
Insulin Resistance and Acne: The Role of Metformin as Alternative Therapy in Men
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
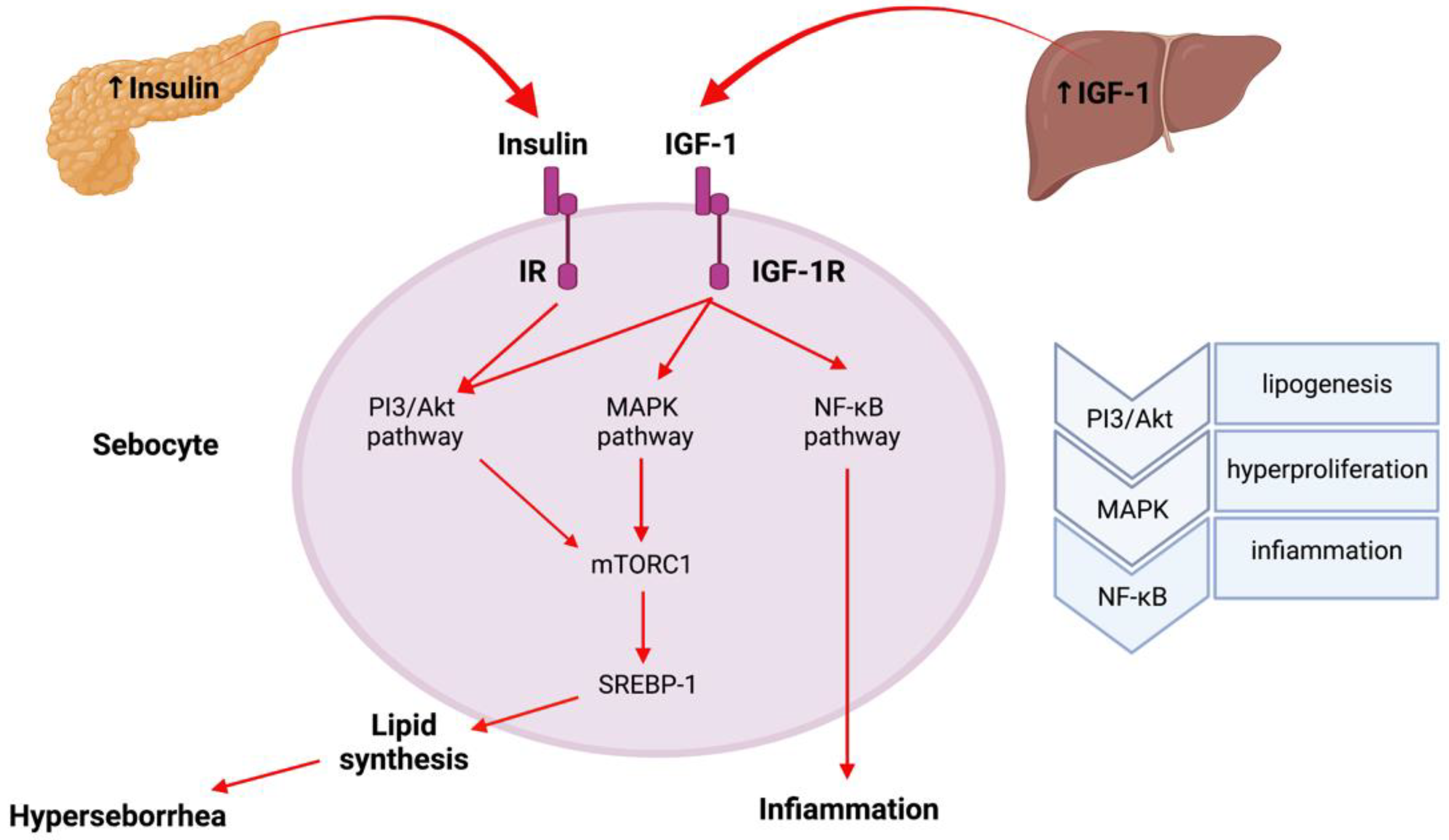
2. Insulin Resistance, IGF-1 and IGFBP-3
3. Metformin and Acne
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Emiroğlu, N.; Cengiz, F.P.; Kemeriz, F. Original paper Insulin resistance in severe acne vulgaris. Adv. Dermatol. Allergol. 2015, 4, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Thappa, D.; Adityan, B.; Kumari, R. Scoring systems in acne vulgaris. Indian J. Dermatol. Venereol. Leprol. 2009, 75, 323. [Google Scholar] [CrossRef]
- Balta, I.; Ekiz, O.; Ozuguz, P.; Ustun, I.; Karaca, S.; Dogruk Kacar, S.; Eksioglu, M. Insulin resistance in patients with post-adolescent acne. Int. J. Dermatol. 2015, 54, 662–666. [Google Scholar] [CrossRef]
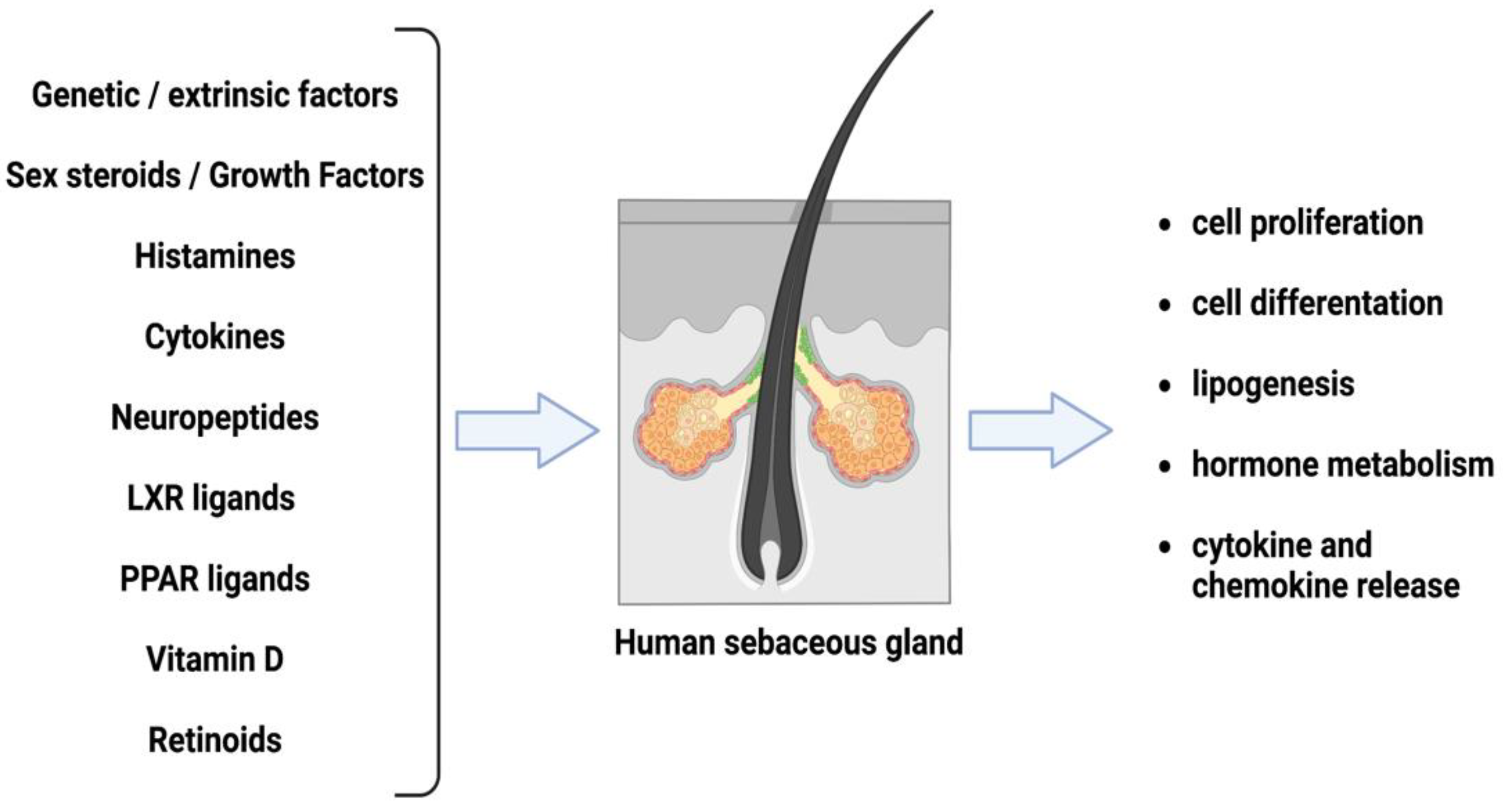
- Makrantonaki, E.; Ganceviciene, R.; Zouboulis, C.C. An update on the role of the sebaceous gland in the pathogenesis of acne. Dermatoendocrinol. 2011, 3, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Thody, A.J.; Shuster, S. Control and function of sebaceous glands. Physiol. Rev. 1989, 69, 383–416. [Google Scholar] [CrossRef] [PubMed]
- Lovászi, M.; Szegedi, A.; Zouboulis, C.C.; Törőcsik, D. Sebaceous-immunobiology is orchestrated by sebum lipids. Dermatoendocrinology 2017, 9, e1375636. [Google Scholar] [CrossRef] [Green Version]
- Yeh, S.; Tsai, M.Y.; Xu, Q.; Mu, X.M.; Lardy, H.; Huang, K.E.; Lin, H.; Yeh, S.D.; Altuwaijri, S.; Zhou, X.; et al. Generation and characterization of androgen receptor knockout (ARKO) mice: An in vivo model for the study of androgen functions in selective tissues. Proc. Natl. Acad. Sci. USA 2002, 99, 13498–13503. [Google Scholar] [CrossRef] [Green Version]
