
Targeting Wnt/Beta-Catenin Signaling in HPV-Positive Head and Neck Squamous Cell Carcinoma

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
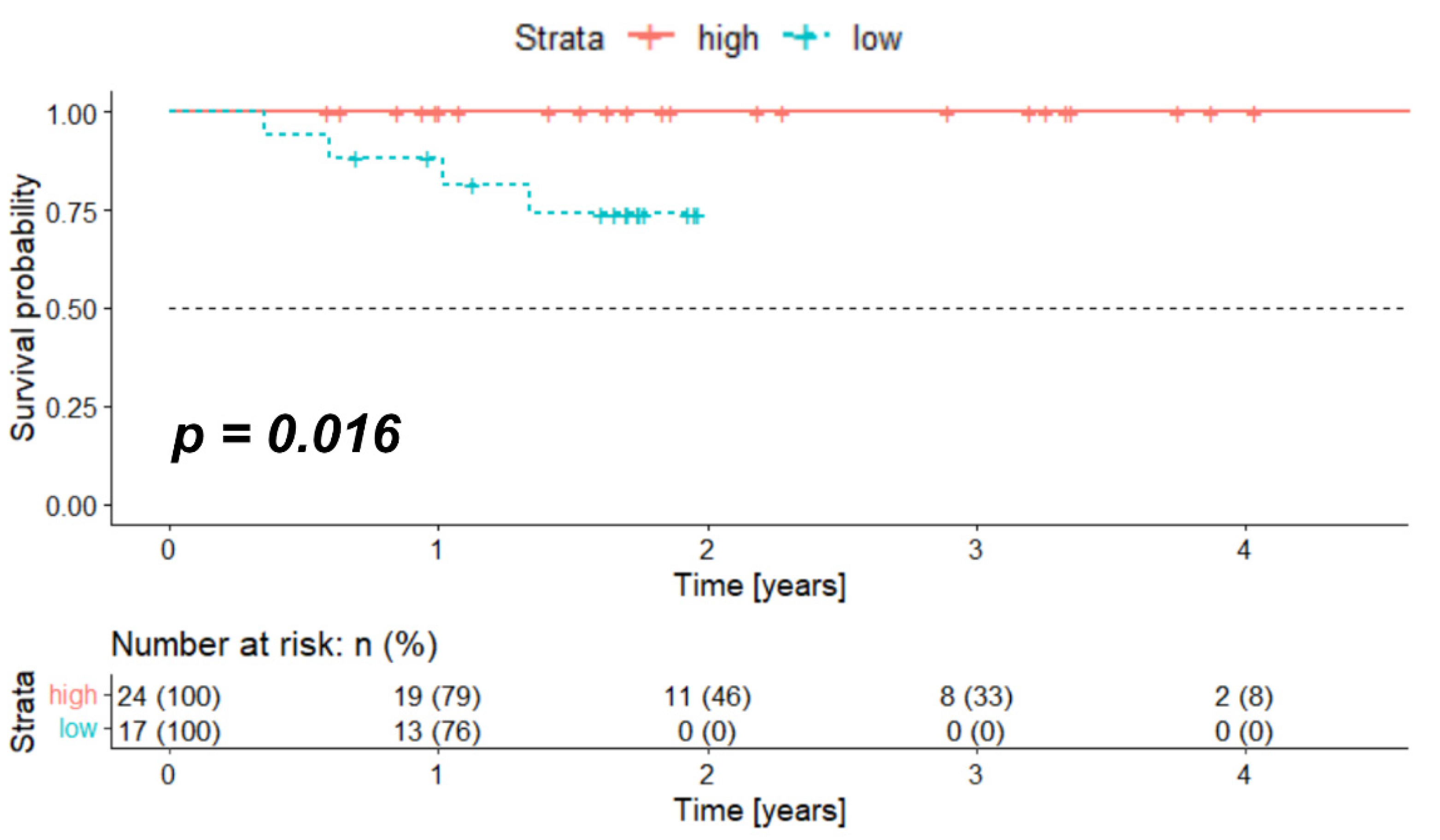
2.1. High Expression of Crebbp at mRNA Level Associates with Better Survival
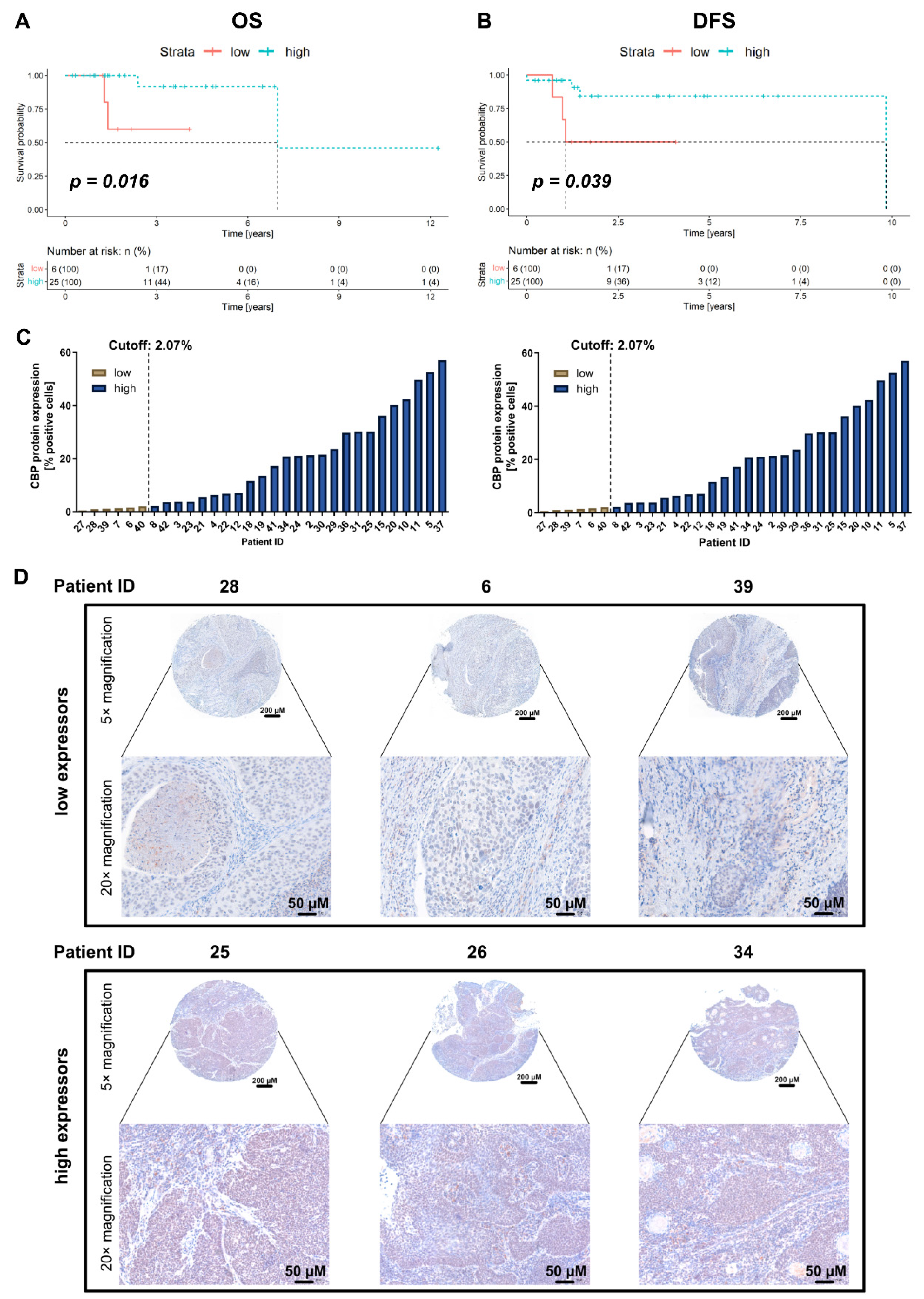
2.2. Association of CBP Protein Expression with Survival in the In-House Cohort
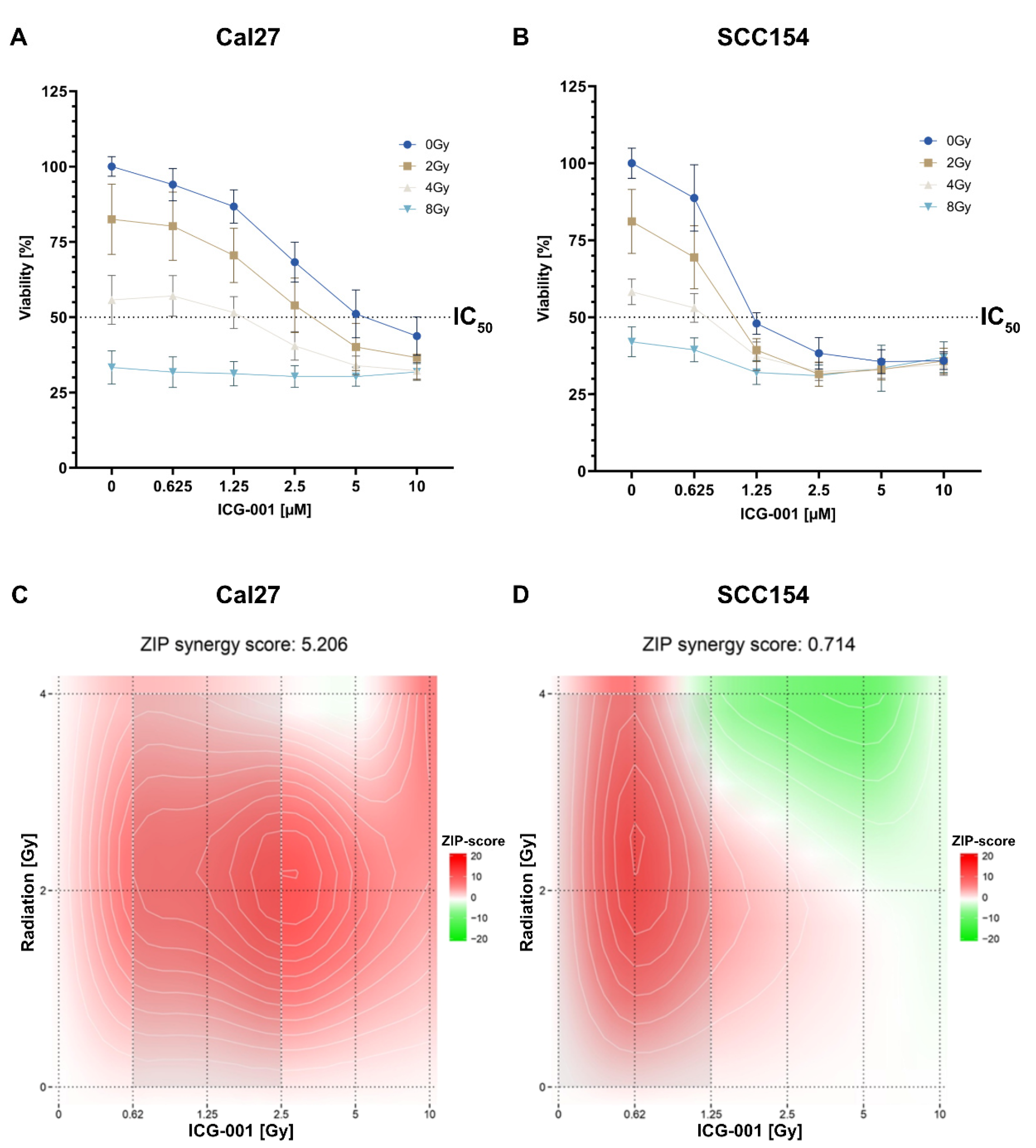
2.3. Combining ICG-001 with Irradiation Leads to a Decreased Cell Viability in a Dose-Dependent Manner in SCC154 and Cal27
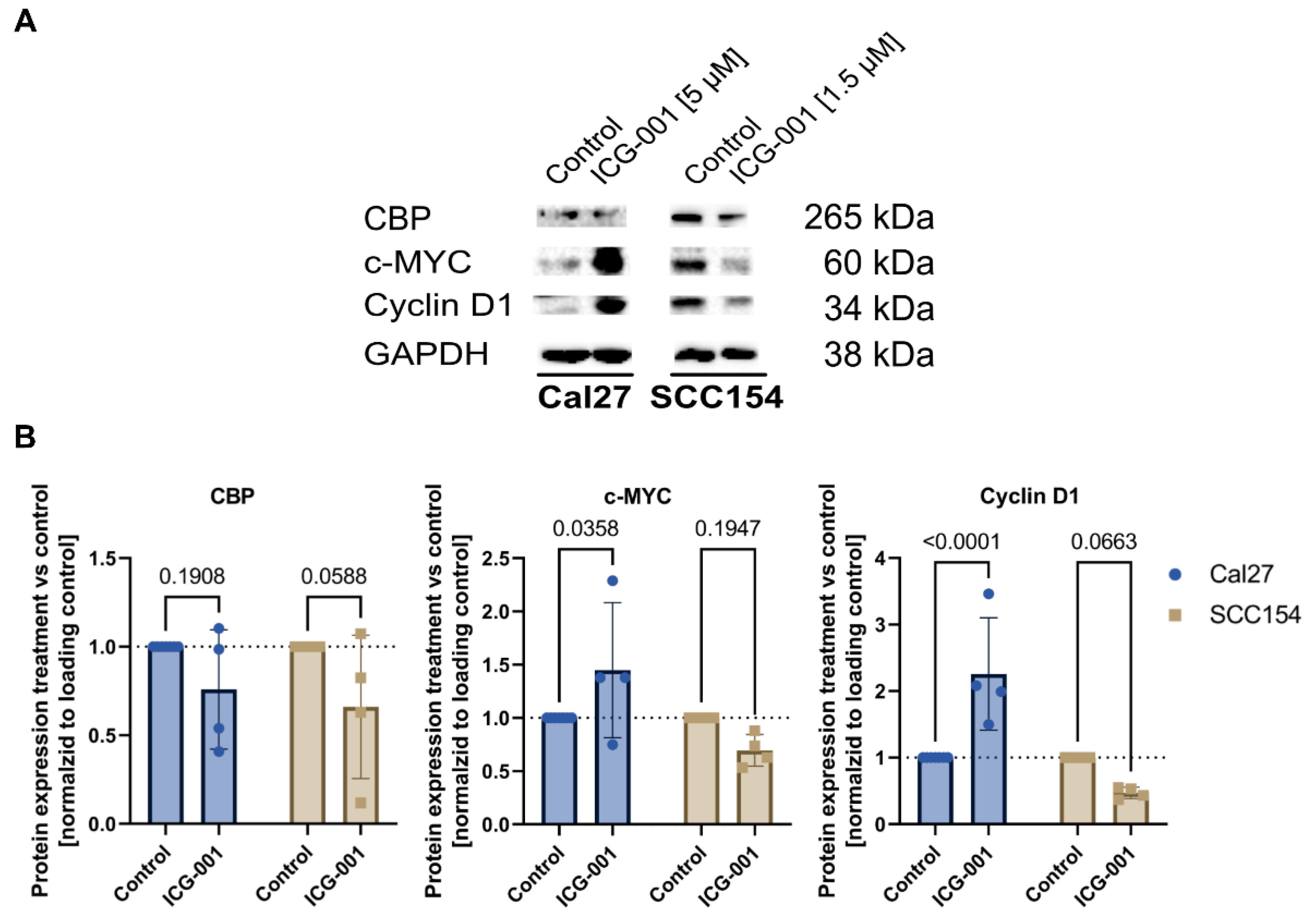
2.4. Treatment with ICG-001 Downregulates CBP and Shows Different Down-Stream Modulation of Cell-Cycle Control between HPV-Negative and HPV-Positive HNSCC Cells
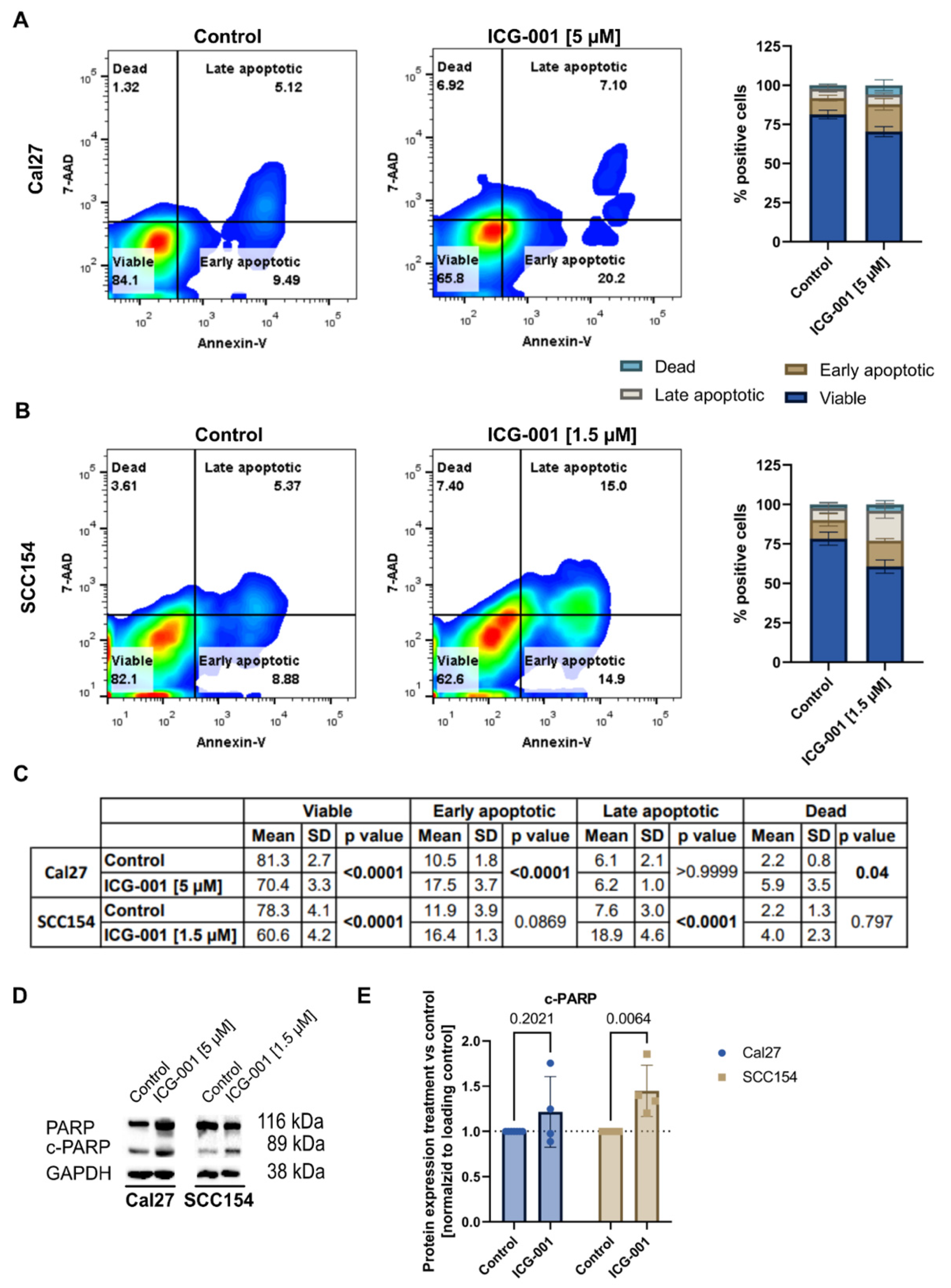
2.5. Treatment with ICG-001 Induces Apoptosis in SCC154 and Cal27 Cells
2.6. Treatment with ICG-001 Shows Antimigratory Effects In Vitro
