
Recent Advances in Hepatocellular Carcinoma Treatment with Radionuclides
1
Institute of Molecular Medicine, College of Life and Health Sciences, Northeastern University, Shenyang 110000, China
2
State Key Laboratory of Drug Research, Molecular Imaging Center, Shanghai Institute of Materia Medica, Chinese Academy of Sciences, Shanghai 201203, China
3
Shandong Laboratory of Yantai Drug Discovery, Bohai Rim Advanced Research Institute for Drug Discovery, Yantai 264117, China
*
Authors to whom correspondence should be addressed.
Pharmaceuticals 2022, 15(11), 1339; https://doi.org/10.3390/ph15111339
Submission received: 29 September 2022
/
Revised: 25 October 2022
/
Accepted: 25 October 2022
/
Published: 28 October 2022
(This article belongs to the Special Issue Molecular Imaging in Oncology: Radiopharmaceuticals for PET and SPECT 2022)
Abstract
:As the third leading cause of cancer death worldwide, hepatocellular carcinoma (HCC) is characterized by late detection, difficult diagnosis and treatment, rapid progression, and poor prognosis. Current treatments for liver cancer include surgical resection, radiofrequency ablation, liver transplantation, chemotherapy, external radiation therapy, and internal radionuclide therapy. Radionuclide therapy is the use of high-energy radiation emitted by radionuclides to eradicate tumor cells, thus achieving the therapeutic effect. Recently, with the continuous development of biomedical technology, the application of radionuclides in treatment of HCC has progressed steadily. This review focuses on three types of radionuclide-based treatment regimens, including transarterial radioembolization (TARE), radioactive seed implantation, and radioimmunotherapy. Their research progress and clinical applications are summarized. The advantages, limitations, and clinical potential of radionuclide treatment of HCC are discussed.
1. Introduction
Hepatocellular carcinoma (HCC) is the third leading cause of cancer death worldwide [1]. HCC is the main histologic type of primary liver cancer, accounting for 70–90% of liver cancer. Cirrhosis is the strongest risk factor of HCC, and the main causes of cirrhosis are chronic hepatitis B (HBV) or hepatitis C (HCV) virus infection, excessive alcohol consumption, and excessive dietary intake of aflatoxins [2,3]. Aflatoxin, a food contaminant produced by Aspergillus molds, has been shown to be an important pathogen in the pathogenesis of HCC. Increased aflatoxin intake is associated with the risk of HCC [4].
Clinical treatments for liver cancer mainly include surgical resection, liver transplantation, radiofrequency ablation (RFA), external radiation therapy, transcatheter arterial chemoembolization (TACE), and targeted drugs such as sorafenib. Sorafenib is a multiple-target tyrosine kinase inhibitor, which can inhibit RAF-1, B-Raf, and kinase activities in the Ras/Raf/MEK/ERK signaling pathway to inhibit tumor cell proliferation, and prolong the overall median survival of patients with advanced HCC [5]. According to the progression, the Barcelona Clinic Liver Cancer (BCLC) classification defines liver cancer into four stages: early (BCLC 0/A), middle (BCLC B), late (BCLC C), and terminal (BCLC D) [6]. For patients with early liver cancer or cirrhosis (BCLC grade 0 or A), surgical resection, liver transplantation, and radiofrequency ablation (RFA) are the main treatments. These treatments are effective and significantly prolong the survival of patients. However, liver cancer is usually asymptomatic or asymptomatic in the early stages. Therefore, most patients are in the middle or late stage at diagnosis, and they are not suitable for the above treatment protocols.
Unlike most cancers, HCC can be diagnosed by imaging without tissue sampling. MRI and CT are clinical methods used to diagnose HCC with an excellent performance. Dynamic MRI has slightly better diagnostic performance than CT imaging. CT has the advantages of a lower cost, higher availability, and faster scanning time [7]. For unresectable HCC (BCLC B), TACE may be used to deliver the drug to the tumor site via the hepatic artery. Considering that the liver cancer cells are mainly supplied by the hepatic artery, the treatment can effectively reduce the damage to normal liver tissue caused by the drug. Patients with TACE failure or BCLC grade C can be treated with systemic therapy agents such as sorafenib [8,9,10,11].
