
The Management of Immunosuppression in Kidney Transplant Recipients with COVID-19 Disease: An Update and Systematic Review of the Literature

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
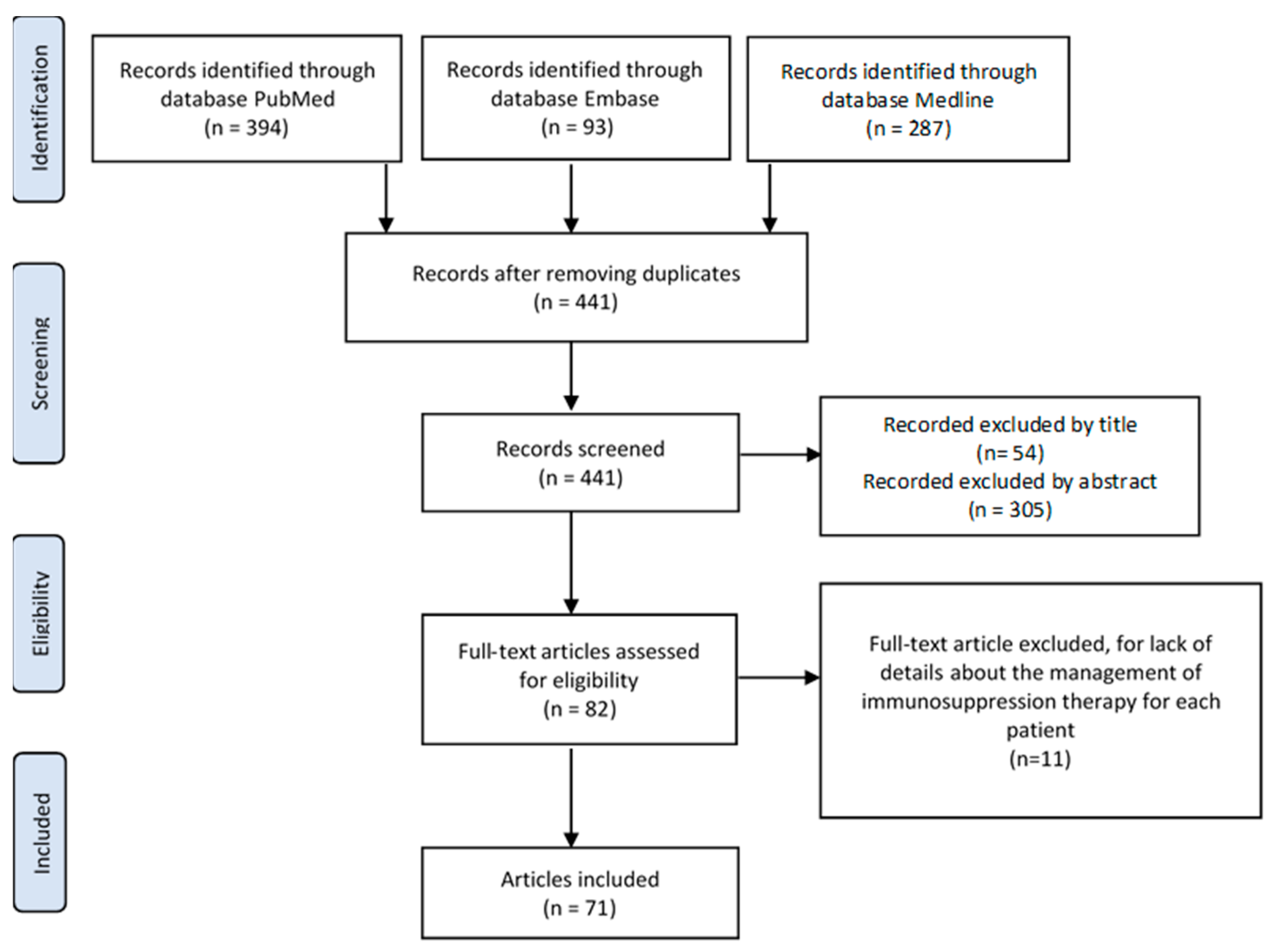
2.2. Screening Process
2.3. Study Selection and Data Extraction
2.4. Study Quality Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Wolfe, R.A.; Roys, E.C.; Merion, R.M. Trends in Organ Donation and Transplantation in the United States, 1999–2008. Am. J. Transplant. 2010, 10 Pt 2, 961–972. [Google Scholar] [CrossRef]
- Favi, E.; Salerno, M.; Romagnoli, J.; Castagneto, M.; Citterio, F. Significant Improvement in Patient Survival After Renal Transplantation in the Last Decade. Transplant. Proc. 2011, 43, 285–287. [Google Scholar] [CrossRef] [PubMed]
- Howard, R.J.; Patton, P.R.; Reed, A.I.; Hemming, A.W.; Van Der Werf, W.J.; Pfaff, W.W.; Srinivas, T.R.; Scornik, J.C. The changing causes of graft loss and death after kidney transplantation. Transplantation 2002, 73, 1923–1928. [Google Scholar] [CrossRef] [PubMed]
- Pruthi, R.; Steenkamp, R.; Feest, T. UK Renal Registry 16th Annual Report: Chapter 8 Survival and Cause of Death of UK Adult Patients on Renal Replacement Therapy in 2012: National and Centre-specific Analyses. Nephron Clin. Pr. 2013, 125, 139–169. [Google Scholar] [CrossRef] [PubMed]
- Lovato, A.; De Filippis, C.; Marioni, G. Upper airway symptoms in coronavirus disease 2019 (COVID-19). Am. J. Otolaryngol. 2020, 41, 102474. [Google Scholar] [CrossRef] [PubMed]
- Monaco, A.; Manzia, T.M.; Angelico, R.; Iaria, G.; Gazia, C.; Al Alawi, Y.; Fourtounas, K.; Tisone, G.; Cacciola, R. Awareness and Impact of Non-pharmaceutical Interventions During Coronavirus Disease 2019 Pandemic in Renal Transplant Recipients. Transplant. Proc. 2020, 52, 2607–2613. [Google Scholar] [CrossRef]
- Centers for Disease Control nd Prevention. People with Underying Medical Conditions, Immunocompromides State (Weakened Immune System) from Solid Organ Transplant. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.htmn#immunocom-promised-state (accessed on 20 March 2021).