- Kimura, S.; Matsumoto, T.; Matsuyama, R.; Shiina, H.; Sato, T.; Takeyama, K.I.; Kato, S. Androgen receptor function in folliculogenesis and its clinical implication in premature ovarian failure. Trends Endocrinol. Metab. 2007, 18, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zouboulis, C.C.; Fritsch, M.; Blume-Peytavi, U.; Kodelja, V.; Goerdt, S.; Luu-The, V.; Orfanos, C.E. Evidence of Heterogeneity and Quantitative Differences of the Type 1 5α-Reductase Expression in Cultured Human Skin Cells—Evidence of its Presence in Melanocytes. J. Investig. Dermatol. 1998, 110, 84–89. [Google Scholar] [CrossRef] [Green Version]
- Zouboulis, C.; Chen, W.-C.; Thornton, M.; Qin, K.; Rosenfield, R. Sexual Hormones in Human Skin. Horm. Metab. Res. 2007, 39, 85–95. [Google Scholar] [CrossRef]
- Lembo, S.; Di Caprio, R.; Balato, A.; Caiazzo, G.; Fabbrocini, G.; Skroza, N.; Tolino, E.; Potenza, C. The increase of mTOR expression is consistent with FoxO1 decrease at gene level in acne but not in psoriasis. Arch. Dermatol. Res. 2020, 312, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Melnik, B.C.; Zouboulis, C.C. Potential role of FoxO1 and m TORC1 in the pathogenesis of Western diet-induced acne. Exp. Dermatol. 2013, 22, 311–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agamia, N.F.; Abdallah, D.M.; Sorour, O.; Mourad, B.; Younan, D.N. Skin expression of mammalian target of rapamycin and forkhead box transcription factor O1, and serum insulin-like growth factor-1 in patients with acne vulgaris and their relationship with diet. Br. J. Dermatol. 2016, 174, 1299–1307. [Google Scholar] [CrossRef] [PubMed]
- Fritsch, M.; Orfanos, C.E.; Zouboulis, C.C. Sebocytes are the Key Regulators of Androgen Homeostasis in Human Skin. J. Investig. Dermatol. 2001, 116, 793–800. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Thiboutot, D.; Zouboulis, C.C. Cutaneous Androgen Metabolism: Basic Research and Clinical Perspectives. J. Investig. Dermatol. 2002, 119, 992–1007. [Google Scholar] [CrossRef] [Green Version]
