
Cost-Effectiveness of Targeted Prophylaxis among Allogenic Stem Cell Transplant Recipients

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
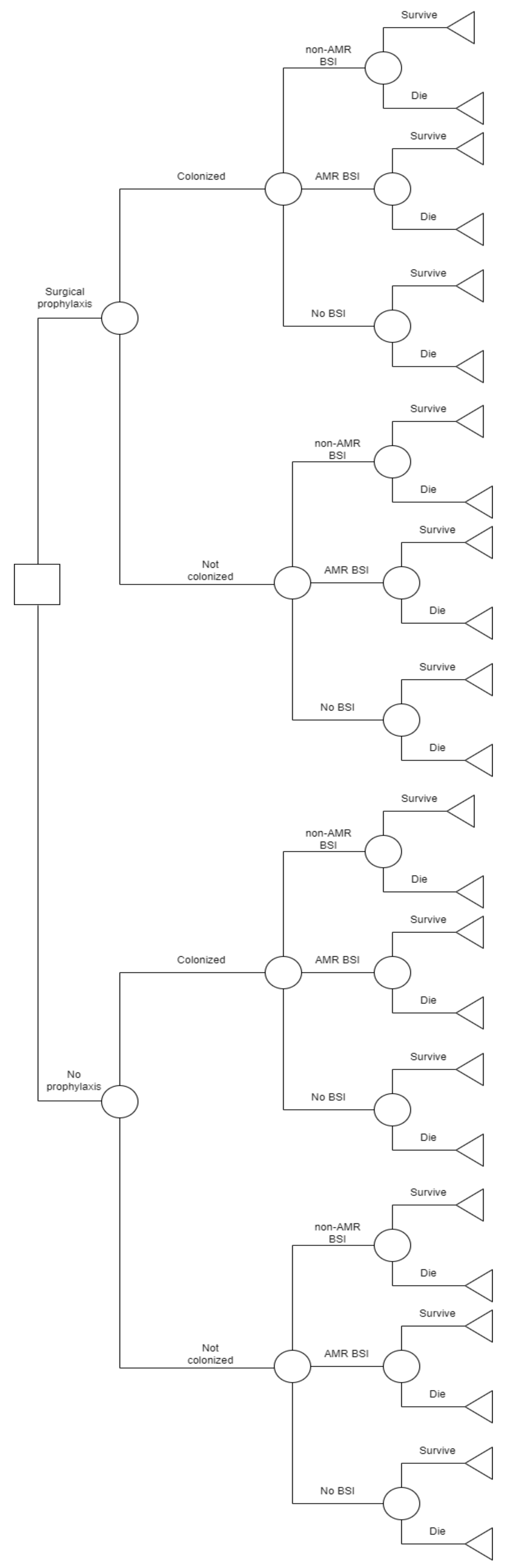
2.1. Study Design and Definitions
2.2. Microbiology Detection Methods
2.3. Costs and Utilities
2.4. Statistical Analysis
3. Results
3.1. Cost-Effectiveness Analysis
3.2. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kokkayil, P.; Agarwal, R.; Mohapatra, S.; Bakshi, S.; Das, B.; Sood, S.; Dhawan, B.; Kapil, A. Bacterial profile and antibiogram of blood stream infections in febrile neutropenic patients with haematological malignancies. J. Infect. Dev. Ctries. 2018, 12, 442–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNamara, J.F.; Righi, E.; Wright, H.; Hartel, G.F.; Harris, P.N.; Paterson, D.L. Long-term morbidity and mortality following bloodstream infection: A systematic literature review. J. Infect. 2018, 77, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bordino, V.; Vicentini, C.; D’Ambrosio, A.; Quattrocolo, F.; Zotti, C.; Novati, R.; Sticchi, C.; Bersani, M.; Fedeli, U.; Fabbri, L.; et al. Burden of healthcare-associated infections in Italy: Incidence, attributable mortality and disability-adjusted life years (DALYs) from a nationwide study, 2016. J. Hosp. Infect. 2021, 113, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Gudiol, C.; Tubau, F.; Calatayud, L.; Garcia-Vidal, C.; Cisnal, M.; Sanchez-Ortega, I.; Duarte, R.; Calvo, M.; Carratala, J. Bacteraemia due to multidrug-resistant Gram-negative bacilli in cancer patients: Risk factors, antibiotic therapy and outcomes. J. Antimicrob. Chemother. 2011, 66, 657–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Baño, J.; Picón, E.; Gijón, P.; Hernández, J.R.; Cisneros, J.M.; Peña, C.; Almela, M.; Almirante, B.; Grill, F.; Colomina, J.; et al. Risk factors and prognosis of nosocomial bloodstream infections caused by extended-spectrum-beta-lactamase-producing Escherichia coli. J. Clin. Microbiol. 2010, 48, 1726–1731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuderer, N.M.; Dale, D.C.; Crawford, J.; Cosler, L.E.; Lyman, G.H. Mortality, morbidity, and cost associated with febrile neutropenia in adult cancer patients. Cancer 2006, 106, 2258–2266. [Google Scholar] [CrossRef] [PubMed]
- Feld, R. Bloodstream infections in cancer patients with febrile neutropenia. Int. J. Antimicrob. Agents 2008, 32, S30–S33. [Google Scholar] [CrossRef]
