
Immediate Effects of Diaphragmatic Breathing with Cervical Spine Mobilization on the Pulmonary Function and Craniovertebral Angle in Patients with Chronic Stroke


Abstract
:1. Introduction
2. Methods
2.1. Design
2.2. Sample Size Calculation
2.3. Participants and Recruitment
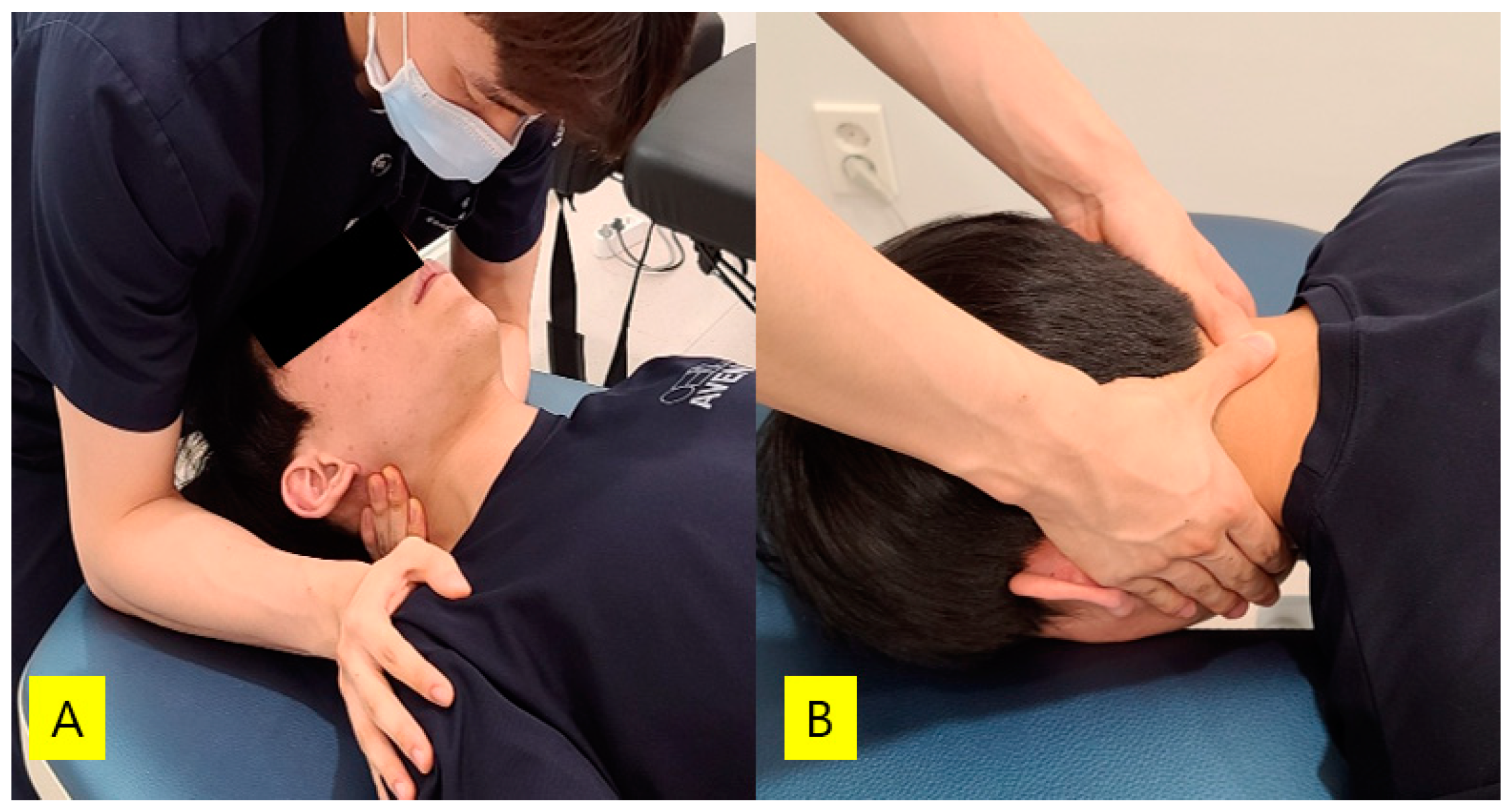
2.4. Intervention
Diaphragmatic Breathing with Joint Mobilization
2.5. Assessments
2.5.1. Pulmonary Function
2.5.2. Craniovertebral Angle
2.6. Statistical Analyses
3. Results
3.1. General Characteristics of Subjects
3.2. Changes in Pulmonary Function, Craniovertebral Angle
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Menezes, K.K.; Nascimento, L.; Ada, L.; Polese, J.C.; Avelino, P.R.; Teixeira-Salmela, L.F. Respiratory muscle training increases respiratory muscle strength and reduces respiratory complications after stroke: A systematic review. J. Physiother. 2016, 62, 138–144. [Google Scholar] [CrossRef] [Green Version]
- Teixeira-Salmela, L.F.; Parreira, V.F.; Britto, R.R.; Brant, T.C.; Inácio, P.; Alcântara, T.O.; Carvalho, I.F. Respiratory Pressures and Thoracoabdominal Motion in Community-Dwelling Chronic Stroke Survivors. Arch. Phys. Med. Rehabil. 2005, 86, 1974–1978. [Google Scholar] [CrossRef]
- Jung, J.-H.; Kim, N.-S. The correlation between diaphragm thickness, diaphragmatic excursion, and pulmonary function in patients with chronic stroke. J. Phys. Ther. Sci. 2017, 29, 2176–2179. [Google Scholar] [CrossRef] [Green Version]
- Lanini, B.; Bianchi, R.; Romagnoli, I.; Coli, C.; Binazzi, B.; Gigliotti, F.; Pizzi, A.; Grippo, A.; Scano, G. Chest Wall Kinematics in Patients with Hemiplegia. Am. J. Respir. Crit. Care Med. 2003, 168, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Lanini, B.; Gigliotti, F.; Coli, C.; Bianchi, R.; Pizzi, A.; Romagnoli, I.; Grazzini, M.; Stendardi, L.; Scano, G.J.C.S. Dissociation between respiratory effort and dyspnoea in a subset of patients with stroke. Clin. Sci. 2002, 103, 467–473. [Google Scholar] [CrossRef]
- Rochester, C.L.; Mohsenin, V. Respiratory Complications of Stroke. Semin. Respir. Crit. Care Med. 2002, 23, 248–260. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, M.B.; Polese, J.C.; Faria, C.; Machado, G.; Parreira, V.F.; Britto, R.R.; Teixeira-Salmela, L.F. Inspiratory muscular weakness is most evident in chronic stroke survivors with lower walking speeds. Eur. J. Phys. Rehabil. Med. 2014, 50, 301–307. [Google Scholar]
