
Vital Pulp Therapy in Permanent Mature Posterior Teeth with Symptomatic Irreversible Pulpitis: A Systematic Review of Treatment Outcomes

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Extraction and Analysis
2.2. Recall Rate and Treatment Outcomes
2.3. Quality Assessment
3. Results
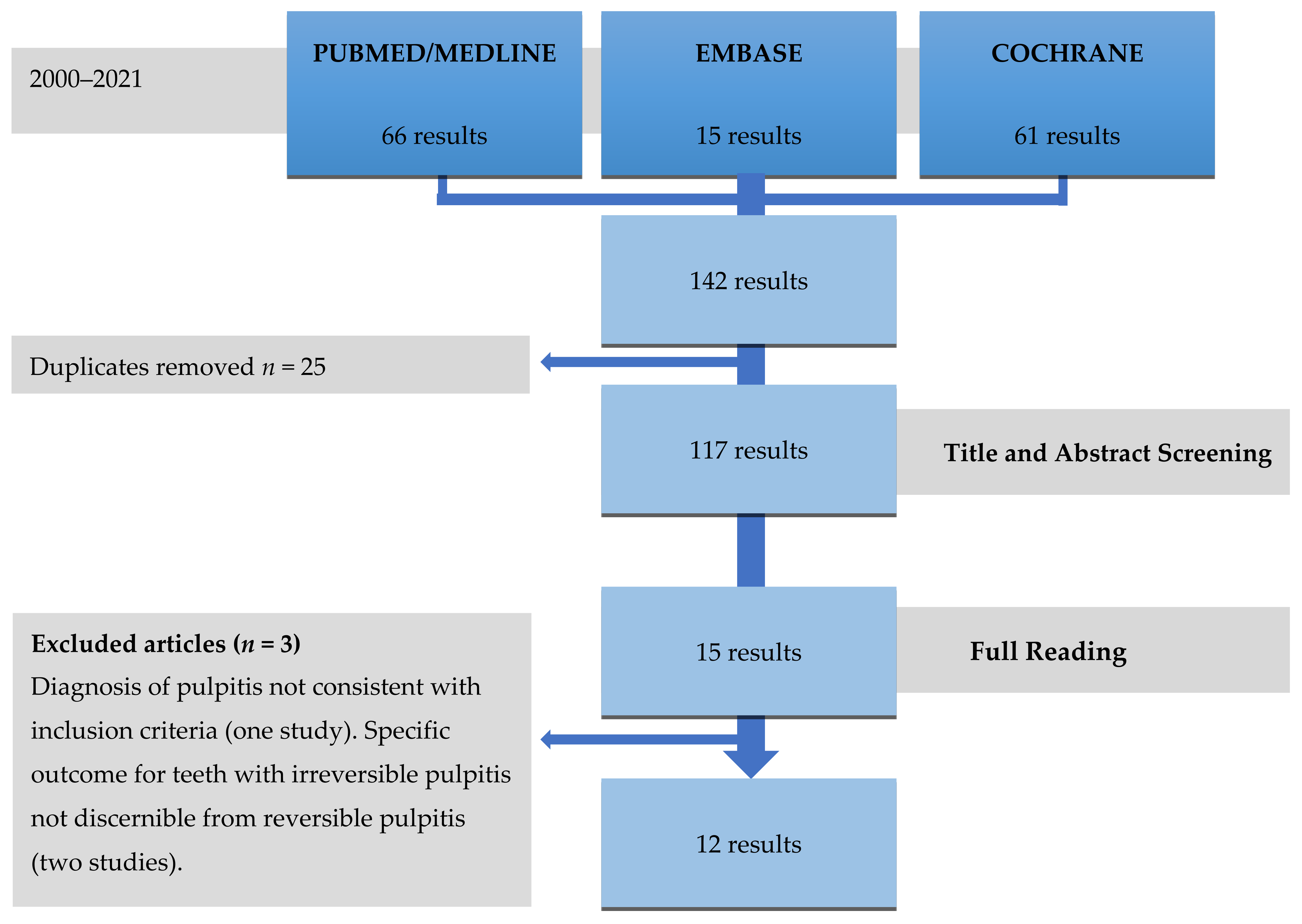
3.1. Selected Studies
3.2. Quality Assessment
3.3. Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wolters, W.J.; Duncan, H.F.; Tomson, P.L.; Karim, I.E.; McKenna, G.; Dorri, M.; Stangvaltaite, L.; Van Der Sluis, L.W.M. Minimally invasive endodontics: A new diagnostic system for assessing pulpitis and subsequent treatment needs. Int. Endod. J. 2017, 50, 825–829. [Google Scholar] [CrossRef]
- Asgary, S.; Eghbal, M.J.; Ghoddusi, J.; Yazdani, S. One-year results of vital pulp therapy in permanent molars with irreversible pulpitis: An ongoing multicenter, randomized, non-inferiority clinical trial. Clin. Oral Investig. 2013, 17, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Asgary, S.; Eghbal, M.J.; Ghoddusi, J. Two-year results of vital pulp therapy in permanent molars with irreversible pulpitis: An ongoing multicenter randomized clinical trial. Clin. Oral Investig. 2014, 18, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Asgary, S.; Eghbal, M.J.; Fazlyab, M.; Baghban, A.A.; Ghoddusi, J. Five-year results of vital pulp therapy in permanent molars with irreversible pulpitis: A non-inferiority multicenter randomized clinical trial. Clin. Oral Investig. 2015, 19, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Asgary, S.; Eghbal, M.J. Treatment outcomes of pulpotomy in permanent molars with irreversible pulpitis using biomaterials: A multi-center randomized controlled trial. Acta Odontol. Scand. 