
The Efficacy of Manual Therapy in Patients with Knee Osteoarthritis: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
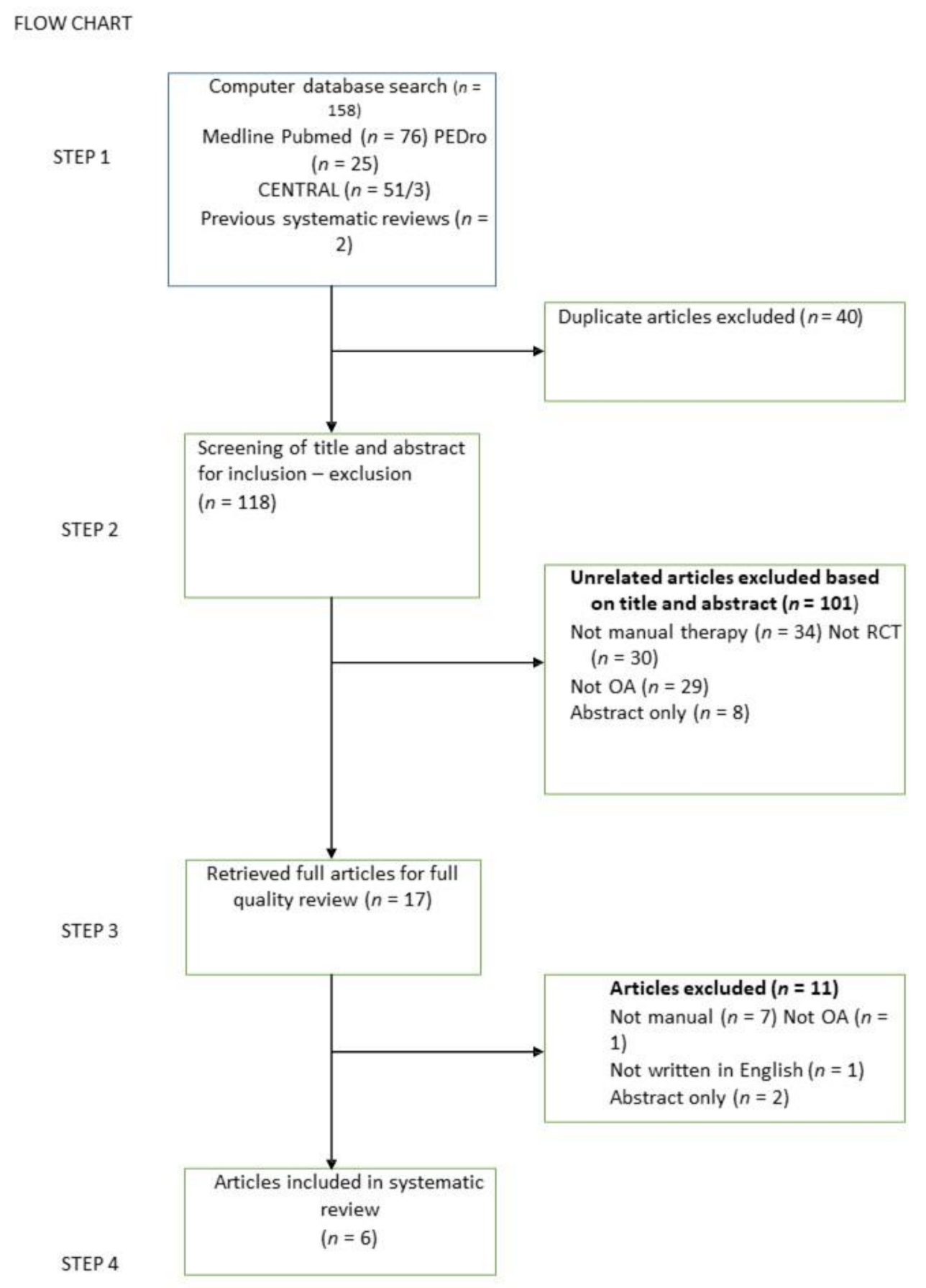
3. Results
3.1. Characteristics of the Included Studies
3.2. Trials
3.3. Interventions
3.4. Risk of Bias
3.5. Study Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bijlsma, J.W.; Berenbaum, F.; Lafeber, F.P. Osteoarthritis: An update with relevance for clinical practice. Lancet 2011, 377, 2115–2126. [Google Scholar] [CrossRef]
- Chan, W.P.; Lang, P.; Stevens, M.P.; Sack, K.; Majumdar, S.; Stoller, D.W.; Basch, C.; Genant, H.K. Osteoarthritis of the knee: Comparison of radiography, CT, and MR imaging to assess extent and severity. AJR Am. J. Roentgenol. 1991, 157, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Muehleman, C.; Bareither, D.; Huch, K.; Cole, A.A.; Kuettner, K.E. Prevalence of degenerative morphological changes in the joints of the lower extremity. Osteoarthr. Cartil. 1997, 5, 23–37. [Google Scholar] [CrossRef] [Green Version]
- Gamble, R.; Wyeth-Ayerst, J.; Johnson, E.L.; Searle, W.A.; Beecham, S. Recommendations for the medical management of osteoarthritis of the hip and knee. ArthritisRheum 2000, 43, 1905–1915. [Google Scholar]
- Bennell, K.L.; Hinman, R.S. A review of the clinical evidence for exercise in osteoarthritis of the hip and knee. J. Sci. Med. Sport 2011, 14, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Jackson, B.D.; Wluka, A.E.; Teichtahl, A.J.; Morris, M.E.; Cicuttini, F.M. Reviewing knee osteoarthritis—A biomechanical perspective. J. Sci. Med. Sport 2004, 7, 347–357. [Google Scholar] [CrossRef]
- Cook, C. Orthopedic Manual Therapy: An Evidence-Based Approach; Pearson Education: Upper Saddle River, NJ, USA, 2012. [Google Scholar]
- Cookson, J.C.; Kent, B.E. Orthopedic Manual Therapy—An Overview: Part I: The Extremities. Phys. Ther. 1979, 59, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.W.; Lucas, N. What is ‘manipulation’? A reappraisal. Man. Ther. 2010, 15, 286–291. [Google Scholar] [CrossRef]
- Bialosky, J.E.; Bishop, M.D.; Price, D.D.; Robinson, M.E.; George, S.Z. The mechanisms of manual therapy in the treatment of musculoskeletal pain: A comprehensive model. Man. Ther. 2009, 14, 531–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cookson, J.C. Orthopedic Manual Therapy—An Overview: Part II: The Spine. Phys. Ther. 1979, 59, 259–267. [Google Scholar] [CrossRef]
- Bishop, M.D.; Torres-Cueco, R.; Gay, C.W.; Lluch-Girbés, E.; Beneciuk, J.M.; Bialosky, J.E. What effect can manual therapy have on a patient’s pain experience? Pain Manag. 2015, 5, 455–464. [Google Scholar] [CrossRef] [Green Version]