- Maggiore, U.; Abramowicz, D.; Crespo, M.; Mariat, C.; Mjoen, G.; Peruzzi, L.; Sever, M.S.; Oniscu, G.C.; Hilbrands, L.; Watschinger, B. How should I manage immunosuppression in a kidney transplant patient with COVID-19? An ERA-EDTA DESCARTES expert opinion. Nephrol. Dial. Transplant. 2020, 35, 899–904. [Google Scholar] [CrossRef]
- Kasiske, B.L.; Zeier, M.G.; Chapman, J.R.; Craig, J.C.; Ekberg, H.; Garvey, C.A.; Green, M.D.; Jha, V.; Josephson, M.A.; Kiberd, B.A.; et al. KDIGO clinical practice guideline for the care of kidney transplant recipients: A summary. Kidney Int. 2010, 77, 299–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Akdur, A.; Karakaya, E.; Soy, E.H.A.; Alshalabi, O.; Kırnap, M.; Arslan, H.; Ulubay, G.; Hekimoglu, K.; Moray, G.; Haberal, M. Coronavirus Disease (COVID-19) in Kidney and Liver Transplant Patients: A Single-Center Experience. Exp. Clin. Transplant. 2020, 18, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Allam, S.R.; Dao, A.; Madhrira, M.M.; Antiporta, P.B.; Nair, R.R.; Guiteau, J.J.; Reyad, A.I. Interleukin-6 receptor antagonist therapy to treat SARS-CoV-2 driven inflammatory syndrome in a kidney transplant recipient. Transpl. Infect. Dis. 2020, 22, e13326. [Google Scholar] [CrossRef]
- Bartiromo, M.; Borchi, B.; Botta, A.; Bagalà, A.; Lugli, G.; Tilli, M.; Cavallo, A.; Xhaferi, B.; Cutruzzulà, R.; Vaglio, A.; et al. Threatening drug-drug interaction in a kidney transplant patient with coronavirus disease 2019 (COVID-19). Transpl. Infect. Dis. 2020, 22, e13286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Billah, M.; Santeusanio, A.; Delaney, V.; Cravedi, P.; Farouk, S.S. A catabolic state in a kidney transplant recipient with COVID-19. Transpl. Int. 2020, 33, 1140–1141. [Google Scholar] [CrossRef] [PubMed]
- Bussalino, E.; De Maria, A.; Russo, R.; Paoletti, E. Immunosuppressive therapy maintenance in a kidney transplant recipient with SARS-CoV-2 pneumonia: A case report. Am. J. Transplant. 2020, 20, 1922–1924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.; Yin, Q.; Shi, H.; Du, D.; Chang, S.; Ni, L.; Qiu, H.; Chen, Z.; Zhang, J.; Zhang, W. A familial cluster, including a kidney transplant recipient, of Coronavirus Disease 2019 (COVID-19) in Wuhan, China. Am. J. Transplant. 2020, 20, 1869–1874. [Google Scholar] [CrossRef] [PubMed]
- Cheng, D.; Wen, J.; Liu, Z.; Lv, T.; Chen, J. Coronavirus disease 2019 in renal transplant recipients: Report of two cases. Transpl. Infect. Dis. 2020, 22, e13329. [Google Scholar] [CrossRef]
- Chenna, A.; Konala, V.M.; Gayam, V.; Naramala, S.; Adapa, S. Coronavirus Disease 2019 (COVID-19) in a Renal Transplant Patient. Cureus 2020, 12, e8038. [Google Scholar] [CrossRef]
- Mathiasen, V.D.; Jensen-Fangel, S.; Skov, K.; Leth, S. Uneventful case of COVID-19 in a kidney transplant recipient. BMJ Case Rep. 2020, 13, e237427. [Google Scholar] [CrossRef]
- Dirim, A.B.; Demir, E.; Ucar, A.R.; Garayeva, N.; Safak, S.; Oto, O.A.; Yazici, H.; Alibeyoglu, A.M.; Orhun, G.; Cagatay, A.A.; et al. Fatal SARS-CoV-2 infection in a renal transplant recipient. CEN Case Rep. 2020, 9, 409–412. [Google Scholar] [CrossRef]
- Fontana, F.; Alfano, G.; Mori, G.; Amurri, A.; Tei, L.; Ballestri, M.; Leonelli, M.; Facchini, F.; Damiano, F.; Magistroni, R.; et al. COVID-19 pneumonia in a kidney transplant recipient successfully treated with tocilizumab and hydroxychloroquine. Am. J. Transplant. 2020, 20, 1902–1906. [Google Scholar] [CrossRef] [Green Version]
- Gandolfini, I.; Delsante, M.; Fiaccadori, E.; Zaza, G.; Manenti, L.; Degli Antoni, A.; Peruzzi, L.; Riella, L.V.; Cravedi, P.; Maggiore, U. COVID-19 in kidney transplant recipients. Am. J. Transplant. 2020, 20, 1941–1943. [Google Scholar] [CrossRef] [PubMed]
- Guillen, E.; Pineiro, G.J.; Revuelta, I.; Rodriguez, D.; Bodro, M.; Moreno, A.; Campistol, J.M.; Diekmann, F.; Ventura-Aguiar, P. Case report of COVID-19 in a kidney transplant recipient: Does immunosuppression alter the clinical presentation? Am. J. Transplant. 2020, 20, 1875–1878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, S.H.; Smith, R.; Camilleri, B. Belatacept, kidney transplantation and COVID-19: Successful management of the first reported case within the United Kingdom. Clin. Transplant. 2020, 34, e14026. [Google Scholar] [CrossRef]
- Hsu, J.J.; Gaynor, P.; Kamath, M.; Fan, A.; Al-Saffar, F.; Cruz, D.; Nsair, A. COVID-19 in a high-risk dual heart and kidney transplant recipient. Am. J. Transplant. 2020, 20, 1911–1915. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Lin, H.; Wu, Y.; Fang, Y.; Kumar, R.; Chen, G.; Lin, S. COVID-19 in posttransplant patients—Report of 2 cases. Am. J. Transplant. 2020, 20, 1879–1881. [Google Scholar] [CrossRef]
- Jiang, J.; Miao, Y.; Zhao, Y.; Lu, X.; Zhou, P.; Zhou, X.; Chen, Z.; Du, D. Convalescent plasma therapy: Helpful treatment of COVID-19 in a kidney transplant recipient presenting with severe clinical manifestations and complex complications. Clin. Transplant. 2020, 34, e14025. [Google Scholar] [CrossRef]
- Kates, O.S.; Fisher, C.E.; Stankiewicz-Karita, H.C.; Shepherd, A.K.; Church, E.C.; Kapnadak, S.G.; Lease, E.D.; Riedo, F.X.; Rakita, R.M.; Limaye, A.P. Earliest cases of coronavirus disease 2019 (COVID-19) identified in solid organ transplant recipients in the United States. Am. J. Transplant. 2020, 20, 1885–1890. [Google Scholar] [CrossRef]
- Kemmner, S.; Guba, M.O.; Schönermarck, U.; Stangl, M.; Fischereder, M. Cyclosporine as a preferred calcineurin inhibitor in renal allograft recipients with COVID-19 infection. Kidney Int. 2020, 98, 507–508. [Google Scholar] [CrossRef]