In addition to the above modalities, the therapeutic methods related to radionuclides represent an important research direction in the field of HCC treatment. The main radionuclide-related therapies for HCC include transarterial radioembolization (TARE), intratumoral implantation of radioactive particles, and radioimmunotherapy. The radionuclides commonly used in these treatments are 131iodine (131I), 90yttrium (90Y), 188rhenium (188Re), 166holmium (166Ho), and 125iodine(125I); the related studies and data are shown in Table 1 [12,13,14]. This review article introduces the above three therapeutic methods; summarizes the clinical application status and research progress of related radiopharmaceuticals; and discusses the advantages, limitations, and prospects of radionuclides in the treatment of HCC.
2. Transarterial Radioembolization
TARE is a new modality of radionuclide therapy of HCC [15]. Between 70% and 80% of the blood supply of liver tumors comes from the hepatic artery while normal liver tissue mainly relies on the portal vein for blood supply, with only 20%–30% coming from the hepatic artery [16,17]. According to the differences in the blood supply source between tumor tissue and normal liver tissue [18,19], the injection of radioactive agent into patients through the hepatic artery can deliver more radiation to the tumor site, thus reducing drug-induced hepatotoxicity [20,21].
2.1. TARE-Related Radiation Agents
The main radioactive agents used in TARE are 131I-lipiodol, 90Y-microspheres, 188re-lipiodol, and 166Ho-microspheres. The properties of these radionuclides are shown in Table 1. The beta rays emitted by these radionuclides break the double strands of DNA and kill surrounding cells. TARE allows the drug to be delivered to the tumor to kill more tumor cells and cause less damage to normal tissue [14,22,23,24]. Under normal circumstances, the radiation dose of external radiotherapy is 35 Gy, and the therapeutic effect is limited, with approximately 5% of patients going on to develop radiation-induced liver disease. Internal radiotherapy embolization can increase the radiation dose to 120 Gy or even higher, which not only effectively improves the therapeutic effect but also greatly reduces other side-effects caused by radiation [25,26]. 131I has a long physical half-life of 8.02 days and emits both beta and gamma rays. Patients require hospitalization after 131I injection for radiation protection after treatment. Although 188Re also emits beta and gamma rays, it has a 16.9 h half-life and emits fewer low-energy rays, which means that hospitalization after treatment is unnecessary. 90Y is a pure beta emitter with a physical half-life of 64.1 h. Patients can be discharged quickly after injection without radiological protection [27].
2.1.1. 131I-Lipiodol
131I is the first radionuclide used for transcatheter arteria radioembolization. Lipiodol is a mixture of ethyl iodide of fatty acids from poppy seed oil, which typically contains 37% iodine. It is formed by replacing iodine in lipiodol with radioactive 131I through an atom–atom exchange reaction [28]. 131I-Lipiodol was first applied to humans in 1986 [29]. Intrahepatic arterial injection of 131I-lipiodol is selective and remains in tumors for a long time. Lipiodol is often used as a carrier of anticancer agent and contrast agents for radiography [30].
Studies have shown that 131I-lipiodol treatment is well tolerated. It has little toxic side effects and relieves patients’ pain to a certain extent. In recent studies, 131I-lipiodol has been used either as a single treatment or as an adjuvant treatment along with other regimens.
131I-Lipiodol as a treatment alone can effectively increase the survival rate of patients. In the study by Lintia-Gaultier et al., 50 patients with advanced liver cancer received 131I-lipiodol and 36 patients received only medical support. The 6-month, 1-year, and 2-year survival rates of patients in the 131I-lipiodol group were 65%, 35%, and 22%, respectively, while those in the control group were 28%, 8%, and 0%, respectively. The results indicate that 131I-lipiodol treatment significantly prolongs the survival time of patients with advanced HCC [28].