- Zhang, X.; Zheng, Y.; Dang, Y.; Wang, L.; Cheng, Y.; Zhang, X.; Mao, M.; Lu, X. Can inspiratory muscle training benefit patients after stroke? A systematic review and meta-analysis of randomized controlled trials. Clin. Rehabil. 2020, 34, 866–876. [Google Scholar] [CrossRef]
- Britto, R.R.; Rezende, N.R.; Marinho, K.C.; Torres, J.L.; Parreira, V.F.; Teixeira-Salmela, L.F. Inspiratory Muscular Training in Chronic Stroke Survivors: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2011, 92, 184–190. [Google Scholar] [CrossRef]
- Kigin, C.M. Breathing exercises for the medical patient: The art and the science. Phys. Ther. 1990, 70, 700–706. [Google Scholar] [CrossRef]
- Seo, K.C.; Lee, H.M.; Kim, H.A. The Effects of Combination of Inspiratory Diaphragm Exercise and Exspiratory Pursed-Lip Breathing Exercise on Pulmonary Functions of Stroke Patients. J. Phys. Ther. Sci. 2013, 25, 241–244. [Google Scholar] [CrossRef] [Green Version]
- Shetty, N.; Samuel, S.R.; Alaparthi, G.K.; Amaravadi, S.K.; Joshua, A.M.; Pai, S. Comparison of Diaphragmatic Breathing Exercises, Volume, and Flow-Oriented Incentive Spirometry on Respiratory Function in Stroke Subjects: A Non-Randomized Study. Ann. Neurosci. 2021, 0972753121990193. [Google Scholar] [CrossRef]
- Lee, H.-J.; Kang, T.-W.; Kim, B.-R. Effects of diaphragm and deep abdominal muscle exercise on walking and balance ability in patients with hemiplegia due to stroke. J. Exerc. Rehabil. 2018, 14, 648–653. [Google Scholar] [CrossRef]
- Seo, K.; Hwan, P.S.; Park, K. The effects of inspiratory diaphragm breathing exercise and expiratory pursed-lip breathing exercise on chronic stroke patients’ respiratory muscle activation. J. Phys. Ther. Sci. 2017, 29, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iyengar, Y.; Vijayakumar, K.; Abraham, J.; Misri, Z.; Suresh, B.; Unnikrishnan, B. Relationship between postural alignment in sitting by photogrammetry and seated postural control in post-stroke subjects. NeuroRehabilitation 2014, 35, 181–190. [Google Scholar] [CrossRef]
- Haghighat, F.; Moradi, R.; Rezaie, M.; Yarahmadi, N.; Ghaffarnejad, F. Added Value of Diaphragm Myofascial Release on forward Head Posture and Chest Expansion in Patients with Neck Pain: A Randomized Controlled Trial. 2020. Available online: https://assets.researchsquare.com/files/rs-53279/v1/e2455ee7-327f-43ab-a291-4b303dd5bcdb.pdf?fbclid=IwAR0xwROyiiX44msrom6gZ1cPCi3NUl4Kf9WWGMnLH-8fYpaVh0sKmQ3rDrA (accessed on 15 July 2021).
