
Bone Marrow Aspirate Concentrate versus Platelet Rich Plasma or Hyaluronic Acid for the Treatment of Knee Osteoarthritis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
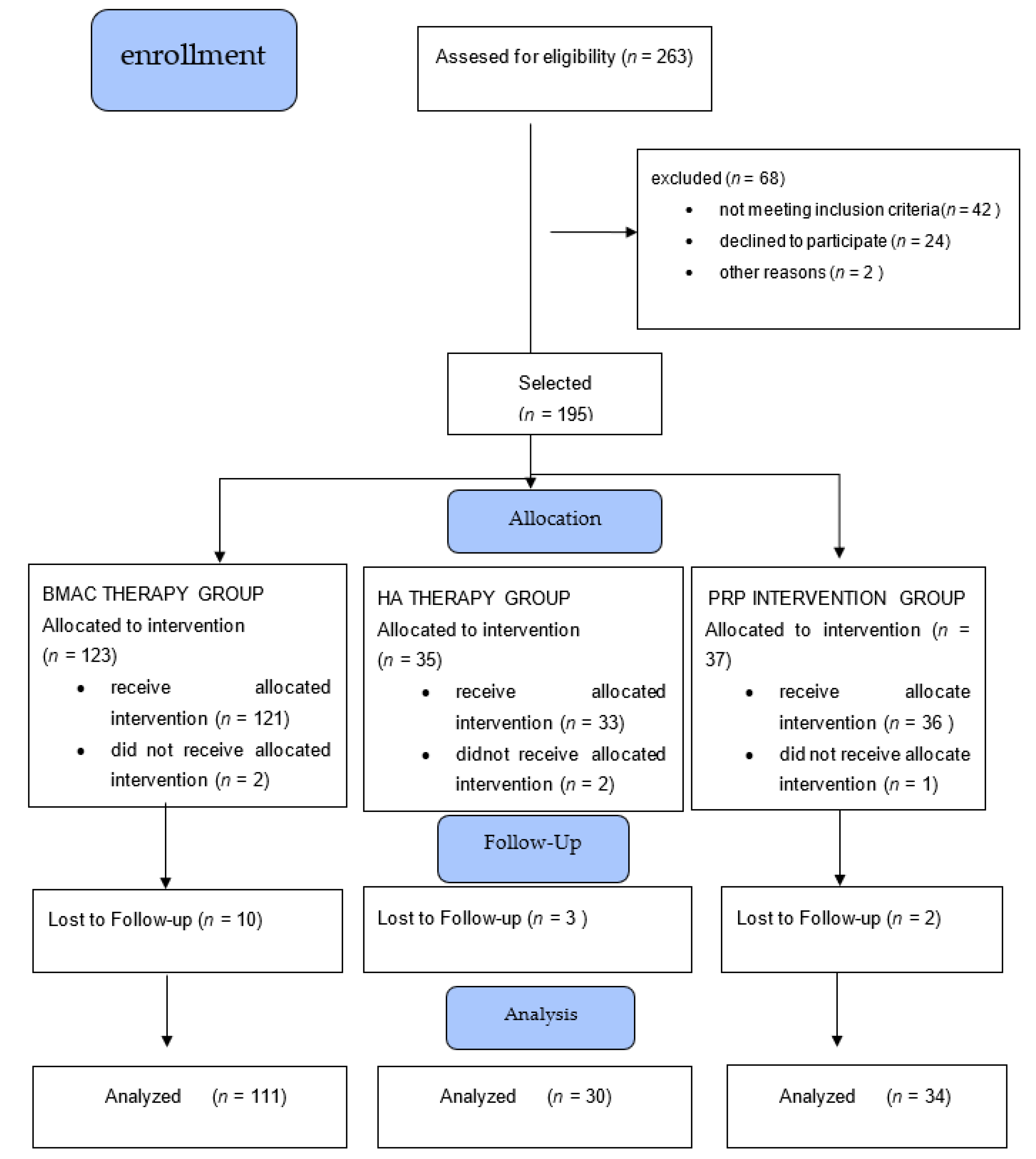
2.1. Study Design and Population
2.2. BMAC Processing Procedure
2.3. In-Vitro Experiments
2.4. PRP Procedure
2.5. HA Injection
2.6. Data Collection
2.7. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Jones, I.A.; Togashi, R.; Wilson, M.L.; Heckmann, N.; Vangsness, C.T., Jr. Intra-articular treatment options for knee osteoarthritis. Nat. Rev. Rheumatol. 2019, 15, 77–90. [Google Scholar] [CrossRef]
- Delanois, R.E.; Etcheson, J.I.; Sodhi, N.; Henn, R.F.; Gwam, C.U.; George, N.E.; Mont, M.A. Biologic Therapies for the Treatment of Knee Osteoarthritis. J. Arthroplast. 2019, 34, 801–813. [Google Scholar] [CrossRef]
- Connolly, J.F.; Guse, R.; Tiedeman, J.; Dehne, R. Autologous marrow injection as a substitute for operative grafting of tibial nonunions. Clin. Orthop. Relat. Res. 1991, 266, 259–270. [Google Scholar] [CrossRef]
- Kitaori, T.; Ito, H.; Schwarz, E.M.; Tsutsumi, R.; Yoshitomi, H.; Oishi, S.; Nakano, M.; Fujii, N.; Nagasawa, T.; Nakamura, T. Stromal cell-derived factor 1/CXCR4 signaling is critical for the recruitment of mesenchymal stem cells to the fracture site during skeletal repair in a mouse model. Arthritis Rheum. 2009, 60, 813–823. [Google Scholar] [CrossRef] [Green Version]
- Masaki, H.; Ide, H. Regeneration potency of mouse limbs. Dev. Growth Differ. 2007, 49, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.B.; Moncivais, K.; Caplan, A. Mesenchymal stem cells: Environmentally responsive therapeutics for regenerative medicine. Exp. Mol. Med. 2013, 45, e54. [Google Scholar] [CrossRef] [Green Version]