2013, 71, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Asgary, S.; Eghbal, M.J.; Bagheban, A.A. Long-term outcomes of pulpotomy in permanent teeth with irreversible pulpitis: A multi-center randomized controlled trial. Am. J. Dent. 2017, 30, 151–155. [Google Scholar] [PubMed]
- Taha, N.A.; Khazali, M.A. Partial Pulpotomy in Mature Permanent Teeth with Clinical Signs Indicative of Irreversible Pulpitis: A Randomized Clinical Trial. J. Endod. 2017, 43, 1417–1421. [Google Scholar] [CrossRef] [PubMed]
- Uesrichai, N.; Nirunsittirat, A.; Chuveera, P.; Srisuwan, T.; Sastraruji, T.; Chompu-Inwai, P. Partial pulpotomy with two bioactive cements in permanent teeth of 6- to 18-year-old patients with signs and symptoms indicative of irreversible pulpitis: A noninferiority randomized controlled trial. Int. Endod. J. 2019, 52, 749–759. [Google Scholar] [CrossRef]
- Ricucci, D.; Loghin, S.; Siqueira, J.F. Correlation between Clinical and Histologic Pulp Diagnoses. J. Endod. 2014, 40, 1932–1939. [Google Scholar] [CrossRef]
- Ricucci, D.; Siqueira, J.F.; Li, Y.; Tay, F.R. Vital pulp therapy: Histopathology and histobacteriology-based guidelines to treat teeth with deep caries and pulp exposure. J. Dent. 2019, 86, 41–52. [Google Scholar] [CrossRef]
- Quality guidelines for endodontic treatment: Consensus report of the European Society of Endodontology. Int. Endod. J. 2006, 39, 921–930. [CrossRef]
- American Association of Endodontists, Guide to Clinical Endodontics 2013. Available online: https://www.aae.org/specialty/clinical-resources/guide-clinicalendodontics/ (accessed on 1 September 2020).
