
Pentoxifylline Effects on Hospitalized COVID-19 Patients with Cytokine Storm Syndrome: A Randomized Clinical Trial
 ,
,  , , , , , and
, , , , , and
Abstract
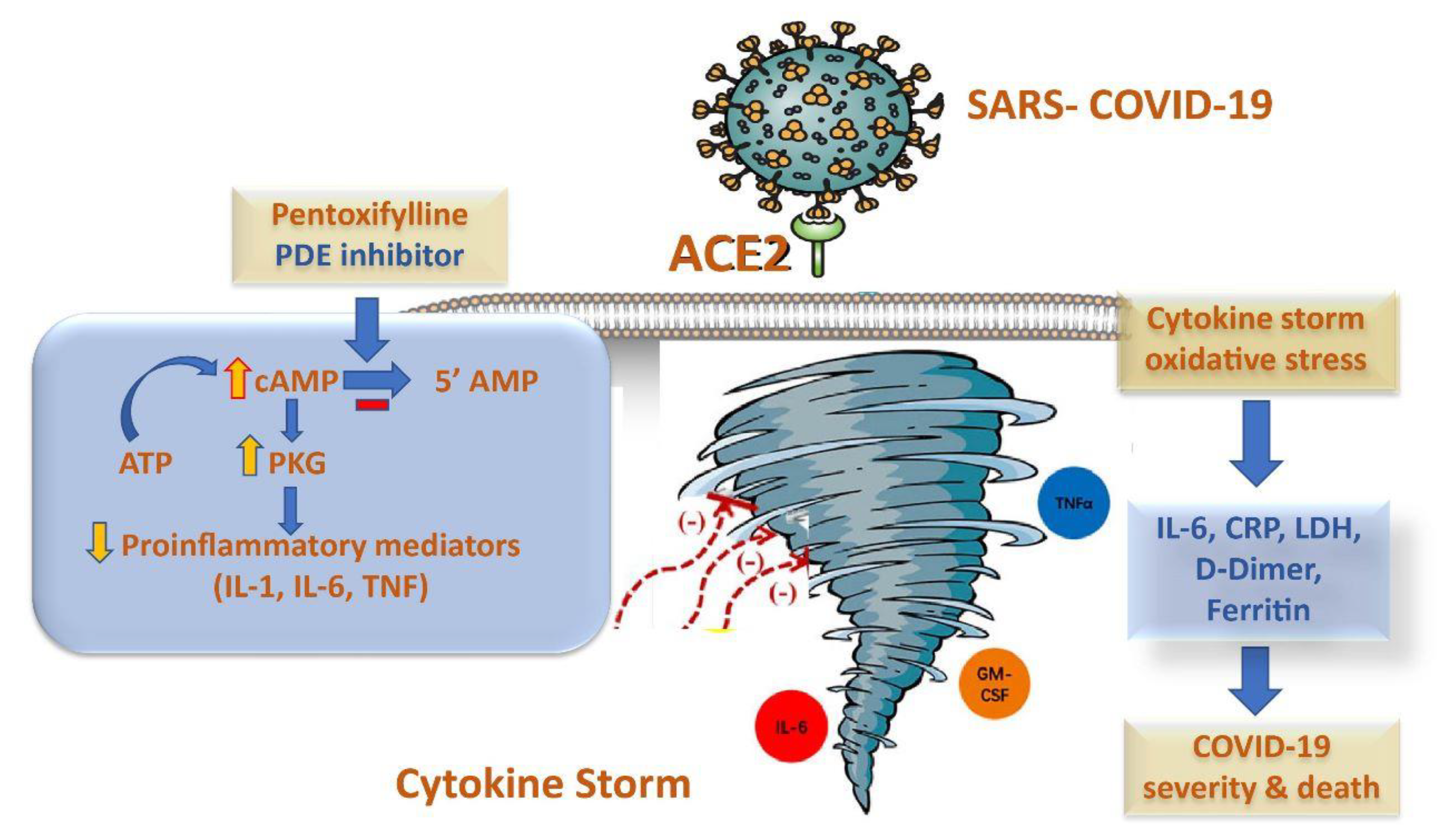
:1. Introduction
2. Results
2.1. Baseline Clinical Characteristics
2.2. Comparison between Initial and Outcome Treatment Laboratory Parameters
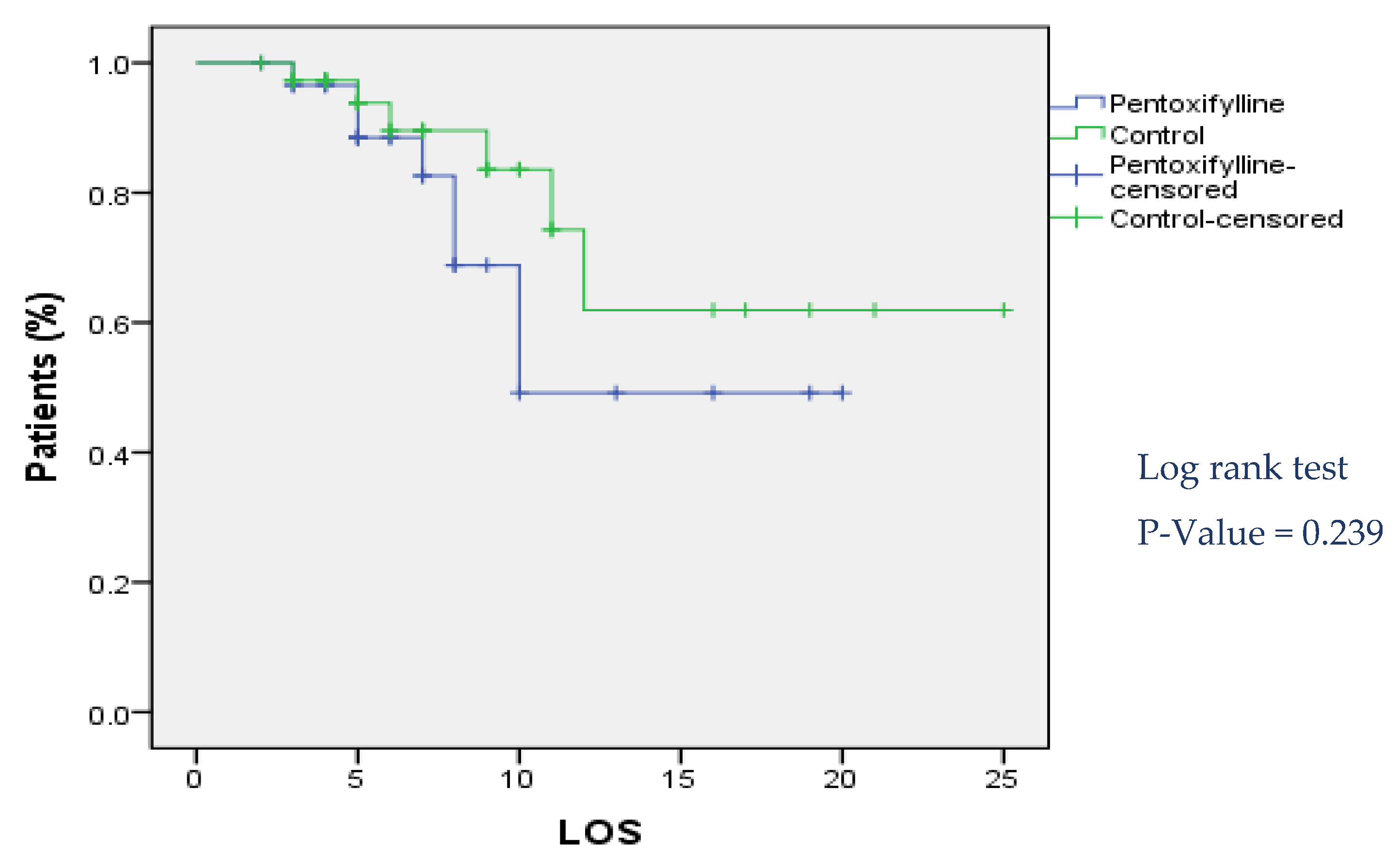
2.3. Comparison of Clinical Outcomes and Kaplan–Meier Curve
2.4. Logistic Regression Model
3. Discussion
4. Patients and Methods
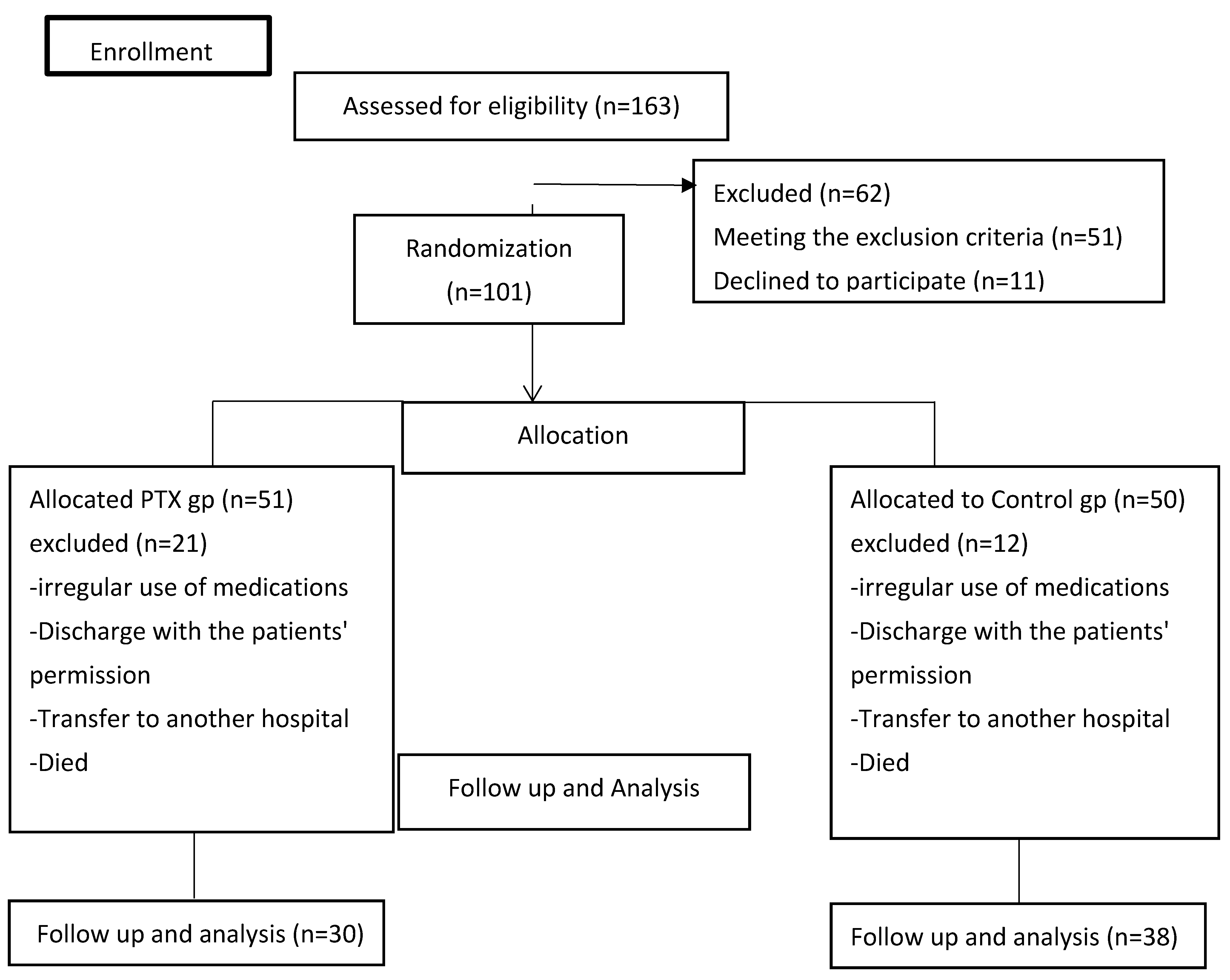
4.1. Study Design
4.2. Study Population
4.3. Study Intervention of the Patients
4.4. Outcomes’ Measurements
4.5. Biochemical Analysis
4.6. Statistical Analysis
4.6.1. Sample Size Calculation
4.6.2. Descriptive and Inferential Statistics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gao, Y.; Xu, G.; Wang, B.; Liu, B. Cytokine storm syndrome in coronavirus disease 2019: A narrative review. J. Intern. Med. 2021, 289, 147–161. [Google Scholar] [CrossRef]
- Montero, F.; Martínez-Barrio, J.; Serrano-Benavente, B.; González, T.; Rivera, J.; Molina Collada, J.; Isabel Castrejón, I.; Álvaro-Gracia, J. Coronavirus disease 2019 (COVID-19) in autoimmune and inflammatory conditions: Clinical characteristics of poor outcomes. Rheumatol. Int. 2020, 40, 1593–1598. [Google Scholar] [CrossRef] [PubMed]
- Ramonfaur, D.; González-Assad, C.A.; Paredes-Vázquez, J.G. Pentoxifylline and COVID-19: A Systematic Review. medRxiv 2020. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Feret, W.; Nalewajska, M.; Wojczyński, Ł.; Witkiewicz, W.; Kłos, P.; Dziedziejko, V.; Pawlik, A. Pentoxifylline as a Potential Adjuvant Therapy for COVID-19: Impeding the Burden of the Cytokine Storm. J. Clin. Med. 2021, 10, 5305. [Google Scholar] [CrossRef] [PubMed]
