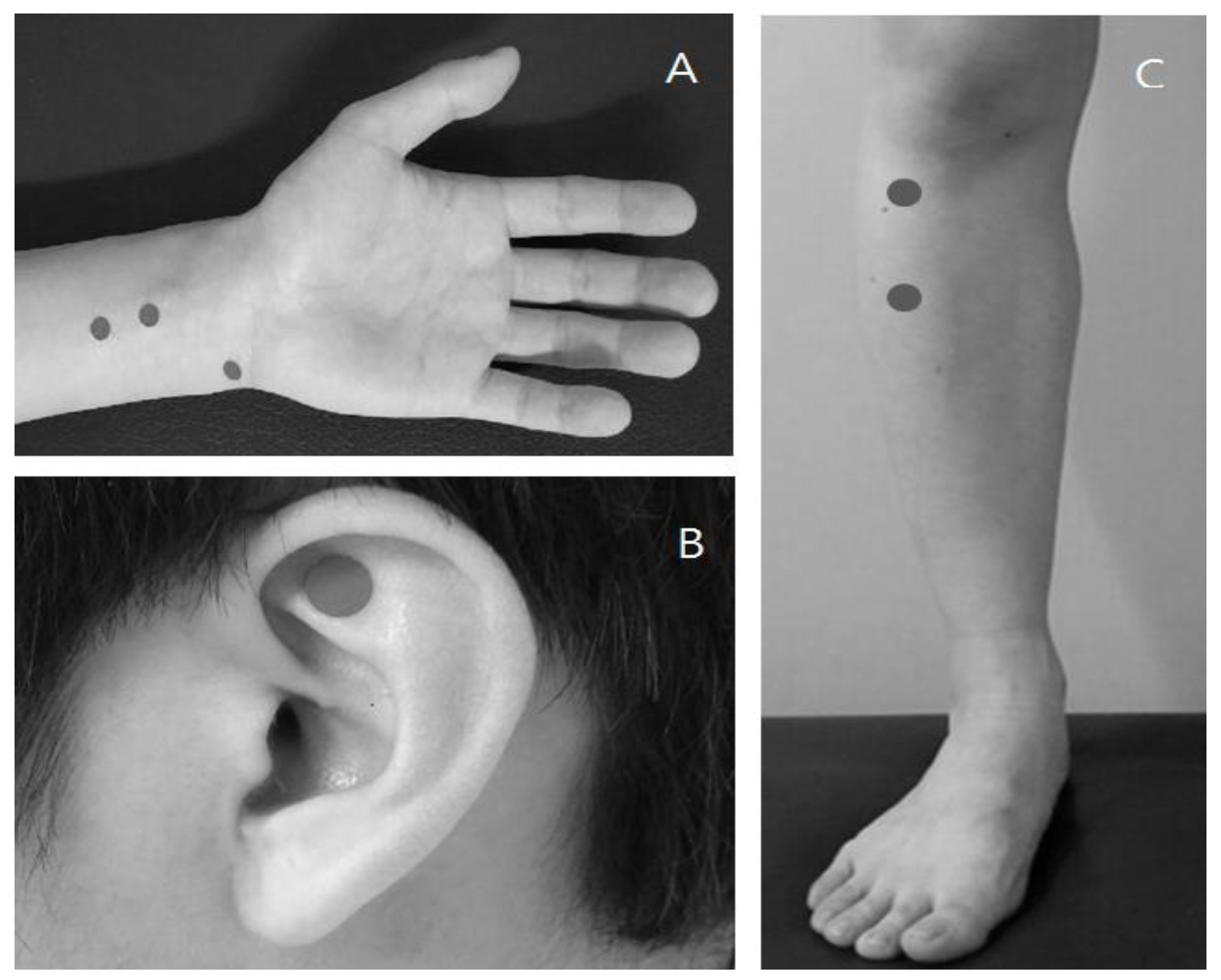
2.6.1. Real Acupuncture Treatment
2.6.2. Sham Acupuncture Treatment
2.7. Sample Size
2.8. Statistical Analysis
2.9. Ethical Considerations
3. Results
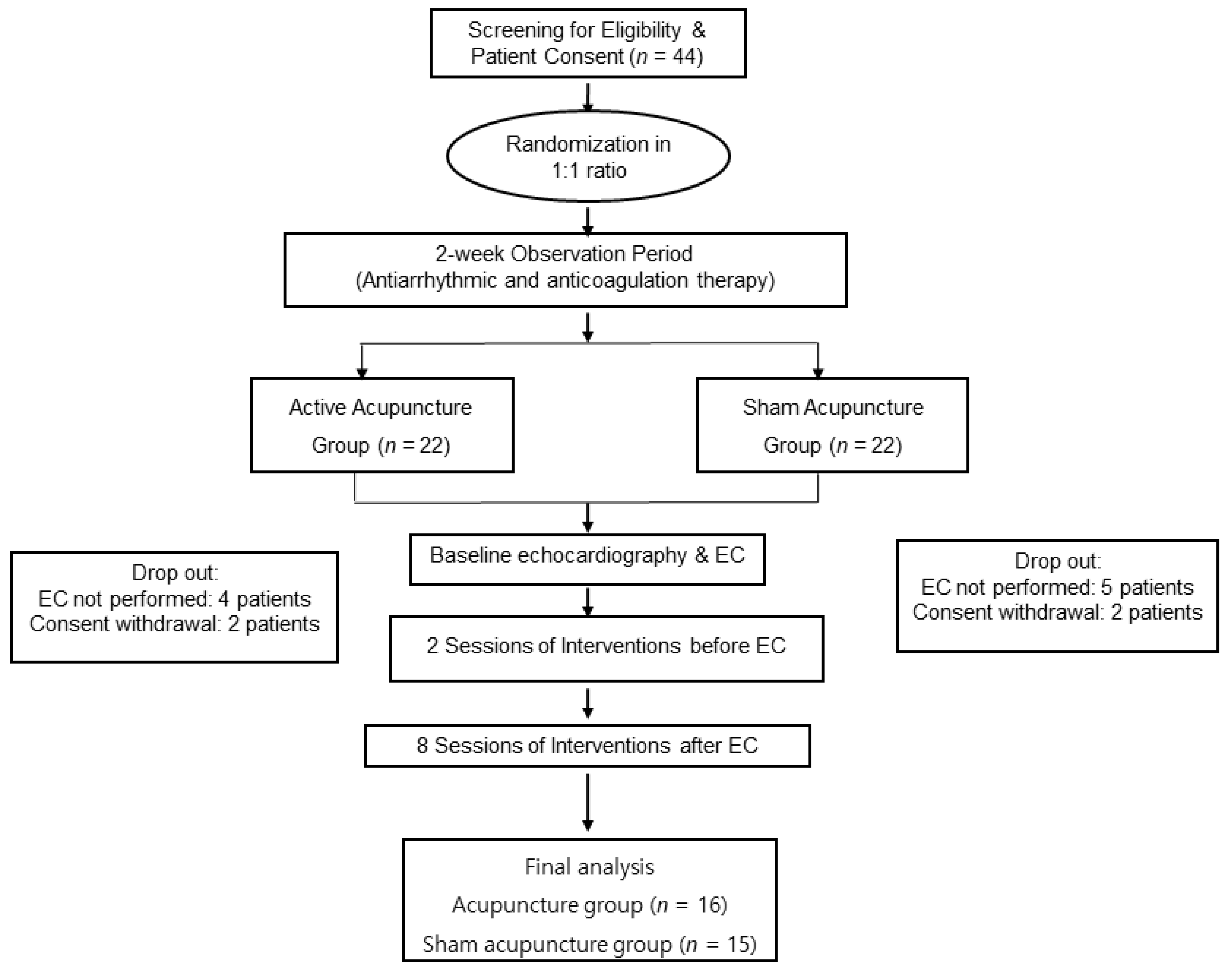
3.1. Participant Flow and Recruitment
3.2. Baseline Characteristics
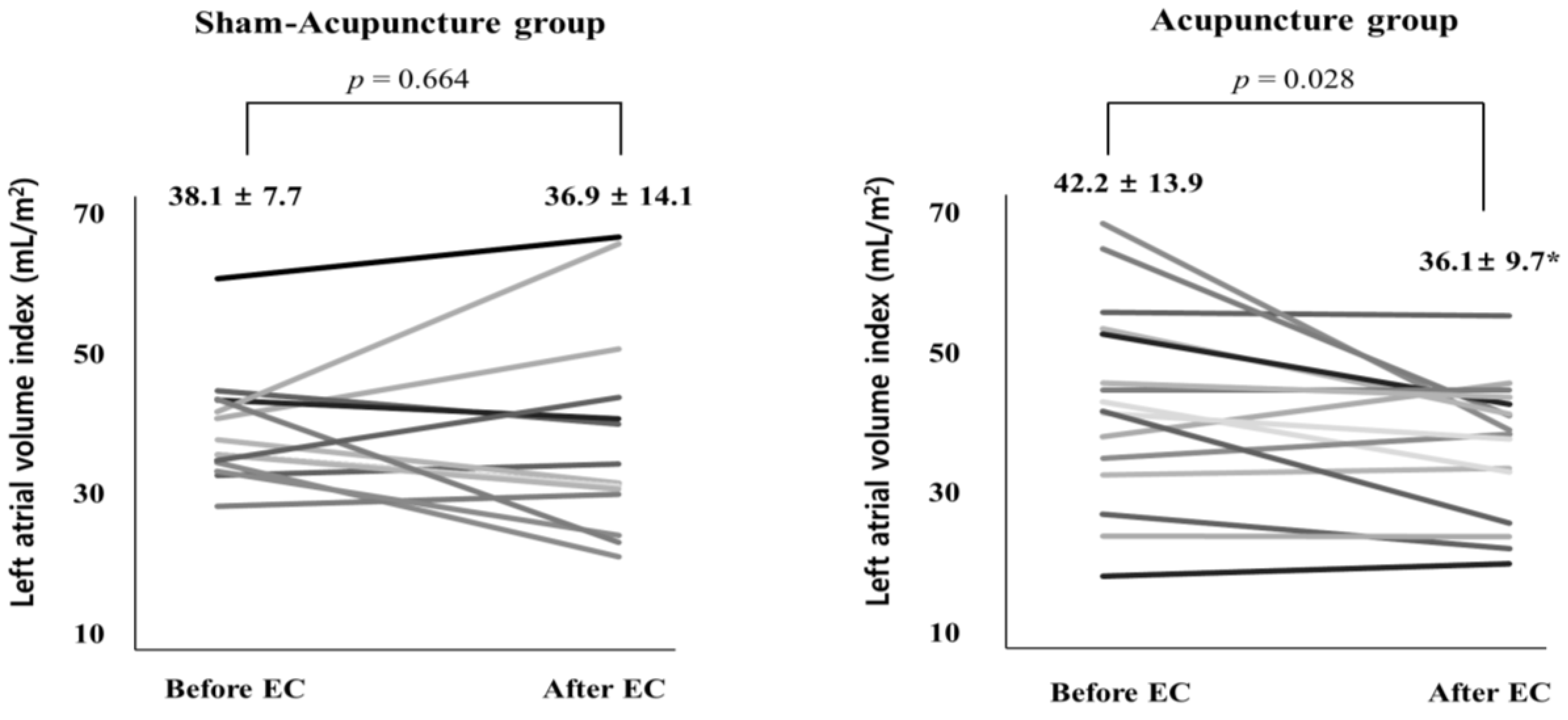
3.3. Primary Outcome
3.4. Secondary Outcomes
4. Discussion
4.1. Summary of Findings
4.2. Discussion
4.3. Strengths and Limitations
4.4. Implications for Future Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.-C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, H.; Cigarroa, J.E.; Cleveland, J.C.; Conti, J.B.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2014, 64, e1–e76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verma, A.; Jiang, C.Y.; Betts, T.R.; Chen, J.; Deisenhofer, I.; Mantovan, R.; Macle, L.; Morillo, C.A.; Haverkamp, W.; Weerasooriya, R.; et al. Approaches to catheter ablation for persistent atrial fibrillation. N. Engl. J. Med. 2015, 372, 1812–1822. [Google Scholar] [CrossRef] [PubMed]
- Calkins, H.; Hindricks, G.; Cappato, R.; Kim, Y.-H.; Saad, E.B.; Aguinaga, L.; Akar, J.G.; Badhwar, V.; Brugada, J.; Camm, J.; et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm 2017, 14, e275–e444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lombardi, F.; Belletti, S.; Battezzati, P.M.; Lomuscio, A. Acupuncture for paroxysmal and persistent atrial fibrillation: An effective non-pharmacological tool? World J. Cardiol. 2012, 4, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Painovich, J.; Longhurst, J. Integrating acupuncture into the cardiology clinic: Can it play a role? Acta Physiol. Sin. 2015, 67, 19–31. [Google Scholar]