- Hasselgren, B.G. Treatment of the Exposed Dentin-Pulp Complex. In Essential Endodontology: Prevention and Treatment of Apical Periodontitis; Ørstavik, D., Pitt-Ford, T., Eds.; Blackwell Munksgaard: Oxford, UK, 2008; pp. 297–315. [Google Scholar]
- Simon, S.; Perard, M.; Zanini, M.; Smith, A.J.; Charpentier, E.; Djole, S.X.; Lumley, P.J. Should pulp chamber pulpotomy be seen as a permanent treatment? Some preliminary thoughts. Int. Endod. J. 2013, 46, 79–87. [Google Scholar] [CrossRef]
- Wigsten, E.; Kvist, T.; Jonasson, P.; Davidson, T.; Bjørndal, L.; Dawson, V.S.; Fransson, H.; Frisk, F.; Markvart, M.; Pigg, M.; et al. Comparing Quality of Life of Patients Undergoing Root Canal Treatment or Tooth Extraction. J. Endod. 2020, 46, 19–28. [Google Scholar] [CrossRef]
- Sjögren, U.; Hägglund, B.; Sundqvist, G.; Wing, K. Factors affecting the long-term results of endodontic treatment. J. Endod. 1990, 16, 498–504. [Google Scholar] [CrossRef]
- De Chevigny, C.; Dao, T.T.; Basrani, B.R.; Marquis, V.; Farzaneh, M.; Abitbol, S.; Friedman, S. Treatment Outcome in Endodontics: The Toronto Study—Phase 4: Initial Treatment. J. Endod. 2008, 34, 258–263. [Google Scholar] [CrossRef]
- Ng, Y.-L.; Mann, V.; Gulabivala, K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: Part 1: Periapical health. Int. Endod. J. 2011, 44, 583–609. [Google Scholar] [CrossRef]
- Dugas, N.N.; Lawrence, H.; Teplitsky, P.E.; Pharoah, M.J.; Friedman, S. Periapical health and treatment quality assessment of root-filled teeth in two Canadian populations. Int. Endod. J. 2003, 36, 181–192. [Google Scholar] [CrossRef]
- Diogo, P.; Palma, P.J.; Caramelo, F.; Dos Santos, J.M.M. Prevalence of apical periodontitis in an adult Portuguese population. Rev. Port. Estomatol. Med. Dentária Cir. Maxilofac. 2014, 55, 36–42. [Google Scholar] [CrossRef] [Green Version]
- Pak, J.G.; Fayazi, S.; White, S.N. Prevalence of Periapical Radiolucency and Root Canal Treatment: A Systematic Review of Cross-sectional Studies. J. Endod. 2012, 38, 1170–1176. [Google Scholar] [CrossRef]
- Jakovljevic, A.; Nikolic, N.; Jacimovic, J.; Pavlovic, O.; Milicic, B.; Beljic-Ivanovic, K.; Miletic, M.; Andric, M.; Milasin, J. Prevalence of Apical Periodontitis and Conventional Nonsurgical Root Canal Treatment in General Adult Population: An Updated Systematic Review and Meta-analysis of Cross-sectional Studies Published between 2012 and 2020. J. Endod. 2020, 46, 1371–1386. [Google Scholar] [CrossRef]
- Duncan, H.F.; Galler, K.M.; Tomson, P.L.; Simon, S.; El-Karim, I.; Kundzina, R.; Krastl, G.; Dammaschke, T.; Fransson, H.; Markvart, M.; et al. European Society of Endodontology position statement: Management of deep caries and the exposed pulp. Int. Endod. J. 2019, 52, 923–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, H.-H.; Chang, Y.-J.; Yeh, C.-L.; Lin, T.-A.; Lin, C.-P. Development of calcium phosphate/calcium sulfate biphasic biomedical material with hyaluronic acid containing collagenase and simvastatin for vital pulp therapy. Dent. Mater. 2020, 36, 755–764. [Google Scholar] [CrossRef] [PubMed]
- Cohenca, N.; Paranjpe, A.; Berg, J. Vital Pulp Therapy. Dent. Clin. N. Am. 2013, 57, 59–73. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, P.; Linsuwanont, P. Vital Pulp Therapy in Vital Permanent Teeth with Cariously Exposed Pulp: A Systematic Review. J. Endod. 2011, 37, 581–587. [Google Scholar] [CrossRef]