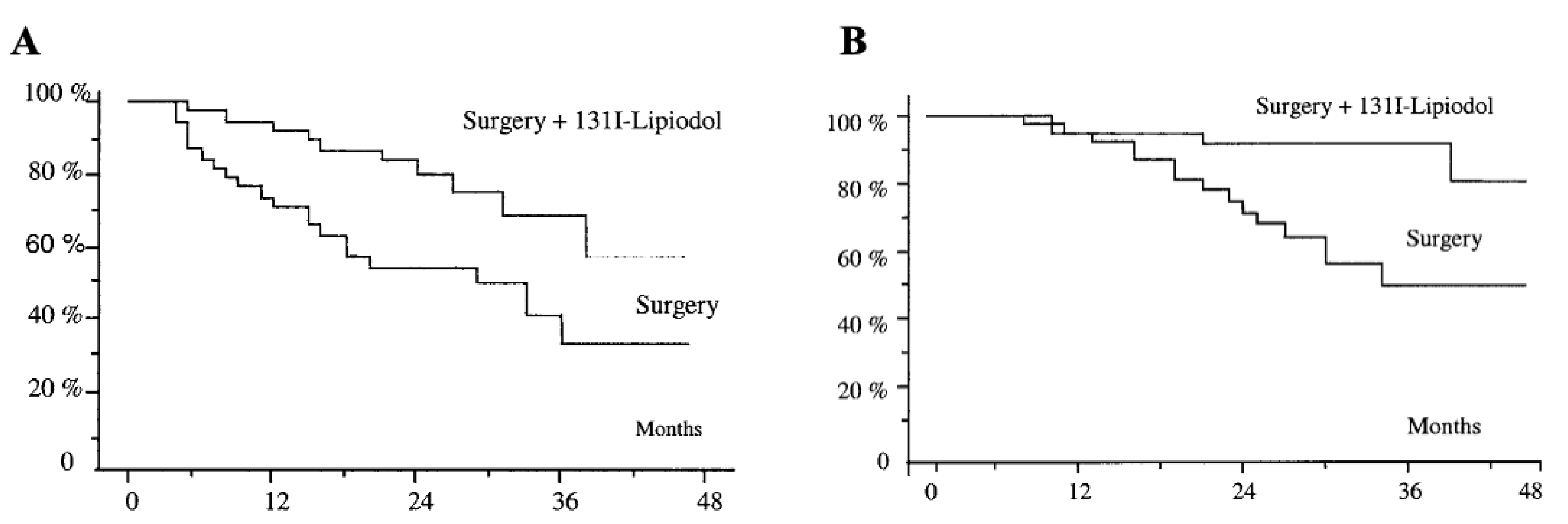
The combination of 131I-lipiodol therapy with other therapies also significantly prolongs the survival time of patients. In the study by Raoul et al., 34 patients were treated with 131I-lipiodol before liver surgery, among whom 25 showed an objective tumor response or histological necrosis of the major lesion site [31]. Boucher et al. conducted a retrospective study of patients treated with 131I-lipiodol after liver resection, and they found that treatment with 131I-lipiodol after surgery prolonged the disease-free and overall survival (Figure 1) [32].
Additionally, several studies have compared 131I-lipiodol therapy with non-radioactive lipiodol therapy. Lipiodol is a radiation carrier for the treatment of unresectable HCC, which is selectively injected into the hepatic artery of HCC patients. Lipiodol has prolonged retention in the tumor, but it shows no obvious anticancer effect. With the addition of 131I, 131I-lipiodol has been proven to be an effective therapeutic agent for HCC. The study by Dumortier et al. compared the efficacy of lipiodol and 131I-lipiodol. Patients with liver cancer (n = 58) were randomly treated with lipiodol or 131I-lipiodol within 6 weeks of tumor resection. The results showed that 131I-lipiodol effectively reduced the recurrence of HCC after hepatectomy, but no significant difference was found in improving the overall survival rate [33]. Moreover, Raoul et al. compared TACE and 131I-lipiodol. The results demonstrated that the 0.5-, 1-, 2-, 3-, and 4-year overall survival rates of patients treated with 131I-lipiodol were 69%, 38%, 22%, 14%, and 10%, respectively, while those of patients in the TACE group were 66%, 42%, 22%, 3%, and 0%, respectively. There was no significant difference in the patient survival between the two treatments, but patients treated with 131I-lipiodol showed better tolerance [29].
Most patients with HCC tolerate 131I-lipiodol therapy well, although interstitial pneumonia is a serious complication that may occur. According to the statistics of Jouneau et al., 15 of 1000 patients developed interstitial pneumonia after treatment and 12 of them died during 1994–2009 [34]. The above 131I-lipiodol-related studies and data are shown in Table 2.
