
A Phase 2a, Randomized, Double-Blind, Placebo-Controlled Study to Assess the Efficacy and Safety of ALS-L1023 in Non-Alcoholic Fatty Liver Disease

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
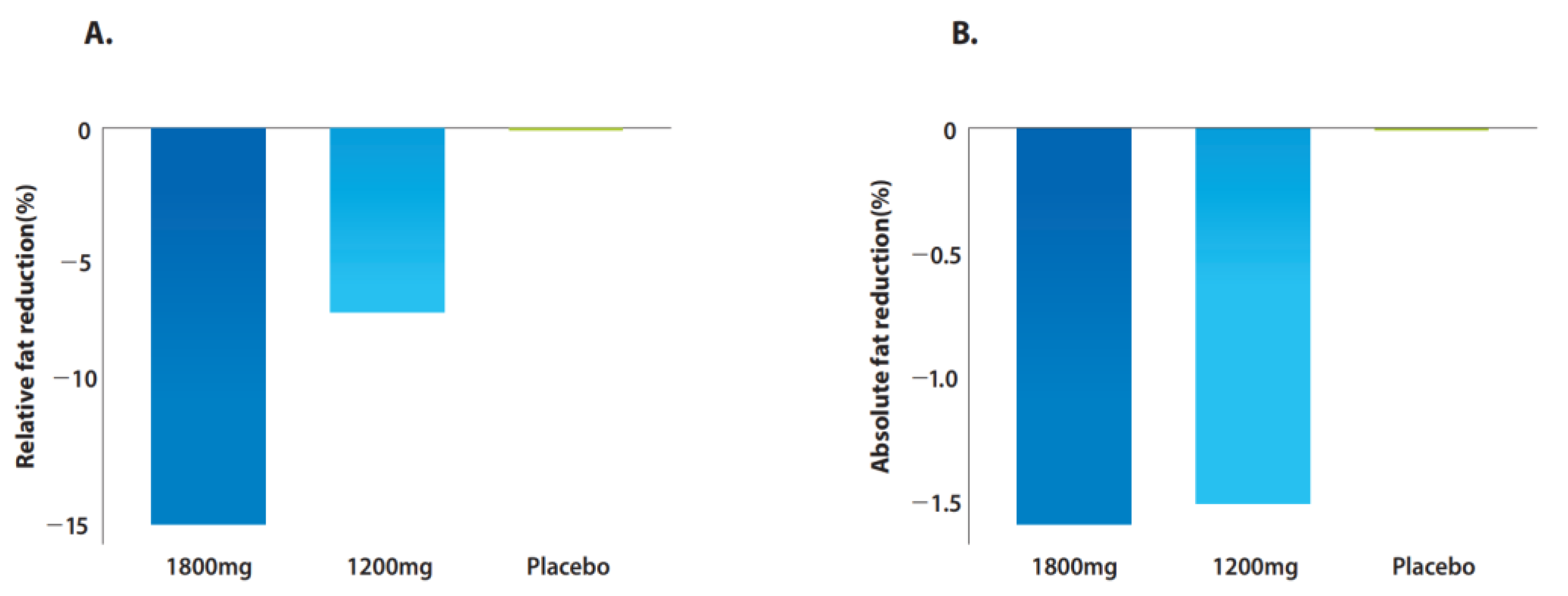
2.2. Changes in Hepatic Steatosis on MRI-PDFF
2.3. Changes in Liver Stiffness on MRE
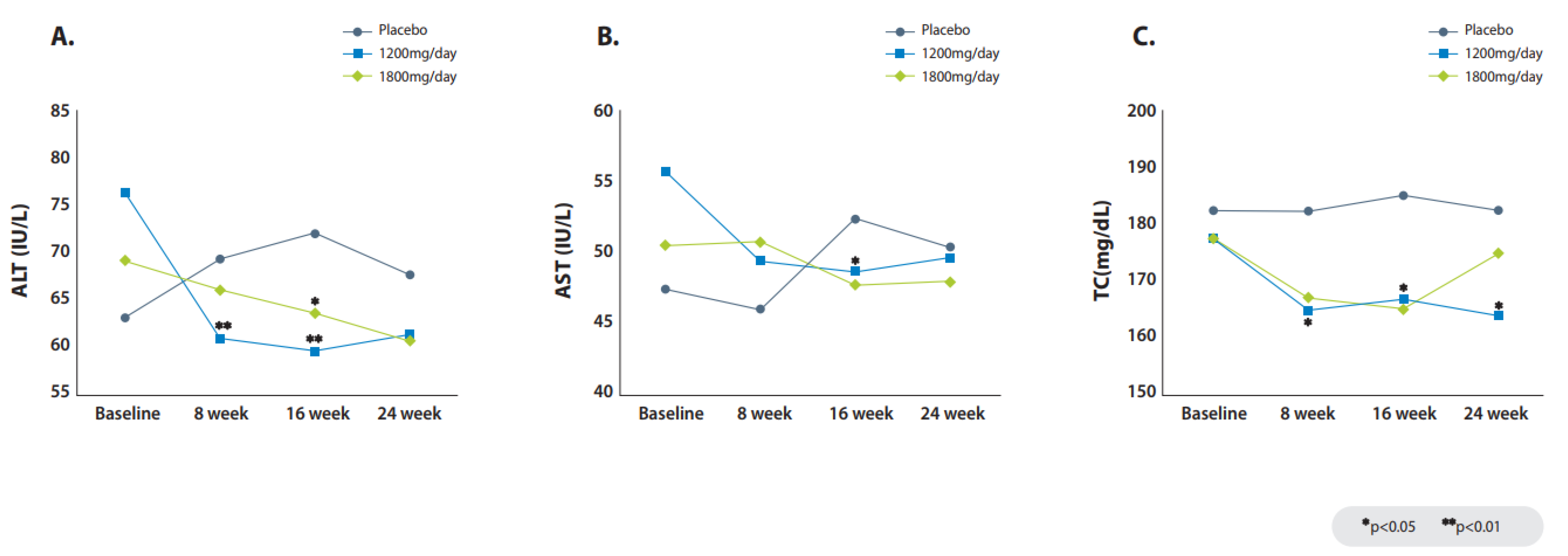
2.4. Changes in Liver Biochemistry
2.5. Safety Results
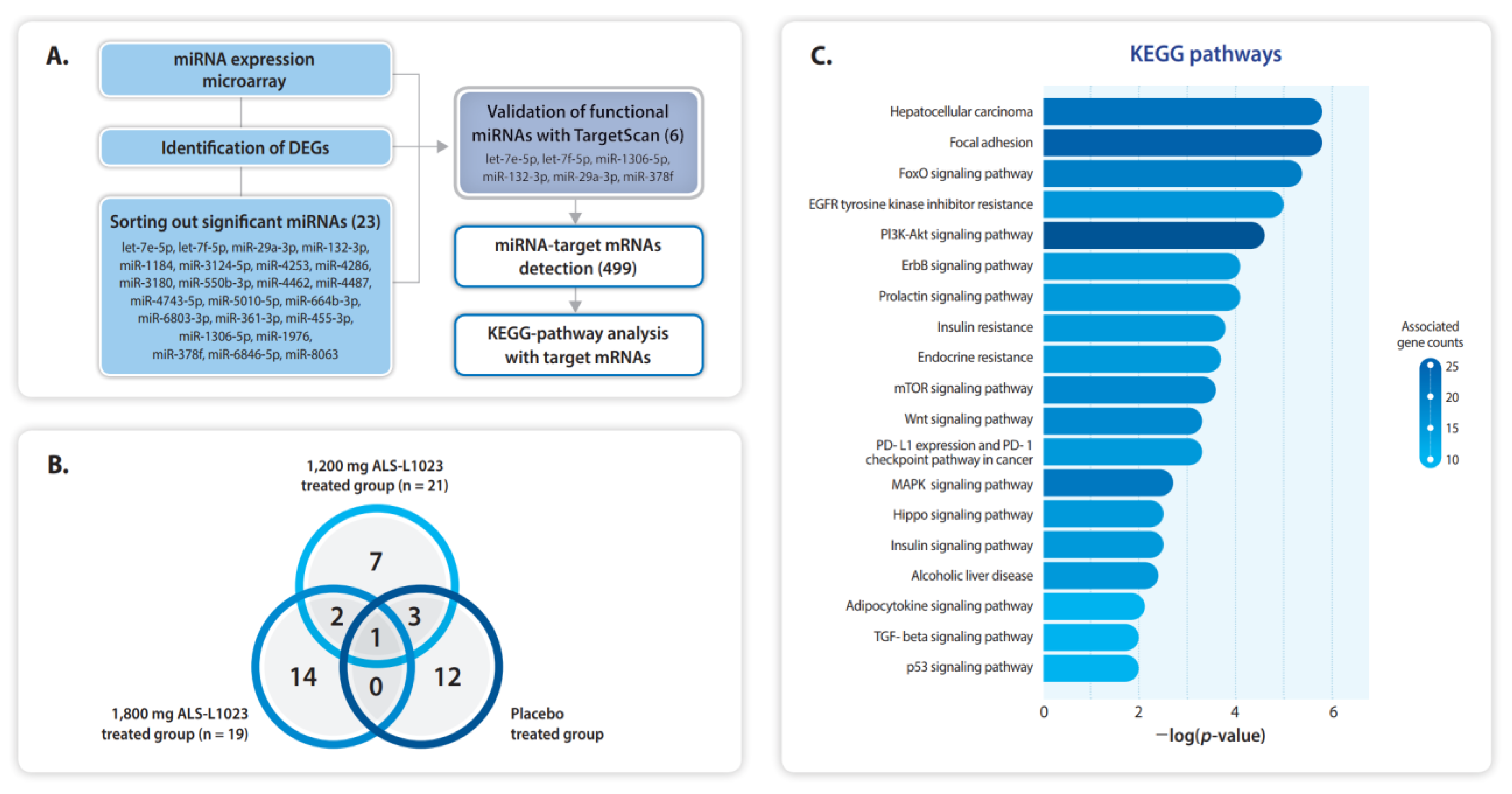
2.6. Selected miRNAs and the Putative Transcripts
3. Discussion
4. Materials and Methods
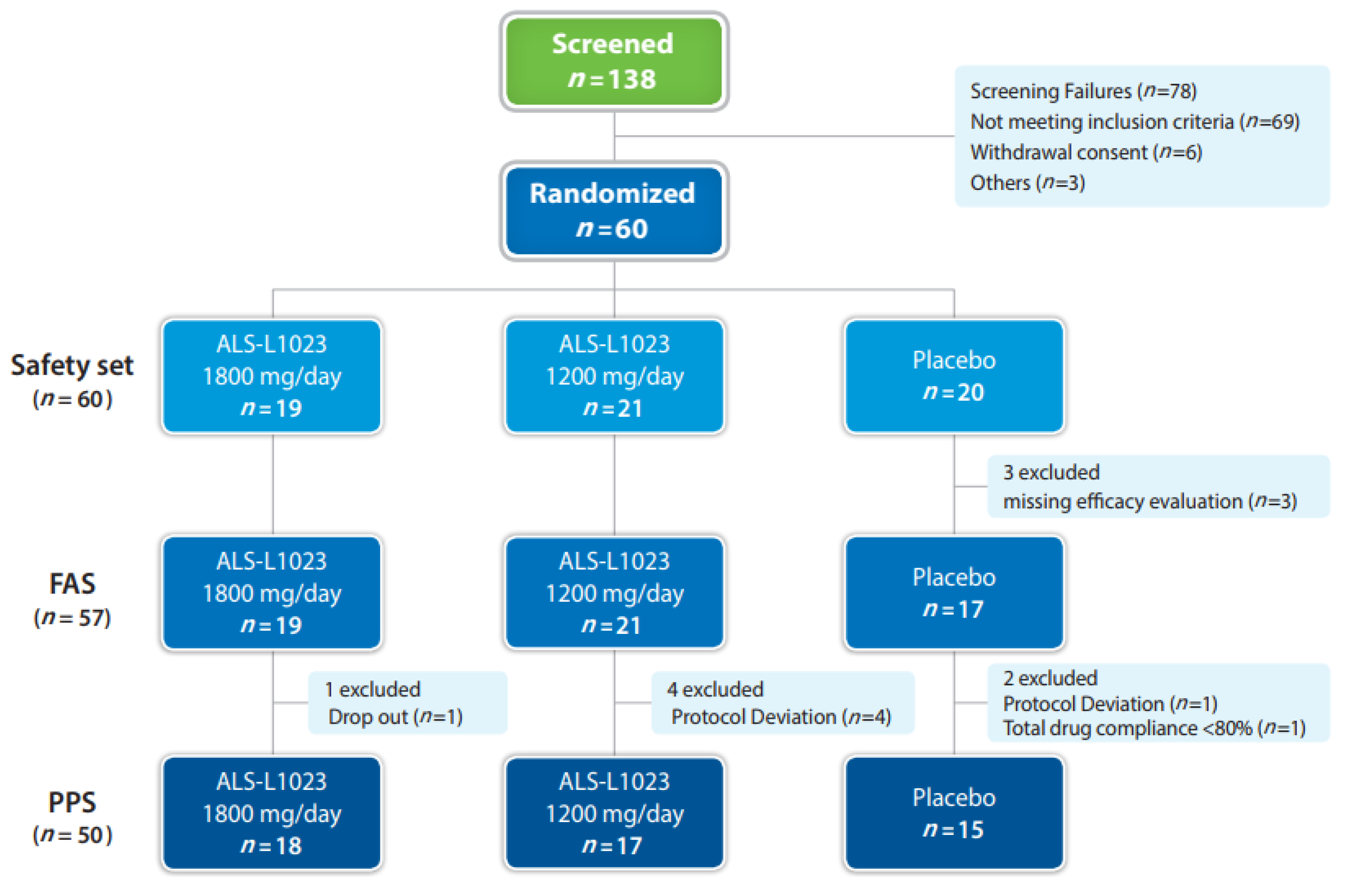
4.1. Study Design
4.2. Inclusion and Exclusion Criteria
4.3. Procedures
4.4. Outcomes
4.5. Assessment of MRI-PDFF and MRE
4.6. miRNA Microarray
4.7. Full Analysis Set and per Protocol Set
4.8. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ye, Q.; Zou, B.; Yeo, Y.H.; Li, J.; Huang, D.Q.; Wu, Y.; Yang, H.; Liu, C.; Kam, L.Y.; Tan, X.X.E.; et al. Global prevalence, incidence, and outcomes of non-obese or lean non-alcoholic fatty liver disease: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 739–752. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Yoon, E.L.; Cho, S.; Lee, C.M.; Kang, B.K.; Park, H.; Jun, D.W.; Nah, E.H. Prevalence of advanced hepatic fibrosis and comorbidity in metabolic dysfunction-associated fatty liver disease in Korea. Liver Int. 2022, 42, 1536–1544. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- Paik, J.M.; Golabi, P.; Younossi, Y.; Mishra, A.; Younossi, Z.M. Changes in the Global Burden of Chronic Liver Diseases from 2012 to 2017: The Growing Impact of NAFLD. Hepatology 2020, 72, 1605–1616. [Google Scholar] [CrossRef] [PubMed]