- Pittenger, M.F.; Mackay, A.M.; Beck, S.C.; Jaiswal, R.K.; Douglas, R.; Mosca, J.D.; Moorman, M.A.; Simonetti, D.W.; Craig, S.; Marshak, D.R. Multilineage Potential of Adult Human Mesenchymal Stem Cells. Science 1999, 284, 143–147. [Google Scholar] [CrossRef] [Green Version]
- Sampson, S.; Bemden, A.B.-V.; Aufiero, D. Stem Cell Therapies for Treatment of Cartilage and Bone Disorders: Osteoarthritis, Avascular Necrosis, and Non-union Fractures. PM&R 2015, 7, S26–S32. [Google Scholar] [CrossRef]
- Lewandowski, K.; Kowalik, M.M.; Pawlaczyk, R.; Rogowski, J.; Hellmann, A. Microscopic examination of bone marrow aspirate in healthy adults—Comparison of two techniques of slide preparation. Int. J. Lab. Hematol. 2011, 34, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Caplan, A.I. Review:Mesenchymal Stem Cells: Cell–Based Reconstructive Therapy in Orthopedics. Tissue Eng. 2005, 11, 1198–1211. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, S.A.; Kazmerchak, S.E.; Heckman, M.G.; Zubair, A.C.; O’Connor, M.I. A Prospective, Single-Blind, Placebo-Controlled Trial of Bone Marrow Aspirate Concentrate for Knee Osteoarthritis. Am. J. Sports Med. 2016, 45, 82–90. [Google Scholar] [CrossRef]
- Centeno, C.; Sheinkop, M.; Dodson, E.; Stemper, I.; Williams, C.; Hyzy, M.; Ichim, T.; Freeman, M. A specific protocol of autologous bone marrow concentrate and platelet products versus exercise therapy for symptomatic knee osteoarthritis: A randomized controlled trial with 2 year follow-up. J. Transl. Med. 2018, 16, 355. [Google Scholar] [CrossRef] [Green Version]
- Dulić, O.; Lalić, I.; Janjić, N.; Rašović, P.; Gavrilović, G.; Abazović, D. In step with contemporary trends-stem-celltherapy as a key driver of regenerative orthopedics at the Clinical Center of Vojvodina-preliminary data for the treatment of knee osteoarthritis and osteochondral lesions. Med. Pregl. 2016, 69 (Suppl. 1), 77–84. [Google Scholar] [CrossRef]