- Kim, Y.; Kwon, O.; Paek, J.H.; Park, W.Y.; Jin, K.; Hyun, M.; Lee, J.Y.; Kim, H.A.; Han, S. Two distinct cases with COVID-19 in kidney transplant recipients. Am. J. Transplant. 2020, 20, 2269–2275. [Google Scholar] [CrossRef]
- Kocak, B.; Arpali, E.; Akyollu, B.; Yelken, B.; Tekin, S.; Kanbay, M.; Turkmen, A.; Kalayoglu, M. Oligosymptomatic Kidney Transplant Patients With COVID-19: Do They Pose a Risk to Other Recipients? Transplant. Proc. 2020, 52, 2663–2666. [Google Scholar] [CrossRef]
- Kolonko, A.; Dudzicz, S.; Wiecek, A.; Król, R. COVID-19 infection in solid organ transplant recipients: A single-center experience with patients immediately after transplantation. Transpl. Infect. Dis. 2021, 23, e13381. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.N.; Tanna, S.D.; Shetty, A.A.; Stosor, V. COVID-19 in an HIV-positive kidney transplant recipient. Transpl. Infect. Dis. 2020, 22, e13338. [Google Scholar] [CrossRef]
- Lauterio, A.; Valsecchi, M.; Santambrogio, S.; De Carlis, R.; Merli, M.; Calini, A.; Centonze, L.; Buscemi, V.; Bottiroli, M.; Puoti, M.; et al. Successful recovery from severe COVID-19 pneumonia after kidney transplantation: The interplay between immunosuppression and novel therapy including tocilizumab. Transpl. Infect. Dis. 2020, 22, e13334. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Cheng, Q.; Zhao, Z.; Dai, N.; Zeng, L.; Zhu, L.; Guo, W.; Li, C.; Wang, J.; Li, S.; et al. Novel coronavirus infection and acute kidney injury in two renal transplant recipients: A case report. J. Int. Med. Res. 2020, 48, 300060520964009. [Google Scholar] [CrossRef]
- Ma, B.M.; Hung, I.F.N.; Chan, G.C.W.; Tam, A.R.; Chan, S.S.K.; Wong, B.C.K.; Fukuda, K.; Ohno, T.; Yuen, K.Y.; Chan, T.M. Case of “relapsing” COVID-19 in a kidney transplant recipient. Nephrology 2020, 25, 933–936. [Google Scholar] [CrossRef] [PubMed]
- Machado, D.J.D.B.; Ianhez, L.E. COVID-19 pneumonia in kidney transplant recipients—Where we are? Transpl. Infect. Dis. 2020, 22, e13306. [Google Scholar] [CrossRef]
- Man, Z.; Jing, Z.; Huibo, S.; Bin, L.; Fanjun, Z. Viral shedding prolongation in a kidney transplant patient with COVID-19 pneumonia. Am. J. Transplant. 2020, 20, 2626–2627. [Google Scholar] [CrossRef]
- Marx, D.; Moulin, B.; Fafi-Kremer, S.; Benotmane, I.; Gautier, G.; Perrin, P.; Caillard, S. First case of COVID-19 in a kidney transplant recipient treated with belatacept. Am. J. Transplant. 2020, 20, 1944–1946. [Google Scholar] [CrossRef]
- Meziyerh, S.; Zwart, T.C.; Van Etten, R.W.; Janson, J.A.; Van Gelder, T.; Alwayn, I.P.J.; De Fijter, J.W.; Reinders, M.E.J.; Moes, D.J.A.R.; De Vries, A.P. Severe COVID-19 in a renal transplant recipient: A focus on pharmacokinetics. Am. J. Transplant. 2020, 20, 1896–1901. [Google Scholar] [CrossRef]
- Namazee, N.; Mahmoudi, H.; Afzal, P.; Ghaffari, S. Novel coronavirus 2019 pneumonia in a kidney transplant recipient. Am. J. Transplant. 2020, 20, 2599–2601. [Google Scholar] [CrossRef]
- Ning, L.; Liu, L.; Li, W.; Liu, H.; Wang, J.; Yao, Z.; Zhang, S.; Zhao, D.; Nashan, B.; Shen, A.; et al. Novel coronavirus (SARS-CoV-2) infection in a renal transplant recipient: Case report. Am. J. Transplant. 2020, 20, 1864–1868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakulkonkij, P.; Bruminhent, J.; Pankongngam, C.; Chalermphunchai, N. A family cluster of diagnosed coronavirus disease 2019 (COVID-19) kidney transplant recipient in Thailand. Immun. Inflamm. Dis. 2020, 8, 534–543. [Google Scholar] [CrossRef] [PubMed]
- Seminari, E.; Colaneri, M.; Sambo, M.; Gallazzi, I.; Di Matteo, A.; Roda, S.; Bruno, R.; the COVID19 IRCCS San Matteo Pavia Task Force. SARS Cov-2 infection in a renal-transplanted patient: A case report. Am. J. Transplant. 2020, 20, 1882–1884. [Google Scholar] [CrossRef] [PubMed]
- Shingare, A.; Bahadur, M.M.; Raina, S. COVID-19 in recent kidney transplant recipients. Am. J. Transplant. 2020, 20, 3206–3209. [Google Scholar] [CrossRef] [PubMed]
- Antony, S.J.; Singh, J.; De Jesus, M.; Lance, J. Early use of tocilizumab in respiratory failure associated with acute COVID -19 pneumonia in recipients with solid organ transplantation. IDCases 2020, 21, e00888. [Google Scholar] [CrossRef]
- Suwanwongse, K.; Shabarek, N. Fatal Outcome in a Kidney-Pancreas Transplant Recipient With COVID-19. Cureus 2020, 12, e8691. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, R.; Kakuta, Y.; Tsutahara, K.; Nakagawa, M.; Ichimaru, N.; Sakaguchi, K.; Kato, T.; Imamura, R.; Nonomura, N.; Takao, T. Successful recovery from coronavirus disease 2019 in a living kidney transplant recipient using low-dose methylprednisolone. IJU Case Rep. 2021, 4, 22–24. [Google Scholar] [CrossRef]
- Tantisattamo, E.; Reddy, U.G.; Duong, D.K.; Ferrey, A.J.; Ichii, H.; Dafoe, D.C.; Kalantar-Zadeh, K. Hyponatremia: A possible immuno-neuroendocrine interface with COVID-19 in a kidney transplant recipient. Transpl. Infect. Dis. 2020, 22, e13355. [Google Scholar] [CrossRef]
- Thammathiwat, T.; Tungsanga, S.; Tiankanon, K.; Torvorapanit, P.; Chumpangern, W.; Udomkarnjananun, S.; Avihingsanon, Y.; Sriprasart, T.; Srisawat, N.; Jutivorakool, K.; et al. A case of successful treatment of severe COVID-19 pneumonia with favipiravir and tocilizumab in post–kidney transplant recipient. Transpl. Infect. Dis. 2021, 23, e13388. [Google Scholar] [CrossRef] [PubMed]
