
64Cu-SAR-Bombesin PET-CT Imaging in the Staging of Estrogen/Progesterone Receptor Positive, HER2 Negative Metastatic Breast Cancer Patients: Safety, Dosimetry and Feasibility in a Phase I Trial
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Safety and Adverse Events
2.3. Dosimetry and Blood Clearance
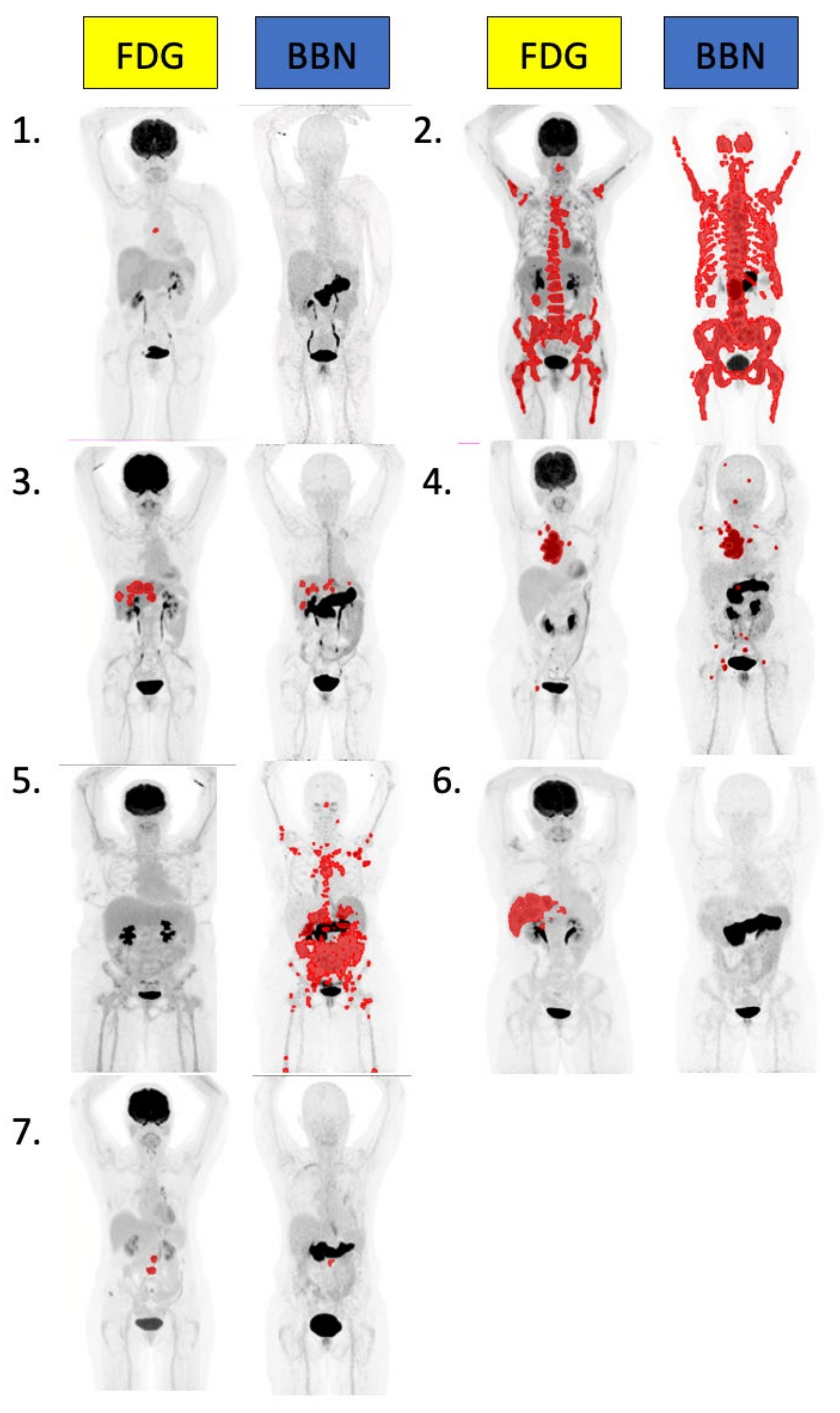
2.4. [64Cu]Cu-SAR-BBN and FDG PET Per Patient Analysis