- Mehta, S.; Watson, J.T. Platelet Rich Concentrate: Basic Science and Current Clinical Applications. J. Orthop. Trauma 2008, 22, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Kabiri, A.; Esfandiari, E.; Esmaeili, A.; Hashemibeni, B.; Pourazar, A.; Mardani, M. Platelet-rich plasma application in chondrogenesis. Adv. Biomed. Res. 2014, 3, 138. [Google Scholar] [CrossRef] [PubMed]
- Dohan Ehrenfest, D.M.; Andia, I.; Zumstein, M.A.; Zhang, C.-Q.; Pinto, N.R.; Bielecki, T. Classification of platelet concentrates (Platelet-Rich Plasma-PRP, Platelet-Rich Fibrin-PRF) for topical and infiltrative use in orthopedic and sports medicine: Current consensus, clinical implications and perspectives. Muscle Ligaments Tendons J. 2014, 4, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Laudy, A.B.M.; Bakker, E.; Rekers, M.; Moen, M.H. Efficacy of platelet-rich plasma injections in osteoarthritis of the knee: A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 657–672. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25416198 (accessed on 15 March 2020). [CrossRef] [Green Version]
- Dai, W.-L.; Zhou, A.-G.; Zhang, H.; Zhang, J. Efficacy of Platelet-Rich Plasma in the Treatment of Knee Osteoarthritis: A Meta-analysis of Randomized Controlled Trials. Arthrosc. J. Arthrosc. Relat. Surg. 2017, 33, 659–670.e1. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.D.; Manjoo, A.; Fierlinger, A.; Niazi, F.; Nicholls, M. The mechanism of action for hyaluronic acid treatment in the osteoarthritic knee: A systematic review. BMC Musculoskelet. Disord. 2015, 16, 321. [Google Scholar] [CrossRef] [Green Version]
- Ayhan, E.; Kesmezacar, H.; Akgun, I. Intraarticular injections (corticosteroid, hyaluronic acid, platelet rich plasma) for the knee osteoarthritis. World J. Orthop. 2014, 5, 351–361. Available online: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=4095029&tool=pmcentrez&rendertype=abstract (accessed on 15 March 2020). [CrossRef]