- Tzukert, K.; Abel, R.; Levi, I.M.Y.; Gork, I.; Orpaz, L.Y.; Azmanov, H.; Elhalel, M.D. The Challenge of Treating Kidney Transplant Recipients Infected with COVID-19: Report of the First Cases in Israel. Isr. Med. Assoc. J. 2020, 22, 602–604. [Google Scholar] [PubMed]
- Velioglu, A.; Tuglular, S. Care of asymptomatic SARS-CoV-2 positive kidney transplant recipients. Transpl. Int. 2020, 33, 1331–1332. [Google Scholar] [CrossRef]
- Wang, J.; Li, X.; Cao, G.; Wu, X.; Wang, Z.; Yan, T. COVID-19 in a Kidney Transplant Patient. Eur. Urol. 2020, 77, 769–770. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.X.; Cardona, O.Q.; Ho, D.Y.; Busque, S.; Lenihan, C.R. Influence of immunosuppression on seroconversion against SARS-CoV-2 in two kidney transplant recipients. Transpl. Infect. Dis. 2021, 23, e13423. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.J.; Samaha, D.; Mondhe, S.; Massicotte-Azarniouch, D.; Knoll, G.; Ruzicka, M. Renal infarct in a COVID-19–positive kidney–pancreas transplant recipient. Am. J. Transplant. 2020, 20, 3221–3224. [Google Scholar] [CrossRef]
- Zhong, Z.; Zhang, Q.; Xia, H.; Wang, A.; Liang, W.; Zhou, W.; Zhou, L.; Liu, X.; Rao, L.; Li, Z.; et al. Clinical characteristics and immunosuppressant management of coronavirus disease 2019 in solid organ transplant recipients. Am. J. Transplant. 2020, 20, 1916–1921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, L.; Shu, H.; Li, H.; Qiu, T.; Zhou, J.; Chen, G. Slow Recovery from Critical Coronavirus Disease 2019 Pneumonia in an Immunosuppressed Renal Transplant Recipient with Early Acute Cardiorenal Syndrome. Cardiorenal Med. 2020, 10, 470–475. [Google Scholar] [CrossRef]
- Zhu, L.; Xu, X.; Ma, K.; Yang, J.; Guan, H.; Chen, S.; Chen, Z.; Chen, G. Successful recovery of COVID-19 pneumonia in a renal transplant recipient with long-term immunosuppression. Am. J. Transplant. 2020, 20, 1859–1863. [Google Scholar] [CrossRef] [Green Version]
- Akalin, E.; Azzi, Y.; Bartash, R.; Seethamraju, H.; Parides, M.; Hemmige, V.; Ross, M.; Forest, S.; Goldstein, Y.D.; Ajaimy, M.; et al. Covid-19 and Kidney Transplantation. N. Engl. J. Med. 2020, 382, 2475–2477. [Google Scholar] [CrossRef] [PubMed]
- Alberici, F.; Delbarba, E.; Manenti, C.; Econimo, L.; Valerio, F.; Pola, A.; Maffei, C.; Possenti, S.; Zambetti, N.; Moscato, M.; et al. A single center observational study of the clinical characteristics and short-term outcome of 20 kidney transplant patients admitted for SARS-CoV2 pneumonia. Kidney Int. 2020, 97, 1083–1088. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, D.; Popoola, J.; Shah, S.; Ster, I.C.; Quan, V.; Phanish, M. COVID-19 infection in kidney transplant recipients. Kidney Int. 2020, 97, 1076–1082. [Google Scholar] [CrossRef] [PubMed]
- Bösch, F.; Börner, N.; Kemmner, S.; Lampert, C.; Jacob, S.; Koliogiannis, D.; Stangl, M.; Michel, S.; Kneidinger, N.; Schneider, C.; et al. Attenuated early inflammatory response in solid organ recipients with COVID-19. Clin. Transplant. 2020, 34, e14027. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.Y.; Farghaly, S.; Cham, S.; Tatem, L.L.; Sin, J.H.; Rauda, R.; Ribisi, M.; Sumrani, N. COVID-19 pneumonia in kidney transplant recipients: Focus on immunosuppression management. Transpl. Infect. Dis. 2020, 22, e13378. [Google Scholar] [CrossRef] [PubMed]
- The Columbia University Kidney Transplant Program. Early Description of Coronavirus 2019 Disease in Kidney Transplant Recipients in New York. J. Am. Soc. Nephrol. 2020, 31, 1150–1156. [Google Scholar] [CrossRef] [PubMed]
- Crespo, M.; Pérez-Sáez, M.J.; Redondo-Pachón, D.; Llinàs-Mallol, L.; Montero, M.M.; Villar-García, J.; Arias-Cabrales, C.; Buxeda, A.; Burballa, C.; Vázquez, S.; et al. COVID-19 in elderly kidney transplant recipients. Am. J. Transplant. 2020, 20, 2883–2889. [Google Scholar] [CrossRef]
- Devresse, A.; Belkhir, L.; Vo, B.; Ghaye, B.; Scohy, A.; Kabamba, B.; Goffin, E.; De Greef, J.; Mourad, M.; De Meyer, M.; et al. COVID-19 Infection in Kidney Transplant Recipients: A Single-Center Case Series of 22 Cases From Belgium. Kidney Med. 2020, 2, 459–466. [Google Scholar] [CrossRef]
- Elias, M.; Pievani, D.; Randoux, C.; Louis, K.; Denis, B.; DeLion, A.; Le Goff, O.; Antoine, C.; Greze, C.; Pillebout, E.; et al. COVID-19 Infection in Kidney Transplant Recipients: Disease Incidence and Clinical Outcomes. J. Am. Soc. Nephrol. 2020, 31, 2413–2423. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Ruiz, M.; Andrés, A.; Loinaz, C.; Delgado, J.F.; López-Medrano, F.; Juan, R.S.; González, E.; Polanco, N.; Folgueira, M.D.; Lalueza, A.; et al. COVID-19 in solid organ transplant recipients: A single-center case series from Spain. Am. J. Transplant. 2020, 20, 1849–1858. [Google Scholar] [CrossRef]
- Fung, M.; Chiu, C.Y.; DeVoe, C.; Doernberg, S.B.; Schwartz, B.S.; Langelier, C.; Henrich, T.J.; Yokoe, D.; Davis, J.; Hays, S.R.; et al. Clinical outcomes and serologic response in solid organ transplant recipients with COVID-19: A case series from the United States. Am. J. Transplant. 2020, 20, 3225–3233. [Google Scholar] [CrossRef]
- Hartzell, S.; Bin, S.; Benedetti, C.; Haverly, M.; Gallon, L.; Zaza, G.; Riella, L.V.; Menon, M.C.; Florman, S.; Rahman, A.H.; et al. Evidence of potent humoral immune activity in COVID-19-infected kidney transplant recipients. Am. J. Transplant. 2020, 20, 16261. [Google Scholar] [CrossRef] [PubMed]
- Lubetzky, M.; Aull, M.J.; Craig-Schapiro, R.; Lee, J.R.; Marku-Podvorica, J.; Salinas, T.; Gingras, L.; Lee, J.B.; Sultan, S.; Kodiyanplakkal, R.P.; et al. Kidney allograft recipients, immunosuppression, and coronavirus disease-2019: A report of consecutive cases from a New York City transplant center. Nephrol. Dial. Transplant. 2020, 35, 1250–1261. [Google Scholar] [CrossRef] [PubMed]