Overall, when 131I-lipiodol is used as a radiopharmaceutical in the treatment of unresectable HCC patients for whom TACE or sorafenib is not appropriate, it can prolong disease-free survival, although its effect on overall survival is limited. Patients treated with 131I-lipiodol had a longer time from clinically confirmed complete remission to lesion recurrence, which greatly reduces the risk of tumor recurrence. Moreover, for patients waiting for liver transplantation, treatment with 131I-Lipiodol during the waiting period can slow tumor growth and metastasis and reduce the risk of being removed from the waiting list. Currently, the application of 131I-lipiodol for treatment HCC still needs the support of more effective clinical data.
2.1.2. 188Re-Lipiodol
In the study of radionuclides applied in the medical field, 188Re is one of the ideal radionuclides used in treatment. It has a half-life of 16.9 h and emits both β and γ rays. Compared to 131I, 188Re has the advantages of a low price, no hospitalization and isolation after treatment, and it is more suitable for Asian and African countries [6]. At present, there are three types of 188Re-related preparations in clinical research, including 188Re-HDD lipiodol, 188Re-SSS lipiodol, and 188Re–DEDC lipiodol. Various methods of labeling lipiodol with 188Re have been proposed. So far, three different 188Re-labeled lipiodol complexes have been tested in humans, namely 188Re-HDD lipiodol, 188Re-SSS lipiodol, and 188Re-DEDC lipiodol. 188Re-HDD lipiodol is the most widely studied compound, but the in vivo stability of this complex is not optimal. Compared with 188Re-HDD lipiodol, 188Re-SSS lipiodol has superior in vivo stability. 188Re-DEDC lipiodol has been tested in animals and humans and showed prolonged retention in tumors with no significant release of the complex after in vivo administration [35].
The 188Re-HDD lipiodol Phase I and II clinical studies sponsored by the International Atomic Energy Agency (IAEA) evaluated the safety and efficacy of transarterial 188Re-HDD lipiodol for treatment-inoperable HCC. In the Phase I clinical trial, 70 patients received at least one 188Re-HDD lipiodol treatment and the results showed a median survival of 9.5 months [36]. The Phase II clinical trial results of the study, published in 2007, show that of the 185 patients from 8 countries who received 188Re iodine oil treatment, the 1-year and 2-year survival rates were 46% and 23%, respectively, with an observed good tolerance [37].
Kostas Delaunay et al. conducted a Phase I study of 188Re-SSS lipiodol for the treatment of HCC. The results show that 188Re-SSS lipiodol has a good biodistribution in radioactive embolism, and, of the radiolabeled lipiodols reported to date, it is the most stable in the body [38]. However, clinical studies of 188Re-DEDC lipiodol only show that it is safe and effective for treating inoperable HCC [39]. Further studies and clinical trial data are required to support the use of 188Re-related lipiodol in HCC. The above 188Re-lipiodol-related studies and data are shown in Table 3.
2.1.3. 90Y-microspheres
90Y-microspheres was first used for tumor treatment in the 1960s [40], and it is the first radionuclide used for the treatment of HCC with portal vein thrombosis [41]. Clinical studies of 90Y-microspheres have been focused on bridging and downgrading in the middle and late stages of HCC and before liver transplantation [42,43]. Currently, 90Y-microspheres for the treatment of HCC are mainly made of glass and resin. 90Y-glass microspheres were approved by the Food Drug Administration (FDA) in 1999 for the adjuvant therapy of unresectable HCC and bridging liver transplantation, and it was later approved for the treatment of HCC with portal vein thrombosis. 90Y-resin microspheres were approved by the FDA in 2002 to be used along with fluorouridine for treating liver metastatic colorectal cancer [44,45]. 90Y-glass microspheres range from 20 to 30 microns, whereas 90Y-resin microspheres are usually 20 to 60 microns. The radiation activity of the 90Y-glass microspheres generally used is 2500 Bq while that of 90Y-resin microspheres is only 50 Bq [46,47].