2.5. [64Cu]Cu-SAR-BBN Negative
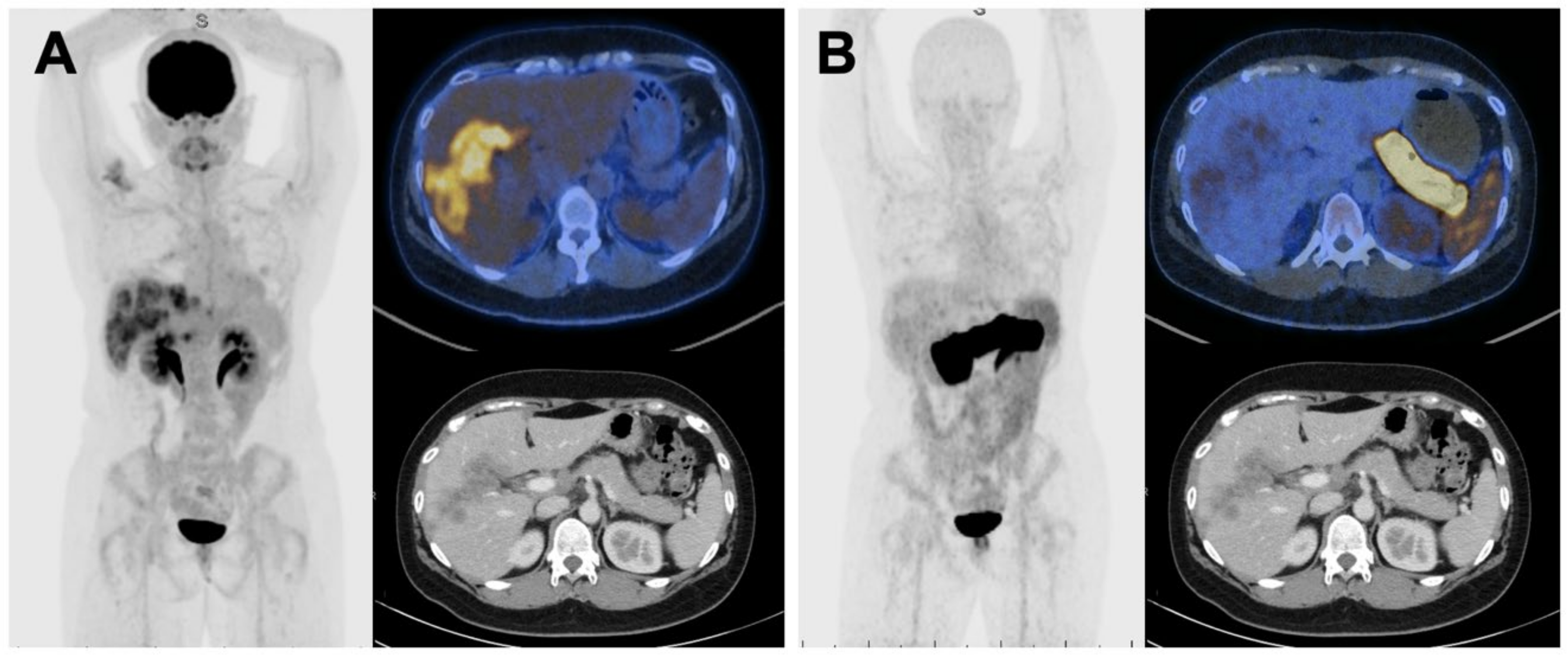
2.6. FDG Negative, [64Cu]Cu-SAR-BBN Positive
2.7. [64Cu]Cu-SAR-BBN and FDG PET Quantitative Analysis
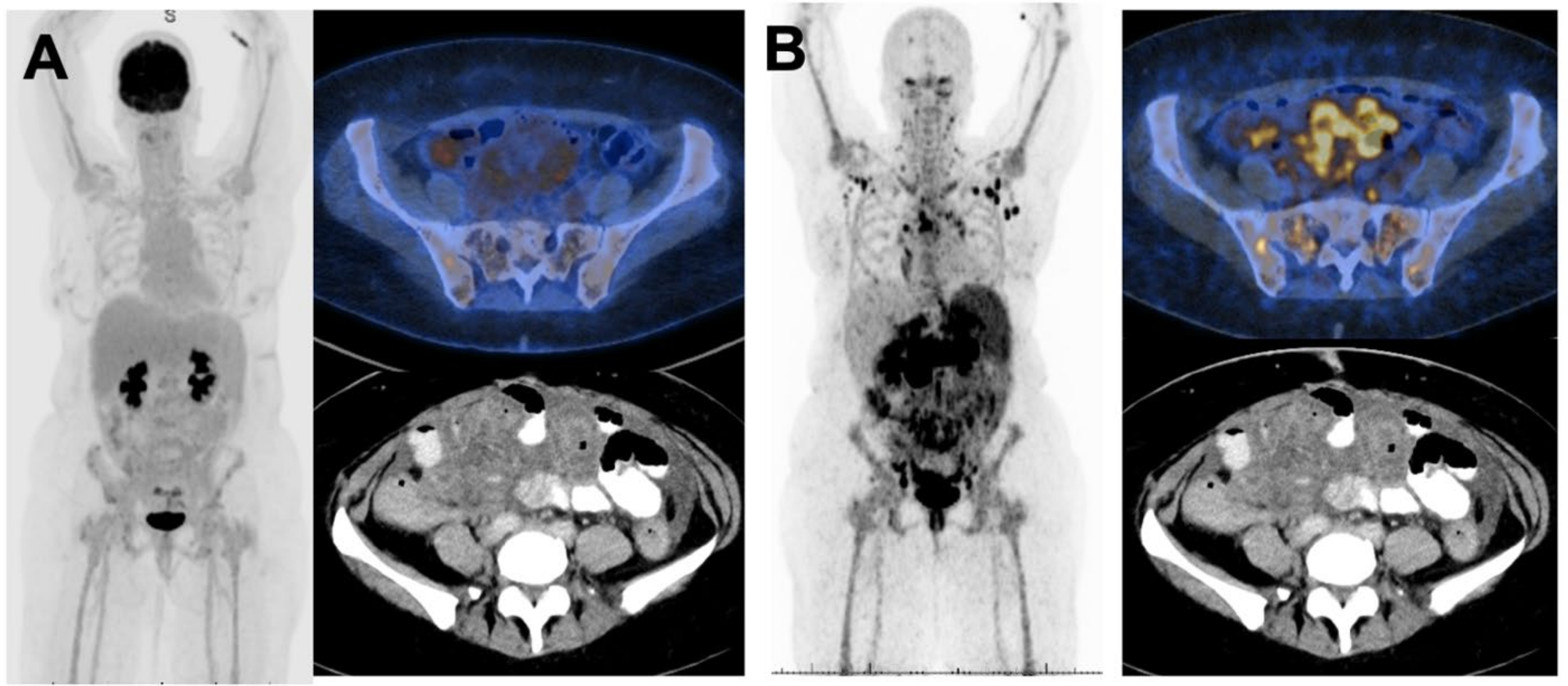
2.8. Classical Lobular Subtype
2.9. Biopsy of Metastatic Lesions and Receptor Status
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Patient Enrolment
4.3. [64Cu]Cu-SAR-BBN Production and Quality Control
4.4. [64Cu]Cu-SAR-BBN Imaging
4.5. FDG Protocol
4.6. Bone Scan and Diagnostic CT
4.7. Image Interpretation
4.8. Safety Assessment
4.9. Dosimetry
4.10. Blood Activity
4.11. Metastatic Biopsy and GRPR Staining
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Breast Cancer Foundation. Breast Cancer Stats. Available online: https://nbcf.org.au/about-breast-cancer/breast-cancer-stats/ (accessed on 22 May 2022).