- VanWormer, A.M.; Lindquist, R.; Sendelbach, S.E. The effects of acupuncture on cardiac arrhythmias: A literature review. Heart Lung J. Crit. Care 2008, 37, 425–431. [Google Scholar] [CrossRef]
- Yin, J.; Yang, M.; Yu, S.; Fu, H.; Huang, H.; Yang, B.; Liu, Y.; He, B.; Bao, M.; Wu, G.; et al. Effect of acupuncture at Neiguan point combined with amiodarone therapy on early recurrence after pulmonary vein electrical isolation in patients with persistent atrial fibrillation. J. Cardiovasc. Electrophysiol. 2019, 30, 910–917. [Google Scholar] [CrossRef]
- Stavrakis, S.; Humphrey, M.B.; Scherlag, B.J.; Hu, Y.; Jackman, W.M.; Nakagawa, H.; Lockwood, D.; Lazzara, R.; Po, S.S. Low-level transcutaneous electrical vagus nerve stimulation suppresses atrial fibrillation. J. Am. Coll. Cardiol. 2015, 65, 867–875. [Google Scholar] [CrossRef] [Green Version]
- Lomuscio, A.; Belletti, S.; Battezzati, P.M.; Lombardi, F. Efficacy of acupuncture in preventing atrial fibrillation recurrences after electrical cardioversion. J. Cardiovasc. Electrophysiol. 2011, 22, 241–247. [Google Scholar] [CrossRef]
- Park, J.; Kim, H.S.; Lee, S.M.; Yoon, K.; Kim, W.-S.; Woo, J.S.; Lee, S.; Kim Ji Kim, W. Acupuncture antiarrhythmic effects on drug refractory persistent atrial fibrillation: Study protocol for a randomized, controlled trial. Evid. Based Complementary Altern. Med. Ecam. 2015, 2015, 613970. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Standard Acupuncture Point Locations in the Western Pacific Region; World Health Organization: Manila, Philippines, 2008. [Google Scholar]