- Moreland, L.W. Intra-articular hyaluronan (hyaluronic acid) and hylans for the treatment of osteoarthritis: Mechanisms of action. Arthritis Res. 2003, 5, 54–67. [Google Scholar] [CrossRef] [Green Version]
- Phillips, M.; Vannabouathong, C.; Devji, T.; Patel, R.; Gomes, Z.; Patel, A.; Dixon, M.; Bhandari, M. Differentiating factors of intra-articular injectables have a meaningful impact on knee osteoarthritis outcomes: A network meta-analysis. Knee Surgery, Sports Traumatol. Arthrosc. 2020, 28, 3031–3039. [Google Scholar] [CrossRef] [Green Version]
- Anz, A.W.; Hubbard, R.; Rendos, N.; Everts, P.A.; Andrews, J.R.; Hackel, J.G. Bone Marrow Aspirate Concentrate Is Equivalent to Platelet-Rich Plasma for the Treatment of Knee Osteoarthritis at 1 Year: A Prospective, Randomized Trial. Orthop. J. Sports Med. 2020, 8, 2325967119900958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malfait, A.-M.; Miller, R.J. Emerging Targets for the Management of Osteoarthritis Pain. Curr. Osteoporos. Rep. 2016, 14, 260–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, R.; Block, J.; Malfait, A.-M. What is new in pain modification in osteoarthritis? Rheumatology 2018, 57, iv99–iv107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centeno, C.J.; Al-Sayegh, H.; Freeman, M.D.; Smith, J.; Murrell, W.D.; Bubnov, R. A multi-center analysis of adverse events among two thousand, three hundred and seventy two adult patients undergoing adult autologous stem cell therapy for orthopaedic conditions. Int. Orthop. 2016, 40, 1755–1765. [Google Scholar] [CrossRef] [Green Version]
- Filardo, G.; Madry, H.; Jelic, M.; Roffi, A.; Cucchiarini, M.; Kon, E. Mesenchymal stem cells for the treatment of cartilage lesions: From preclinical findings to clinical application in orthopaedics. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 1717–1729. [Google Scholar] [CrossRef]