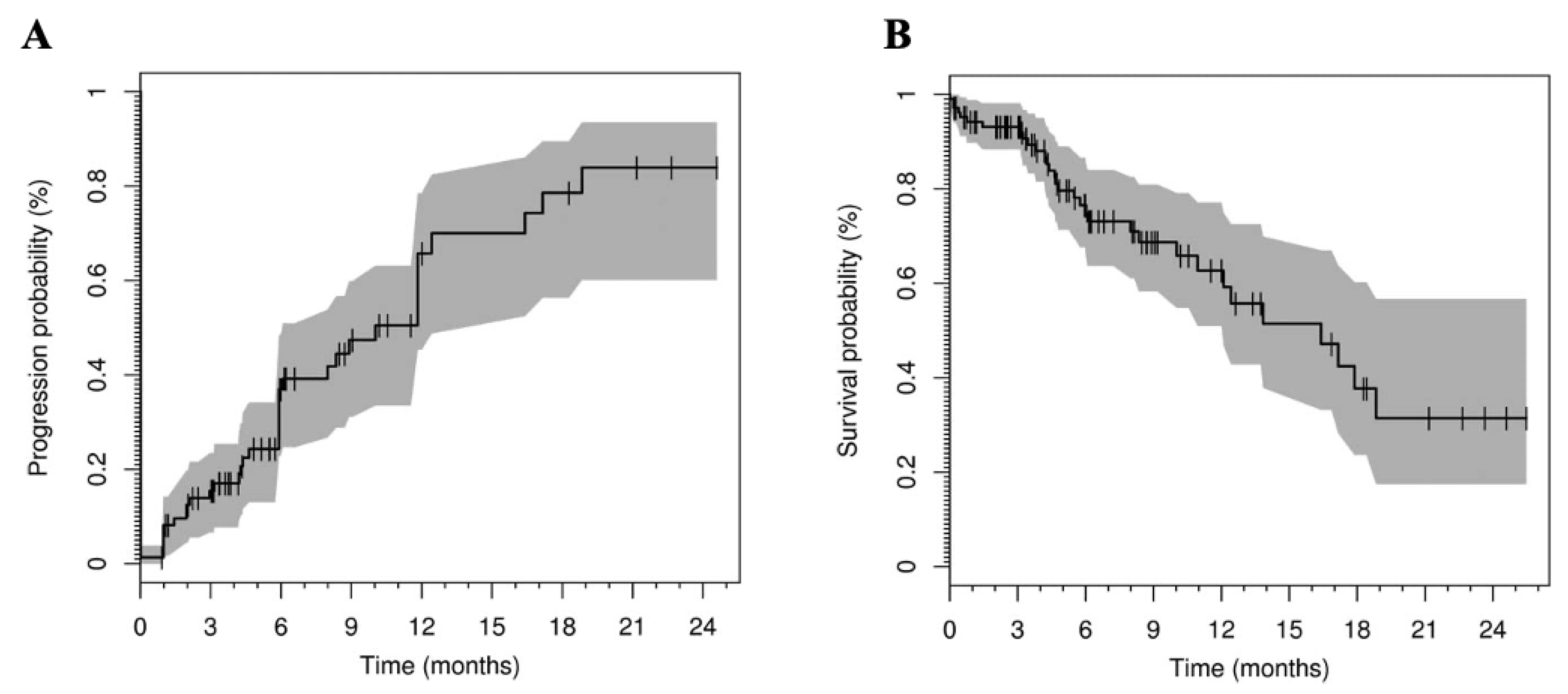
In 2018, the American Association for the Study of Liver Diseases recommended the use of 90Y-microspheres TARE as the first-line treatment for HCC [15]. The institute determined the overall survival of patients with HCC who received 90Y-microspheres radionuclide embolization between 2003 and 2017 according to the BCLC staging. The overall survival of BCLC A, B, and C was 47.3 (39.5–80.3 months), 25.0 (17.3 to 30.5 months), and 15.0 months (13.8 to 17.7 months), respectively. The efficacy of the 90Y-microspheres TARE treatment for HCC has been confirmed by several studies. Hilgard et al. analyzed the data from 108 patients with advanced liver cancer and cirrhosis who received 90Y-microspheres TARE. According to the European Association for the Study of the Liver (EASL) criteria, the patients with a complete response, partial response, and disease stability accounted for 3%, 37%, and 53%, respectively, and 6% of the patients showed primary progression. The median progression time was 10 months and the median survival time was 6.4 months. In this study, the time to progression (TTP) and survival data of patients with advanced HCC were analyzed. It was found that the efficacy of 90Y-microspheres TARE was comparable to that of systemic therapy for patients with advanced HCC (Figure 2) [48]. D’Avola et al. demonstrated that 90Y-microspheres TARE extends the median survival compared to conventional care alone. This study compared the overall survival of 35 patients with unresectable HCC who received 90Y-microspheres treatment with 43 patients who received routine care only. The results showed that the median survival time was 16 months in the embolization group versus only 8 months in the control group [49].