- Salton, F.; Confalonieri, P.; Campisciano, G.; Cifaldi, R.; Rizzardi, C.; Generali, D.; Pozzan, R.; Tavano, S.; Bozzi, C.; Lapadula, G.; et al. Cytokine Profiles as Potential Prognostic and Therapeutic Markers in SARS-CoV-2-Induced ARDS. J. Clin. Med. 2022, 11, 2951. [Google Scholar] [CrossRef]
- Sarhan, R.M.; Harb, H.S.; Warda, A.E.A.; Salem-Bekhit, M.M.; Shakeel, F.; Alzahrani, S.A.; Madney, Y.M.; Boshra, M.S. Efficacy of the early treatment with tocilizumab-hydroxychloroquine and tocilizumab-remdesivir in severe COVID-19 Patients. J. Infect. Public Health 2022, 15, 116–122. [Google Scholar] [CrossRef]
- Giorgi, M.; Cardarelli, S.; Ragusa, F.; Saliola, M.; Biagioni, S.; Poiana, G.; Naro, F.; Massimi, M. Phosphodiesterase Inhibitors: Could They Be Beneficial for the Treatment of COVID-19? Int. J. Mol. Sci. 2020, 21, 5338. [Google Scholar] [CrossRef]
- Zanza, C.; Romenskaya, T.; Manetti, A.C.; Franceschi, F.; La Russa, R.; Bertozzi, G.; Maiese, A.; Savioli, G.; Volonnino, G.; Longhitano, Y. Cytokine Storm in COVID-19: Immunopathogenesis and Therapy. Medicina 2022, 58, 144. [Google Scholar] [CrossRef]
- Marc, F.; Moldovan, C.M.; Hoza, A.; Magheru, S.; Ciavoi, G.; Farcas, D.M.; Sachelarie, L.; Calin, G.; Romila, L.; Damir, D.; et al. Comparative Study of Cytokine Storm Treatment in Patients with COVID-19 Pneumonia Using Im-munomodulators. J. Clin. Med. 2022, 11, 2945. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; Barroso-Aranda, J. Harnessing adenosine A2A receptors as a strategy for suppressing the lung inflammation and thrombotic complications of COVID-19: Potential of pentoxifylline and dipyridamole. Med. Hypotheses 2020, 143, 110051. [Google Scholar] [CrossRef]
- Li, H.; Zuo, J.; Tang, W. Phosphodiesterase-4 inhibitors for the treatment of inflammatory diseases. Front. Pharmacol. 2018, 9, 1048. [Google Scholar] [CrossRef] [PubMed]