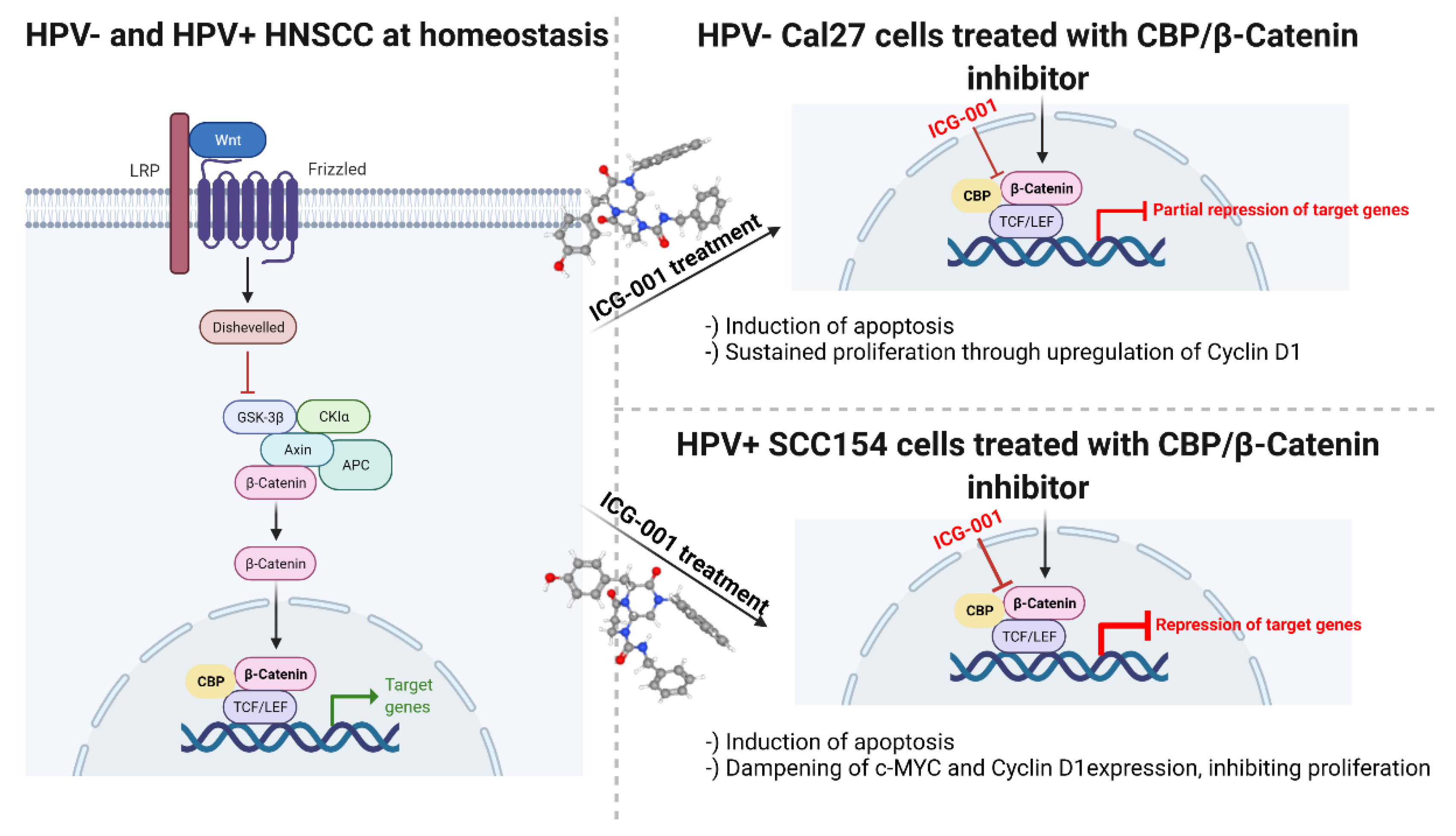
2.7. Proposed Mechanism of ICG-001 in the Tested HNSCC Cell Lines
3. Discussion
4. Materials and Methods
4.1. The Cancer Genome Atlas (TCGA)—TCGA Cohort
4.2. Immunohistochemistry—The MUV Cohort
4.3. Cell Culture
4.4. Cytotoxicity Assay
4.5. Migration Assay
4.6. Cell Apoptosis: Fluorescence-Activated Cell Sorting (FACS)—Annexin V Assay
4.7. Immunoblotting
4.8. Statistics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mirza, A.H.; Thomas, G.; Ottensmeier, C.H.; King, E.V. Importance of the immune system in head and neck cancer. Head Neck 2019, 41, 2789–2800. [Google Scholar] [CrossRef] [PubMed]
- Brkic, F.F.; Kadletz-Wanke, L.; Kenner, L.; Füreder, T.; Jank, B.; Brunner, M.; Heiduschka, G. An analysis of distant metastasis cases from HPV-associated oropharyngeal squamous cell carcinoma. J. Craniomaxillofac. Surg. 2021, 49, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.J.; Thirdborough, S.M.; Mellows, T.; Riley, C.; Harris, S.; Suchak, K.; Webb, A.; Hampton, C.; Patel, N.N.; Randall, C.J.; et al. Tumour-infiltrating lymphocytes predict for outcome in HPV-positive oropharyngeal cancer. Br. J. Cancer 2014, 21, 489–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timbang, M.R.; Sim, M.W.; Bewley, A.F.; Farwell, D.G.; Mantravadi, A.; Moore, M.G. HPV-related oropharyngeal cancer: A review on burden of the disease and opportunities for prevention and early detection. Hum. Vaccin. Immunother. 2019, 15, 1920–1928. [Google Scholar] [CrossRef] [PubMed]
- Combes, J.D.; Franceschi, S. Role of human papillomavirus in non-oropharyngeal head and neck cancers. Oral Oncol. 2014, 50, 370–379. [Google Scholar] [CrossRef]
- Mehanna, H.; Robinson, M.; Hartley, A.; Kong, A.; Foran, B.; Fulton-Lieuw, T.; Dalby, M.; Mistry, P.; Sen, M.; O’Toole, L.; et al. Radiotherapy plus cisplatin or cetuximab in low-risk human papillomavirus-positive oropharyngeal cancer (De-ESCALaTE HPV): An open-label randomised controlled phase 3 trial. Lancet 2019, 393, 51–60. [Google Scholar] [CrossRef] [Green Version]
- Mirghani, H.; Blanchard, P. Treatment de-escalation for HPV-driven oropharyngeal cancer: Where do we stand? Clin. Transl. Radiat. Oncol. 2017, 8, 4–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iyer, N.G.; Dogan, S.; Palmer, F.; Rahmati, R.; Nixon, I.J.; Lee, N.; Patel, S.G.; Shah, J.P.; Ganly, I. Detailed Analysis of Clinicopathologic Factors Demonstrate Distinct Difference in Outcome and Prognostic Factors Between Surgically Treated HPV-Positive and Negative Oropharyngeal Cancer. Ann. Surg. Oncol. 2015, 22, 4411–4421. [Google Scholar] [CrossRef] [Green Version]
- Brkic, F.F.; Mayer, C.; Besser, G.; Altorjai, G.; Herrmann, H.; Heiduschka, G.; Haymerle, G.; Kadletz-Wanke, L. Potential association of the prognostic index and survival in patients with p16-positive oropharyngeal squamous cell carcinoma. Wien. Klin. Wochenschr. 