- Choi, Y.J.; Jeong, Y.H.; Kim, H.J.; Lee, J.H.; Cho, A.; Yun, M.; Lee, J.D.; Kang, W.J. Correlation between hormonal receptor status/human epidermal growth factor receptor 2 overexpression and 18F-FDG uptake in patients with breast cancer. J. Nucl. Med. 2012, 53 (Suppl. 1), 1285. [Google Scholar]
- Yoon, H.J.; Kang, K.W.; Chun, I.K.; Cho, N.; Im, S.A.; Jeong, S.; Lee, S.; Jung, K.C.; Jeong, J.M.; Moon, W.K. Correlation of breast cancer subtypes, based on estrogen receptor, progesterone receptor, and HER2, with functional imaging parameters from ⁶⁸Ga-RGD PET/CT and ¹⁸F-FDG PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1534–1543. [Google Scholar] [CrossRef]
- Basu, S.; Chen, W.; Tchou, J.; Mavi, A.; Cermik, T.; Czerniecki, B.; Schnall, M.; Alavi, A. Comparison of triple-negative and estrogen receptor-positive/progesterone receptor-positive/HER2-negative breast carcinoma using quantitative fluorine-18 fluorodeoxyglucose/positron emission tomography imaging parameters: A potentially useful method for disease characterization. Cancer 2008, 112, 995–1000. [Google Scholar] [PubMed]
- Morgat, C.; MacGrogan, G.; Brouste, V.; Vélasco, V.; Sevenet, N.; Bonnefoi, H.; Fernandez, P.; Debled, M.; Hindie, E. Expression of Gastrin-Releasing Peptide Receptor in Breast Cancer and Its Association with Pathologic, Biologic, and Clinical Parameters: A Study of 1,432 Primary Tumors. J. Nucl. Med. 2017, 58, 1401–1407. [Google Scholar] [CrossRef] [PubMed]
- Parry, J.J.; Andrews, R.; Rogers, B.E. MicroPET imaging of breast cancer using radiolabeled bombesin analogs targeting the gastrin-releasing peptide receptor. Breast Cancer Res. Treat. 2007, 101, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Gugger, M.; Reubi, J.C. Gastrin-releasing peptide receptors in non-neoplastic and neoplastic human breast. Am. J. Pathol. 1999, 155, 2067–2076. [Google Scholar] [CrossRef] [Green Version]
- Scopinaro, F.; Varvarigou, A.; Ussof, W.; De Vincentis, G.; Archimandritis, S.; Evangelatos, G.; Corleto, V.; Capoccetti, F.; Massa, R.; Remediani, S. Breast cancer takes up 99mTc bombesin. A preliminary report. Tumori J. 2002, 88, S25–S28. [Google Scholar] [CrossRef]
- Van de Wiele, C.; Phonteyne, P.; Pauwels, P.; Goethals, I.; Van den Broecke, R.; Cocquyt, V.; Dierckx, R.A. Gastrin-Releasing Peptide Receptor Imaging in Human Breast Carcinoma Versus Immunohistochemistry. J. Nucl. Med. 2008, 49, 260–264. [Google Scholar] [CrossRef] [Green Version]
- Huynh, T.T.; van Dam, E.M.; Sreekumar, S.; Mpoy, C.; Blyth, B.J.; Muntz, F.; Harris, M.J.; Rogers, B.E. Copper-67-Labeled Bombesin Peptide for Targeted Radionuclide Therapy of Prostate Cancer. Pharmaceuticals 2022, 15, 728. [Google Scholar] [CrossRef]
- Gourni, E.; Del Pozzo, L.; Kheirallah, E.; Smerling, C.; Waser, B.; Reubi, J.C.; Paterson, B.M.; Donnelly, P.S.; Meyer, P.T.; Maecke, H.R. Copper-64 Labeled Macrobicyclic Sarcophagine Coupled to a GRP Receptor Antagonist Shows Great Promise for PET Imaging of Prostate Cancer. Mol. Pharm. 2015, 12, 2781–2790. [Google Scholar] [CrossRef]