- Maritati, F.; Cerutti, E.; Zuccatosta, L.; Fiorentini, A.; Finale, C.; Ficosecco, M.; Cristiano, F.; Capestro, A.; Balestra, E.; Taruscia, D.; et al. SARS-CoV-2 infection in kidney transplant recipients: Experience of the italian marche region. Transpl. Infect. Dis. 2020, 22, e13377. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.A.; Leonard, J.; Labella, P.; Cartiera, K.; Soomro, I.; Neumann, H.; Montgomery, R.A.; Ali, N.M. Outpatient management of kidney transplant recipients with suspected COVID-19—Single-center experience during the New York City surge. Transpl. Infect. Dis. 2020, 22, e13383. [Google Scholar] [CrossRef] [PubMed]
- Mella, A.; Mingozzi, S.; Gallo, E.; Lavacca, A.; Rossetti, M.; Clari, R.; Randone, O.; Maffei, S.; Salomone, M.; Imperiale, D.; et al. Case series of six kidney transplanted patients with COVID-19 pneumonia treated with tocilizumab. Transpl. Infect. Dis. 2020, 22, 13348. [Google Scholar] [CrossRef] [PubMed]
- Monfared, A.; Dashti-Khavidaki, S.; Jafari, R.; Jafari, A.; Ramezanzade, E.; Lebadi, M.; Haghdar-Saheli, Y.; Aghajanzadeh, P.; Khosravi, M.; Movassaghi, A.; et al. Clinical characteristics and outcome of COVID-19 pneumonia in kidney transplant recipients in Razi hospital, Rasht, Iran. Transpl. Infect. Dis. 2020, 22, e13420. [Google Scholar] [CrossRef]
- Nair, V.; Jandovitz, N.; Hirsch, J.S.; Nair, G.; Abate, M.; Bhaskaran, M.; Grodstein, E.; Berlinrut, I.; Hirschwerk, D.; Cohen, S.L.; et al. COVID-19 in kidney transplant recipients. Am. J. Transplant. 2020, 20, 1819–1825. [Google Scholar] [CrossRef]
- Pierrotti, L.C.; Reusing, J.O., Jr.; Freire, M.P.; Machado, D.J.B.; Moreira, R.M.; Ventura, C.G.; Litvoc, M.N.; Nahas, W.C.; David-Neto, E. COVID-19 among kidney-transplant recipients requiring hospitalization: Preliminary data and outcomes from a single-center in Brazil. Transpl. Int. 2020, 33, 1837–1842. [Google Scholar] [CrossRef]
- Rodriguez-Cubillo, B.; De La Higuera, M.A.M.; Lucena, R.; Franci, E.V.; Hurtado, M.; Romero, N.C.; Moreno, A.R.; Valencia, D.; Velo, M.; Fornie, I.S.; et al. Should cyclosporine be useful in renal transplant recipients affected by SARS-CoV-2? Am. J. Transplant. 2020, 20, 3173–3181. [Google Scholar] [CrossRef]
- Silva, F.; Cipriano, A.; Cruz, H.; Tavares, J.; Fragoso, J.; Malheiro, J.; Almeida, M.; Martins, L.S.; Abreu, M.; Pedroso, S.; et al. SARS-CoV-2 infection in kidney transplant recipients: Early report of five cases. Transpl. Infect. Dis. 2021, 23, e13394. [Google Scholar] [CrossRef]
- Trujillo, H.; Caravaca-Fontán, F.; Sevillano, Á.; Gutiérrez, E.; Caro, J.; Gutiérrez, E.; Yuste, C.; Andrés, A.; Praga, M. SARS-CoV-2 Infection in Hospitalized Patients with Kidney Disease. Kidney Int. Rep. 2020, 5, 905–909. [Google Scholar] [CrossRef]
- Zhu, L.; Gong, N.; Liu, B.; Lu, X.; Chen, D.; Chen, S.; Shu, H.; Ma, K.; Xu, X.; Guo, Z.; et al. Coronavirus Disease 2019 Pneumonia in Immunosuppressed Renal Transplant Recipients: A Summary of 10 Confirmed Cases in Wuhan, China. Eur. Urol. 2020, 78, e158. [Google Scholar] [CrossRef]
- Deeks, J.J.; Dinnes, J.; D’Amico, R.; Sowden, A.J.; Sakarovitch, C.; Song, F.; Petticrew, M.; Altman, D.G. Evaluating non-randomised intervention studies. Health Technol. Assess. 2003, 7. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-directorgeneral-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 20 March 2021).
- Hilbrands, L.B.; Duivenvoorden, R.; Vart, P.; Franssen, C.F.M.; Hemmelder, M.H.; Jager, K.J.; Kieneker, L.M.; Noordzij, M.; Pena, M.J.; de Vries, H.; et al. COVID-19-related mortality in kidney transplant and dialysis patients: Results of the ERACODA collaboration. Nephrol. Dial. Transplant. 2020, 35, 1973–1983. [Google Scholar] [CrossRef] [PubMed]
- ERA EDTA Registry. 22 June 2020. Available online: https://www.era-edta.org/en/registry/projects-and-collaborations/covid-19/ (accessed on 20 March 2021).
- Tu, G.; Ju, M.; Zheng, Y.; Xu, M.; Rong, R.; Zhu, D.; Zhu, T.; Luo, Z. Early- and late-onset severe pneumonia after renal transplantation. J. Clin. Exp. Med. 2015, 8, 1324–1332. [Google Scholar]
- Gagliardi, I.; Patella, G.; Michael, A.; Serra, R.; Provenzano, M.; Andreucci, M. COVID-19 and the Kidney: From Epidemiology to Clinical Practice. J. Clin. Med. 2020, 9, 2506. [Google Scholar] [CrossRef] [PubMed]
- Molaei, H.; Khedmat, L.; Nemati, E.; Rostami, Z.; Saadat, S.H. Iranian kidney transplant recipients with COVID-19 infection: Clinical outcomes and cytomegalovirus coinfection. Transpl. Infect. Dis. 2021, 23, 13455. [Google Scholar] [CrossRef]
- Liu, J.; Li, S.; Liu, J.; Liang, B.; Wang, X.; Wang, H.; Li, W.; Tong, Q.; Yi, J.; Zhao, L.; et al. Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients. EBioMedicine 2020, 55, 102763. [Google Scholar] [CrossRef] [PubMed]
- Hu, Q.; Zhong, Z.; Xiong, Y.; Ye, S.; Wang, Y.; Ye, Q. Management of immunosuppression in kidney transplant recipients with COVID-19 pneumonia: A summary of 41 confirmed cases reported worldwide. Transpl. Infect. Dis. 2021, 23, e13425. [Google Scholar] [CrossRef]
- American Association for the Study of Liver Diseases. Clinical Insights for Hepatology and Liver Transplant Providers During the COVID-19 Pandemic. 23 March 2020. Available online: https://www.aasld.org/sites/default/files/2020-11/AASLD-COVID19ExpertPanelConsensusStatement-November092020.pdf (accessed on 20 March 2021).