- Mejare, I.; Cvek, M. Partial pulpotomy in young permanent teeth with deep carious lesions. Dent. Traumatol. 1993, 9, 238–242. [Google Scholar] [CrossRef]
- Witherspoon, D.E.; Small, J.C.; Harris, G.Z. Mineral trioxide aggregate pulpotomies: A case series outcomes assessment. J. Am. Dent. Assoc. 2006, 137, 610–618. [Google Scholar] [CrossRef] [Green Version]
- Chueh, L.-H.; Chiang, C.-P. Histology of Irreversible Pulpitis Premolars Treated with Mineral Trioxide Aggregate Pulpotomy. Oper. Dent. 2010, 35, 370–374. [Google Scholar] [CrossRef] [Green Version]
- Mente, J.; Hufnagel, S.; Leo, M.; Michel, A.; Gehrig, H.; Panagidis, D.; Saure, D.; Pfefferle, T. Treatment Outcome of Mineral Trioxide Aggregate or Calcium Hydroxide Direct Pulp Capping: Long-term Results. J. Endod. 2014, 40, 1746–1751. [Google Scholar] [CrossRef]
- Li, Y.; Sui, B.; Dahl, C.; Bergeron, B.; Shipman, P.; Niu, L.; Chen, J.; Tay, F.R. Pulpotomy for carious pulp exposures in permanent teeth: A systematic review and meta-analysis. J. Dent. 2019, 84, 1–8. [Google Scholar] [CrossRef]
- Elmsmari, F.; Ruiz, X.-F.; Miró, Q.; Feijoo-Pato, N.; Durán-Sindreu, F.; Olivieri, J.G. Outcome of Partial Pulpotomy in Cariously Exposed Posterior Permanent Teeth: A Systematic Review and Meta-analysis. J. Endod. 2019, 45, 1296–1306. [Google Scholar] [CrossRef]
- Alqaderi, H.; Lee, C.-T.; Borzangy, S.; Pagonis, T.C. Coronal pulpotomy for cariously exposed permanent posterior teeth with closed apices: A systematic review and meta-analysis. J. Dent. 2016, 44, 1–7. [Google Scholar] [CrossRef]
- Juneja, R.; Kumar, V.; Duhan, J.; Sangwan, P.; Tewari, S. Comparative evaluation of platelet-rich fibrin, mineral trioxide aggregate, and calcium hydroxide as pulpotomy agents in permanent molars with irreversible pulpitis: A randomized controlled trial. Contemp. Clin. Dent. 2016, 7, 512–518. [Google Scholar] [CrossRef]
- Qudeimat, M.A.; Alyahya, A.; Hasan, A.A.; Barrieshi-Nusair, K.M. Mineral trioxide aggregate pulpotomy for permanent molars with clinical signs indicative of irreversible pulpitis: A preliminary study. Int. Endod. J. 2017, 50, 126–134. [Google Scholar] [CrossRef]
- Taha, N.A.; Abdulkhader, S.Z. Full Pulpotomy with Biodentine in Symptomatic Young Permanent Teeth with Carious Exposure. J. Endod. 2018, 44, 932–937. [Google Scholar] [CrossRef]
- Taha, N.A.; Abdelkhader, S.Z. Outcome of full pulpotomy using Biodentine in adult patients with symptoms indicative of irreversible pulpitis. Int. Endod. J. 2018, 51, 819–828. [Google Scholar] [CrossRef]
- Asgary, S.; Hassanizadeh, R.; Torabzadeh, H.; Eghbal, M.J. Treatment Outcomes of 4 Vital Pulp Therapies in Mature Molars. J. Endod. 2018, 44, 529–535. [Google Scholar] [CrossRef]
- Cushley, S.; Duncan, H.F.; Lappin, M.J.; Tomson, P.L.; Lundy, F.T.; Cooper, P.; Clarke, M.; El Karim, I.A. Pulpotomy for mature carious teeth with symptoms of irreversible pulpitis: A systematic review. J. Dent. 2019, 88, 103158. [Google Scholar] [CrossRef]
- Taha, N.A.; Ahmad, M.B.; Ghanim, A. Assessment of Mineral Trioxide Aggregate pulpotomy in mature permanent teeth with carious exposures. Int. Endod. J. 2016, 50, 117–125. [Google Scholar] [CrossRef]