- French, H.P.; Brennan, A.; White, B.; Cusack, T. Manual therapy for osteoarthritis of the hip or knee—A systematic review. Man. Ther. 2011, 16, 109–117. [Google Scholar] [CrossRef]
- Jansen, M.J.; Viechtbauer, W.; Lenssen, A.F.; Hendriks, E.J.; de Bie, R.A. Strength training alone, exercise therapy alone, and exercise therapy with passive manual mobilisation each reduce pain and disability in people with knee osteoarthritis: A systematic review. J. Physiother. 2011, 57, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Salamh, P.; Cook, C.; Reiman, M.P.; Sheets, C. Treatment effectiveness and fidelity of manual therapy to the knee: A systematic review andmeta-analysis. Musculoskelet. Care 2017, 15, 238–248. [Google Scholar] [CrossRef]
- Xu, Q.; Pang, J.; Zheng, Y.; Zhan, H.; Cao, Y.; Ding, C. The effectiveness of manual therapy for relieving pain, stiffness and dysfunction in knee osteoarthritis: A systematic review and meta-analysis. Osteoarthr. Cartil. 2015, 23, A387. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2011; Volume 4. [Google Scholar]
- Dickersin, K.; Manheimer, E.; Wieland, S.; Robinson, K.A.; Lefebvre, C.; McDonald, S.; Central Development Group. Development of the Cochrane Collaboration’s CENTRAL Register of controlled clinical trials. Eval. Health Prof. 2002, 25, 38–64. [Google Scholar]
- Michaleff, Z.A.; Costa, L.O.; Moseley, A.M.; Maher, C.G.; Elkins, M.R.; Herbert, R.D.; Sherrington, C. CENTRAL, PEDro, PubMed, and EMBASE are the most comprehensive databases indexing randomized controlled trials of physical therapy interventions. Phys. Ther. 2011, 91, 190–197. [Google Scholar] [CrossRef]
- Abbott, J.H.; Chapple, C.M.; Fitzgerald, G.K.; Fritz, J.M.; Childs, J.D.; Harcombe, H.; Stout, K. The incremental effects of manual therapy or booster sessions in addition to exercise therapy for knee osteoarthritis: A randomized clinical trial. J. Orthop. Sports Phys. Ther. 2015, 45, 975–983. [Google Scholar] [CrossRef]
- Asser, A.L.; Subramanian, L. Effectiveness of manual traction of tibio-femoral joint on the functional outcome in knee joint osteoarthritis. Indian J. Phys. Ther. 2014, 2, 56–61. [Google Scholar]
- Fitzgerald, G.K.; Fritz, J.M.; Childs, J.D.; Brennan, G.P.; Talisa, V.; Gil, A.B.; Neilson, B.D.; Abbott, J.H. Exercise, manual therapy, and use of booster sessions in physical therapy for knee osteoarthritis: A multi-center, factorial randomized clinical trial. Osteoarthr. Cartil. 2016, 24, 1340–1349. [Google Scholar] [CrossRef] [Green Version]
- Kaya Mutlu, E.; Ercin, E.; RazakOzdıncler, A.; Ones, N. A comparison of two manual physical therapy approaches and electrotherapy modalities for patients with knee osteoarthritis: A randomized three arm clinical trial. Physiother. Theory Pract. 2018, 34, 600–612. [Google Scholar] [CrossRef] [PubMed]