- Liu, J.; Li, S.N.; Liu, L.; Zhou, K.; Li, Y.; Cui, X.-Y.; Wan, J.; Lu, J.-J.; Huang, Y.-C.; Wang, X.S.; et al. Conventional Acupuncture for Cardiac Arrhythmia: A Systematic Review of Randomized Controlled Trials. Chin. J. Integr. Med. 2018, 24, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Fei, Y.; Fei, R.; Zhang, J.; Sun, Y.; Yu, Q. Systematic Evaluation of Efficacy and Safety of Acupuncture Treatment for Patients with Atrial Fibrillation. Open Access Maced. J. Med. Sci. 2019, 7, 461–466. [Google Scholar] [CrossRef] [Green Version]
- Nattel, S.; Harada, M. Atrial Remodeling and Atrial Fibrillation: Recent Advances and Translational Perspectives. J. Am. Coll. Cardiol. 2014, 63, 2335–2345. [Google Scholar] [CrossRef] [Green Version]
- Vaziri, S.M.; Larson, M.G.; Benjamin, E.J.; Levy, D. Echocardiographic predictors of nonrheumatic atrial fibrillation. Fram. Heart Study Circ. 1994, 89, 724–730. [Google Scholar] [CrossRef] [Green Version]
- Toufan, M.; Kazemi, B.; Molazadeh, N. The significance of the left atrial volume index in prediction of atrial fibrillation recurrence after electrical cardioversion. J. Cardiovasc. Thorac. Res. 2017, 9, 54–59. [Google Scholar] [CrossRef] [Green Version]
- Njoku, A.; Kannabhiran, M.; Arora, R.; Reddy, P.; Gopinathannair, R.; Lakkireddy, D.; Dominic, P. Left atrial volume predicts atrial fibrillation recurrence after radiofrequency ablation: A meta-analysis. Europace 2018, 20, 33–42. [Google Scholar] [CrossRef]