- Zafar, H.; Albarrati, A.; Alghadir, A.H.; Iqbal, Z.A. Effect of Different Head-Neck Postures on the Respiratory Function in Healthy Males. BioMed Res. Int. 2018, 2018, 4518269. [Google Scholar] [CrossRef] [Green Version]
- Triangto, K.; Widjanantie, S.C.; Nusdwinuringtyas, N. Biomechanical Impacts of forward Head Posture on the Respiratory Function. Indones. J. Phys. Med. Rehabil. 2019, 8, 50–64. [Google Scholar] [CrossRef]
- Maitland, G.D. Vertebral Manipulation; Butterworth-Heinemann: Oxford, UK, 2013. [Google Scholar]
- Park, S.-J. The Immediate Effect of Maitland Cervical Spine Mobilization on Tone and Stiffness of Upper Limb Muscles in Chronic Stroke Patients. Phys. Ther. Korea 2018, 25, 13–21. [Google Scholar] [CrossRef]
- Park, S.-J.; Kim, S.-H.; Min, K.-O. The immediate effects of rib cage joint mobilization and chest wall stretch on muscle tone and stiffness of respiratory muscles and chest expansion ability in patients with chronic stroke. J. Phys. Ther. Sci. 2017, 29, 1960–1963. [Google Scholar] [CrossRef] [Green Version]
- Park, S.J. Effects of Inspiratory Muscles Training Plus Rib Cage Mobilization on Chest Expansion, Inspiratory Accessory Muscles Activity and Pulmonary Function in Stroke Patients. Appl. Sci. 2020, 10, 5178. [Google Scholar] [CrossRef]
- Behne, G.; Silva, P.; Ré, D.d.; Vazatta, M.; Carvalho, A.R. Maximal respiratory pressures: Comparison between immediate manipulation effect and mobilization of the third cervical vertebra. Arq. Ciências Saúde da UNIPAR 2013, 17, 69–76. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Do, J.G.; Park, C.-H.; Lee, Y.-T.; Yoon, K.J. Association between underweight and pulmonary function in 282,135 healthy adults: A cross-sectional study in Korean population. Sci. Rep. 2019, 9, 14308. [Google Scholar] [CrossRef] [PubMed]
- Sheikhhoseini, R.; Shahrbanian, S.; Sayyadi, P.; O’Sullivan, K. Effectiveness of Therapeutic Exercise on forward Head Posture: A Systematic Review and Meta-Analysis. J. Manip. Physiol. Ther. 2018, 41, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.; Na, D.L.; Hahn, S.H. A validity study on the Korean Mini-Mental State Examination (K-MMSE) in dementia patients. J. Korean Neurol. Assoc. 1997, 15, 300–308. [Google Scholar]
- Do Bonfim, R.V.F.; de Moura Rocha, G.M.; da Silveira Sousa, A.M.; Rodrigues, B.F.O.; Almeida, V.R. Effect of Vertebral Mobilizations on Respiratory Pressure. In Proceedings of the XXVI Brazilian Congress on Biomedical Engineering, Vitória, Brazil, 26–30 October 2020; pp. 201–205. [Google Scholar]
- Vicenzino, B.; Cartwright, T.; Collins, D.; Wright, A. Cardiovascular and respiratory changes produced by lateral glide mobilization of the cervical spine. Man. Ther. 1998, 3, 67–71. [Google Scholar] [CrossRef]
- Miller, M.R.; Crapo, R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. General considerations for lung function testing. Eur. Respir. J. 2005, 26, 153–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salahzadeh, Z.; Maroufi, N.; Ahmadi, A.; Behtash, H.; Razmjoo, A.; Gohari, M.; Parnianpour, M. Assessment of forward head posture in females: Observational and photogrammetry methods. J. Back Musculoskelet. Rehabil. 2014, 27, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Park, S.J.; Park, S.E. Effect of upper thoracic mobilization on cervical alignment in stroke patients with forward head posture: A case study. J. Int. Acad. Phys. Ther. Res. 2018, 9, 1513–1516. [Google Scholar] [CrossRef] [Green Version]
- Park, S.J.; Kim, S.H. Effects of Kinesio Taping on the Pulmonary Function in Patients with Stroke during Manual Wheelchairs. J. Int. Acad. Phys. Ther. Res. 2018, 9, 1533–1536. [Google Scholar] [CrossRef]