- Andremont, A.; Lancar, R.; Lê, N.A.; Hattchouel, J.-M.; Baron, S.; Tavakoli, T.; Daniel, M.-F.; Tancrède, C.; Lê, M.G. Secular trends in mortality associated with bloodstream infections in 4268 patients hospitalized in a cancer referral left between 1975 and 1989. Clin. Microbiol. Infect. 1996, 1, 160–167. [Google Scholar] [CrossRef] [Green Version]
- Tsering, L.T.; Barola, S.; Chandra, A.B. Assessing Bacterial Isolates in Bloodstream Infections and Trend of the Antimicrobial Resistance in the Hematological and Solid Malignancies. Blood 2015, 126, 5628. [Google Scholar] [CrossRef]
- Mikulska, M.; Del Bono, V.; Raiola, A.M.; Bruno, B.; Gualandi, F.; Occhini, D.; di Grazia, C.; Frassoni, F.; Bacigalupo, A.; Viscoli, C. Blood Stream Infections in Allogeneic Hematopoietic Stem Cell Transplant Recipients: Reemergence of Gram-Negative Rods and Increasing Antibiotic Resistance. Biol. Blood Marrow Transplant. 2009, 15, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Mikulska, M.; Averbuch, D.; Tissot, F.; Cordonnier, C.; Akova, M.; Calandra, T.; Ceppi, M.; Bruzzi, P.; Viscoli, C.; Aljurf, M.; et al. Fluoroquinolone prophylaxis in haematological cancer patients with neutropenia: ECIL critical appraisal of previous guidelines. J. Infect. 2018, 76, 20–37. [Google Scholar] [CrossRef] [PubMed]
- Bucaneve, G.; Castagnola, E.; Viscoli, C.; Leibovici, L.; Menichetti, F. Quinolone prophylaxis for bacterial infections in afebrile high risk neutropenic patients. Eur. J. Cancer Suppl. 2007, 5, 5–12. [Google Scholar] [CrossRef]
- Hughes, W.T.; Armstrong, D.; Bodey, G.P.; Bow, E.J.; Brown, A.E.; Calandra, T.; Feld, R.; Pizzo, P.A.; Rolston, K.V.I.; Shenep, J.L.; et al. 2002 guidelines for the use of antimicrobial agents in neutropenic patients with cancer. Clin. Infect. Dis. 2002, 34, 730–751. [Google Scholar] [CrossRef] [Green Version]
- Kanafani, Z.; Mehiosibai, A.; Araj, G.; Kanaan, M.; Kanj, S. Epidemiology and risk factors for extended-spectrum β-lactamase-producing organisms: A case control study at a tertiary care center in Lebanon. Am. J. Infect. Control 2005, 33, 326–332. [Google Scholar] [CrossRef]
- Lautenbach, E.; Patel, J.B.; Bilker, W.B.; Edelstein, P.H.; Fishman, N.O. Extended-Spectrum β-Lactamase-Producing Escherichia coli and Klebsiella pneumoniae: Risk Factors for Infection and Impact of Resistance on Outcomes. Clin. Infect. Dis. 2001, 32, 1162–1171. [Google Scholar] [CrossRef] [PubMed]
- Colodner, R.; Rock, W.; Chazan, B.; Keller, N.; Guy, N.; Sakran, W.; Raz, R. Risk Factors for the Development of Extended-Spectrum Beta-Lactamase-Producing Bacteria in Nonhospitalized Patients. Eur. J. Clin. Microbiol. Infect. Dis. 2004, 23, 163–167. [Google Scholar] [CrossRef]