- Koli, B.; Chawla, A.; Logani, A.; Kumar, V.; Sharma, S. Combination of Nonsurgical Endodontic and Vital Pulp Therapy for Management of Mature Permanent Mandibular Molar Teeth with Symptomatic Irreversible Pulpitis and Apical Periodontitis. J. Endod. 2021, 47, 374–381. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; A Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Galani, M.; Tewari, S.; Sangwan, P.; Mittal, S.; Kumar, V.; Duhan, J. Comparative Evaluation of Postoperative Pain and Success Rate after Pulpotomy and Root Canal Treatment in Cariously Exposed Mature Permanent Molars: A Randomized Controlled Trial. J. Endod. 2017, 43, 1953–1962. [Google Scholar] [CrossRef] [PubMed]
- American Association of Endodontists, Glossary of Endodontic Terms, Tenth Ed., Chicago, IL. Available online: https://www.aae.org/specialty/clinicalresources/glossary-endodontic-terms/ (accessed on 13 March 2020).
- Zanini, M.; Hennequin, M.; Cousson, P.-Y. A Review of Criteria for the Evaluation of Pulpotomy Outcomes in Mature Permanent Teeth. J. Endod. 2016, 42, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Azimi, S.; Fazlyab, M.; Sadri, D.; Saghiri, M.A.; Khosravanifard, B.; Asgary, S. Comparison of pulp response to mineral trioxide aggregate and a bioceramic paste in partial pulpotomy of sound human premolars: A randomized controlled trial. Int. Endod. J. 2014, 47, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Zanini, M.; Hennequin, M.; Cousson, P. Which procedures and materials could be applied for full pulpotomy in permanent mature teeth? A systematic review. Acta Odontol. Scand. 2019, 77, 541–551. [Google Scholar] [CrossRef]
- Lin, L.M.; Ricucci, D.; Saoud, T.M.; Sigurdsson, A.; Kahler, B. Vital pulp therapy of mature permanent teeth with irreversible pulpitis from the perspective of pulp biology. Aust. Endod. J. 2020, 46, 154–166. [Google Scholar] [CrossRef]
- Sundqvist, G. Bacteriological Studies of Necrotic Dental Pulps; University of Umeå: Umeå, Sweden, 1976. [Google Scholar]
- Stashenko, P.; Teles, R.; D’Souza, R. Periapical Inflammatory Responses and Their Modulation. Crit. Rev. Oral Biol. Med. 1998, 9, 498–521. [Google Scholar] [CrossRef]
- Abella, F.; Patel, S.; Duran-Sindreu, F.; Mercadé, M.; Bueno, R.; Roig, M. Evaluating the Periapical Status of Teeth with Irreversible Pulpitis by Using Cone-beam Computed Tomography Scanning and Periapical Radiographs. J. Endod. 2012, 38, 1588–1591. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Authors, Year | Title | Design |
|---|---|---|
| Asgary et al. 2013 [2] | One-year results of vital pulp therapy in permanent molars with irreversible pulpitis: an ongoing multicenter, randomized, non-inferiority clinical trial | Randomized controlled trial |
| Asgary et al. 2014 [3] | Two-year results of vital pulp therapy in permanent molars with irreversible pulpitis: an ongoing multicenter, randomized clinical trial | Randomized controlled trial |
| Asgary et al. 2015 [4] | Five-year results of vital pulp therapy in permanent molars with irreversible pulpitis: a non-inferiority multicenter, randomized clinical trial | Randomized controlled trial |
| Asgary & Eghbal 2013 [5] | Treatment outcomes of pulpotomy in permanent molars with irreversible pulpitis using biomaterials: a multi-center, randomized controlled trial | Randomized controlled trial |
| Asgary et al. 2017 [6] | Long-term outcomes of pulpotomy in permanent teeth with irreversible pulpitis: a multicenter, randomized controlled trial | Randomized controlled trial |