- Kokubu, N.; Yuda, S.; Tsuchihashi, K.; Hashimoto, A.; Nakata, T.; Miura, T.; Ura, N.; Nagao, K.; Tsuzuki, M.; Wakabayashi, C.; et al. Noninvasive assessment of left atrial function by strain rate imaging in patients with hypertension: A possible beneficial effect of renin-angiotensin system inhibition on left atrial function. Hypertens. Res. 2007, 30, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Matsuyama, N.; Tsutsumi, T.; Kubota, N.; Nakajima, T.; Suzuki, H.; Takeyama, Y. Direct action of an angiotensin II receptor blocker on angiotensin II-induced left atrial conduction delay in spontaneously hypertensive rats. Hypertens. Res. 2009, 32, 721–726. [Google Scholar] [CrossRef] [Green Version]
- Thomas, L.; Abhayaratna, W.P. Left Atrial Reverse Remodeling, Mechanisms, Evaluation, and Clinical Significance. JACC Cardiovasc. Imaging 2017, 10, 65–77. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Leem, J.; Park, J.H.; Yoon, K.H.; Woo, J.S.; Lee, J.M.; Kim, J.-B.; Kim, W.; Lee, S. Close look at the experiences of patients enrolled in a clinical trial of acupuncture treatment for atrial fibrillation in Korea: A qualitative study nested within a randomised controlled trial. BMJ Open 2017, 7, e013180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chae, Y.; Lee, Y.S.; Enck, P. How Placebo Needles Differ from Placebo Pills? Front. Psychiatry 2018, 9, 243. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.; Jung, W.-S.; Yang, S.; Jin, C.; Cho, S.-Y.; Park, S.-U.; Moon, S.-K.; Park, J.-M.; Ko, C.-N.; Cho, K.-H.; et al. Safety of Acupuncture in Patients Taking Newer Oral Anticoagulants: A Retrospective Chart Review Study. Evid. -Based Complementary Altern. Med. Ecam 2018, 2018, 8042198. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kim, M.