- Navarro, J.; Punzón, C.; Jiménez, J.L.; Fernández-Cruz, E.; Pizarro, A.; Fresno, M.; Muñoz-Fernández, M.A. Inhibition of Phosphodiesterase Type IV Suppresses Human Immunodeficiency Virus Type 1 Replication and Cytokine Production in Primary T Cells: Involvement of NF-κB and NFAT. J. Virol. 1998, 72, 4712. [Google Scholar] [CrossRef] [PubMed]
- Brie, D.; Sahebkar, A.; Penson, P.E.; Dinca, M.; Ursoniu, S.; Serban, M.C.; Zanchetti, A.; Howard, G.; Ahmed, A.; Aronow, W.S.; et al. Effects of pentoxifylline on inflammatory markers and blood pressure: A systematic review and meta-analysis of randomized controlled trials. J. Hypertens. 2016, 34, 2318–2329. [Google Scholar] [CrossRef] [PubMed]
- Marques, L.J.; Zheng, L.; Poulakis, N.; Guzman, J.; Costabel, U. Pentoxifylline inhibits TNF-α production from human alveolar macrophages. Am. J. Respir. Crit. Care Med. 1999, 159, 508–511. [Google Scholar] [CrossRef]
- Martin, J.B.; Jimenez, J.L.; MuEóz-Fernández, A. Pentoxifylline and severe acute respiratory syndrome (SARS): A drug to be considered. Med. Sci. Monit. 2003, 9, SR29–SR34. [Google Scholar]
- Wen, W.X.; Lee, S.Y.; Siang, R.; Koh, R.Y. Repurposing pentoxifylline for the treatment of fibrosis: An overview. Adv. Ther. 2017, 34, 1245–1269. [Google Scholar] [CrossRef]
- Milne, G.R.; Palmer, T.M. Anti-inflammatory and immunosuppressive effects of the A2A adenosine receptor. Sci. World J. 2011, 11, 320–339. [Google Scholar] [CrossRef] [PubMed]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; MacAry, P.A.; Ng, L.F. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Seirafianpour, F.; Mozafarpoor, S.; Fattahi, N.; Sadeghzadeh-Bazargan, A.; Hanifiha, M.; Goodarzi, A. Treatment of COVID-19 with pentoxifylline: Could it be a potential adjuvant therapy? Dermatol. Ther. 2020, 33, e13733. [Google Scholar] [CrossRef]