| Kumar et al. 2016 [34] | Comparative evaluation of platelet-rich fibrin, mineral trioxide aggregate, and calcium hydroxide as pulpotomy agents in permanent molars with irreversible pulpitis: A randomized controlled trial | Randomized controlled trial |
| Qudeimat et al. 2017 [35] | Mineral trioxide aggregate pulpotomy for permanent molars with clinical signs indicative of irreversible pulpitis: a preliminary study | Prospective cohort study |
| Taha & Abdulkhader 2018 [36] | Full pulpotomy with Biodentine in symptomatic young permanent teeth with carious exposure | Prospective cohort study |
| Taha & Abdelkhader 2018 [37] | Outcome of full pulpotomy using Biodentine in adult patients with symptoms indicative of irreversible pulpitis | Prospective cohort study |
| Taha & Khazali 2017 [7] | Partial pulpotomy in mature permanent teeth with clinical signs indicative of irreversible pulpitis: A randomized clinical trial | Randomized controlled trial |
| Uesrichai et al. 2019 [8] | Partial pulpotomy with two bioactive cements in permanent teeth of 6-to-18-year-old patients with signs and symptoms indicative of irreversible pulpitis: a non-inferiority randomised controlled trial | Randomized controlled trial |
| Koli et al. 2021 [41] | Combination of nonsurgical endodontic and vital pulp therapy for management of mature permanent mandibular molar teeth with symptomatic irreversible pulpitis and apical periodontitis | Randomized controlled trial |
| Article | Study Arm | Study Sample (n) | Recall Rate (%) | Pulpitis Diagnosis | Age Range (years) | Time for Bleeding Control | Success Rate (%) at Different Follow-Up Periods | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Initial | Final | 1 year | 2 years | >2 years | ||||||
| Asgary et al. 2013 [2] 2 study arms | FP CEM | 205 | 167 | 84.0% | Spontaneous pain for a few seconds to several hours, pain exacerbating with hot and cold fluids, radiating pain, or reproducible pain with cold testing | 9–65 | NR | C: 97.6% R: 92.2% | - | - |
| NSRCT | 202 | 175 | C: 98.3% R: 70.3% | - | - | |||||
| Asgary et al. 2014 [3] 2 study arms | FP CEM | 205 | 166 | 81.6% | Spontaneous pain for a few seconds to several hours, pain exacerbating with hot and cold fluids, radiating pain, or reproducible pain with cold testing | 9–65 | NR | - | C: 98.2% R: 86.1% | - |
| NSRCT | 202 | 166 | - | C: 98.2% R: 79.5% | - | |||||
| Asgary et al. 2015 [4] 2 study arms | FP CEM | 205 | 137 | 66.6% | Spontaneous pain for a few seconds to several hours, pain exacerbating with hot and cold fluids, radiating pain, or reproducible pain with cold testing | 9–65 | NR | - | - | 5 years O: 78.1% |
| NSRCT | 202 | 134 | - | - | 5 years O: 75.3% | |||||
| Asgary & Eghbal 2013 [5] 2 study arms | FP MTA | 208 | 179 | 83.7% | Spontaneous pain for a few seconds to several hours with extensive caries; pain exacerbated with hot and cold fluids and/or radiating pain | 9–65 | NR | C: 98.3% R: 95.0% | - | - |
| FP CEM *** | 205 | 167 | C: 97.6% R: 92.2% | - | - | |||||
| Asgary et al. 2017 [6] 2 study arms | FPMTA | 208 | 2 years 178 5 years 154 | 2 years 83.2% 5 years 73.6% | Spontaneous pain for a few seconds to several hours with extensive caries; pain exacerbated with hot and cold fluids and/or radiating pain | 9–65 | NR | - | C: 98.9% R: 94.9% | 5 years C: 98.1% R: 84.6% |