- O’ Donoghue, J.A.; Baidoo, N.; Deland, D.; Welt, S.; Divgi, C.R.; Sgouros, G. Hematologic Toxicity in Radioimmunotherapy: Dose-Response Relationships for I-131 Labeled Antibody Therapy. Cancer Biother. Radiopharm. 2002, 17, 435–443. [Google Scholar] [CrossRef]
- Dawson, L.A.; Kavanagh, B.D.; Paulino, A.C.; Das, S.K.; Miften, M.; Li, X.A.; Pan, C.; Haken, R.K.T.; Schultheiss, T.E. Radiation-associated kidney injury. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76 (Suppl. 3), S108–S115. [Google Scholar] [CrossRef]
- Marks, L.B.; Yorke, E.D.; Jackson, A.; Ten Haken, R.K.; Constine, L.S.; Eisbruch, A.; Bentzen, S.M.; Nam, J.; Deasy, J.O. Use of normal tissue complication probability models in the clinic. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76 (Suppl. 3), S10–S19. [Google Scholar] [CrossRef] [Green Version]
- Ming, Y.; Wu, N.; Qian, T.; Li, X.; Wan, D.Q.; Li, C.; Li, Y.; Wu, Z.; Wang, X.; Wu, N.; et al. Progress and Future Trends in PET/CT and PET/MRI Molecular Imaging Approaches for Breast Cancer. Front. Oncol. 2020, 10, 1301. [Google Scholar] [CrossRef]
- Morgat, C.; Schollhammer, R.; Macgrogan, G.; Barthe, N.; Vélasco, V.; Vimont, D.; Cazeau, A.-L.; Fernandez, P.; Hindié, E. Comparison of the binding of the gastrin-releasing peptide receptor (GRP-R) antagonist 68Ga-RM2 and 18F-FDG in breast cancer samples. PLoS ONE 2019, 14, e0210905. [Google Scholar] [CrossRef] [Green Version]
- Fujii, T.; Yajima, R.; Kurozumi, S.; Higuchi, T.; Obayashi, S.; Tokiniwa, H.; Nagaoka, R.; Takata, D.; Horiguchi, J.; Kuwano, H. Clinical Significance of 18F-FDG-PET in Invasive Lobular Carcinoma. Anticancer Res. 2016, 36, 5481–5485. [Google Scholar] [CrossRef]
- Groheux, D.; Cochet, A.; Humbert, O.; Alberini, J.L.; Hindié, E.; Mankoff, D. ¹⁸F-FDG PET/CT for Staging and Restaging of Breast Cancer. J. Nucl. Med. 2016, 57 (Suppl. 1), 17s–26s. [Google Scholar] [CrossRef] [Green Version]
- Hogan, M.P.; Goldman, D.A.; Dashevsky, B.; Riedl, C.C.; Gönen, M.; Osborne, J.R.; Jochelson, M.; Hudis, C.; Morrow, M.; Ulaner, G.A. Comparison of 18F-FDG PET/CT for Systemic Staging of Newly Diagnosed Invasive Lobular Carcinoma Versus Invasive Ductal Carcinoma. J. Nucl. Med. 2015, 56, 1674–1680. [Google Scholar] [CrossRef] [Green Version]
- Jung, N.Y.; Kim, S.H.; Kim, S.H.; Seo, Y.Y.; Oh, J.K.; Choi, H.S.; You, W.J. Effectiveness of Breast MRI and (18)F-FDG PET/CT for the Preoperative Staging of Invasive Lobular Carcinoma versus Ductal Carcinoma. J. Breast Cancer 2015, 18, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Zang, J.; Mao, F.; Wang, H.; Zhang, J.; Liu, Q.; Peng, L.; Li, L.; Lang, L.; Chen, X.; Zhu, Z.; et al. 68Ga-NOTA-RM26 PET/CT in the Evaluation of Breast Cancer: A Pilot Prospective Study. Clin. Nucl. Med. 2018, 43, 663–669. [Google Scholar] [CrossRef]