- Gafter-Gvili, A.; Fraser, A.; Paul, M.; Leibovici, L. Meta-analysis: Antibiotic prophylaxis reduces mortality in neutropenic patients. Ann. Intern. Med. 2005, 142 Pt 1, 979–995. [Google Scholar] [CrossRef]
- Cullen, M.; Steven, N.; Billingham, L.; Gaunt, C.; Hastings, M.; Simmonds, P.; Stuart, N.; Rea, D.; Bower, M.; Fernando, I.; et al. Antibacterial Prophylaxis after Chemotherapy for Solid Tumors and Lymphomas. N. Engl. J. Med. 2005, 353, 988–998. [Google Scholar] [CrossRef] [Green Version]
- Bucaneve, G.; Micozzi, A.; Menichetti, F.; Martino, P.; Dionisi, M.S.; Martinelli, G.; Allione, B.; D’Antonio, D.; Buelli, M.; Nosari, A.M.; et al. Levofloxacin to prevent bacterial infection in patients with cancer and neutropenia. N. Engl. J. Med. 2005, 353, 977–987. [Google Scholar] [CrossRef] [Green Version]
- Memorial Sloan-Kettering Cancer Center. Prevention and Treatment of Cancer-Related Infections. J. Natl. Compr. Cancer Netw. 2008, 6, 122. [Google Scholar] [CrossRef]
- Slavin, M.; Lingaratnam, S.; Mileshkin, L.; Booth, D.L.; Cain, M.J.; Ritchie, D.S.; Wei, A.; Thursky, K.A. Use of antibacterial prophylaxis for patients with neutropenia. Australian Consensus Guidelines 2011 Steering Committee. Intern. Med. J. 2011, 41, 102–109. [Google Scholar] [CrossRef] [PubMed]
- RPubs. Decision Tree Model in R Tutorial. Available online: https://rpubs.com/mbounthavong/decision_tree_model_tutorial (accessed on 30 October 2022).
- Life Expectancy at Birth, Total (Years)—Italy. Data. Available online: https://data.worldbank.org/indicator/SP.DYN.LE00.IN?locations=IT (accessed on 31 October 2022).
- Bhatia, S.; Dai, C.; Landier, W.; Hageman, L.; Wu, J.; Schlichting, E.; Siler, A.; Funk, E.; Hicks, J.; Bosworth, A.; et al. Trends in Late Mortality and Life Expectancy After Allogeneic Blood or Marrow Transplantation Over 4 Decades: A Blood or Marrow Transplant Survivor Study Report. JAMA Oncol. 2021, 7, 1626–1634. [Google Scholar] [CrossRef] [PubMed]
- Kamiński, B.; Jakubczyk, M.; Szufel, P. A framework for sensitivity analysis of decision trees. Central Eur. J. Oper. Res. 2017, 26, 135–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AR-ISS: Sorveglianza Nazionale dell’Antibiotico-Resistenza. Available online: https://www.epicentro.iss.it/antibiotico-resistenza/ar-iss/RIS-1_2021.pdf (accessed on 31 January 2023).
- Seremi. Servizio di Riferimento Regionale di Epidemiologia per la Sorveglianza, la Prevenzione e il Controllo delle Malattie Infettive. Available online: https://www.seremi.it/ (accessed on 31 January 2023).