- Ma-Lauer, Y.; Zheng, Y.; Malešević, M.; Von Brunn, B.; Fischer, G.; Von Brunn, A. Influences of cyclosporin A and non-immunosuppressive derivatives on cellular cyclophilins and viral nucleocapsid protein during human coronavirus 229E replication. Antivir. Res. 2020, 173, 104620. [Google Scholar] [CrossRef]
- Cavagna, L.; Seminari, E.; Zanframundo, G.; Gregorini, M.; Di Matteo, A.; Rampino, T.; Montecucco, C.; Pelenghi, S.; Cattadori, B.; Pattonieri, E.F.; et al. Calcineurin Inhibitor-Based Immunosuppression and COVID-19: Results from a Multidisciplinary Cohort of Patients in Northern Italy. Microorganisms 2020, 8, 977. [Google Scholar] [CrossRef]
- Shen, L.; Niu, J.; Wang, C.; Huang, B.; Wang, W.; Zhu, N.; Deng, Y.; Wang, H.; Ye, F.; Cen, S.; et al. High-Throughput Screening and Identification of Potent Broad-Spectrum Inhibitors of Coronaviruses. J. Virol. 2019, 93, 00023-19. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef] [PubMed]
- Kindrachuk, J.; Ork, B.; Hart, B.J.; Mazur, S.; Holbrook, M.R.; Frieman, M.B.; Traynor, D.; Johnson, R.F.; Dyall, J.; Kuhn, J.H.; et al. Antiviral Potential of ERK/MAPK and PI3K/AKT/mTOR Signaling Modulation for Middle East Respiratory Syndrome Coronavirus Infection as Identified by Temporal Kinome Analysis. Antimicrob. Agents Chemother. 2015, 59, 1088–1099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, N.; Hayano, T.; Suzuki, M. Peptidyl-prolyl cis-trans isomerase is the cyclosporin A-binding protein cyclophilin. Nat. Cell Biol. 1989, 337, 473–475. [Google Scholar] [CrossRef] [PubMed]
- Harding, M.W.; Galat, A.; Uehling, D.E.; Schreiber, S.L. A receptor for the immunosuppressant FK506 is a cis-trans peptidyl-prolyl isomerase. Nature 1989, 337, 473–475. [Google Scholar] [CrossRef]
- Flanagan, W.M.; Corthésy, B.; Bram, R.J.; Crabtree, G.R. Nuclear association of a T-cell transcription factor blocked by FK-506 and cyclosporin A. Nat. Cell Biol. 1991, 352, 803–807. [Google Scholar] [CrossRef]
- De Wilde, A.H.; Zevenhoven-Dobbe, J.C.; Van Der Meer, Y.; Thiel, V.; Narayanan, K.; Makino, S.; Snijder, E.J.; Van Hemert, M.J. Cyclosporin A inhibits the replication of diverse coronaviruses. J. Gen. Virol. 2011, 92, 2542–2548. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Mirjalili, M.; Shafiekhani, M.; Vazin, A. Coronavirus Disease 2019 (COVID-19) and Transplantation: Pharmacotherapeutic Management of Immunosuppression Regimen. Ther. Clin. Risk Manag. 2020, 16, 617–629. [Google Scholar] [CrossRef]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. N. Engl. J. Med. 2020, nejmoa2021436. [Google Scholar] [CrossRef]
- Chihrin, S.; Loutfy, M.R. Overview of antiviral and anti-inflammatory treatment for severe acute respiratory syndrome. Expert Rev. Anti-Infect. Ther. 2005, 3, 251–262. [Google Scholar] [CrossRef] [Green Version]
- Russell, B.; Moss, C.; George, G.; Santaolalla, A.; Cope, A.; Papa, S.; Van Hemelrijck, M. Associations between immune-suppressive and stimulating drugs and novel COVID-19—a systematic review of current evidence. Ecancermedicalscience 2020, 14, 1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkar, S.; Khanna, P.; Soni, K.D. Are the steroids a blanket solution for COVID-19? A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 1538–1547. [Google Scholar] [CrossRef]
- Imam, A.; Tzukert, K.; Merhav, H.; Imam, R.; Abu-Gazala, S.; Abel, R.; Elhalel, M.D.; Khalaileh, A. Practical recommendations for kidney transplantation in the COVID-19 pandemic. World J. Transplant. 2020, 10, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Nashan, B. Antibody Induction Therapy in Renal Transplant Patients Receiving Calcineurin-Inhibitor Immunosuppressive Regimens. BioDrugs 2005, 19, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Akalin, E.; Sehgal, V.; Ames, S.; Hossain, S.; Daly, L.; Barbara, M.; Bromberg, J.S. Cytomegalovirus Disease in High-Risk Transplant Recipients Despite Ganciclovir or Valganciclovir Prophylaxis. Am. J. Transplant. 2003, 3, 731–735. [Google Scholar] [CrossRef]
- Mourad, G.; Garrigue, V.; Squifflet, J.P.; Besse, T.; Berthoux, F.; Alamartine, E.; Durand, D.; Rostaing, L.; Lang, P.; Baron, C.; et al. Induction versus noninduction in renal transplant recipients with tacrolimus-based immunosuppression. Transplantation 2001, 72, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Terasaki, P.I. Induction Immunosuppression Improves Long-Term Graft and Patient Outcome in Organ Transplantation: An Analysis of United Network for Organ Sharing Registry Data. Transplantation 2010, 90, 1511–1515. [Google Scholar] [CrossRef] [PubMed]
- Bamoulid, J.; Staeck, O.; Crépin, T.; Halleck, F.; Saas, P.; Brakemeier, S.; Ducloux, D.; Budde, K. Anti-thymocyte globulins in kidney transplantation: Focus on current indications and long-term immunological side effects. Nephrol. Dial. Transplant. 2016, 32, 1601–1608. [Google Scholar] [CrossRef] [PubMed]
- Hellemans, R.; Bosmans, J.; Abramowicz, D. Induction Therapy for Kidney Transplant Recipients: Do We Still Need Anti-IL2 Receptor Monoclonal Antibodies? Am. J. Transplant. 2017, 17, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Fishman, J.A. Infection in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2007, 357, 2601–2614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fishman, J.A. Infection in Organ Transplantation. Am. J. Transplant. 2017, 17, 856–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gralla, J.; Wiseman, A.C. The Impact of IL2ra Induction Therapy in Kidney Transplantation Using Tacrolimus- and Mycophenolate-Based Immunosuppression. Transplantation 2010, 90, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Webster, A.C.; Taylor, R.R.; Chapman, J.R.; Craig, J.C. Tacrolimus versus cyclosporin as primary immunosuppression for kidney transplant recipients. Cochrane Database Syst. Rev. 2005, 4, CD003961. [Google Scholar] [CrossRef] [PubMed]