-S.; You, S.-H.; Jung, S.-Y. Conducting and Reporting a Clinical Research Using Korean Healthcare Claims Database. Korean J. Fam. Med. 2020, 41, 146–152. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sham Acupuncture (N = 15) | Acupuncture (N = 16) | p-Value | |
|---|---|---|---|
| Age (years) | 63.7 ± 6.5 | 69.6 ± 7.3 | 0.024 |
| Male, n (%) | 12 (80.0%) | 13 (81.2%) | 1 |
| Hypertension, n (%) | 10 (66.7%) | 14 (87.5%) | 0.339 |
| Diabetes Mellitus, n (%) | 3 (20.0%) | 2 (12.5%) | 0.937 |
| Stroke, n (%) | 0 (0.0%) | 3 (18.8%) | 0.247 |
| Vascular disease, n (%) | 0 (0.0%) | 1 (6.2%) | 1 |
| CHA2DS2VASC score | 1.6 ± 1.0 | 2.8 ± 1.5 | 0.02 |
| BSA (kg/m2) | 1.8 ± 0.2 | 1.8 ± 0.2 | 0.961 |
| TTE parameters | |||
| LVEF (%) | 64.2 ± 5.3 | 61.0 ± 6.8 | 0.151 |
| LAVI (mL/m2) | 38.1 ± 7.7 | 42.2 ± 13.9 | 0.31 |
| E/E’ * | 11.5 [9.6–11.9] | 12.6 [10.4–14.7] | 0.455 |
| Medications | |||
| Beta blocker | 1 (6.7%) | 1 (6.2%) | 1.0 |
| Calcium channel blocker | 3 (20%) | 5 (31.2%) | 0.685 |
| ACEi | 0 | 2 (12.5%) | 0.484 |
| ARB | 5 (33.3%) | 8 (50%) | 0.347 |
| ACEi or ARB | 5 (33.3%) | 10 (66.6%) | 0.104 |
| Loop diuretics | 2 (13.3%) | 1 (6.2%) | 0.6 |
| Thiazide | 1 (6.7%) | 0 | 0.484 |
| Spironolactone | 2 (13.3%) | 2 (12.5%) | 1.0 |
| Any diuretics | 3 (20%) | 2 (12.5%) | 0.654 |
| Nitrate | 1 (6.7%) | 1 (6.2%) | 1.0 |
| Digitalis | 1 (6.7%) | 0 | 0.484 |
| Anticoagulant | 0.461 | ||
| Warfarin | 11 (73.3%) | 13 (81.2%) | |
| DOACs | 4 (26.7%) | 3 (18.8%) | |
| (Apixaban) | 0 | 1 (6.2%) | |
| (Dabigatran) | 3 (20%) | 1 (6.2%) | |
| (Edoxaban) | 1 (6.7%) | 0 | |
| (Rivaroxaban) | 0 | 1 (6.2%) |