- Pollard, H.; Ward, G.; Hoskins, W.; Hardy, K. The effect of a manual therapy knee protocol on osteoarthritic knee pain: A randomised controlled trial. J. Can. Chiropr. Assoc. 2008, 52, 229. [Google Scholar] [PubMed]
- Sit, R.W.S.; Chan, K.K.W.; Zou, D.; Chan, D.C.C.; Yip, B.H.K.; Zhang, D.D.; Chan, Y.H.; Chung, V.C.H.; Reeves, K.D.; Wong, S.Y.S. Clinic-based patellar mobilization therapy for knee osteoarthritis: A randomized clinical trial. Ann. Fam. Med. 2018, 16, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Bialosky, J.E.; Beneciuk, J.M.; Bishop, M.D.; Coronado, R.A.; Penza, C.W.; Simon, C.B.; George, S.Z. Unraveling the Mechanisms of Manual Therapy: Modeling an Approach. JOSPT 2018, 48, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Voogt, L.; de Vries, J.; Meeus, M.; Struyf, F.; Meuffels, D.; Nijs, J. Analgesic effects of manual therapy in patients with musculoskeletal pain: A systematic review. Man. Ther. 2015, 20, 250–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McPartland, J.M.; Giuffrida, A.; King, J.; Skinner, E.; Scotter, J.; Musty, R.E. Cannabimimetic effects of osteopathic manipulative treatment. J. Am. Osteopath. Assoc. 2005, 105, 283–291. [Google Scholar] [PubMed]
- Lima, C.R.; Martins, D.F.; Reed, W.R. Physiological Responses Induced by Manual Therapy in Animal Models: A Scoping Review. Front. Neurosci. 2020, 14, 430. [Google Scholar] [CrossRef]
- Teodorczyk-Injeyan, J.A.; Triano, J.J.; Gringmuth, R.; DeGraauw, C.; Chow, A.; Injeyan, H.S. Effects of spinal manipulative therapy on inflammatory mediators in patients with non-specific low back pain: A non-randomized controlled clinical trial. Chiropr. Man. Therap. 2021, 29, 3. [Google Scholar] [CrossRef]
- Savva, C.; Giakas, G.; Efstathiou, M. The role of the descending inhibitory pain mechanism in musculoskeletal pain following high-velocity, low amplitude thrust manipulation: A review of the literature. J. Back Musculoskelet. Rehabil. 2014, 27, 377–382. [Google Scholar] [CrossRef] [Green Version]
- Courtney, C.A.; Steffen, A.D.; Fernández-de-las-Pñas, C.; Kim, J.; Chmell, S.J. Joint Mobilization Enhances Mechanisms of Conditioned Pain Modulation in Individuals With Osteoarthritis of the Knee. JOSPT 2016, 46, 168–176. [Google Scholar] [CrossRef] [Green Version]
- Brantingham, J.W.; Bonnefin, D.; Perle, S.M.; Cassa, T.K.; Globe, G.; Pribicevic, M.; Hicks, M.; Korporaal, C. Manipulative therapy for lower extremity conditions: Update of a literature review. J. Manip. Physiol. Ther. 2012, 35, 127–166. [Google Scholar] [CrossRef]