- Mahajan, R. Acute lung injury: Options to improve oxygenation. Contin. Educ. Anaesth. Crit. Care Pain 2005, 5, 52–55. [Google Scholar] [CrossRef]
- Michetti, C.; Coimbra, R.; Hoyt, D.B.; Loomis, W.; Junger, W.; Wolf, P. Pentoxifylline reduces acute lung injury in chronic endotoxemia. J. Surg. Res. 2003, 115, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Champion, S.; Lapidus, N.; Cherié, G.; Spagnoli, V.; Oliary, J.; Solal, A.C. Pentoxifylline in heart failure: A meta-analysis of clinical trials. Cardiovasc. Ther. 2014, 32, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Parker, R.; Armstrong, M.; Corbett, C.; Rowe, I.A.; Houlihan, D.D. Systematic review: Pentoxifylline for the treatment of severe alcoholic hepatitis. Aliment. Pharmacol. Ther. 2013, 37, 845–854. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.-K.; Duan, S.-B.; Pan, P.; Xu, X.-Q.; Liu, N.; Xu, J. Preventive effect of pentoxifylline on contrast-induced acute kidney injury in hypercholesterolemic rats. Exp. Ther. Med. 2015, 9, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Yuan, X.; Xie, W. Pentoxifylline exerts anti-inflammatory effects on cerebral ischemia reperfusion-induced injury in a rat model via the p38 mitogen-activated protein kinase signaling pathway. Mol. Med. Rep. 2018, 17, 1141–1147. [Google Scholar] [CrossRef]
- Staubach, K.H.; Schröder, J.; Stüber, F.; Gehrke, K.; Traumann, E.; Zabel, P. Effect of pentoxifylline in severe sepsis: Results of a randomized, double-blind, placebo-controlled study. Arch. Surg. 1998, 133, 94–100. [Google Scholar] [CrossRef]
- Pammi, M.; Haque, K.N. Pentoxifylline for treatment of sepsis and necrotizing enterocolitis in neonates. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Dhameliya, H.A.; Thakkar, V.R.; Trivedi, G.N.; Mesara, S.N.; Subramanian, R.B. Pentoxifylline: An immunomodulatory drug for the treatment of COVID-19. J. Pure Appl. Microbiol. 2020, 14, 861–867. [Google Scholar] [CrossRef]