| Sham Acupuncture (N = 15) | Acupuncture (N = 16) | p-Value | |
|---|---|---|---|
| Rhythm outcomes | 0.611 | ||
| AF recurrence | 9 (60.0%) | 12 (75.0%) | |
| Sinus rhythm | 6 (40.0%) | 4 (25.0%) | |
| TTE parameters | |||
| LVEF | 63.8 ± 4.6 | 63.6 ± 5.2 | 0.903 |
| LAVI | 36.9 ± 14.1 | 36.1 ± 9.7 | 0.865 |
| E/E’ | 11.9 ± 4.5 | 11.9 ± 3.9 | 0.984 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.M.; Lee, S.M.K.; Leem, J.; Kim, J.-B.; Park, J.; Park, J.H.; Lee, S.; Kim, H.O.; Chung, H.; Woo, J.S.; et al. Effects of Acupuncture on Cardiac Remodeling in Patients with Persistent Atrial Fibrillation: Results of a Randomized, Placebo-Controlled, Patient- and Assessor-Blinded Pilot Trial and Its Implications for Future Research. Medicina 2022, 58, 41. https://doi.org/10.3390/medicina58010041
Lee JM, Lee SMK, Leem J, Kim J-B, Park J, Park JH, Lee S, Kim HO, Chung H, Woo JS, et al. Effects of Acupuncture on Cardiac Remodeling in Patients with Persistent Atrial Fibrillation: Results of a Randomized, Placebo-Controlled, Patient- and Assessor-Blinded Pilot Trial and Its Implications for Future Research. Medicina. 2022; 58(1):41. https://doi.org/10.3390/medicina58010041
Chicago/Turabian StyleLee, Jung Myung, Seung Min Kathy Lee, Jungtae Leem, Jin-Bae Kim, Jimin Park, Jun Hyeong Park, Suji Lee, Hyung Oh Kim, Hyemoon Chung, Jong Shin Woo, and et al. 2022. "Effects of Acupuncture on Cardiac Remodeling in Patients with Persistent Atrial Fibrillation: Results of a Randomized, Placebo-Controlled, Patient- and Assessor-Blinded Pilot Trial and Its Implications for Future Research" Medicina 58, no. 1: 41. https://doi.org/10.3390/medicina58010041