- Stoykow, C.; Erbes, T.; Maecke, H.R.; Bulla, S.; Bartholomä, M.; Mayer, S.; Drendel, V.; Bronsert, P.; Werner, M.; Meyer, P.T.; et al. Gastrin-releasing Peptide Receptor Imaging in Breast Cancer Using the Receptor Antagonist (68)Ga-RM2 And PET. Theranostics 2016, 6, 1641–1650. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Mao, F.; Niu, G.; Peng, L.; Lang, L.; Li, F.; Chen, X.; Ying, H.; Wu, H.; Pan, B.; et al. (68)Ga-BBN-RGD PET/CT for GRPR and Integrin α(v)β(3) Imaging in Patients with Breast Cancer. Theranostics 2018, 8, 1121–1130. [Google Scholar] [CrossRef] [PubMed]
- Michalski, K.; Kemna, L.; Asberger, J.; Grosu, A.L.; Meyer, P.T.; Ruf, J.; Sprave, T. Gastrin-Releasing Peptide Receptor Antagonist [(68)Ga]RM2 PET/CT for Staging of Pre-Treated, Metastasized Breast Cancer. Cancers 2021, 13, 6106. [Google Scholar] [CrossRef] [PubMed]
- Sgouros, G.; Bodei, L.; McDevitt, M.R.; Nedrow, J.R. Radiopharmaceutical therapy in cancer: Clinical advances and challenges. Nat. Rev. Drug Discov. 2020, 19, 589–608. [Google Scholar] [CrossRef] [PubMed]
- Kurth, J.; Krause, B.J.; Schwarzenböck, S.M.; Bergner, C.; Hakenberg, O.W.; Heuschkel, M. First-in-human dosimetry of gastrin-releasing peptide receptor antagonist [(177)Lu]Lu-RM2: A radiopharmaceutical for the treatment of metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 123–135. [Google Scholar] [CrossRef]
- Dalm, S.U.; Bakker, I.L.; de Blois, E.; Doeswijk, G.N.; Konijnenberg, M.W.; Orlandi, F.; Barbato, D.; Tedesco, M.; Maina, T.; de Jong, M. 68Ga/177Lu-NeoBOMB1, a Novel Radiolabeled GRPR Antagonist for Theranostic Use in Oncology. J. Nucl. Med. 2017, 58, 293–299. [Google Scholar] [CrossRef] [Green Version]
- Kaloudi, A.; Lymperis, E.; Giarika, A.; Dalm, S.; Orlandi, F.; Barbato, D.; Tedesco, M.; Maina, T.; De Jong, M.; Nock, B.A. NeoBOMB1, a GRPR-Antagonist for Breast Cancer Theragnostics: First Results of a Preclinical Study with [(67)Ga]NeoBOMB1 in T-47D Cells and Tumor-Bearing Mice. Molecules 2017, 22, 1950. [Google Scholar] [CrossRef] [Green Version]
- Huynh, T.; Van Dam, E.; Houston, Z.; McInnes, L.; Mpoy, C.; Harris, M.; Thurecht, K.; Donnelly, P.; Rogers, B. A Cu-64/Cu-67 Bombesin ligand as a theranostic for cancer. J. Nucl. Med. 2021, 62 (Suppl. 1), 1237. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Median Age (Years) | 60 (38–81) |
|---|---|
| Median time from diagnosis (years) | 3 (0–29) |
| Type of primary cancer | |
| Invasive Carcinoma NOS | 5 |
| Invasive lobular carcinoma | 2 |
| Stage (at diagnosis) | |
| M0 | 5 |
| M1 | 1 |
| Unknown | 1 |
| Number of lines of prior therapy | |
| 0 | 1 |
| 1 | 3 |
| 2 or more | 3 |
| Most immediate prior therapy | |
| Chemotherapy | 2 |
| Endocrine therapy | 0 |
| Targeted therapy (OTHERS) | 4 |
| Pt | Histological Subtype | ER/PR (%) Primary | Metastatic Biopsy site | ER/PR (%) Metastatic | Immediate Prior therapy |
|---|---|---|---|---|---|
| 1 | Invasive ductal | 90/80 | Liver | 90/− |
Letrozole/ Palbociclib |
| 2 | Classical lobular | n/a | Liver | 95/70 | Vinorelbine |
| 3 | Invasive ductal | 95/95 | Liver | +/+ |
Fulvestrant/ Palbociclib |
| 4 | Invasive ductal | +/+ | Chest wall | 95/95 | Letrozole |
| 5 | Classical lobular | n/a | Skin | 95/− | − |
| 6 | Invasive ductal | 80/− | Liver | 90/− |
Carboplatin/ Gemcitabine |
| 7 | Invasive ductal | 62/53 | Pleura | 100/5 | Letrozole/Ribociclib |