- Maldonado, V.; Loza-Mejía, M.A.; Chávez-Alderete, J. Repositioning of pentoxifylline as an immunomodulator and regulator of the renin-angiotensin system in the treatment of COVID-19. Med. Hypotheses 2020, 144, 109988. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, V.; Hernandez-Ramírez, C.; Oliva-Pérez, E.A.; Sánchez-Martínez, C.O.; Pimentel-González, J.F.; Molina-Sánchez, J.R.; Jiménez-Villalba, Y.Z.; Chávez-Alderete, J.; Loza-Mejía, M.A. Pentoxifylline decreases serum LDH levels and increases lymphocyte count in COVID-19 patients: Results from an external pilot study. Int. Immunopharmacol. 2021, 90, 107209. [Google Scholar] [CrossRef]
- Ghasemnejad-Berenji, M.; Pashapour, S.; Sadeghpour, S. Pentoxifylline: A drug with antiviral and anti-inflammatory effects to be considered in the treatment of coronavirus disease 2019. Med. Princ. Pract. 2021, 30, 98–100. [Google Scholar] [CrossRef]
- Lai, C.-C.; Ko, W.-C.; Lee, P.-I.; Jean, S.-S.; Hsueh, P.-R. Extra-respiratory manifestations of COVID-19. Int. J. Antimicrob. Agents 2020, 56, 106024. [Google Scholar] [CrossRef] [PubMed]
- Matthay, M.A.; Zemans, R.L.; Zimmerman, G.A.; Arabi, Y.M.; Beitler, J.R.; Mercat, A.; Herridge, M.; Randolph, A.G.; Calfee, C.S. Acute respiratory distress syndrome. Nat. Rev. Dis. Prim. 2019, 5, 18. [Google Scholar] [CrossRef]
- Monji, F.; Siddiquee, A.; Hashemian, F. Potential Role of Methylxanthines as an Adjuvant to COVID-19 Treatment: A Review of Pentoxifylline and Caffeine as the Case of Any Port in the Storm. Authorea Preprints. 2020. Available online: https://www.authorea.com/doi/full/10.22541/au.159015270.02586731 (accessed on 20 October 2022).