- Domen, R. Adverse reactions associated with autologous blood transfusion: Evaluation and incidence at a large academic hospital. Transfusion 1998, 38, 296–300. [Google Scholar] [CrossRef]
- Khoshbin, A.; Leroux, T.; Wasserstein, D.; Marks, P.; Theodoropoulos, J.; Ogilvie-Harris, D.; Gandhi, R.; Takhar, K.; Lum, G.; Chahal, J. The Efficacy of Platelet-Rich Plasma in the Treatment of Symptomatic Knee Osteoarthritis: A Systematic Review with Quantitative Synthesis. Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 2037–2048. [Google Scholar] [CrossRef]
- Campbell, K.A.; Saltzman, B.M.; Mascarenhas, R.; Khair, M.M.; Verma, N.N.; Bach, B.R.; Cole, B.J. Does Intra-articular Platelet-Rich Plasma Injection Provide Clinically Superior Outcomes Compared With Other Therapies in the Treatment of Knee Osteoarthritis? A Systematic Review of Overlapping Meta-analyses. Arthrosc. J. Arthrosc. Relat. Surg. 2015, 31, 2213–2221. [Google Scholar] [CrossRef]
- Sampson, S.; Smith, J.; Vincent, H.; Aufiero, D.; Zall, M.; Botto-Van-Bemden, A. Intra-articular bone marrow concentrate injection protocol: Short-term efficacy in osteoarthritis. Regen. Med. 2016, 11, 511–520. [Google Scholar] [CrossRef] [Green Version]
- Centeno, C.; Pitts, J.; Al-Sayegh, H.; Freeman, M. Efficacy of Autologous Bone Marrow Concentrate for Knee Osteoarthritis with and without Adipose Graft. BioMed Res. Int. 2014, 2014, 370621. [Google Scholar] [CrossRef] [Green Version]
- Oliver, K.S.; Bayes, M.; Crane, D.; Pathikonda, C. Clinical Outcome of Bone Marrow Concentrate in Knee Osteoarthritis. J. Prolotherapy 2015, 7, 937–946. [Google Scholar]
- Manchikanti, L.; Centeno, C.J.; Atluri, S.; Albers, S.L.; Shapiro, S.; A Malanga, G.; Abd-Elsayed, A.; Jerome, M.; A Hirsch, J.; Kaye, A.D.; et al. Bone Marrow Concentrate (BMC) Therapy in Musculoskeletal Disorders: Evidence-Based Policy Position Statement of American Society of Interventional Pain Physicians (ASIPP). Pain Physician 2020, 23, E85–E131. [Google Scholar] [PubMed]