2021, 133, 1117–1121. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Koo, B.S.; Kim, J.M.; Huang, S.; Rho, Y.S.; Bae, W.J.; Kang, H.J.; Kim, Y.S.; Moon, J.H.; Lim, Y.C. Wnt/β-catenin signalling maintains self-renewal and tumourigenicity of head and neck squamous cell carcinoma stem-like cells by activating Oct4. J. Pathol. 2014, 234, 99–107. [Google Scholar] [CrossRef]
- Zhan, T.; Rindtorff, N.; Boutros, M. Wnt signaling in cancer. Oncogene 2017, 36, 1461–1473. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.H.; Lee, S.H.; Lim, Y.C. Wnt/β-catenin/Slug pathway contributes to tumor invasion and lymph node metastasis in head and neck squamous cell carcinoma. Clin. Exp. Metastasis 2021, 38, 163–174. [Google Scholar] [CrossRef]
- Bello, J.O.; Nieva, L.O.; Paredes, A.C.; Gonzalez, A.M.; Zavaleta, L.R.; Lizano, M. Regulation of the Wnt/β-Catenin Signaling Pathway by Human Papillomavirus E6 and E7 Oncoproteins. Viruses 2015, 7, 4734–4755. [Google Scholar] [CrossRef] [PubMed]
- Manzo-Merino, J.; Contreras-Paredes, A.; Vázquez-Ulloa, E.; Rocha-Zavaleta, L.; Fuentes-Gonzalez, A.M.; Lizano, M. The role of signaling pathways in cervical cancer and molecular therapeutic targets. Arch. Med. Res. 2014, 45, 525–539. [Google Scholar] [CrossRef] [PubMed]
- Kartha, V.K.; Alamoud, K.A.; Sadykov, K.; Nguyen, B.C.; Laroche, F.; Feng, H.; Lee, J.; Pai, S.I.; Varelas, X.; Egloff, A.M.; et al. Functional and genomic analyses reveal therapeutic potential of targeting β-catenin/CBP activity in head and neck cancer. Genome Med. 2018, 10, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Center for Biotechnology Information. PubChem Compound Summary for CID 11238147. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/icg-001 (accessed on 17 March 2022).