- Uemura, M.; Tamura, K.; Chung, S.; Honma, S.; Okuyama, A.; Nakamura, Y.; Nakagawa, H. Novel 5α-steroid reductase (SRD5A3, type-3) is overexpressed in hormone-refractory prostate cancer. Cancer Sci. 2007, 99, 81–86. [Google Scholar] [CrossRef]
- Samson, M.; Labrie, F.; Zouboulis, C.C.; Luu-The, V. The Biosynthesis of Dihydrotestosterone by a Pathway that Does Not Require Testosterone as an Intermediate in the SZ95 Sebaceous Gland Cell Line. J. Investig. Dermatol. 2010, 130, 602–604. [Google Scholar] [CrossRef]
- Chen, W.; Zouboulis, C.C.; Orfanos, C.E. The 5α-Recluctase System and Its Inhibitors. Dermatology 1996, 193, 177–184. [Google Scholar] [CrossRef]
- Cantagrel, V.; Lefeber, D.J.; Ng, B.G.; Guan, Z.; Silhavy, J.L.; Bielas, S.L.; Lehle, L.; Hombauer, H.; Adamowicz, M.; Swiezewska, E.; et al. SRD5A3 Is Required for Converting Polyprenol to Dolichol and Is Mutated in a Congenital Glycosylation Disorder. Cell 2010, 142, 203–217. [Google Scholar] [CrossRef] [Green Version]
- Imperato-McGinley, J.; Gautier, T.; Cai, L.Q.; Yee, B.; Epstein, J.; Pochi, P. The androgen control of sebum production. Studies of subjects with dihydrotestosterone deficiency and complete androgen insensitivity. J. Clin. Endocrinol. Metab. 1993, 76, 524–528. [Google Scholar] [CrossRef]
- Seiffert, K.; Seltmann, H.; Fritsch, M.; Zouboulis, C. Inhibition of 5α-Reductase Activity in SZ95 Sebocytes and HaCaT Keratinocytes In Vitro. Horm. Metab. Res. 2007, 39, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Leyden, J.; Bergfeld, W.; Drake, L.; Dunlap, F.; Goldman, M.P.; Gottlieb, A.B.; Heffernan, M.P.; Hickman, J.G.; Hordinsky, M.; Jarrett, M.; et al. A systemic type i 5 α-reductase inhibitor is ineffective in the treatment of acne vulgaris. J. Am. Acad. Dermatol. 