- Diehl, A.M.; Day, C. Cause, Pathogenesis, and Treatment of Nonalcoholic Steatohepatitis. N. Engl. J. Med. 2017, 377, 2063–2072. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Yoon, E.L.; Kim, M.; Kim, J.H.; Cho, S.; Jun, D.W.; Nah, E.H. Fibrosis Burden of Missed and Added Populations According to the New Definition of Metabolic Dysfunction-Associated Fatty Liver. J. Clin. Med. 2021, 10, 4625. [Google Scholar] [CrossRef] [PubMed]
- Lefere, S.; Devisscher, L.; Geerts, A. Angiogenesis in the progression of non-alcoholic fatty liver disease. Acta Gastroenterol. Belg. 2020, 83, 301–307. [Google Scholar] [PubMed]
- Orlandi, P.; Solini, A.; Banchi, M.; Brunetto, M.R.; Cioni, D.; Ghiadoni, L.; Bocci, G. Antiangiogenic Drugs in NASH: Evidence of a Possible New Therapeutic Approach. Pharmaceuticals 2021, 14, 995. [Google Scholar] [CrossRef] [PubMed]
- Park, B.Y.; Lee, H.; Woo, S.; Yoon, M.; Kim, J.; Hong, Y.; Lee, H.S.; Park, E.K.; Hahm, J.C.; Kim, J.W.; et al. Reduction of Adipose Tissue Mass by the Angiogenesis Inhibitor ALS-L1023 from Melissa officinalis. PLoS ONE 2015, 10, e0141612. [Google Scholar] [CrossRef]
- Kim, J.; Lee, H.; Lim, J.; Oh, J.; Shin, S.S.; Yoon, M. The Angiogenesis Inhibitor ALS-L1023 from Lemon-Balm Leaves Attenuates High-Fat Diet-Induced Nonalcoholic Fatty Liver Disease through Regulating the Visceral Adipose-Tissue Function. Int. J. Mol. Sci. 2017, 18, 846. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, H.; Lim, J.; Lee, H.; Yoon, S.; Shin, S.S.; Yoon, M. The lemon balm extract ALS-L1023 inhibits obesity and nonalcoholic fatty liver disease in female ovariectomized mice. Food Chem. Toxicol. 2017, 106 Pt A, 292–305. [Google Scholar] [CrossRef]
- Shin, Y.; Lee, D.; Ahn, J.; Lee, M.; Shin, S.S.; Yoon, M. The herbal extract ALS-L1023 from Melissa officinalis reduces weight gain, elevated glucose levels and β-cell loss in Otsuka Long-Evans Tokushima fatty rats. J. Ethnopharmacol. 2021, 264, 113360. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Shin, Y.; Jang, J.; Park, Y.; Ahn, J.; Jeong, S.; Shin, S.S.; Yoon, M. The herbal extract ALS-L1023 from Melissa officinalis alleviates visceral obesity and insulin resistance in obese female C57BL/6J mice. J. Ethnopharmacol. 2020, 253, 112646. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Shin, Y.; Roh, J.S.; Ahn, J.; Jeoong, S.; Shin, S.S.; Yoon, M. Lemon Balm Extract ALS-L1023 Regulates Obesity and Improves Insulin Sensitivity via Activation of Hepatic PPARα in High-Fat Diet-Fed Obese C57BL/6J Mice. Int. J. Mol. Sci. 2020, 21, 4256. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.; Bettencourt, R.; Cui, J.; Salotti, J.; Hooker, J.; Bhatt, A.; Hernandez, C.; Nguyen, P.; Aryafar, H.; Valasek, M.; et al. Association of noninvasive quantitative decline in liver fat content on MRI with histologic response in nonalcoholic steatohepatitis. Therap. Adv. Gastroenterol. 2016, 9, 692–701. [Google Scholar] [CrossRef] [PubMed]
- Stine, J.G.; Munaganuru, N.; Barnard, A.; Wang, J.L.; Kaulback, K.; Argo, C.K.; Singh, S.; Fowler, K.J.; Sirlin, C.B.; Loomba, R. Change in MRI-PDFF and Histologic Response in Patients with Nonalcoholic Steatohepatitis: A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2021, 19, 2274–2283.e2275. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Neuschwander-Tetri, B.A.; Sanyal, A.; Chalasani, N.; Diehl, A.M.; Terrault, N.; Kowdley, K.; Dasarathy, S.; Kleiner, D.; Behling, C.; et al. Multicenter Validation of Association between Decline in MRI-PDFF and Histologic Response in NASH. Hepatology 2020, 72, 1219–1229. [Google Scholar] [CrossRef] [PubMed]
- Dulai, P.S.; Sirlin, C.B.; Loomba, R. MRI and MRE for non-invasive quantitative assessment of hepatic steatosis and fibrosis in NAFLD and NASH: Clinical trials to clinical practice. J. Hepatol. 2016, 65, 1006–1016. [Google Scholar] [CrossRef] [PubMed]