- Knapik, D.M.; Harris, J.D.; Pangrazzi, G.; Griesser, M.J.; Siston, R.A.; Agarwal, S.; Flanigan, D.C. The Basic Science of Continuous Passive Motion in Knee Health: A Systematic Review of Studies in a Rabbit Model. Arthroscopy 2013, 29, 1722–1731. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Criteria for Evaluating the Methodological Quality of the Research Studies | Assessment |
|---|---|
| Random sequence generation | +/−/? |
| Allocation concealment | +/−/? |
| Blinding of the research | +/−/? |
| Blinding of the participants | +/−/? |
| Blinding of the outcome assessment | +/−/? |
| Selective reporting | +/−/? |
| Incomplete outcome data | +/−/? |
| Other potential threats | +/−/? |
| Study Characteristics | Kaya Mutlu et al., 2018 | Sit et al., 2018 | Fitzgerald et al., 2016 | Abbott et al., 2015 | Aseerand Subramanian, 2014 | Pollard et al., 2008 |
|---|---|---|---|---|---|---|
| No. of participants | 64 (21 MWM, 21 PJM, 22 ET) | 208 (104 in the control group and 104 in the intervention group | 300 (75 Ex, 76 ExB, 75 Ex+MT, 74 Ex+B+MT) | 75 (Ex19, ExB 19, Ex+MT 18, Ex+B+MT 19) | 40 (20 control group, 20 experimental group) | 43 (26 MIMG, 17 control group) |
| Sex | 56 females 8 males | 167 females 41 males | 199 females 101 males | 46 females 29 males | 26 females 14 males | 14 females 29 males |
| Group distribution by sex/BMI/age | No significant differences between groups | No significant differences between groups | No significant differences between groups | No significant differences between groups | No significant differences between groups | Not reported |
| Dropouts | 14 | 13 | Not reported | 9 | 0 | 0 |
| Diagnostic criteria | MRI, Clinical examination | MRI and clinical examination | Not reported- | Clinical examination | MRI and clinical examination | McGill pain questionnaire |
| Therapeutic intervention | MWM PJM electrotherapy | PMT Conventional medication PT Acupuncture Drugs | Ex ExB MTEx MTBEx | Ex ExB Ex+MT Ex+B+MT | Pain control modalities MT Exercise | MIMG Placebo MIMG |
| Duration of intervention | 4 weeks | 24weeks | No boosters: 9 weeks Boosters: 11 months | No boosters: 9 weeks Boosters: 11 months | 2 weeks | 2 weeks |
| Outcome evaluation | WOMAC VAS ROM Muscle strength | WOMAC VAS EuroQuol-SD Clinical tests | WOMAC VAS Clinical tests | WOMAC VAS Clinical tests | VAS ROM KOOS | VAS |
| Reassessment | 12 months | 2 months–4 months–6 months | 12 months | 12 months | - | - |
| Studies | ||||||
|---|---|---|---|---|---|---|
| Criteria | Kaya Mutlu et al., 2018 | Sit et al., 2018 | Fitzgerald et al., 2016 | Abbott et al., 2015 | Aseer and Subramanian, 2014 | Pollard et al., 2008 |