2004, 50, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Gilliver, S.C.; Ashworth, J.J.; Mills, S.J.; Hardman, M.J.; Ashcroft, G.S. Androgens modulate the inflammatory response during acute wound healing. J. Cell Sci. 2006, 119, 722–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belgorosky, A.; Baquedano, M.S.; Guercio, G.; Rivarola, M.A. Adrenarche: Postnatal Adrenal Zonation and Hormonal and Metabolic Regulation. Horm. Res. Paediatr. 2008, 70, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Laganà, A.S.; Rossetti, P.; Buscema, M.; La Vignera, S.; Condorelli, R.A.; Gullo, G.; Granese, R.; Triolo, O. Metabolism and Ovarian Function in PCOS Women: A Therapeutic Approach with Inositols. Int. J. Endocrinol. 2016, 2016, 6306410. [Google Scholar] [CrossRef] [Green Version]
- Borisov, N.; Aksamitiene, E.; Kiyatkin, A.; Legewie, S.; Berkhout, J.; Maiwald, T.; Kaimachnikov, N.P.; Timmer, J.; Hoek, J.B.; Kholodenko, B.N. N. Systems-level interactions between insulin–EGF networks amplify mitogenic signaling. Mol. Syst. Biol. 2009, 5, 256. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, H.; Tan, J. Effects of Diet on Acne and Its Response to Treatment. Am. J. Clin. Dermatol. 2021, 22, 55–65. [Google Scholar] [CrossRef]
- Smith, R.N.; Mann, N.J.; Braue, A.; Mäkeläinen, H.; Varigos, G.A. A low-glycemic-load diet improves symptoms in acne vulgaris patients: A randomized controlled trial. Am. J. Clin. Nutr. 2007, 86, 107–115. [Google Scholar] [CrossRef] [Green Version]
- Andreadi, A.; Bellia, A.; Di Daniele, N.; Meloni, M.; Lauro, R.; Della-Morte, D.; Lauro, D. The molecular link between oxidative stress, insulin resistance, and type 2 diabetes: A target for new therapies against cardiovascular diseases. Curr. Opin. Pharmacol. 2022, 62, 85–96. [Google Scholar] [CrossRef]
- Berra, B.; Rizzo, A.M. Glycemic Index, Glycemic Load: New Evidence for a Link with Acne. J. Am. Coll. Nutr. 2009, 28 (Suppl. S4), 450S–454S. [Google Scholar] [CrossRef]