- Lin, Z.; Li, Q.; Zhao, Y.; Lin, Z.; Cheng, N.; Zhang, D.; Liu, G.; Lin, J.; Zhang, H.; Lin, D. Combination of Auranofin and ICG-001 Suppress the Proliferation and Metastasis of Colon Cancer. Front. Oncol. 2021, 11, 738085. [Google Scholar] [CrossRef] [PubMed]
- Chan, L.S.; Man, O.Y.; Kwok, H.H.; Chen, L.; Chan, K.C.; Lung, H.L.; Ngan, R.K.; Wong, R.N.; Lo, K.W.; Lee, A.W.; et al. The Wnt modulator ICG 001 mediates the inhibition of nasopharyngeal carcinoma cell migration in vitro via the miR 150/CD44 axis. Int. J. Oncol. 2019, 54, 1010–1020. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Chen, H.; Zheng, P.; Zheng, Y.; Luo, Q.; Xie, G.; Ma, Y.; Shen, L. ICG-001 suppresses growth of gastric cancer cells and reduces chemoresistance of cancer stem cell-like population. J. Exp. Clin. Cancer Res. 2017, 36, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arensman, M.D.; Telesca, D.; Lay, A.R.; Kershaw, K.M.; Wu, N.; Donahue, T.R.; Dawson, D.W. The CREB-binding protein inhibitor ICG-001 suppresses pancreatic cancer growth. Mol. Cancer Ther. 2014, 13, 2303–2314. [Google Scholar] [CrossRef] [Green Version]
- Evangelisti, C.; Chiarini, F.; Cappellini, A.; Paganelli, F.; Fini, M.; Santi, S.; Martelli, A.M.; Neri, L.M.; Evangelisti, C. Targeting Wnt/β-catenin and PI3K/Akt/mTOR pathways in T-cell acute lymphoblastic leukemia. J. Cell Physiol. 2020, 235, 5413–5428. [Google Scholar] [CrossRef]
- Rühlmann, F.; Windhof-Jaidhauser, I.M.; Menze, C.; Beißbarth, T.; Bohnenberger, H.; Ghadimi, M.; Dango, S. The prognostic capacities of CBP and p300 in locally advanced rectal cancer. World J. Surg. Oncol. 2019, 17, 224. [Google Scholar] [CrossRef] [PubMed]
- Hashida, Y.; Higuchi, T.; Matsumoto, S.; Iguchi, M.; Murakami, I.; Hyodo, M.; Daibata, M. Prognostic significance of human papillomavirus 16 viral load level in patients with oropharyngeal cancer. Cancer Sci. 2021, 112, 4404–4417. [Google Scholar] [CrossRef] [PubMed]
- Rampias, T.; Boutati, E.; Pectasides, E.; Sasaki, C.; Kountourakis, P.; Weinberger, P.; Psyrri, A. Activation of Wnt signaling pathway by human papillomavirus E6 and E7 oncogenes in HPV16-positive oropharyngeal squamous carcinoma cells. Mol. Cancer Res. 2010, 8, 433–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muñoz-Bello, J.O.; Olmedo-Nieva, L.; Castro-Muñoz, L.J.; Manzo-Merino, J.; Contreras-Paredes, A.; González-Espinosa, C.; López-Saavedra, A.; Lizano, M. HPV-18 E6 Oncoprotein and Its Spliced Isoform E6*I Regulate the Wnt/β-Catenin Cell Signaling Pathway through the TCF-4 Transcriptional Factor. Int. J. Mol. Sci. 2018, 19, 3153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lacau St Guily, J.; Rousseau, A.; Baujat, B.; Périé, S.; Schultz, P.; Barry, B.; Dufour, X.; Malard, O.; Pretet, J.L.; Clavel, C.; et al. Oropharyngeal cancer prognosis by tumour HPV status in France: The multicentric Papillophar study. Oral Oncol. 2017, 67, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Sheng, H.; Xiao, Y.; Hu, W.; Zhang, Z.; Chen, Y.; Zhu, Z.; Wu, D.; Cao, C.; Sun, J. Wnt/β-catenin inhibitor ICG-001 enhances the antitumor efficacy of radiotherapy by increasing radiation-induced DNA damage and improving tumor immune microenvironment in hepatocellular carcinoma. Radiother. Oncol. 2021, 162, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Gökyildirim, M.Y.; Grandel, U.; Hattar, K.; Dahlem, G.; Schuetz, E.; Leinberger, F.H.; Eberle, F.; Sibelius, U.; Grimminger, F.; Seeger, W.; et al. Targeting CREB-binding protein overrides LPS induced radioresistance in non-small cell lung cancer cell lines. Oncotarget 2018, 9, 28976–28988. [Google Scholar] [CrossRef] [Green Version]
- Schultz, J.D.; Sommer, J.U.; Hoedt, S.; Erben, P.; Hofheinz, R.D.; Faber, A.; Thorn, C.; Hörmann, K.; Sauter, A. Chemotherapeutic alteration of β-catenin and c-kit expression by imatinib in p16-positive squamous cell carcinoma compared to HPV-negative HNSCC cells in vitro. Oncol. Rep. 2012, 27, 270–280. [Google Scholar] [CrossRef] [Green Version]