- Noureddin, M.; Lam, J.; Peterson, M.R.; Middleton, M.; Hamilton, G.; Le, T.A.; Bettencourt, R.; Changchien, C.; Brenner, D.A.; Sirlin, C.; et al. Utility of magnetic resonance imaging versus histology for quantifying changes in liver fat in nonalcoholic fatty liver disease trials. Hepatology 2013, 58, 1930–1940. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Kang, B.K.; Jun, D.W.; Kim, Y. MR elastography of the liver: Comparison of three measurement methods. Clin. Radiol. 2020, 75, e711–e715. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | ALS-L1023 1800 mg (n = 19) | ALS-L1023 1200 mg (n = 21) | Placebo (n = 20) | p 1 |
|---|---|---|---|---|
| Demographic factors | ||||
| Age, mean ± SD, years | 57.1 ± 13.8 | 51.2 ± 15.0 | 48.3 ± 14.1 | 0.15 |
| Male sex, n (%) | 12 (63.2) | 11 (52.4) | 12 (60.0) | 0.78 |
| Diabetes mellitus, n (%) | 9 (47.4) | 8 (38.1) | 7 (35.0) | 0.72 |
| Hypertension, n (%) | 12 (63.2) | 6 (28.6) | 8 (40.0) | 0.08 |
| Body mass index, median (Q1, Q3), kg/m2 | 29.7 (26.5, 31.6) | 27.8 (26.0, 34.1) | 27.5 (26.2, 31.0) | 0.71 |
| Serum biochemical levels | ||||
| ALT, median (Q1, Q3), U/L | 54.0 (45.0, 89.0) | 65.0 (42.5, 91.0) | 52.5 (34.3, 80.5) | 0.62 |
| AST, median (Q1, Q3), U/L | 46.0 (33.0, 60.0) | 54.0 (33.5, 76.0) | 44.5 (27.3, 64.5) | 0.53 |
| GGT, median (Q1, Q3), U/L | 42.0 (34.0, 92.0) | 70 (41.5, 109.5) | 44.0 (26.5, 61.8) | 0.05 |
| ALP, median (Q1, Q3), U/L | 80.0 (73.0, 95.0) | 77.0 (67.0, 92.5) | 83.5 (62.5, 111.0) | 0.91 |
| Total bilirubin, median (Q1, Q3), U/L | 0.8 (0.6, 1.1) | 0.8 (0.6, 0.8) | 0.8 (0.6, 1.2) | 0.71 |
| Total cholesterol, median (Q1, Q3), mg/dL | 168 (144, 208) | 172 (156, 207) | 182 (150, 206) | 0.99 |
| HDL cholesterol, median (Q1, Q3), mg/dL | 48 (39, 58) | 46 (38, 57) | 46 (41, 52) | 0.77 |
| LDL cholesterol, median (Q1, Q3), mg/dL | 107 (87, 123) | 101 (83, 126) | 113 (87, 136) | 0.69 |