| Patient | 1 | 2 | 3 | 4 | 5 | 6 | 7 | Mean ± SD |
|---|---|---|---|---|---|---|---|---|
| Effective Dose (mSv/MBq) | 0.0116 | 0.0124 | 0.0080 | 0.0069 | 0.0084 | 0.0111 | 0.0083 | 0.0095 ± 0.0021 |
| Target Tissues | Estimated Absorbed Dose in Gy | Dose Limits (Gy) | ||||
|---|---|---|---|---|---|---|
| GBq/Patient | 10 | 20 | 40 | 60 | 87 | |
| Pancreas | 3.0 ± 1.2 | 6.1 ± 2.5 | 12.1 ± 5.0 | 18.2 ± 7.5 | 26.3 ± 10.8 | - |
| Kidneys | 0.7 ± 0.3 | 1.4 ± 0.5 | 2.8 ± 1.0 | 4.2 ± 1.5 | 6.0 ± 2.2 | 23 |
| Alveolar-interstitial | 0.4 ± 0.1 | 0.8 ± 0.2 | 1.5 ± 0.4 | 2.3 ± 0.6 | 3.3 ± 0.8 | 20 |
| Liver | 0.3 ± 0.1 | 0.6 ± 0.2 | 1.2 ± 0.4 | 1.8 ± 0.6 | 2.6 ± 0.9 | 30 |
| Red (active) marrow | 0.2 ± 0.1 | 0.5 ± 0.3 | 0.9 ± 0.6 | 1.4 ± 0.9 | 2.0 ± 1.3 | 2 |
| Spleen | 0.3 ± 0.1 | 0.5 ± 0.1 | 1.0 ± 0.3 | 1.5 ± 0.4 | 2.2 ± 0.5 | |
| Bronchioles secretary cells | 0.2 ± 0.0 | 0.4 ± 0.1 | 0.8 ± 0.2 | 1.1 ± 0.3 | 1.7 ± 0.4 | |
| Heart wall | 0.2 ± 0.0 | 0.4 ± 0.1 | 0.7 ± 0.2 | 1.1 ± 0.3 | 1.5 ± 0.4 | 26 |
| Pt | Histological Subtype | FDG | BBN (1 h) | ||
|---|---|---|---|---|---|
| SUV Max | TV | SUV Max | TV | ||
| 1 | Invasive ductal | 7 | 2 | <3 | 0 |
| 2 | Classical lobular | 11 | 504 | 20 | 2033 |
| 3 | Invasive ductal | 7 | 91 | 6 | 13 |
| 4 | Invasive ductal | 20 | 168 | 27 | 209 |
| 5 | Classical lobular | <3 | 0 | 19 | 634 |
| 6 | Invasive ductal | 7 | 381 | <3 | 0 |
| 7 | Invasive ductal | 8 | 8 | 5 | 3 |
| BBN (1 h) | FDG | |
|---|---|---|
| TTV | 413 (751) | 164 (202) |
| SUV Max | 11 (11) | 9 (6) |
| SUV Mean | 4 (3) | 4 (3) |
| No. of lesions | 49 (74) | 9 (12) |
| Patient | Metastatic Site | GRPR Staining | FDG SUV Max | BBN 1 h SUV Max |
|---|---|---|---|---|
| 2 | Liver | Negative | 4.4 | 11.5 |
| 3 | Liver | Negative | 4.6 | - |
| 4 | Sternum | Positive | 4.4 | 11.5 |
| 5 | Skin Lesion * | Negative | n/a | n/a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, K.; Sheehan-Dare, G.; Nguyen, A.; Ho, B.; Liu, V.; Lee, J.; Brown, L.; Dear, R.; Chan, L.; Sharma, S.; et al. 64Cu-SAR-Bombesin PET-CT Imaging in the Staging of Estrogen/Progesterone Receptor Positive, HER2 Negative Metastatic Breast Cancer Patients: Safety, Dosimetry and Feasibility in a Phase I Trial. Pharmaceuticals 2022, 15, 772. https://doi.org/10.3390/ph15070772
Wong K, Sheehan-Dare G, Nguyen A, Ho B, Liu V, Lee J, Brown L, Dear R, Chan L, Sharma S, et al. 64Cu-SAR-Bombesin PET-CT Imaging in the Staging of Estrogen/Progesterone Receptor Positive, HER2 Negative Metastatic Breast Cancer Patients: Safety, Dosimetry and Feasibility in a Phase I Trial. Pharmaceuticals. 2022; 15(7):772. https://doi.org/10.3390/ph15070772
Chicago/Turabian StyleWong, Keith, Gemma Sheehan-Dare, Andrew Nguyen, Bao Ho, Victor Liu, Jonathan Lee, Lauren Brown, Rachel Dear, Lyn Chan, Shikha Sharma, and et al. 2022. "64Cu-SAR-Bombesin PET-CT Imaging in the Staging of Estrogen/Progesterone Receptor Positive, HER2 Negative Metastatic Breast Cancer Patients: Safety, Dosimetry and Feasibility in a Phase I Trial" Pharmaceuticals 15, no. 7: 772. https://doi.org/10.3390/ph15070772