- Lorusso, P.M. Inhibition of the PI3K/AKT/mTOR Pathway in Solid Tumors. J. Clin. Oncol. 2016, 34, 3803–3815. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wang, W. Safety and efficacy of anaplastic lymphoma kinase tyrosine kinase inhibitors in non-small cell lung cancer (Review). Oncol. Rep. 2021, 45, 13–28. [Google Scholar] [CrossRef]
- Kimura, K.; Ikoma, A.; Shibakawa, M.; Shimoda, S.; Harada, K.; Saio, M.; Imamura, J.; Osawa, Y.; Kimura, M.; Nishikawa, K.; et al. Safety, Tolerability, and Preliminary Efficacy of the Anti-Fibrotic Small Molecule PRI-724, a CBP/β-Catenin Inhibitor, in Patients with Hepatitis C Virus-related Cirrhosis: A Single-Center, Open-Label, Dose Escalation Phase 1 Trial. EBioMedicine 2017, 23, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Lenz, H.J.; Kahn, M. Safely targeting cancer stem cells via selective catenin coactivator antagonism. Cancer Sci. 2014, 105, 1087–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Khoueiry, A.B.; Ning, Y.; Yang, D.; Cole, S.; Kahn, M.; Zoghbi, M.; Berg, J.; Fujimori, M.; Inada, T.; Kouji, H.; et al. A phase I first-in-human study of PRI-724 in patients (pts) with advanced solid tumors. J. Clin. Oncol. 2013, 31, 2501. [Google Scholar] [CrossRef]
- Ko, A.H.; Chiorean, E.G.; Kwak, E.L.; Lenz, H.J.; Nadler, P.I.; Wood, D.L.; Fujimori, M.; Inada, T.; Kouji, H.; McWilliams, R.R. Final results of a phase Ib dose-escalation study of PRI-724, a CBP/beta-catenin modulator, plus gemcitabine (GEM) in patients with advanced pancreatic adenocarcinoma (APC) as second-line therapy after FOLFIRINOX or FOLFOX. J. Clin. Oncol. 2016, 34, e15721. [Google Scholar] [CrossRef]
- Deng, J.; Hua, L.; Han, T.; Tian, M.; Wang, D.; Tang, H.; Sun, S.; Chen, H.; Cheng, H.; Zhang, T.; et al. The CREB-binding protein inhibitor ICG-001: A promising therapeutic strategy in sporadic meningioma with NF2 mutations. Neurooncol. Adv. 2020, 2, vdz055. [Google Scholar] [CrossRef] [PubMed]
- Mirghani, H.; Amen, F.; Blanchard, P.; Moreau, F.; Guigay, J.; Hartl, D.M.; Lacau St Guily, J. Treatment de-escalation in HPV-positive oropharyngeal carcinoma: Ongoing trials, critical issues and perspectives. Int. J. Cancer 2015, 136, 1494–1503. [Google Scholar] [CrossRef] [PubMed]
- The Cancer Genome Atlas Program. Available online: https://www.cancer.gov/tcga (accessed on 1 March 2021).
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Crebbp Low | Crebbp High | Total | |
|---|---|---|---|
| Number of patients | 17 | 24 | 41 |
| Age, median (years) | 59.5 | 53.5 | 57.0 |
| Range (years) | 41.1–68.3 | 40.6–71.5 | 40.6–71.5 |
| T4, n | 4 | 4 | 8 |
| T3, n | 3 | 2 | 5 |
| T2, n | 7 | 14 | 21 |
| T1, n | 3 | 3 | 6 |
| Tx, n | 0 | 1 | 1 |
| N3, n | 0 | 1 | 1 |
| N2, n | 13 | 13 | 26 |
| N1, n | 1 | 4 | 5 |
| N0, n | 2 | 6 | 8 |
| Nx, n | 1 | 0 | 1 |
| M0, n | 15 | 23 | 38 |
| Mx, n | 2 | 1 | 3 |
| Patients | 29 | ||
|---|---|---|---|
| Age, median (y) | 63.7 | ||
| Range (y) | 37.0–80.5 | ||
| n | % | ||
| Female | 13 | 44.8 | |
| Male | 16 | 55.2 | |
| T4 | 4 | 13.8 | |
| T3 | 1 | 3.4 | |
| T2 | 15 | 51.7 | |
| T1 | 9 | 31.0 | |
| N3 | 1 | 3.4 | |
| N2 | 13 | 44.8 | |
| N1 | 10 | 34.5 | |
| N0 | 5 | 17.2 | |
| M0 | 29 | 100.0 | |
| PORT | |||
| Yes | 21 | 72.4 | |
| No | 8 | 27.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brkic, F.F.; Stoiber, S.; Maier, T.; Gurnhofer, E.; Kenner, L.; Heiduschka, G.; Kadletz-Wanke, L. Targeting Wnt/Beta-Catenin Signaling in HPV-Positive Head and Neck Squamous Cell Carcinoma. Pharmaceuticals 2022, 15, 378. https://doi.org/10.3390/ph15030378
Brkic FF, Stoiber S, Maier T, Gurnhofer E, Kenner L, Heiduschka G, Kadletz-Wanke L. Targeting Wnt/Beta-Catenin Signaling in HPV-Positive Head and Neck Squamous Cell Carcinoma. Pharmaceuticals. 2022; 15(3):378. https://doi.org/10.3390/ph15030378
Chicago/Turabian StyleBrkic, Faris F., Stefan Stoiber, Tobias Maier, Elisabeth Gurnhofer, Lukas Kenner, Gregor Heiduschka, and Lorenz Kadletz-Wanke. 2022. "Targeting Wnt/Beta-Catenin Signaling in HPV-Positive Head and Neck Squamous Cell Carcinoma" Pharmaceuticals 15, no. 3: 378. https://doi.org/10.3390/ph15030378