- McCormick, M.; Friehling, E.; Kalpatthi, R.; Smith, K. Levofloxacin Prophylaxis Is Effective and Cost-Effective in Pediatric Patients with Acute Myeloid Leukemia. Blood 2019, 134 (Suppl. S1), 335. [Google Scholar] [CrossRef]
- McCormick, M.; Friehling, E.; Kalpatthi, R.; Siripong, N.; Smith, K. Cost-Effectiveness of Levofloxacin Prophylaxis Against Bacterial Infection in Pediatric Patients with Acute Myeloid Leukemia. Pediatr. Blood Cancer 2020, 67, e28469. [Google Scholar] [CrossRef] [PubMed]
- Pagano, L.; Caira, M.; Nosari, A.; Rossi, G.; Viale, P.; Aversa, F.; Tumbarello, M. Etiology of Febrile Episodes in Patients with Acute Myeloid Leukemia: Results from the Hema e-Chart Registry. Arch. Intern. Med. 2011, 171, 1502–1503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fadda, G.; Nicoletti, G.; Schito, G.; Tempera, G. Antimicrobial Susceptibility Patterns of Contemporary Pathogens from Uncomplicated Urinary Tract Infections Isolated in a Multicenter Italian Survey: Possible Impact on Guidelines. J. Chemother. 2005, 17, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, L.; Bapat, A.; Drumright, L.N.; Lambourne, J.; Jimenez-England, F.G.; Aries, J.; Eccersley, L.; Hallam, S.; Montoto, S.; Oakervee, H.; et al. Cessation of Ciprofloxacin Prophylaxis in Hemato-Oncology Patients. Clin. Infect. Dis. 2022, 75, 178–179. [Google Scholar] [CrossRef]
- Abushaheen, M.A.; Muzaheed; Fatani, A.J.; Alosaimi, M.; Mansy, W.; George, M.; Acharya, S.; Rathod, S.; Divakar, D.D.; Jhugroo, C.; et al. Antimicrobial resistance, mechanisms and its clinical significance. Dis. Mon. 2020, 66, 100971. [Google Scholar] [CrossRef]
- Raso, R.; di Pietrantonj, C.; Zottarelli, F.; Rocchetti, A.; Leli, C. Sorveglianza Delle Batteriemie Da Enterobatteri Resistenti Ai Carbapenemi (CRE). Istituto Superiore di Sanità 2022, 11. Available online: https://www.iss.it/-/rapporto-iss-sorveglianza-ris-2/2022-cre-sorveglianza-nazionale-delle-batteriemie-da-enterobatteri-resistenti-ai-carbapenemi.-dati-2021.-simone-iacchini-alessandra-caramia-giulia-fadda-monica-monaco-giulia-errico-maria-del-grosso-maria-giufr%C3%A8-annalis (accessed on 20 March 2023).