- Chiu, A.; Chon, S.Y.; Kimball, A.B. The Response of Skin Disease to Stress: Changes in the Severity of Acne Vulgaris as Affected by Examination Stress. Arch. Dermatol. 2003, 139, 897–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pryor, P.R.; Liu, S.C.; Clark, A.E.; Yang, J.; Holman, G.D.; Tosh, D. Chronic insulin effects on insulin signalling and GLUT4 endocytosis are reversed by metformin. Biochem. J. 2000, 348 Pt 1, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Horton, R.; Pasupuletti, V.; Antonipillai, I. Androgen induction of steroid 5 alpha-reductase may be mediated via insulin-like growth factor-I. Endocrinology 1993, 133, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Kumari, R.; Thappa, D. Role of insulin resistance and diet in acne. Indian J. Dermatol. Venereol. Leprol. 2013, 79, 291. [Google Scholar] [CrossRef]
- Zhang, L.; Li, W.H.; Anthonavage, M.; Pappas, A.; Rossetti, D.; Cavender, D.; Seiberg, M.; Eisinger, M. Melanocortin-5 receptor and sebogenesis. Eur. J. Pharmacol. 2011, 660, 202–206. [Google Scholar] [CrossRef]
- Im, M.; Kim, S.Y.; Sohn, K.C.; Choi, D.K.; Lee, Y.; Seo, Y.J.; Kim, C.D.; Hwang, Y.L.; Zouboulis, C.C.; Lee, J.H. Epigallocatechin-3-Gallate Suppresses IGF-I-Induced Lipogenesis and Cytokine Expression in SZ95 Sebocytes. J. Investig. Dermatol. 2012, 132, 2700–2708. [Google Scholar] [CrossRef] [Green Version]
- Robinson, S.; Kwan, Z.; Tang, M.M. Metformin as an adjunct therapy for the treatment of moderate to severe acne vulgaris: A randomized open-labeled study. Dermatol. Ther. 2019, 32, e12953. [Google Scholar] [CrossRef]
- Hunt, D.W.; Winters, G.C.; Brownsey, R.W.; Kulpa, J.E.; Gilliland, K.L.; Thiboutot, D.M.; Hofland, H.E. Inhibition of Sebum Production with the Acetyl Coenzyme A Carboxylase Inhibitor Olumacostat Glasaretil. J. Investig. Dermatol. 2017, 137, 1415–1423. [Google Scholar] [CrossRef] [Green Version]