Additionally, 90Y-microspheres TARE is used as an adjunctive therapy for preoperative bridging and degradation in patients awaiting liver transplantation. Gabr et al. performed a study of 90Y-microspheres for the treatment of liver transplantation patients from 2004 to 2018, among which 169 of 207 patients were treated with 90Y-microspheres TARE before liver transplantation, and another 38 patients received liver transplantation after staging was reduced by 90Y-microspheres TARE. According to the histopathology, 94 patients had complete necrosis of the tumor, accounting for 45% of the total patients; 60 patients had major necrosis of tumor tissue; and only 53 patients had local necrosis, accounting for 23%. The 3-, 5-, and 10-year survival rates were 84%, 77%, and 60% for patients with complete, major, and partial tumor necrosis, respectively. These results suggest that 90Y-microspheres TARE as an emerging adjunctive therapy is highly effective for bridging or reducing staging before liver transplantation [50]. Levi Sandri et al. also published similar data following a review of 20 global studies on 90Y-microspheres TARE as bridging and staging reduction for liver transplantation. A total of 178 patients were treated with 90Y-microspheres TARE before liver transplantation. The statistical results showed that 90Y-microspheres TARE was more effective than TACE in patients with advanced HCC (BCLC C) [51].
90Y-microspheres TARE is also used to treat patients with HCC with iatrogenic acute liver failure and portal vein thrombosis (PVT). 90Y-microspheres is the first radiopharmaceutical to be used for the treatment of HCC with PVT. According to the statistics of Ozkan et al., among 29 patients with HCC treated with 90Y-microspheres TARE between 2009 and 2014, PVT was formed in 12 patients, and the median survival was 17 ± 2.5 months. The statistical results showed that PVT formation is not an important factor affecting prognosis, and that 90Y-microspheres TARE treatment did not affect the median survival time of patients with PVT; however, TACE was contraindicated [52]. Similar results were found in a retrospective analysis published in 2010 by Inarrairaegui et al. The authors analyzed the data of 25 patients with PVT-formed HCC treated with 90Y-microspheres TARE. The statistical results demonstrated that the treatment of the PVT-formed HCC was well tolerated and had a favorable median survival. No hepatotoxicity was observed after 1–2 months of treatment, and the median survival of the patients was 10 months. However, the statistical results lacked further validation [53].
Whether 90Y-microspheres TARE combined with other methods is better than single therapy for HCC remains to be determined. Sorafenib and Micro-therapy Guided by Primovist Enhanced MRI in Patients With Inoperable Liver Cancer (SORAMIC) is a multicenter, randomized controlled trial for treating HCC that combines 90Y-microspheres TARE with sorafenib. In this study, a total of 424 patients with advanced HCC were randomized to 90Y-resin microspheres along with sorafenib treatment or sorafenib alone. The results showed that the median survival was 12.1 months in the combination group and 11.4 months in the other group, suggesting that the combination therapy showed no significant improvement regarding the survival of the patients [54].
Researchers have also tried combining this treatment with the PD-1 inhibitor in a clinical study. PD-1 inhibitors are important immunosuppressive molecules that help immune cells in the body recognize and kill tumors. Nivolumab, a PD-1 inhibitor approved by the FDA in 2015, is aimed at patients with advanced HCC who have been treated with sorafenib. In 2018, Wehrenberg-klee reported a case in which a patient was successfully bridged for partial hepatectomy using 90Y-microspheres TARE combined with PD-1 inhibitor therapy. The combined use of 90Y-microspheres with nivolumab or other immunotherapies may help improve the efficiency and degree of response to HCC therapy, enhance the ability to deliver radiation doses to tumors, and mediate other possible pro-inflammatory effects of embolism. Therefore, 90Y-microspheres TARE combined with immunotherapy may have an impact on advanced HCC [55].