- Chahla, J.; Dean, C.S.; Moatshe, G.; Pascual-Garrido, C.; Serra Cruz, R.; LaPrade, R.F. Concentrated Bone Marrow Aspirate for the Treatment of Chondral Injuries and Osteoarthritis of the Knee: A Systematic Review of Outcomes. Orthop. J. Sport. Med. 2016, 4, 2325967115625481. Available online: http://ojs.sagepub.com/content/4/1/2325967115625481.full (accessed on 15 March 2020). [CrossRef] [Green Version]
- Ziegler, C.G.; Van Sloun, R.; Gonzalez, S.; Whitney, K.E.; DePhillipo, N.N.; Kennedy, M.I.; Dornan, G.; Evans, T.A.; Huard, J.; Laprade, R.F. Characterization of Growth Factors, Cytokines, and Chemokines in Bone Marrow Concentrate and Platelet-Rich Plasma: A Prospective Analysis. Am. J. Sports Med. 2019, 47, 2174–2187. [Google Scholar] [CrossRef]
- Narbona-Carceles, J.; Vaquero, J.; Suárez-Sancho, S.; Forriol, F.; Santos, M.E.F. Bone marrow mesenchymal stem cell aspirates from alternative sources Is the knee as good as the iliac crest? Injury 2014, 45, S42–S47. [Google Scholar] [CrossRef]
- Chang, K.-V.; Hung, C.-Y.; Aliwarga, F.; Wang, T.-G.; Han, D.-S.; Chen, W.-S. Comparative Effectiveness of Platelet-Rich Plasma Injections for Treating Knee Joint Cartilage Degenerative Pathology: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2014, 95, 562–575. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, B.; Wragg, N.; Wilson, S.L. The use of PRP injections in the management of knee osteoarthritis. Cell Tissue Res. 2019, 376, 143–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnoczky, S.P.; Shebani-Rad, S. The basic science of platelet-rich plasma (PRP): What clinicians need to know. Sports Med. Arthrosc. 2013, 21, 180–185. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BMAC | HA | PRP | p | |
|---|---|---|---|---|
| Total Number | 111 | 30 | 34 | |
| Age, years (means ± SD) | 56.9 ± 10.8 | 59.4 ± 14.0 | 58.8 ± 11.2 | One way ANOVA F = 0.728; p = 0.485 |