- Yao, D.; Luo, J.; He, Q.; Shi, H.; Li, J.; Wang, H.; Xu, H.; Chen, Z.; Yi, Y.; Loor, J.J. SCD1 Alters Long-Chain Fatty Acid (LCFA) Composition and Its Expression Is Directly Regulated by SREBP-1 and PPARγ 1 in Dairy Goat Mammary Cells: SCD1 and Fatty Acid Metabolism. J. Cell. Physiol. 2017, 232, 635–649. [Google Scholar] [CrossRef]
- Adeshirlarijaney, A.; Zou, J.; Tran, H.Q.; Chassaing, B.; Gewirtz, A.T. Amelioration of metabolic syndrome by metformin associates with reduced indices of low-grade inflammation independently of the gut microbiota. Am. J. Physiol.-Endocrinol. Metab. 2019, 317, E1121–E1130. [Google Scholar] [CrossRef]
- Marini, H.R. Mediterranean Diet and Soy Isoflavones for Integrated Management of the Menopausal Metabolic Syndrome. Nutrients 2022, 14, 1550. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.M.; Nicol, C.J.; Cheng, Y.C.; Lin, K.H.; Chen, Y.L.; Pei, D.; Lin, C.H.; Shih, Y.N.; Yen, C.H.; Chen, S.J.; et al. Metformin activation of AMPK suppresses AGE-induced inflammatory response in hNSCs. Exp. Cell Res. 2017, 352, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Melnik, B.C.; Schmitz, G. Role of insulin, insulin-like growth factor-1, hyperglycaemic food and milk consumption in the pathogenesis of acne vulgaris. Exp. Dermatol. 2009, 18, 833–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, S.; Mathur, D.K.; Paliwal, V.; Bhargava, P. Efficacy of Metformin in the Treatment of Acne in Women with Polycystic Ovarian Syndrome: A Newer Approach to Acne Therapy. J. Clin. Aesthetic Dermatol. 2019, 12, 34–38. [Google Scholar]
- Nagpal, M.; De, D.; Handa, S.; Pal, A.; Sachdeva, N. Insulin Resistance and Metabolic Syndrome in Young Men with Acne. JAMA Dermatol. 2016, 152, 399. [Google Scholar] [CrossRef] [Green Version]