Compared to TACE, 90Y-microspheres TARE does not significantly extend the total survival time of patients, but it is obviously superior to TACE in prolonging the time before progression. According to a Phase II clinical trial by Salem et al., between 2009 and 2015, 179 BCLC A or B patients with HCC were randomized to conventional TACE or 90Y-microspheres TARE. The results showed that the median progression time in the 90Y-microspheres TARE group was longer than 26 months while that in the TACE group was only 6.8 months [56]. Salem et al. retrospectively analyzed the data of 245 patients with HCC, including 122 who received TACE and 123 who received 90Y-microspheres TARE. The median progression time was 13.3 months in the 90Y-microsphere TARE group and 8.4 months in the TACE group while the median survival time was 20.5 months in the 90Y-microspheres TARE group and 17.4 months in the TACE group [57]. These studies showed that 90Y-microspheres TARE significantly prolongs the median progression time in patients with HCC.
Although 90Y-microspheres TARE has no significant improvement on the survival of patients compared to the traditional drug sorafenib, 90Y-microspheres TARE significantly increases the tumor response, reduces the occurrence of adverse events, and improves patients’ quality of life. This conclusion is supported by two large randomized controlled clinical trials. Chow et al. reported a Phase III trial in which 360 patients with HCC from 11 countries in the Asia-Pacific region were randomly assigned to be treated with 90Y-microspheres TARE or sorafenib. The results showed that the median survival was 8.8 months for patients treated with 90Y-microspheres TARE while that of patients treated with sorafenib was 10 months, indicating that there was no significant difference in extending the median survival in patients with locally advanced HCC [58]. Moreover, a Phase III clinical trial in Germany on advanced HCC with TARE examined 467 patients with advanced HCC who were randomized to receive 90Y resin-based microspheres or sorafenib treatment. The median survival time was 8 months for patients treated with 90Y resin-based microspheres TARE while that of patients treated with sorafenib was 9.9 months. The results demonstrate that there is no significant difference between the two treatments in extending the median survival of patients [59].
Patients with HCC who are treated with 90Y-microspheres TARE may have minimal adverse effects with less severe symptoms, including fatigue, nausea, vomiting, anorexia, fever, and abdominal discomfort; these symptoms are less likely to occur and generally do not require hospitalization. More serious symptoms include hepatic dysfunction, biliary toxicity, fibrosis, radiation pneumonitis, gastrointestinal complications, and vascular injury [44]. However, the probability of these serious side effects is extremely low, with less than 4% of liver disease cases being induced by radiation. According to Salem et al., less than 2% of patients require interventional therapy due to biliary toxicity induced by radioembolization, and the incidence of radiation pneumonitis induced by radioembolization is less than 1% [60,61,62,63]. Kallini et al. performed a retrospective analysis to determine whether there is a safety difference between 90Y-glass microspheres and 90Y-resin microspheres. A total of 1579 patients in 24 studies were treated with 90Y-glass microspheres, and 720 patients in 9 studies were treated with resin microspheres. The statistical results showed that compared to the 90Y-resin microspheres, 90Y-glass microspheres have a lower incidence of gastrointestinal and pulmonary adverse events for the treatment of HCC [64]. The 90Y-microspheres-TARE-related studies and data are detailed in Table 4.
90Y-microspheres TARE treatment is not significantly different from TACE or sorafenib treatment in terms of extending the overall survival in patients. TACE is used for bridging or degrading before liver transplantation, reducing the risk of patients being disqualified from transplantation due to tumor progression while waiting for liver transplantation. For patients with HCC with PVT, the replacement of TACE with 90Y-microspheres TARE does not affect the median survival. Patients with advanced HCC who are not responding to TACE or sorafenib may also be considered for treatment with 90Y-microspheres TARE. The phase of the use of 90Y-microspheres TARE in the standardized treatment of HCC is not clear yet, and there are also uncertainties about the prognostic effect of 90Y-microspheres TARE in different HCC patients.