- Mehta, P.; Fajgenbaum, D.C. Is severe COVID-19 a cytokine storm syndrome: A hyperinflammatory debate. Curr. Opin. Rheumatol. 2021, 33, 419. [Google Scholar] [CrossRef] [PubMed]
- Sayah, W.; Berkane, I.; Guermache, I.; Sabri, M.; Lakhal, F.Z.; Rahali, S.Y.; Djidjeli, A.; Mahammed, L.L.; Merah, F.; Belaid, B.; et al. Interleukin-6, procalcitonin and neutrophil-to-lymphocyte ratio: Potential immune-inflammatory parameters to identify severe and fatal forms of COVID-19. Cytokine 2021, 141, 155428. [Google Scholar] [CrossRef] [PubMed]
- Smilowitz, N.R.; Kunichoff, D.; Garshick, M.; Shah, B.; Pillinger, M.; Hochman, J.S.; Berger, J.S. C-reactive protein and clinical outcomes in patients with COVID-19. Eur. Heart J. 2021, 42, 2270–2279. [Google Scholar] [CrossRef] [PubMed]
- González-Pacheco, H.; Amezcua-Guerra, L.M.; Sandoval, J.; Arias-Mendoza, A. Potential usefulness of pentoxifylline, a non-specific phosphodiesterase inhibitor with anti-inflammatory, anti-thrombotic, antioxidant, and anti-fibrogenic properties, in the treatment of SARS-CoV-2. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 7612–7614. [Google Scholar]
- Chavarría, A.P.; Vázquez, R.R.V.; Cherit, J.G.D.; Bello, H.H.; Suastegui, H.C.; Moreno-Castañeda, L.; Estrada, G.A.; Hernández, F.; González-Marcos, O.; Saucedo-Orozco, H.; et al. Antioxidants and pentoxifylline as coadjuvant measures to standard therapy to improve prognosis of patients with pneumonia by COVID-19. Comput. Struct. Biotechnol. J. 2021, 19, 1379–1390. [Google Scholar] [CrossRef]
- Azizi, H.; Rouhani, N.; Shaki, F.; Karimpour-Razkenari, E.; Ghazaeian, M.; Salehifar, E.; Saeedi, M.; Fallah, S. Pentoxifylline effects on hospitalized patients with COVID19: A randomized, double-blind clinical trial. Int. Immunopharmacol. 2021, 101, 108227. [Google Scholar] [CrossRef]
- Li, X.; Liu, C.; Mao, Z.; Xiao, M.; Wang, L.; Qi, S.; Zhou, F. Predictive values of neutrophil-to-lymphocyte ratio on disease severity and mortality in COVID-19 patients: A systematic review and meta-analysis. Crit. Care 2020, 24, 647. [Google Scholar] [CrossRef] [PubMed]
- González-Pacheco, H.; Amezcua-Guerra, L.M.; Sandoval, J.; Arias-Mendoza, A. Hypothesis for potential pathogenesis of SARS-CoV-2 infection—A review of immune changes in patients with viral pneumonia. Emerg. Microbes Infect. 2020, 9, 727–732. [Google Scholar]
- Palladino, M. Complete blood count alterations in COVID-19 patients: A narrative review. Biochem. Med. 2021, 31. [Google Scholar] [CrossRef] [PubMed]
- Violetis, O.A.; Chasouraki, A.M.; Giannou, A.M.; Baraboutis, I.G. COVID-19 infection and haematological involvement: A review of epidemiology, pathophysiology and prognosis of full blood count findings. SN Compr. Clin. Med. 2020, 2, 1089–1093. [Google Scholar] [CrossRef] [PubMed]
- Selim, S. Leukocyte count in COVID-19: An important consideration. Egypt. J. Bronchol. 2020, 14, 1089–1093. [Google Scholar] [CrossRef]
- Yao, Y.; Cao, J.; Wang, Q.; Shi, Q.; Liu, K.; Luo, Z.; Chen, X.; Chen, S.; Yu, K.; Huang, Z.; et al. D-dimer as a biomarker for disease severity and mortality in COVID-19 patients: A case control study. J. Intensive Care 2020, 8, 49. [Google Scholar] [CrossRef] [PubMed]