- Fabbrocini, G.; Izzo, R.; Faggiano, A.; Del Prete, M.; Donnarumma, M.; Marasca, C.; Marciello, F.; Savastano, R.; Monfrecola, G.; Colao, A. Low glycaemic diet and metformin therapy: A new approach in male subjects with acne resistant to common treatments. Clin. Exp. Dermatol. 2016, 41, 38–42. [Google Scholar] [CrossRef]
- Doshi, A.; Zaheer, A.; Stiller, M. A comparison of current acne grading systems and proposal of a novel system. Int. J. Dermatol. 1997, 36, 416–418. [Google Scholar] [CrossRef]
- Del Prete, M.; Mauriello, M.C.; Faggiano, A.; Di Somma, C.; Monfrecola, G.; Fabbrocini, G.; Colao, A. Insulin resistance and acne: A new risk factor for men? Endocrine 2012, 42, 555–560. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Population | Mean Age—Year | Metformin | GAGS | HOMA-IR | BMI kg/m2 | Plasma Insulin, μIU/mL | Total Cholesterol mg/dL | HDL Cholesterol mg/dL | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case | Control | Case | Control | p Value | Case | Control | Case | Control | Case | Control | p Value | Case | Control | p Value | Case | Control | p Value | Case | Control | Case | Control | |
| Robinson et al., 2019 [37] | 42 (35.7% male) | 42 (23.8% male) | 22.6 | 23.2 | 0.501 | Yes | N/A | N/A | 1.6 | 1.8 | 0.295 | 21.6 | 22.6 | 0.303 | 7.4 | 8.2 | 0.468 | N/A | N/A | N/A | N/A | |
| Fabbroccini et al. 2016 [46] | 10 | 10 | 19.5 | 19.5 | N/A | Yes | 14 ± 10.4 | 19.4 ± 7.418 | 1.5 ± 0.1 | 1.5 ± 0.8 | N/A | 22.9 ± 3.5 | 24.1 ± 2.5 | N/A | 9.6 ± 7.5 | 10.4 ± 1.6 | N/A | 165 ± 4.8 | 166 ± 14.5 | 49.5 ± 0.5 | 50 ± 0.4 | |
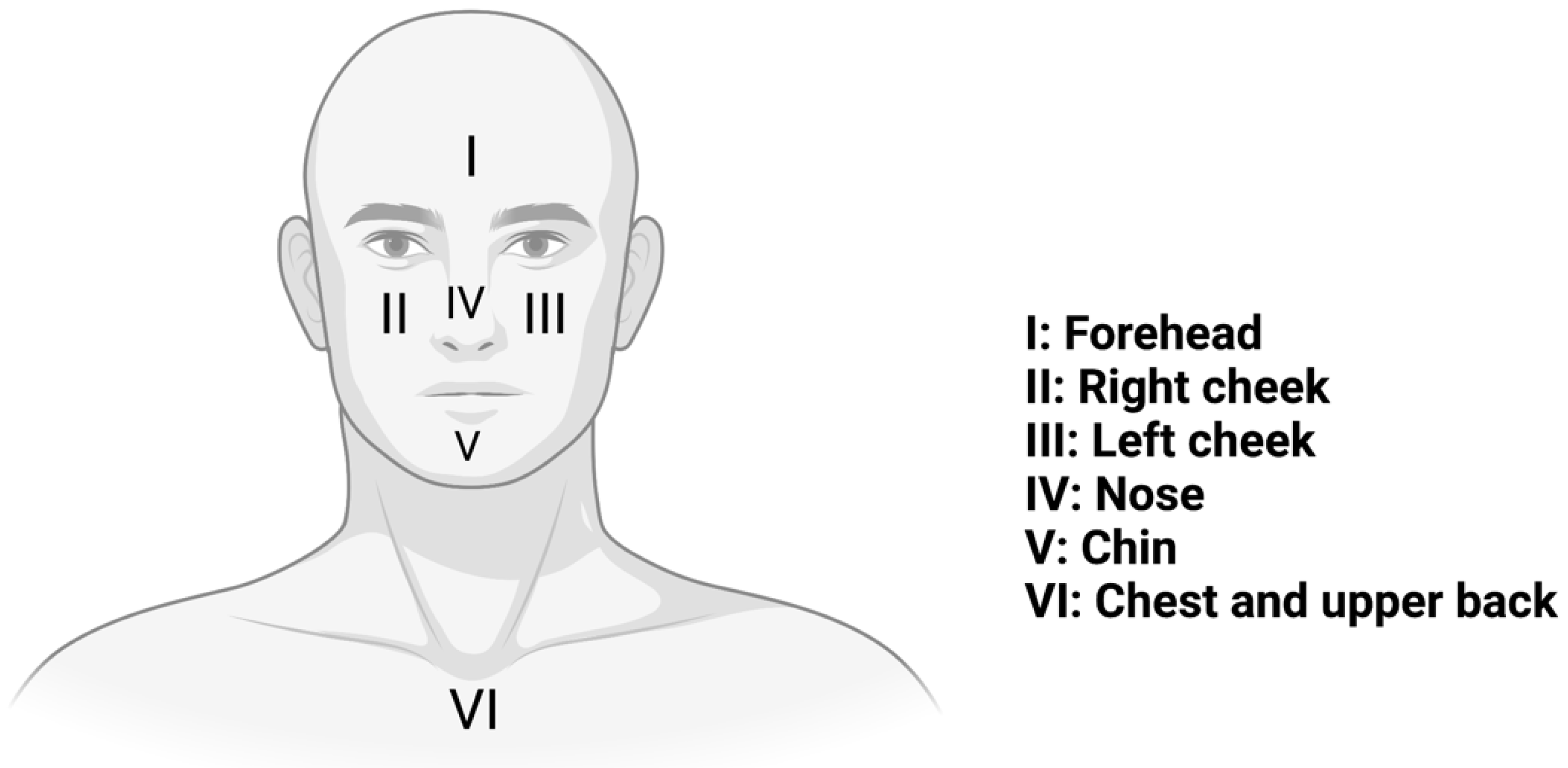
| GAGS (Global acne grading system) | GRADE | ||
| Location | Score | No lesion | 0 |
| I Forehead | 2 | Comedones | 1 |
| II Right cheek | 2 | Papules | 2 |
| III Left cheek | 1 | Pustules | 3 |
| IV Nose | 1 | Nodules/cysts | 4 |
| V Chin | 1 | Nodules/cysts | 4 |
| VI Chest and upper back | 3 | ||