- Da Silva, P.H.L.; de Ré, D.; Behne, G.R.; Vazatta, M.P.; de Carvalho, A.R. Maximum respiratory pressure alterations after spinal manipulation. Eur. J. Physiother. 2013, 15, 64–69. [Google Scholar] [CrossRef]
- John, S.; Tavee, J. Bilateral diaphragmatic paralysis due to cervical chiropractic manipulation. Neurologist 2015, 19, 65–67. [Google Scholar] [CrossRef] [PubMed]
- Koseki, T.; Kakizaki, F.; Hayashi, S.; Nishida, N.; Itoh, M. Effect of forward head posture on thoracic shape and respiratory function. J. Phys. Ther. Sci. 2019, 31, 63–68. [Google Scholar] [CrossRef] [Green Version]
- Jang, S.-H.; Bang, H.-S. Effect of thoracic and cervical joint mobilization on pulmonary function in stroke patients. J. Phys. Ther. Sci. 2016, 28, 257–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.-S.; Cho, K.-H.; Park, S.-J. The immediate effect of diaphragm taping with breathing exercise on muscle tone and stiffness of respiratory muscles and SpO2 in stroke patient. J. Phys. Ther. Sci. 2017, 29, 970–973. [Google Scholar] [CrossRef] [Green Version]
- Gandevia, S.; Rothwell, J.C. Activation of the human diaphragm from the motor cortex. J. Physiol. 1987, 384, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Sriboonreung, T.; Leelarungrayub, J.; Yankai, A.; Puntumetakul, R. Correlation and Predicted Equations of MIP/MEP from the Pulmonary Function, Demographics and Anthropometrics in Healthy Thai Participants aged 19 to 50 Years. Clin. Med. Insights Circ. Respir. Pulm. Med. 2021, 15, 11795484211004494. [Google Scholar] [CrossRef]
- Jo, M.-R.; Kim, N.-S. The correlation of respiratory muscle strength and cough capacity in stroke patients. J. Phys. Ther. Sci. 2016, 28, 2803–2805. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Experimental Group (n = 20) | |
|---|---|
| Gender(male/female) | 14/6 |
| Affected side(left/right) | 12/8 |
| Pathogenesis (hemorrhage/infarction) | 5/15 |
| Disease duration (months) | 11.50 ± 3.33 |
| Age (years) | 64.25 ± 11.47 |
| Height (cm) | 165.68 ± 8.35 |
| Weight (kg) | 64.86 ± 9.43 |
| BMI (kg/m2) | 23.51 ± 1.90 |
| K-MMSE (points) | 25.70 ± 1.78 |
| K-NIHSS (points) | 10.00 ± 3.48 |
| Classification | Experimental Group (n = 20) | Within Group Change a | t | p | % | Effect Size | |
|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | ||||||
| FEV1 (ℓ) | 2.15 ± 0.62 | 2.33 ± 0.64 | 0.18 ± 0.19 (0.10, 0.27) | 4.405 | 0.001 * | 8.37 | 0.95 |
| FVC (ℓ) | 2.64 ± 0.55 | 2.91 ± 0.64 | 0.26 ± 0.22 (0.16, 0.37) | 5.424 | 0.001 * | 10.23 | 1.23 |
| FEV1/FVC (%) | 80.00 ± 9.96 | 79.00 ± 8.51 | −1.00 ± 5.87 (−3.75, 1.75) | −0.762 | 0.455 | −1.25 | 0.17 |
| PEF (ℓ/min) | 213.30 ± 88.52 | 254.00 ± 98.34 | 40.70 ± 46.85 (18.78, 62.62) | 3.885 | 0.001 * | 19.08 | 0.87 |
| CVA (°) | 45.39 ± 6.26 | 46.04 ± 6.14 | 0.64 ± 0.72 (0.31, 0.98) | 4.031 | 0.001 * | 1.43 | 0.90 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
An, H.J.; Kim, A.Y.; Park, S.J. Immediate Effects of Diaphragmatic Breathing with Cervical Spine Mobilization on the Pulmonary Function and Craniovertebral Angle in Patients with Chronic Stroke. Medicina 2021, 57, 826. https://doi.org/10.3390/medicina57080826
An HJ, Kim AY, Park SJ. Immediate Effects of Diaphragmatic Breathing with Cervical Spine Mobilization on the Pulmonary Function and Craniovertebral Angle in Patients with Chronic Stroke. Medicina. 2021; 57(8):826. https://doi.org/10.3390/medicina57080826
Chicago/Turabian StyleAn, Ho Jung, A Yeon Kim, and Shin Jun Park. 2021. "Immediate Effects of Diaphragmatic Breathing with Cervical Spine Mobilization on the Pulmonary Function and Craniovertebral Angle in Patients with Chronic Stroke" Medicina 57, no. 8: 826. https://doi.org/10.3390/medicina57080826