| Sequence generation | + | + | + | + | + | + |
| Allocation concealment | + | + | − | + | ? | + |
| Blinding of the research | − | − | − | − | − | ? |
| Blinding of the participants | ? | − | − | ? | ? | + |
| Blinding of the outcome assessment | + | + | + | + | + | ? |
| Selective reporting | + | + | + | + | + | + |
| Incomplete outcome data | + | + | + | + | + | + |
| Other potential threats | + | + | + | + | + | + |
| Final evaluation | Sufficient quality | Poor quality | Poor quality | Sufficient quality | Unspecified quality | Unspecified quality |
| Results | Kaya Mutlu et al., 2018 | Sit et al., 2018 | Fitzgerald et al., 2016 | Abbott et al., 2015 | Aseer and Subramanian, 2014 | Pollard et al., 2008 |
|---|---|---|---|---|---|---|
| Control group | - | No Significant improvement | - | - | No significant improvement | No significant improvement |
| Intervention group | - | Significant improvement at: WOMAC, clinical tests | - | - | Significant improvement of pain | Significant improvement of pain, functionality and knee joint stiffness |
| PJM | Significant improvement of ROM, the quadriceps, strength and pain | - | - | - | - | - |
| MWM | Significant improvement of ROM, the quadriceps, strength and pain | - | - | - | - | - |
| Electrotherapy group | No significant improvement of ROM, the quadriceps, strength and pain | - | - | - | - | - |
| Ex | - | - | No significant improvement | No significant improvement | - | - |
| ExB | - | - | No significant improvement | Significant improvement compared with Ex | - | - |
| MT + Ex | - | - | Significant improvement in WOMAC | Significant improvement compared with Ex and the four groups Better results in terms of pain | - | - |
| MT + Ex + B | - | - | Significant improvement in WOMAC | No significant improvement | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsokanos, A.; Livieratou, E.; Billis, E.; Tsekoura, M.; Tatsios, P.; Tsepis, E.; Fousekis, K. The Efficacy of Manual Therapy in Patients with Knee Osteoarthritis: A Systematic Review. Medicina 2021, 57, 696. https://doi.org/10.3390/medicina57070696
Tsokanos A, Livieratou E, Billis E, Tsekoura M, Tatsios P, Tsepis E, Fousekis K. The Efficacy of Manual Therapy in Patients with Knee Osteoarthritis: A Systematic Review. Medicina. 2021; 57(7):696. https://doi.org/10.3390/medicina57070696
Chicago/Turabian StyleTsokanos, Alexios, Elpiniki Livieratou, Evdokia Billis, Maria Tsekoura, Petros Tatsios, Elias Tsepis, and Konstantinos Fousekis. 2021. "The Efficacy of Manual Therapy in Patients with Knee Osteoarthritis: A Systematic Review" Medicina 57, no. 7: 696. https://doi.org/10.3390/medicina57070696