| Triglycerides, median (Q1, Q3), mg/dL | 169 (132, 225) | 140 (111, 178) | 188 (137, 232) | 0.20 |
| Fasting glucose, median (Q1, Q3) | 109 (101, 135) | 97 (89, 122) | 98 (93, 119) | 0.06 |
| Fasting insulin, median (Q1, Q3) | 17.1 (11.6, 28.0) | 23 (12.2, 36.8) | 15.6 (12.3, 24.9) | 0.41 |
| HOMA-IR, median (Q1, Q3) | 4.14 (2.9, 7.0) | 5.38 (3.0, 9.2) | 4.18 (2.8, 5.9) | 0.42 |
| Imaging | ||||
| MRI-PDFF, median (Q1, Q3), % | 14.6 (9.8, 21.5) | 15.7 (10.6, 22.2) | 15.7 (10.9, 20.3) | 0.94 |
| MRI-PDFF, mean ± SD, % | 16.15 ± 6.1 | 17.4 ± 7.6 | 16.9 ± 7.4 | |
| MRE, median (Q1, Q3), kPa | 3.3 (2.7, 3.8) | 3.0 (2.6, 4.5) | 2.9 (2.6, 3.3) | 0.51 |
| MRE, mean ± SD, kPa | 3.3 ± 0.7 | 3.7 ± 1.6 | 3.2 ± 0.8 | |
| Common concomitant medications | ||||
| NSAIDs, n (%) | 3 (15.8%) | 1 (4.8%) | 5 (25.0%) | 0.18 |
| Diabetes medicine, n (%) | 9 (47.4%) | 7 (33.3%) | 7 (35.0%) | 0.62 |
| Proton pump inhibitors, n (%) | 3 (15.8%) | 5 (23.8%) | 4 (20.0%) | 0.92 |
| Statins, n (%) | 11 (57.9%) | 14 (66.7%) | 6 (30.0%) | 0.05 |
| Angiotensin-converting enzyme inhibitors, n (%) | 6 (31.6%) | 3 (14.3%) | 6 (30.0%) | 0.37 |
| ALS-L1023 1800 mg | ALS-L1023 1200 mg | Placebo | p 2 | p 3 | ||||
|---|---|---|---|---|---|---|---|---|
| FAS | Value | p 1 | Value | p 1 | Value | p 1 | ||
| PDFF, (relative) % change from baseline | −15.0 (22.0) | 0.03 | −6.9 (47.0) | 0.49 | 0 (30.0) | 0.23 | 0.95 | 0.65 |
| PDFF, (absolute) change from baseline | −1.6 (4.6) | 0.02 | −1.5 (7.0) | 0.41 | 0 (3.8) | 0.34 | 0.48 | 0.85 |
| Patients with ≥20% PDFF reduction | 7 (38.9) | 8 (40.0) | 5 (29.4) | 0.55 | 0.50 | |||
| Patients with ≥15% PDFF reduction | 9 (50.0) | 9 (45.0) | 5 (29.4) | 0.21 | 0.33 | |||
| Patients with ≥7% PDFF reduction | 12 (66.7) | 10 (50.0) | 8 (47.1) | 0.24 | 0.86 | |||
| PPS | Value | p 1 | Value | p 1 | Value | p 1 | ||
| PDFF, (relative) % change from baseline | −15.0 (22.0) | 0.03 | −9.5 (42.6) | 0.58 | 0.3 (43.1) | 0.52 | 0.49 | 0.99 |