| Gender | Male: 57 | Male: 13 | Male: 15 | Pearson Chi-Square = 0.943; p = 0.624 |
| Female: 54 | Female: 17 | Female: 19 | ||
| KL grade (%) | Grade 2: 49 (44.1%) | Grade 2: 13 (43.3%) | Grade 2: 12 (35.3%) | Pearson Chi-Square = 6.661; p = 0.155 |
| Grade 3: 46 (41.4%) | Grade 3: 8 (26.7%) | Grade 3: 12 (35.3%) | ||
| Grade 4: 16 (14.4%) | Grade 4: 9 (30.0%) | Grade 4: 10 (29.4%) | ||
| BMI (means ± SD) | 28.61 ± 4.53 | 29.98 ± 5.24 | 28.47 ± 4.54 | One way ANOVA F = 1.136; p = 0.323 |
| VAS pain sting | 3.52 ± 3.07 | 3.97 ± 2.30 | 4.47 ± 2.64 | One way ANOVA F = 1.492; p = 0.228 |
| VAS pain injection | 3.59 ± 2.85 | 3.57 ± 2.21 | 4.56 ± 2.69 | One way ANOVA F = 1.741; p = 0.178 |
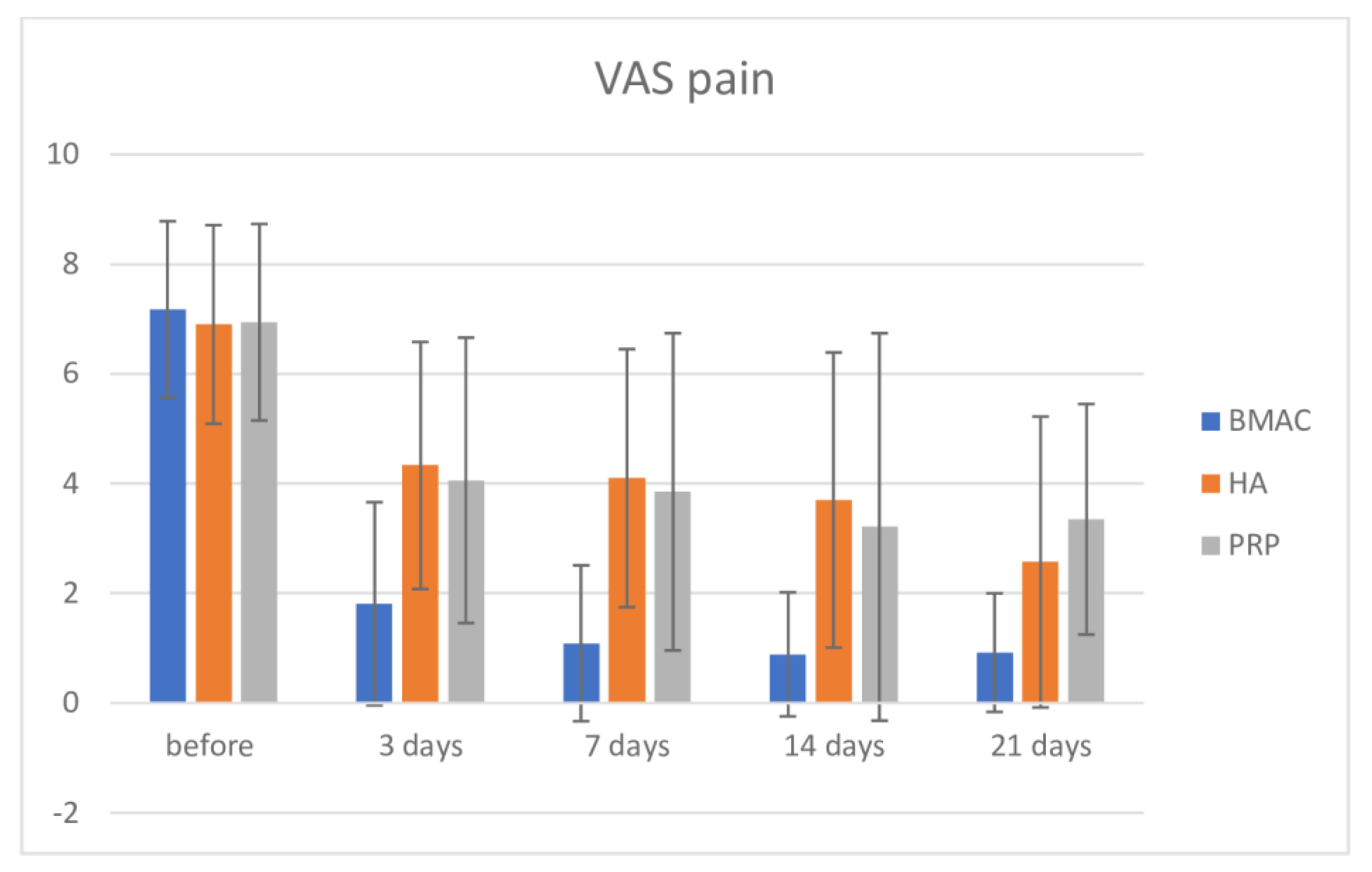
| Intervention | Before | 3 Days | 7 Days | 14 Days | 21 Days |
|---|---|---|---|---|---|
| BMAC | 7.17 ± 1.61 | 1.81 ± 1.85 | 1.09 ± 1.42 | 0.89 ± 1.13 | 0.92 ± 1.08 |
| HA | 6.90 ± 1.81 | 4.33 ± 2.25 | 4.10 ± 2.35 | 3.70 ± 2.69 | 2.57 ± 2.65 |
| PRP | 6.94 ± 1.79 | 4.06 ± 2.60 | 3.85 ± 2.89 | 3.21 ± 3.53 | 3.35 ± 2.10 |
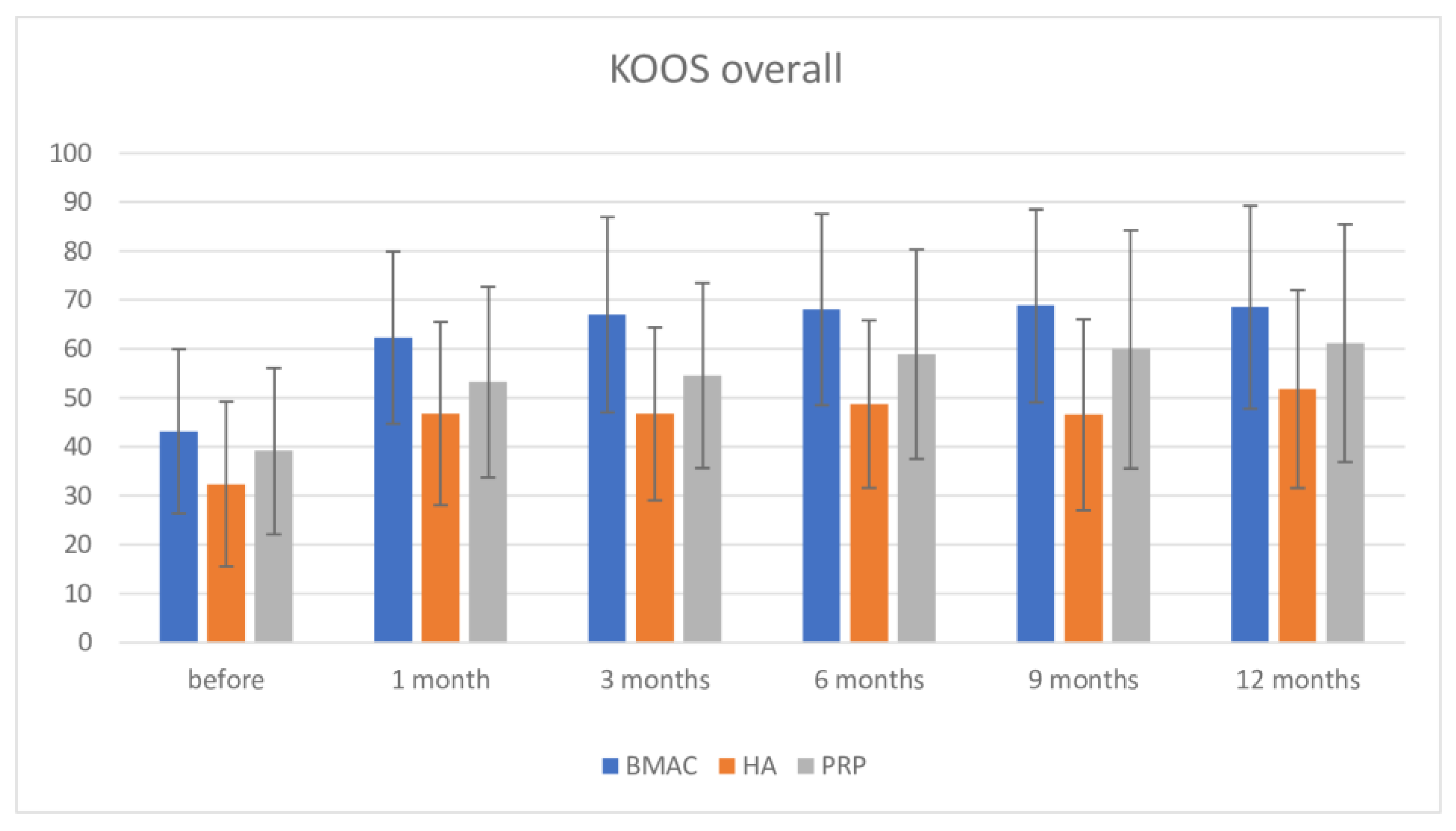
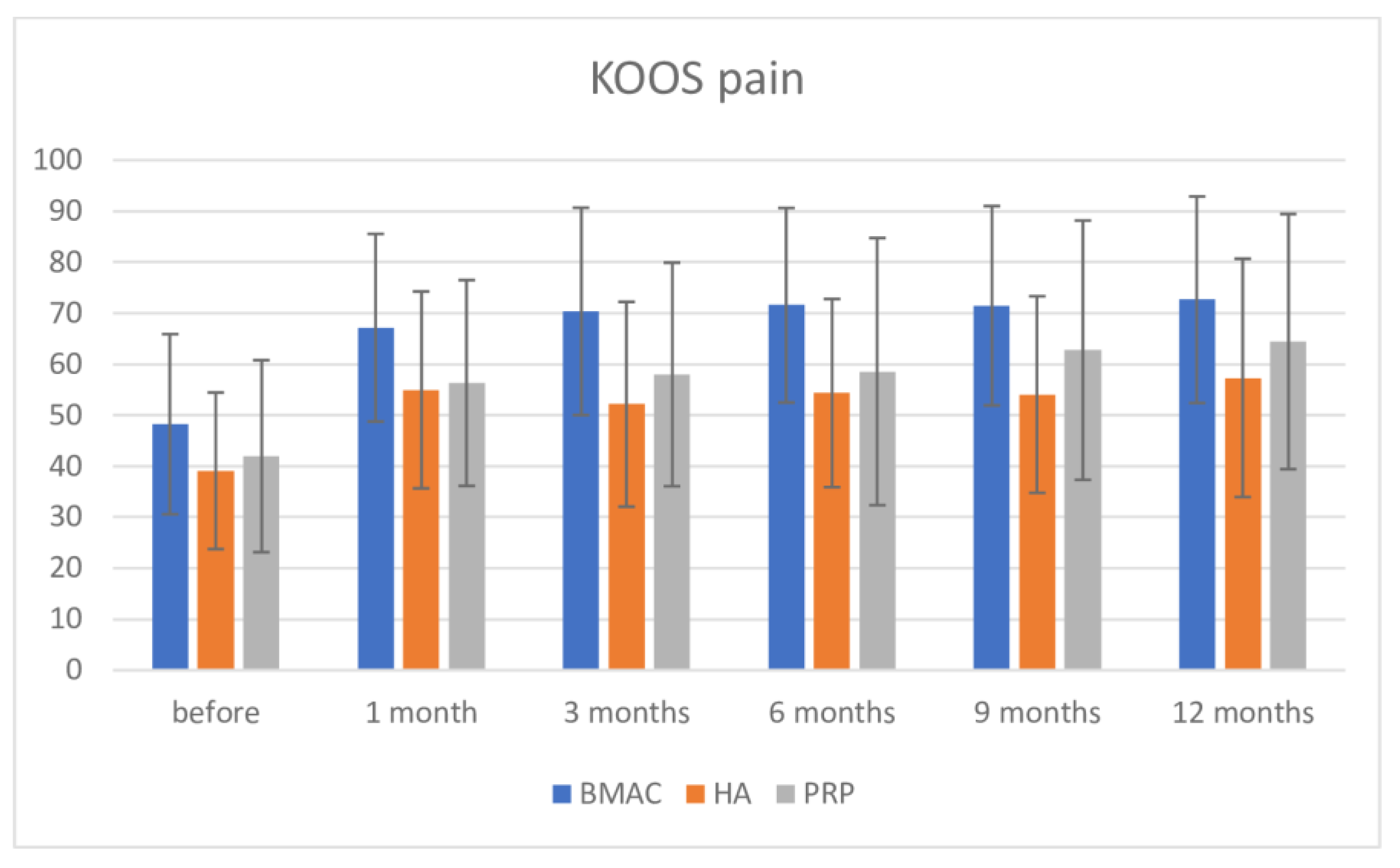
| Before | 1 Month | 3 Months | 6 Months | 9 Months | 12 Months | ||
|---|---|---|---|---|---|---|---|
| KOOS pain | BMAC | 48.24 | 67.13 | 70.35 | 71.55 | 71.46 | 72.63 |
| SD | 17.66 | 18.4 | 20.32 | 19.07 | 19.53 | 20.25 | |
| HA | 39.09 | 54.95 | 52.14 | 54.33 | 54.04 | 57.32 | |
| SD | 15.35 | 19.3 | 20.08 | 18.44 | 19.28 | 23.37 | |
| PRP | 41.96 | 56.31 | 57.99 | 58.54 | 62.75 | 64.43 | |
| SD | 18.82 | 20.19 | 21.92 | 26.19 | 25.43 | 25.02 | |
| KOOS overall | BMAC | 43.18 | 62.38 | 67.03 | 68.09 | 68.84 | 68.52 |
| SD | 16.8 | 17.57 | 19.98 | 19.57 | 19.72 | 20.72 | |
| HA | 32.4 | 46.86 | 46.8 | 48.79 | 46.58 | 51.86 | |
| SD | 16.86 | 18.75 | 17.69 | 17.13 | 19.54 | 20.21 | |