- Ekberg, H.; Tedesco-Silva, H.; Demirbas, A.; Vítko, Š.; Nashan, B.; Guerkan, A.; Margreiter, R.; Hugo, C.; Grinyó, J.M.; Frei, U.; et al. Reduced Exposure to Calcineurin Inhibitors in Renal Transplantation. N. Engl. J. Med. 2007, 357, 2562–2575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Favi, E.; Gargiulo, A.; Spagnoletti, G.; Salerno, M.; Silvestrini, N.; Valente, I.; Citterio, F. Induction with Basiliximab Plus Thymoglobulin Is Effective and Safe in Old-for-Old Renal Transplantation: Six-Month Results of a Prospective Clinical Study. Transplant. Proc. 2010, 42, 1114–1117. [Google Scholar] [CrossRef]


{kind=link}
| Authors | Region/Country | N° pts | Type of Study | IS Modifications | Outcomes | HD Necessity | Graft Loss |
|---|---|---|---|---|---|---|---|
| [11] Akdur et al. | Ankara, Turkey | 1 | Case Report | Withdrawal (AD+Tac) | Alive | No | No |
| [12] Allam et al. | Fort Worth, TX, USA | 1 | Case Report | AD withdrawal, Tac reduction | Alive | No | No |
| [13] Bartiromo et al. | Florence, Italy | 1 | Case Report | Tac withdrawal | Alive | No | No |
| [14] Billah et al. | New York, NT, USA | 1 | Case Report | Tac reduction (AD stable) | Alive | Yes | Yes |
| [15] Bussalino et al. | Genova, Italy | 1 | Case Report | None (Tac+AD stable) | Alive | No | No |
| [16] Chen et al. | Wuhan, China | 1 | Case Report | Withdrawal (Tac+AD) | Alive | No | No |
| [17] Cheng et al. | Nanjiing, China | 2 | Case Report | Withdrawal (Tac+AD) | Alive | No | No |
| [18] Chenna et al. | Albany, NY, USA | 1 | Case Report | Withdrawal (Tac+AD) | Died | No | DwGF |
| [19] Dahl et al | Aarhus N, Denmark | 1 | Case Report | None (Tac stable) | Alive | No | No |
| [20] Dirim et al. | Istanbul, Turkey | 1 | Case Report | AD withdrawal, Tac reduction | Died | Yes | Yes |
| [21] Fontana et al. | Modena, Italy | 1 | Case Report | CyA withdrawal | Alive | No | No |
| [22] Gandolfini et al. | Parma, Italy | 2 | Case Report | Withdrawal (Tac+AD) | Alive (1)/ Died (1) | No | DwGF (1) No (1) |
| [23] Guillen et al. | Barcelona, Spain | 1 | Case Report | Withdrawal (Tac+mTOR) | Alive | No | No |
| [24] Hasan Ahmad et al. | Ipswich, UK | 1 | Case Report | Withdrawal (AD+BELAT) | Alive | No | No |
| [25] Hsu et al. | Los Angeles, CA, USA | 1 | Case Report | AD withdrawal, Tac stable | Alive | No | No |
| [26] Huang et al. | Fuzhou, China | 1 | Case Report | Withdrawal (AD) | Died | Yes | Yes |
| [27] Jiang et al. | Wuhan, China | 1 | Case Report | CyA Withdrawal, AD reduction | Alive | NA | NA |
| [28] Kates et al. | Seattle, WA, USA | 1 | Case Report | AD withdrawal, Tac reduction | Alive | No | No |
| [29] Kemmner et al. | Munich, Germany | 1 | Case Report | AD withdrawal, CyA introduction | Alive | No | No |
| [30] Kim et al. | Daegu, Korea | 2 | Case Report | Tac withdrawal (1)/Tac stable (1), AD withdrawal (2) | Alive | No | No |
| [31] Kocak et al. | Istanbul, Turkey | 2 | Case Report | AD withdrawal (2), Tac reduced (1)/ Tac withdrawal (1) | Alive | No | No |
| [32] Kolonko et al. | Katowice, Poland | 3 | Case Report | AD withdrawal (1)/AD reduction (2), Tac stable (2)/Tac reduction (1) | Died (1)/ Alive (2) | No | No (2) DwGF (1) |
| [33] Kumar et al. | Chicago, IL, USA | 1 | Case Report | Reduction (Tac+AD) | Alive | No | No |
| [34] Lauterio et al. | Milan, Italy | 1 | Case Report | Withdrawal (CyA+mTORi) | Alive | No | No |
| [35] Li.Q | Peking, China | 2 | Case Report | CyA withdrawal (1) Tac withdrawal (1), AD withdrawal (1) | Died (1) | No | Worsening (1) |
| [36] Ma et al. | Hong Kong | 1 | Case Report | Tac withdrawal, AD reduction | Alive | No | No |
| [37] Machado et al. | Sao Paulo, Brazil | 1 | Case Report | Withdrawal (Tac+AD) | Alive | No | No |
| [38] Man et al. | Wuhan, China | 1 | Case Report | Withdrawal (Tac+AD) | Alive | No | No |
| [39] Marx et al. | Strasbourg, France | 1 | Case Report | Withdrawal (AD+BELAC) | Alive | No | No |
| [40] Meziyerh et al. | Leiden, the Netherlands | 1 | Case Report | Withdrawal (mTORi) | Alive | No | Worsening |
| [41] Namazee et al. | Semnan, Iran | 1 | Case Report | Withdrawal (CyA+AD) | Died | No | Yes |
| [42] Ning et al. | Hefei, China | 1 | Case Report | Stable (CyA+AD) | Alive | No | No |
| [43] Sakulkonkij et al. | Lampang, Thailand | 1 | Case Report | Tac reduction, AD withdrawal | Alive | No | No |
| [44] Seminari et al. | Pavia, Italy | 1 | Case Report | Stable (Tac+AD) | Alive | No | No |
| [45] Shingare et al. | Mumbai, India | 2 | Case Report | Reduction (Tac+AD) | Alive | No | No |
| [46] Sj Antony et al. | El Paso, TX, USA | 1 | Case Report | Withdrawal (Tac+AD) | Alive | No | No |
| [47] Suwanwongse et al. | New York, NY, USA | 1 | Case Report | Tac withdrawal, AD stable | Died | Yes | Yes |
| [48] Tanaka et al | Osaka, Japan | 1 | Case Report | Tac stable, AD withdrawal, mTORi withdrawal | Alive | No | No |
| [49] Tantisattamo et al. | Orange, CA, USA | 1 | Case Report | AD withdrawal, Tac stable | Alive | No | No |
| [50] Thammathiwat et al. | Bangkok, Thailand | 1 | Case Report | Withdrawal (Tac+AD) | Alive | No | No |
| [51] Tzukert T. et al. | Jerusalem, Israel | 2 | Case Report | Tac stable (2), AD withdrawal (1)/AD stable (1) | Alive | No | No |
| [52] Velioglu et al. | Istanbul, Turkey | 1 | Case Report | AD withdrawal, Tac stable | Alive | No | No |
| [53] Wang et al. | Zhengzhou, China | 1 | Case Report | Stable (CyA+AD) | Alive | No | No |
| [54] Wang et al. | Stanford, CA, USA | 2 | Case Report | Tac stable (2), AD withdrawal (2) | Alive | No | No |