| PDFF, (absolute) change from baseline | −1.6 (4.6) | 0.02 | −1.9 (6.8) | 0.54 | 0.1 (5.1) | 0.43 | 0.94 | |
| Patients with ≥20% PDFF reduction | 7 (38.9) | 7 (41.2) | 4 (26.7) | 0.46 | 0.39 | |||
| Patients with ≥15% PDFF reduction | 9 (50.0) | 8 (47.1) | 4 (26.7) | 0.17 | 0.23 | |||
| Patients with ≥7% PDFF reduction | 12 (66.7) | 9 (52.9) | 6 (40.0) | 0.13 | 0.46 | |||
| ALS-L1023 1800 mg | ALS-L1023 1200 mg | Placebo | p 2 | p 3 | ||||
|---|---|---|---|---|---|---|---|---|
| FAS | Value | p 1 | Value | p 1 | Value | p 1 | ||
| MRE, (relative) % change from baseline | −6.2 (20.1) | 0.23 | −10.7 (17.3) | 0.03 | −7.6 (20.7) | 0.14 | 0.66 | 0.20 |
| MRE, (absolute) change from baseline | −0.3 (0.7) | 0.10 | −0.4 (0.7) | 0.02 | −0.2 (0.6) | 0.12 | >0.99 | 0.36 |
| Patients with ≥20% MRE reduction | 2 (11.1) | 7 (35.0) | 4 (23.5) | 0.40 | 0.45 | |||
| Patients with ≥15% MRE reduction | 5 (27.8) | 8 (40.0) | 5 (29.4) | >0.99 | 0.50 | |||
| Patients with ≥7% MRE reduction | 8 (44.4) | 14 (70.0) | 9 (52.9) | 0.62 | 0.29 | |||
| PPS | Value | p 1 | Value | p 1 | Value | p 1 | ||
| MRE, (relative) % change from baseline | −6.2 (20.1) | −10.1 (17.2) | −11.9 (31.4) | 0.16 | 0.62 | 0.53 | ||
| MRE, (absolute) change from baseline | −0.3 (0.7) | −0.4 (0.6) | −0.4 (0.8) | 0.17 | 0.86 | 0.51 | ||
| Patients with ≥20% MRE reduction | 2 (11.1) | 7 (41.2) | 4 (26.7) | 0.37 | 0.39 | |||
| Patients with ≥15% MRE reduction | 5 (27.8) | 7 (41.2) | 5 (33.3) | 1.00 | 0.65 | |||
| Patients with ≥7% MRE reduction | 8 (44.4) | 12 (70.6) | 9 (60.0) | 0.37 | 0.53 | |||
| ALS-L1023 1800 mg | ALS-L1023 1200 mg | Placebo | p 2 | p 3 | ||||
|---|---|---|---|---|---|---|---|---|
| Value | % CFB | p 1 | % CFB | p 1 | % CFB | p 1 | ||
| ALT, U/L | −12.4 (−30.2, 14.3) | 0.09 | −29.8 (−47.2, 21.9) | 0.12 | −4.9 (−15.4, 27.6) | 0.50 | 0.11 | 0.10 |