- Shbaklo, N.; Corcione, S.; Vicentini, C.; Giordano, S.; Fiorentino, D.; Bianco, G.; Cattel, F.; Cavallo, R.; Zotti, C.M.; De Rosa, F.G. An Observational Study of MDR Hospital-Acquired Infections and Antibiotic Use during COVID-19 Pandemic: A Call for Antimicrobial Stewardship Programs. Antibiotics 2022, 11, 695. [Google Scholar] [CrossRef] [PubMed]
- Gyssens, I.C.; Kern, W.V.; Livermore, D.M. The role of antibiotic stewardship in limiting antibacterial resistance among hematology patients. Haematologica 2013, 98, 1821–1825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantón, R.; Akóva, M.; Carmeli, Y.; Giske, C.; Glupczynski, Y.; Gniadkowski, M.; Livermore, D.; Miriagou, V.; Naas, T.; Rossolini, G.; et al. Rapid evolution and spread of carbapenemases among Enterobacteriaceae in Europe. Clin. Microbiol. Infect. 2012, 18, 413–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marston, H.D.; Dixon, D.M.; Knisely, J.M.; Palmore, T.N.; Fauci, A.S. Antimicrobial Resistance. JAMA 2016, 316, 1193–1204. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Input | Frequency | Percentage | 95% CI |
|---|---|---|---|
| I. Probabilities | |||
| FQP | |||
| Colonization KPC/ESBL: | 7 | 6.8% | 2.78–13.5 |
| BSI rate in colonized: | |||
| 4 | 57.97% | 20.48–93.8 |
| 3 | 42.03% | 9.9–81.4 |
| 0 | 0 | |
| BSI rate in not colonized: | |||
| 61 | 63.5% | 53–73 |
| 27 | 28% | 19.4–38.2 |
| 8 | 8.3% | 3.6–15.7 |
| No prophylaxis | |||
| Colonization KPC/ESBL: | 62 | 29.18% | 23.33–36.03 |
| BSI rate in colonized: | |||
| 25 | 40% | 28–53.5 |
| 19 | 30.6% | 19.5–43.6 |
| 18 | 29% | 18.2–41.9 |
| BSI rate in not colonized: | |||
| 79 | 53% | 44.6–61.2 |
| 66 | 44% | 36.17–52.6 |
| 4 | 2.6% | 0.74–6.7 |
| Mortality rate | |||
| 67 | 20.81% | 15.02–27.63 |
| 82 | 25.49% | 18.8–33.16 |
| 111 | 34.38% | 18.57–53.19 |
| II. Costs | |||
| Length of stay | Median (days) | IQR | |
| 32 | 29–37.75 | |
| 35 | 30–44 | |
| 35.5 | 32–43 | |
| Mean (132€) | IQR | |
| 4224 | 3828–4983 | |
| 4620 | 3960–5808 | |
| 4686 | 4224–5676 | |
| Surgical prophylaxis | 0.57€ | ||
| III. Effects | |||
| 3% discounting | 8.42 LY gained | ||
| Strategy | Cost, € | Incremental Cost, € | Effect (Life-Years Gained) | Incremental Effect (Life-Years Gained) | C/E | INCREMENTAL C/E (ICER per LY Gained) |
|---|---|---|---|---|---|---|
| FQP | 4375.26 | 56 | 6.46 | 677.28 | Dominated | |
| No FQP | 4431.26 | 6.39 | −0.07 | 693.47 | Dominant |
| Strategy | Range Cost, € | Range Incremental Cost | Range Effect (Life-Years Gained) | Range Incremental Effect |
|---|---|---|---|---|
| FQP | 4343.52–4412.9 | −87.74–−18.36 | 6.28–6.63 | −0.11–0.24 |
| No FQP | 4408.87–4455.85 | 33.61–80.59 | 6.35–6.43 | −0.11–−0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shbaklo, N.; Vicentini, C.; Busca, A.; Giaccone, L.; Dellacasa, C.; Dogliotti, I.; Lupia, T.; Zotti, C.M.; Corcione, S.; De Rosa, F.G. Cost-Effectiveness of Targeted Prophylaxis among Allogenic Stem Cell Transplant Recipients. Pharmaceuticals 2023, 16, 466. https://doi.org/10.3390/ph16030466
Shbaklo N, Vicentini C, Busca A, Giaccone L, Dellacasa C, Dogliotti I, Lupia T, Zotti CM, Corcione S, De Rosa FG. Cost-Effectiveness of Targeted Prophylaxis among Allogenic Stem Cell Transplant Recipients. Pharmaceuticals. 2023; 16(3):466. https://doi.org/10.3390/ph16030466
Chicago/Turabian StyleShbaklo, Nour, Costanza Vicentini, Alessandro Busca, Luisa Giaccone, Chiara Dellacasa, Irene Dogliotti, Tommaso Lupia, Carla M. Zotti, Silvia Corcione, and Francesco Giuseppe De Rosa. 2023. "Cost-Effectiveness of Targeted Prophylaxis among Allogenic Stem Cell Transplant Recipients" Pharmaceuticals 16, no. 3: 466. https://doi.org/10.3390/ph16030466