- Chousterman, B.G.; Swirski, F.K.; Weber, G.F. Cytokine storm and sepsis disease pathogenesis. In Seminars in Immunopathology; Springer: Berlin/Heidelberg, Germany, 2017; Volume 39, pp. 517–528. [Google Scholar]
- Lee, D.W.; Gardner, R.; Porter, D.L.; Louis, C.U.; Ahmed, N.; Jensen, M.C.; Grupp, S.A.; Mackall, C.L. Current concepts in the diagnosis and management of cytokine release syndrome. Blood J. Am. Soc. Hematol. 2014, 124, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Serdar, C.C.; Cihan, M.; Yücel, D.; A Serdar, M.A. Sample size, power and effect size revisited: Simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochem. Med. 2021, 31, 27–53. [Google Scholar] [CrossRef] [PubMed]
- Viechtbauer, W.; Smits, L.; Kotz, D.; Budé, L.; Spigt, M.; Serroyen, J.; Crutzen, R. A simple formula for the calculation of sample size in pilot studies. J. Clin. Epidemiol. 2015, 68, 1375–1379. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Treatment Group (n = 30) | Control Group (n = 38) | p-Value | |
|---|---|---|---|
| Age and Gender | |||
| Male no. (%) | 19 (63.3%) | 25 (65.8%) | 0.83 |
| Age in yrs. mean ± SD | 63.3 ± 11.75 | 65.4 ± 11.87 | 0.46 |
| Need For Oxygen Therapy | |||
| Low Flow Oxygen no. (%) | 10 (33.3%) | 17 (44.7%) | 0.455 |
| High Flow Oxygen no. (%) | 18 (60%) | 19 (50%) | 0.468 |
| Mechanical Ventilation no. (%) | 2 (6.7%) | 2 (5.3%) | 1.00 |
| Patient History | |||
| Hypertension no. (%) | 18 (60%) | 20 (52.6%) | 0.54 |
| Diabetes Mellitus no. (%) | 11 (36.7%) | 16 (42.1%) | 0.65 |
| Ischemic Heart Disease no. (%) | 5 (16.7%) | 9 (23.7%) | 0.48 |
| Atrial Fibrillation no. (%) | 2 (6.7%) | 0 (0%) | 0.19 |
| Asthma no. (%) | 1 (3.3%) | 7 (18.4%) | 0.07 |
| COPD no. (%) | 3 (10%) | 0 (0%) | 0.08 |
| Chronic Kidney Disease no. (%) | 1 (3.3%) | 1 (2.6%) | 1.00 |
| Chronic Liver Disease no. (%) | 0 (0%) | 1 (2.6%) | 1.00 |
| Malignancy no. (%) | 2 (6.6%) | 4 (10.5%) | 0.94 |
| Thyroid disorders no. (%) | 2 (6.6%) | 1 (2.6%) | 1.00 |
| Stroke no. (%) | 1 (3.3%) | 0 (0%) | 0.20 |
| Obesity no. (%) | 3 (10%) | 5 (13.1%) | 0.521 |
| Smoker no. (%) | 6 (20%) | 9 (23.6%) | 0.49 |
| Treatment Medications | |||
| Remdesivir no. (%) | 25 (83.3%) | 34 (89.5%) | 0.49 |
| Lopinavir/Ritonavir no. (%) | 1 (3.3%) | 2 (5.4%) | 1.00 |
| Hydroxychloroquine no. (%) | 0 (0%) | 2 (5.3%) | 0.50 |
| Tocilizumab no. (%) | 17 (56.7%) | 20 (52.6%) | 0.74 |
| Treatment Group (n = 30) Median Initial Level (Range) | Control Group (n = 38) Median Initial Level (Range) | p-Value | |
|---|---|---|---|
| D-Dimer | 0.5 (4.2) | 0.6 (7.4) | 0.47 |
| LDH | 385.4 (646) | 385.4 (509) | 0.69 |
| Ferritin | 605 (3777) | 1009 (4120) | 0.38 |
| CRP | 112.7 (335) | 93 (309.5) | 0.98 |
| IL6 | 47.2 (355.5) | 52.2 (232) | 0.814 |
| Serum Creatinine | 1.3 (6.1) | 1.4 (10.7) | 0.47 |
| TLC | 7.6 (27.5) | 8.1 (30.3) | 0.91 |
| NLP | 8.6 (22.3) | 8.8 (29.3) | 0.57 |
| ALT | 50 (338) | 40 (1019) | 0.380 |
| AST | 41.5 (179) | 47 (503) | 0.302 |
| P/F | 171.5 (122) | 170 (144) | 0.282 |
| Median Initial Level (Range) | Median Outcome Level (Range) | p-Value | |
|---|---|---|---|
| C-Reactive Protein | |||
| Treatment | 112.7 (335) | 37.5 (601.5) | <0.01 |
| Control | 93 (309.5) | 27.2 (217.8) | <0.01 |