| AST, U/L | 0 (−21.7, 25.0) | 0.56 | −19.6 (−41.3, 15.6) | 0.13 | 0 (−16.1, 34.6) | 0.61 | 0.44 | 0.12 |
| GGT, U/L | −7 (−17.0, 15.8) | 0.37 | −6.3 (−40.6, 15.3) | 0.30 | 1.0 (−9.0, 22.6) | 0.92 | 0.43 | 0.35 |
| ALP, U/L | 1.2 (−7.4, 12.5) | 0.90 | −1.7 (−12.1, 5.9) | 0.27 | −3.6 (−19.2, 12.7) | 0.08 | 0.18 | 0.31 |
| Total bilirubin, mg/dL | −5.9 (−16.9, 25.0) | 0.79 | 13.9 (−13.6, 33.0) | 0.07 | 17.2 (−12.3, 60.2) | 0.28 | 0.44 | 0.91 |
| Triglycerides, mg/dL | −15.5 (−29.6,29.9) | 0.16 | −2.8 (−27.6, 11.4) | 0.49 | −21.3 (−32.1, −5.7) | 0.001 | 0.55 | 0.05 |
| TC, mg/dL | 0.9 (−9.1,7.6) | 0.60 | −5.5 (−12.9, 0.0) | <0.01 | 5.4 (−6.3, 7.5) | 0.59 | 0.52 | 0.03 |
| HDL-C, mg/dL | 2.2 (−9.1, 7.7) | 0.97 | −3.3 (−14.0, 11.5) | 0.57 | 2.0 (−4.0, 15.5) | 0.36 | 0.48 | 0.31 |
| LDL-C, mg/dL | −4.1 (−10.1, 9.3) | 0.32 | −4.9 (−21.5, 4.5) | 0.04 | 5.1 (−5.4, 11.1) | 0.82 | 0.45 | 0.15 |
| Pro-C3 | 1.0 (−6.6, 19.0) | 0.62 | −2.0 (−12.6, 23.5) | 0.44 | 0 (−5.3, 17.6) | 0.63 | 0.99 | 0.64 |
| CK-18 | 14.2 (−34.0, 47.0) | 0.59 | 0.4 (−45.8, 32.3) | 0.47 | −12.9 (−23.2, 87.3) | 0.75 | 0.61 | 0.79 |
| HOMA-IR | −2.3 (−25.7, 39.9) | 0.72 | −1.0 (−37.9, 45.2) | 0.54 | 5.0 (−28.0, 33.8) | 0.86 | 0.85 | 0.75 |
| Leptin | −5.9 (−23.8, 15.9) | 0.62 | 2.5 (−14.6, 28.6) | 0.99 | −5.0 (−16.8, 10.2) | 0.43 | 0.55 | 0.75 |
| Ghrelin | 26.8 (0, 152.1) | 0.01 | 34.8 (−12.7, 76.4) | 0.05 | 17.2 (0.0, 90.5) | 0.03 | 0.74 | 0.49 |
| Adiponectin | 7.4 (−21.6, 13.6) | 0.44 | −5.7 (−17.6, 20.8) | 0.63 | 8.6 (−8.5, 5.9) | 0.61 | 0.90 | 0.70 |
| NFS | 11.4 (−30.2, 29.1) | 0.30 | −13.6 (−27.0, 14.4) | 0.08 | 0.9 (−22.5, 28.3) | 0.63 | 0.27 | 0.64 |
| Visceral Fat mass | −8.9 (−30.2, 9.8) | 0.16 | −4.4 (−15.4, 15.1) | 0.94 | −4.9 (−24.5, 10.9) | 0.34 | 0.49 | 0.41 |
| ALS-L1023 1800 mg (n = 19) | ALS-L1023 1200 mg (n = 21) | Placebo (n = 20) | |