| PRP | 39.19 | 53.29 | 54.63 | 58.94 | 59.98 | 61.24 | |
| SD | 17.01 | 19.49 | 18.91 | 21.39 | 24.36 | 24.34 | |
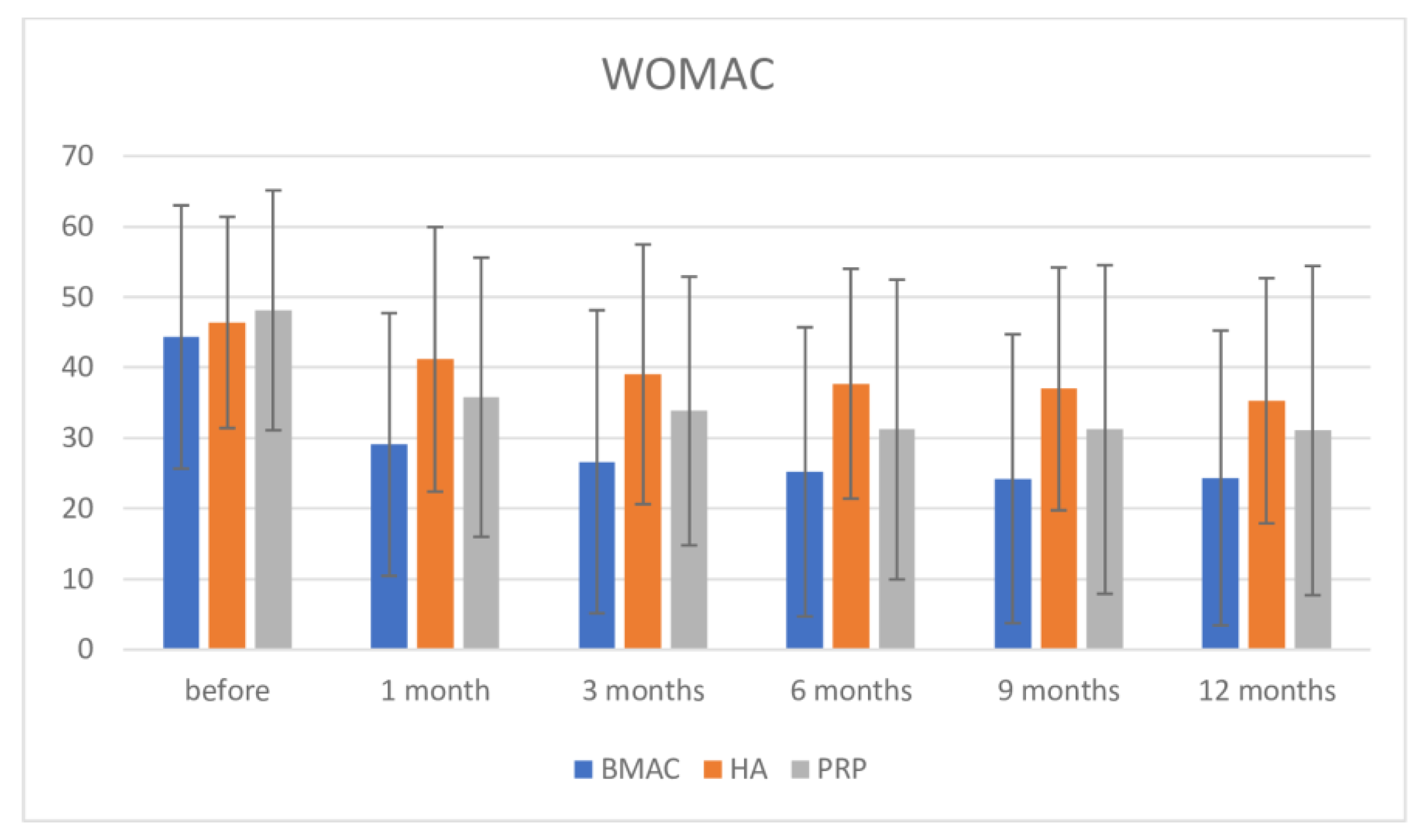
| WOMAC | BMAC | 44.34 | 29.09 | 26.64 | 25.21 | 24.24 | 24.34 |
| SD | 18.67 | 18.63 | 21.49 | 20.51 | 20.48 | 20.91 | |
| HA | 46.41 | 41.17 | 39.05 | 37.71 | 36.98 | 35.29 | |
| SD | 14.98 | 18.77 | 18.41 | 16.31 | 17.22 | 17.39 | |
| PRP | 48.12 | 35.8 | 33.84 | 31.21 | 31.22 | 31.06 | |
| SD | 17.02 | 19.8 | 19.05 | 21.26 | 23.3 | 23.34 | |
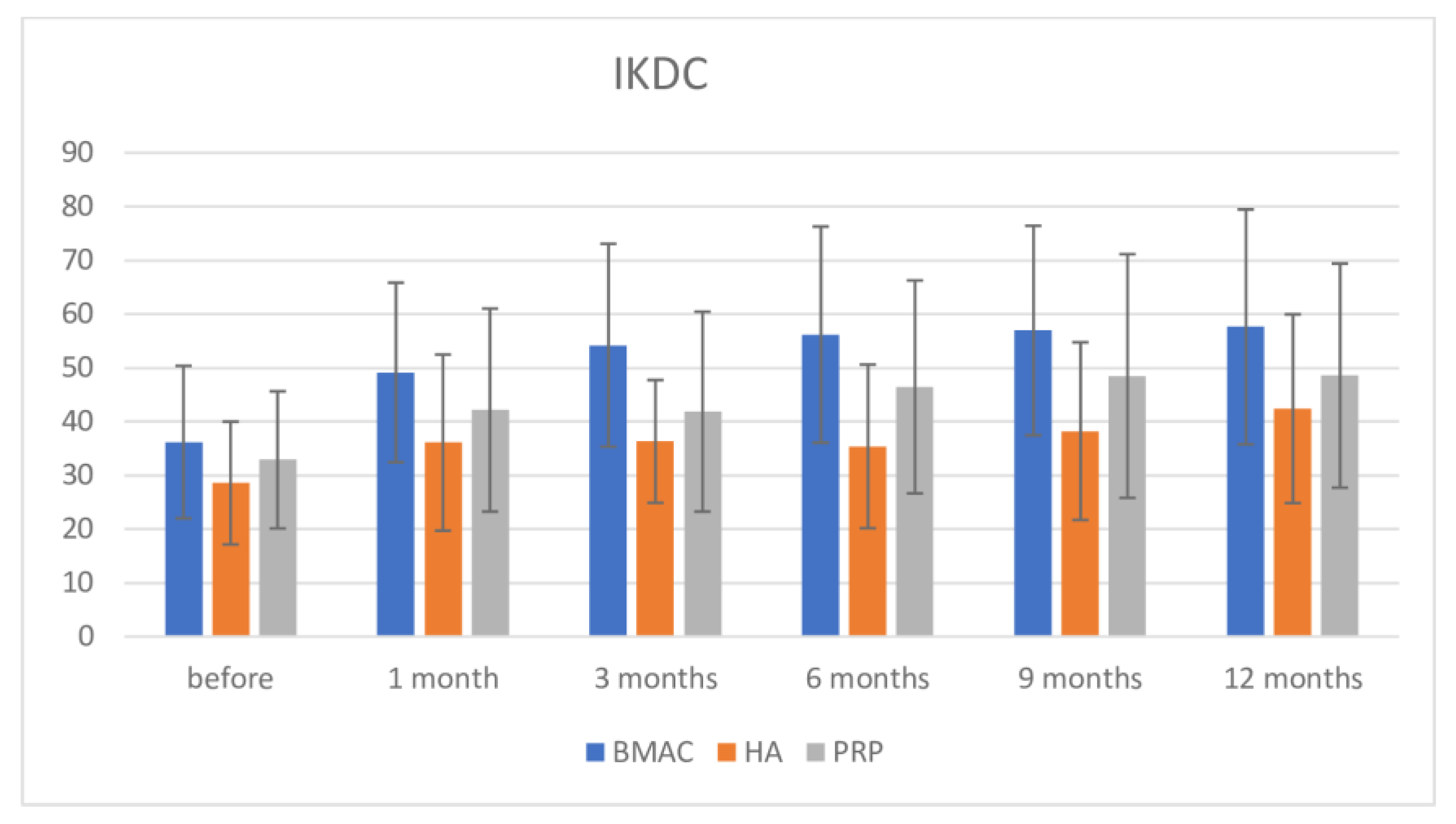
| IKDC | BMAC | 36.19 | 49.13 | 54.2 | 56.18 | 56.94 | 57.62 |
| SD | 14.18 | 16.7 | 18.87 | 20.1 | 19.48 | 21.84 | |
| HA | 28.57 | 36.09 | 36.31 | 35.39 | 38.22 | 42.4 | |
| SD | 11.43 | 16.39 | 11.43 | 15.22 | 16.52 | 17.55 | |
| PRP | 32.89 | 42.14 | 41.85 | 46.45 | 48.48 | 48.55 | |
| SD | 12.75 | 18.88 | 18.6 | 19.81 | 22.67 | 20.83 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dulic, O.; Rasovic, P.; Lalic, I.; Kecojevic, V.; Gavrilovic, G.; Abazovic, D.; Maric, D.; Miskulin, M.; Bumbasirevic, M. Bone Marrow Aspirate Concentrate versus Platelet Rich Plasma or Hyaluronic Acid for the Treatment of Knee Osteoarthritis. Medicina 2021, 57, 1193. https://doi.org/10.3390/medicina57111193
Dulic O, Rasovic P, Lalic I, Kecojevic V, Gavrilovic G, Abazovic D, Maric D, Miskulin M, Bumbasirevic M. Bone Marrow Aspirate Concentrate versus Platelet Rich Plasma or Hyaluronic Acid for the Treatment of Knee Osteoarthritis. Medicina. 2021; 57(11):1193. https://doi.org/10.3390/medicina57111193
Chicago/Turabian StyleDulic, Oliver, Predrag Rasovic, Ivica Lalic, Vaso Kecojevic, Gordan Gavrilovic, Dzihan Abazovic, Dusan Maric, Mladen Miskulin, and Marko Bumbasirevic. 2021. "Bone Marrow Aspirate Concentrate versus Platelet Rich Plasma or Hyaluronic Acid for the Treatment of Knee Osteoarthritis" Medicina 57, no. 11: 1193. https://doi.org/10.3390/medicina57111193