| [55] Xu et al. | Ottawa, Canada | 1 | Case Report | Tac withdrawal, AD stable | Alive | No | No |
| [56] Zhong et al. | Wuhan, China | 1 | Case Report | Reduction (Tac+AD) | Alive | No | No |
| [57] Zhu et al. | Wuhan, China | 1 | Case Report | Tac reduction, AD withdrawal | Alive | No | No |
| [58] Zhu et al. | Wuhan, China | 1 | Case Report | Tac withdrawal, AD withdrawal | Alive | No | No |
| Authors | Region/Country | N° pts | Type of Study | IS Modifications | Mortality Rate (%) | HD Necessity (%) | Graft Loss (%) | DwFG (%) |
|---|---|---|---|---|---|---|---|---|
| [59] Akalin et al. | Bronx, NY, USA | 36 | Case series | AD withdrawal (24)/stable (7), Tac withdrawal (6)/stable (29) | 27.7% | NA | NA | NA |
| [60] Alberici et al. | Brescia, Italy | 20 | Case series | IS Withdrawal [Tac (19), AD (14), mTOR (2)] | 25% | 5% | 25% | 20% |
| [61] Banerjee et al. | London, UK. | 7 | Case series | AD withdrawal (5)/stable (2), Tac stable (4)/reduction (1)/withdrawal (1) | 14.3% | 42.9% | 42.9% | – |
| [62] Bosch et al. | Munich, Germany | 3 | Case series | AD withdrawal (3), Tac withdrawal (1), Cya started (2) | 33.3% | 33.3% | 33.3% | – |
| [63] Chen et al. | Brooklyn, NY, USA | 30 | Case series | AD Withdrawal (12), Tac withdrawal (26), CyA withdrawal (3) | 20% | 13.3% | 20% | 6.7% |
| [64] Columbia University | New York, NY, USA | 15 | Case series | AD withdrawal (12), Tac stable (11)/reduction (2)/withdrawal (1) | 6.7% | 13.3% | 13.3% | – |
| [65] Crespo et al. | Barcelona, Spain | 16 | Case series | AD withdrawal (8), mTORi withdrawal (4)/stable (1), Tac withdrawal (8)/stable (6) | 50% | 18.8% | 18.8% | – |
| [66] Devresse et al. | Brussels, Belgium | 22 | Case series | AD withdrawal (18)/stable (1), Tac reduction (9)/stable (1), CyA withdrawal (2)/stable (3), mTORi withdrawal (1)/reduction (2) | 9.1% | – | 9.1% | 9.1% |
| [67] Elias et al. | Paris, France | 66 | Prospective study | AD withdrawal (39)/stable (22), Tac withdrawal (3)/stable (54), BELAT postponed (1)/regular (5) | 24.2% | 10.6% | 24.2% | 13.6% |
| [68] Fernandez-Riuz et al. | Madrid, Spain | 8 | Case series | AD withdrawal (5)/reduction (1), Tac reduction (6)/stable (1), mTORi withdrawal (1) | 25% | NA | NA | NA |
| [69] Fung et al. | San Francisco, CA, USA | 7 | Case series | AD reduction (1), Tac reduction (2) | 0% | 14.3% | – | – |
| [70] Hartzell et al. | New York, NY, USA | 18 | Case series | AD withdrawal (5)/reduction (13), Tac withdrawal (1)/stable (17) | 38.9% | – | 38.9% | 38.9% |
| [71] Lubetzky et al. | New York, NY, USA | 54 | Case series | AD withdrawal (24)/reduction (15), Tac reduction (17)/stable (35) | 12.96% | 7.4% | 5.55% | NA |
| [72] Maritati et al. | Ancona, Italy | 5 | Case series | AD withdrawal (4), Tac withdrawal (5), mTORi withdrawal (1) | 40% | 20% | 40% | 20% |
| [73] Mehta et al. | New York, NY, USA | 34 | Case series | AD withdrawal (26)/reduction (6)/stable (1), Tac stable (29), Cya stable (1), mTOR stable (1) | 17.6% | – | 17.6% | 17.6% |
| [74] Mella et al. | Turin, Italy | 6 | Case series | AD withdrawal (3), Tac withdrawal (6) | 66.7% | 33.3% | 66.7% | 33.3% |
| [75] Monfaret et al. | Rasht Iran | 22 | Case Series | CNI withdrawal (5)/reduction (13)/stable (3), AD withdrawal (21)/stable (1), mTOR withdrawal (1) | 27.3% | NA | NA | NA |
| [76] Nair et al. | New York, USA | 10 | Case Series | Tac stable (7)/withdrawal (2), AD stable (1)/withdrawal (8), mTORi stable (1)/withdrawal (19) | 30% | 10% | 30% | 20% |
| [77] Pierotti et al. | Sao Paulo, Brazil | 51 | Case series | Tac reduction (32)/withdrawal (12), AD withdrawal (32)/stable (14), mTORi withdrawal (4), CyA withdrawal (7) | 25.5% | 25.5% | 25.5% | – |
| [78] Rodriguez-Cubillo et al. | Madrid, Spain | 29 | Case series | AD withdrawal (22), Tac reduction (1)/withdrawal (15), CyA start (23)/stable (6) | 20.7% | 10.3% | 20.7% | 10.3% |
| [79] Silva et al. | Porto, Portugal | 5 | Case series | AD withdrawal (5), Tac reduction (3)/stable (1), Cya withdrawal (1) | 20% | – | 20% | 20% |
| [80] Trujillo et al. | Madrid, Spain | 26 | Case series | AD withdrawal (13)/stable (1), Tac withdrawal (4)/stable (20), mTORi withdrawal (2)/stable (5) | 23.1% | – | 23.1% | 23.1% |
| [81] Zhu et al. | Wuhan, China | 10 | Case–control study | AD withdrawal (9)/stable (1), Tac withdrawal (7)/reduction (1)/stable (2) | 10% | – | – | Worsening of graft function (10%) |
| Type of IS Drugs | Total | Withdrawal | Reduction | No Modification |
|---|---|---|---|---|
| CNI: | 502 | 160 (31.9%) | 99 (19.7%) | 243 (48.4%) |
| -Tac | 453 | 138 (30.5%) | 86 (19.0%) | 229 (50.6%) |
| -Cya | 28 | 17 (60.7%) | 0 (0%) | 11 (39.3%) |
| -not specified | 21 | 5 (23.8%) | 13 (61.9%) | 3 (14.3%) |
| ADs | 461 | 347 (75.3%) | 44 (9.5%) | 70 (15.2%) |
| mTOR inhibitors | 48 | 38 (79.2%) | 2 (4.1%) | 8 (16.6%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angelico, R.; Blasi, F.; Manzia, T.M.; Toti, L.; Tisone, G.; Cacciola, R. The Management of Immunosuppression in Kidney Transplant Recipients with COVID-19 Disease: An Update and Systematic Review of the Literature. Medicina 2021, 57, 435. https://doi.org/10.3390/medicina57050435
Angelico R, Blasi F, Manzia TM, Toti L, Tisone G, Cacciola R. The Management of Immunosuppression in Kidney Transplant Recipients with COVID-19 Disease: An Update and Systematic Review of the Literature. Medicina. 2021; 57(5):435. https://doi.org/10.3390/medicina57050435
Chicago/Turabian StyleAngelico, Roberta, Francesca Blasi, Tommaso Maria Manzia, Luca Toti, Giuseppe Tisone, and Roberto Cacciola. 2021. "The Management of Immunosuppression in Kidney Transplant Recipients with COVID-19 Disease: An Update and Systematic Review of the Literature" Medicina 57, no. 5: 435. https://doi.org/10.3390/medicina57050435