|---|---|---|---|
| Safety overview | |||
| Any adverse events | 8 (42.1) | 13 (61.9) | 8 (40.0) |
| Grade 3–4 adverse events | 0 (0) | 0 (0) | 0 (0) |
| Serious adverse events | 0 (0) | 0(0) | 1 (5.0) |
| Adverse event leading to discontinuation of any study drug | 0 (0) | 0(0) | 1 (5.0) |
| Death | 0 (0) | 0 (0) | 0 (0) |
| Most common adverse events | |||
| Fatigue | 1(5.3) | 0 (0) | 1 (5.0) |
| Dyspepsia | 1(5.3) | 3 (14.3) | 2 (10.0) |
| Abdominal distension | 0 (0) | 2 (9.5) | 0 (0) |
| Abdominal pain | 1 (5.3) | 1 (4.8) | 0 (0) |
| Dry eye | 1 (5.3) | 0 (0) | 0 (0) |
| Pulpitis dental | 0 (0) | 1 (4.8) | 0 (0) |
| Nasopharyngitis | 1 (5.3) | 0 (0) | 1 (5.0) |
| Urinary tract infection | 1 (5.3) | 3 (14.3) | 2 (10.0) |
| Chest discomfort | 1 (5.3) | 1 (4.8) | 1 (5.0) |
| Intervertebral disc disorder | 1 (5.3) | 0 (0) | 0 (0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, G.-A.; Cho, H.C.; Jeong, S.W.; Kang, B.-K.; Kim, M.; Jung, S.; Hwang, J.; Yoon, E.L.; Jun, D.W. A Phase 2a, Randomized, Double-Blind, Placebo-Controlled Study to Assess the Efficacy and Safety of ALS-L1023 in Non-Alcoholic Fatty Liver Disease. Pharmaceuticals 2023, 16, 623. https://doi.org/10.3390/ph16040623
Kim G-A, Cho HC, Jeong SW, Kang B-K, Kim M, Jung S, Hwang J, Yoon EL, Jun DW. A Phase 2a, Randomized, Double-Blind, Placebo-Controlled Study to Assess the Efficacy and Safety of ALS-L1023 in Non-Alcoholic Fatty Liver Disease. Pharmaceuticals. 2023; 16(4):623. https://doi.org/10.3390/ph16040623
Chicago/Turabian StyleKim, Gi-Ae, Hyun Chin Cho, Soung Won Jeong, Bo-Kyeong Kang, Mimi Kim, Seungwon Jung, Jungwook Hwang, Eileen L. Yoon, and Dae Won Jun. 2023. "A Phase 2a, Randomized, Double-Blind, Placebo-Controlled Study to Assess the Efficacy and Safety of ALS-L1023 in Non-Alcoholic Fatty Liver Disease" Pharmaceuticals 16, no. 4: 623. https://doi.org/10.3390/ph16040623