| D-Dimer | |||
| Treatment | 0.5 (4.2) | 1.3 (6.9) | <0.01 |
| Control | 0.6 (7.4) | 0.9 (38.4) | 0.21 |
| LDH | |||
| Treatment | 385.4 (646) | 440.4 (59.1) | 0.15 |
| Control | 385.4 (509) | 440.4 (221.3) | 0.13 |
| Ferritin | |||
| Treatment | 605 (3777) | 774.5 (2480) | 0.45 |
| Control | 1009 (4120) | 775 (2460) | 0.16 |
| IL6 | |||
| Treatment | 47.2 (355.5) | 16.5 (65) | 0.004 |
| Control | 52.2 (232.1) | 17.95 (77) | 0.001 |
| Total Leukocytic Count | |||
| Treatment | 7.6 (27.5) | 12.5 (25.7) | 0.003 |
| Control | 8.1 (30.3) | 10.6 (19.5) | 0.002 |
| Neutrophil to Lymphocyte Ratio | |||
| Treatment | 8.6 (22.3) | 12.3 (46.7) | 0.002 |
| Control | 8.8 (29.3) | 12.3 (93.5) | 0.001 |
| P/F | |||
| Treatment | 171.5 (122) | 214.5 (188) | 0.328 |
| Control | 170 (144) | 223 (161) | 0.022 |
| ALT | |||
| Treatment | 50 (338) | 42 (213) | 0.848 |
| Control | 40 (1019) | 51(1633) | 0.007 |
| AST | |||
| Treatment | 41.5 (179) | 36 (142) | 0.216 |
| Control | 47 (503) | 40 (505) | 0.806 |
| Outcomes | Treatment Group (n = 30) | Control Group (n = 38) | p-Value |
|---|---|---|---|
| Clinical Improvement no. (%) | 22 (73.3%) | 31 (81.6%) | 0.42 |
| Length of Hospital Stay (LOS), Median (Range) | 6.5 (4.25) | 6.5 (6.25) | 0.918 |
| Death no. (%) | 8 (26.7%) | 6 (15.8%) | 0.27 |
| Occurrence of Adverse Effects no. (%) | |||
| Nausea and Vomiting | 6 (20%) | 4 (10.5%) | 0.497 |
| Abdominal Discomfort | 8 (26.6%) | 9 (23.6%) | 0.421 |
| Anorexia | 3 (10%) | 1 (2.6%) | 0.619 |
| Headache | 4 (13.3%) | 7 (18.4%) | 0.167 |
| Variable | Odds Ratio | Confidence Interval | Significance (p-Value) |
|---|---|---|---|
| IHD | 3.46 | 2.1–4.5 | 0.036 * |
| Asthma | 2.75 | 1.5–3.9 | 0.041 * |
| Baseline IL-6 | 2.06 | 1.3–4.2 | 0.01 * |
| Baseline D-dimer | 1.3 | 1.1–2.04 | 0.048 * |
| Clinical improvement | 7.4 | 3.7–8.3 | 0.008 * |
| Odds Ratio | Confidence Interval | Significance (p-Value) | |
|---|---|---|---|
| Baseline LDH | 0.88 | 0.97–1.02 | 0.19 |
| Baseline IL-6 | 0.69 | 0.45–0.88 | 0.04 * |
| P/F ratio | 1.81 | 1.1–2.4 | 0.036 * |
| Length of stay | 1.23 | 0.8–1.3 | 0.058 |
| Hypertension | 1.12 | 0.12–10.6 | 0.13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarhan, R.M.; E. Altyar, A.; Essam Abou Warda, A.; Saied, Y.M.; Ibrahim, H.S.G.; Schaalan, M.F.; Fathy, S.; Sarhan, N.; Boshra, M.S. Pentoxifylline Effects on Hospitalized COVID-19 Patients with Cytokine Storm Syndrome: A Randomized Clinical Trial. Pharmaceuticals 2023, 16, 631. https://doi.org/10.3390/ph16040631
Sarhan RM, E. Altyar A, Essam Abou Warda A, Saied YM, Ibrahim HSG, Schaalan MF, Fathy S, Sarhan N, Boshra MS. Pentoxifylline Effects on Hospitalized COVID-19 Patients with Cytokine Storm Syndrome: A Randomized Clinical Trial. Pharmaceuticals. 2023; 16(4):631. https://doi.org/10.3390/ph16040631
Chicago/Turabian StyleSarhan, Rania M., Ahmed E. Altyar, Ahmed Essam Abou Warda, Yasmine Mohamed Saied, Haytham Soliman Ghareeb Ibrahim, Mona F. Schaalan, Shaimaa Fathy, Neven Sarhan, and Marian S. Boshra. 2023. "Pentoxifylline Effects on Hospitalized COVID-19 Patients with Cytokine Storm Syndrome: A Randomized Clinical Trial" Pharmaceuticals 16, no. 4: 631. https://doi.org/10.3390/ph16040631