| FP CEM *** | 205 | 2 years 166 5 years 150 | - | C: 98.2% R: 86.1% | 5 years C: 98.0% R: 78.1% | |||||
| Kumar et al. 2016 [34] 3 study arms | FP ProRoot MTA | 19 | 15 | 75.9% | Spontaneous, lingering pain, exacerbated by hot and cold fluids, and/or radiating pain | 14–32 | NR | C: 83.3% R: 53.3% | - | - |
| FP PRF | 17 | 13 | 14–32 | C: 92.8% R: 38.4% | - | - | ||||
| FP CH | 18 | 13 | 14–23 | C: 81.2% R: 46.1% | - | - | ||||
| Taha & Khazali 2017 [7] 2 study arms | PP ProRoot MTA White | 27 | 26 | 98.1% | Severe spontaneous lingering pain that could be reproduced by cold stimuli | 20–52 | A pellet moistened with 2.5% NaOCl for 2 min and repeated as needed | O: 83.0% | O: 85.0% | - |
| PP CH | 23 | 23 | O: 55.0% | O: 43.0% | - | |||||
| Uesrichai et al. 2019 * [8] 2 study arms | PP ProRoot MTA | 13 | 13 | 100% | Spontaneous pain together with sharp and lingering pain with cold testing | 8–17 | Up to 10 min | - | - | 35 ± 14 months O: 85.0% C: 85.0% R: 92.0% |
| PP Biodentine | 10 | 10 | 45 ± 18 months O: 90.0% C: 90.0% R: 100% | |||||||
| Koli et al. 2021 ** [41] 2 study arms | FP MTA + NSRCT | 30 | 28 | 100% | Positive response to a pulp sensibility test with periapical index score ≥ 3 | 18–35 | Up to 8 min | O: 93.3% | ||
| NSRCT | 30 | 27 | O: 90% | |||||||
| Author, Year | Pulpotomy Material | Study Sample (n) | Recall Rate | Pulpitis Diagnosis | Age Range (years) | Time for Bleeding Control | Success Rate (%) at Different Follow-Up Periods | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Initial | Final | 1 year | 2 years | >2 years | ||||||
| Qudeimat et al. 2017 * [35] | ProRoot MTA Grey and White | 13 | 13 | 100% ** | Intermittent or spontaneous pain; rapid exposure to dramatic temperature changes elicited heightened and prolonged episodes of pain even after the thermal stimulus has been removed | 10–13 | 5 to 25 min | - | - | Mean 57.2 months O: 100% |
| Taha & Abdulkhader 2018 * [36] | Biodentine | 17 | 17 | 100% | Spontaneous pain or pain exacerbated by cold stimuli and lasting for a few seconds to several hours interpreted as lingering pain compared with the control teeth | 9–17 | 4 min | C: 100% R: 94.1% | - | - |
| Taha & Abdulkhader 2018 [37] | Biodentine | 64 | 60 | 93.7% | Pain or symptoms classically indicative of symptomatic irreversible pulpitis according to AAE diagnostic terminology | 19–69 | Up to 6 min | C: 100% R: 98.4% | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, J.M.; Pereira, J.F.; Marques, A.; Sequeira, D.B.; Friedman, S. Vital Pulp Therapy in Permanent Mature Posterior Teeth with Symptomatic Irreversible Pulpitis: A Systematic Review of Treatment Outcomes. Medicina 2021, 57, 573. https://doi.org/10.3390/medicina57060573
Santos JM, Pereira JF, Marques A, Sequeira DB, Friedman S. Vital Pulp Therapy in Permanent Mature Posterior Teeth with Symptomatic Irreversible Pulpitis: A Systematic Review of Treatment Outcomes. Medicina. 2021; 57(6):573. https://doi.org/10.3390/medicina57060573
Chicago/Turabian StyleSantos, João Miguel, Joana F. Pereira, Andréa Marques, Diana B. Sequeira, and Shimon Friedman. 2021. "Vital Pulp Therapy in Permanent Mature Posterior Teeth with Symptomatic Irreversible Pulpitis: A Systematic Review of Treatment Outcomes" Medicina 57, no. 6: 573. https://doi.org/10.3390/medicina57060573