| Local score: multiplicate factor × GRADE (0–4) | |||
 | |||
| Global score | |||
| 0 | none | ||
| 1–18 | mild | ||
| 19–30 | Moderate | ||
| 31–38 | severe | ||
| >39 | Very severe | ||
| Study | Population | Mean Age—Years | Metformin | GAGS | HOMA-IR | BMI kg/m2 | Insulin, μIU/mL | Total Cholesterol mg/dL | HDL Cholesterol mg/dL | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case | Control | Case | Control | p Value | Case | Control | Case | Control | Case | Control | p Value | Case | Control | p Value | Case | Control | p Value | Case | Control | Case | Control | |
| Nagpal et al., 2016 [45] | 100 | 100 | 22.7 | 23.7 | 0.06 | No | N/A | 2 | 1.7 | 0.49 | 22.9 | 23.4 | 0.37 | 9.2 | 7.8 | 0.22 | N/A | N/A | 42.5 | 40.8 | ||
| Del Prete et al., 2012 [48] | 22 | 22 | 18.6 | 20.2 | 0.003 | No | N/A | 1.7 | 1.1 | 0.016 | 24 | 20.1 | 0.003 | 10.6 | 5.5 | 0.01 | N/A | N/A | 46.5 | 57.3 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andreadi, A.; Muscoli, S.; Tajmir, R.; Meloni, M.; Minasi, A.; Muscoli, C.; Ilari, S.; Mollace, V.; Della Morte, D.; Bellia, A.; et al. Insulin Resistance and Acne: The Role of Metformin as Alternative Therapy in Men. Pharmaceuticals 2023, 16, 27. https://doi.org/10.3390/ph16010027
Andreadi A, Muscoli S, Tajmir R, Meloni M, Minasi A, Muscoli C, Ilari S, Mollace V, Della Morte D, Bellia A, et al. Insulin Resistance and Acne: The Role of Metformin as Alternative Therapy in Men. Pharmaceuticals. 2023; 16(1):27. https://doi.org/10.3390/ph16010027
Chicago/Turabian StyleAndreadi, Aikaterini, Saverio Muscoli, Rojin Tajmir, Marco Meloni, Alessandro Minasi, Carolina Muscoli, Sara Ilari, Vincenzo Mollace, David Della Morte, Alfonso Bellia, and et al. 2023. "Insulin Resistance and Acne: The Role of Metformin as Alternative Therapy in Men" Pharmaceuticals 16, no. 1: 27. https://doi.org/10.3390/ph16010027