2.1.4. 166Ho-Microspheres
At present, there are three types of commercial radioactive microspheres, namely, 90Y-resin microspheres, 90Y-glass microspheres, and 166Ho-poly-l-lactic acid microspheres. 166Ho emits 81 keV gamma photons when it decays and is also a lanthanide element, and it can be imaged by single-photon emission computed tomography (SPECT)/magnetic resonance imaging (MRI) [65].
The Holmium Embolization Particles for Arterial Radiotherapy (HEPAR) trial is a Phase I clinical trial of 166Ho-microspheres, which eventually determined the maximum radiation dose tolerated by the 166Ho-microspheres to be 60 Gy [66]. Among the 37 patients in Phase II of the HEPAR trial, 73% of the patients showed complete remission, partial remission, or a stable condition after 3 months of treatment. Additionally, the adverse event rate is comparable to that of known 90Y-microspheres TARE therapy [67]. More Phase II trials of 166Ho-microspheres are underway.
3. Radioactive Seed Implantation
Radioactive seed implantation relies on stereoscopic imaging equipment to implant radioactive seed into the tumor for eradication by radiation. The research of 125I seed implantation for the treatment of HCC has increased in recent years.
The 125I seeds are prepared by wrapping a titanium alloy around a silver rod with 125I. This technique relies on B-scan ultrasonography, computed tomography (CT), MRI, and other imaging equipment to guide the 125I seed into the tumor tissue, through which the 125I seed continues to emit low-dose γ rays to treat the tumor. 125I has a long half-life of 60.1 days, which allows it to function continuously in tumor tissue. Additionally, the radiation distance of 125I is only 1.7 cm, which causes a low level of damage to normal tissue [68,69]. Recent studies of 125I seed implantation for the treatment of HCC have focused on the combination of other therapies. Among them, 125I seed implantation combined with TACE, RFA and surgical treatment, or treatment of PVT-formed HCC is the focus of research.
125I seed implantation combined with TACE therapy has received considerable attention, with some studies showing that 125I seed implantation combined with TACE is safe and effective for treating HCC, with a significantly prolonged total and progression-free survival time. Zhang et al. collected clinical data from 110 patients with advanced primary liver cancer from 2014 to 2016, among whom 55 patients received 125I seed implantation plus TACE and 3D conformal radiotherapy while the other 55 patients received TACE plus 3D conformal radiotherapy. The results showed that the objective remission rate of the 125I seed implantation plus TACE and 3D conformal radiotherapy group was 84% while the disease control rate was 96%. However, patients that only received TACE plus 3D conformal radiotherapy showed a conventional objective response rate of 64%, and the disease control rate was 84%, respectively. The results showed that 125I seed implantation combined with conventional treatment can significantly prolong the overall and progression-free survival [70]. In the work of Fang et al., 76 patients with HCC with PVT received TACE plus RFA or 125I seed implantation plus TACE and RFA treatment, respectively; the median survival was 30 and 42 months and the median progression-free period was 11 and 18 months, respectively. These results further validate the safety and efficacy of the combination of the three therapies [71].
Some patients with HCC can be treated with 125I seed implantation after RFA treatment; however, the effect of this combination therapy on patient survival rates has shown variability across studies. In a randomized trial by Chen et al., 136 patients with HCC were randomly divided into two groups: One group received 125I seed implantation therapy after RFA treatment while the other was treated with RFA only. The results showed that the survival rate of the RFA plus 125I seed implantation group was obviously better than that of the single RFA group [72]. However, a randomized controlled trial conducted by Wu et al. showed that the progression-free survival was 18 months in the combined treatment group, which was 7 months longer than that in the RFA group, but there was no significant difference in the overall survival between the two groups [73]. In another clinical trial of 125I seed implantation by Chen et al., 68 patients with HCC undergoing surgery were randomly assigned to receive 125I seed implantation or medical support. The relapse time of the two groups was 60 and 36.7 months, respectively, and the 1-, 3-, and 5-year survival rates were 94%, 74%, and 56%, and 88%, 53%, and 29%, respectively. The results showed that 125I seed implantation therapy after surgery can significantly prolong the disease-free survival and overall survival in patients with HCC [74]. Currently, the study of 125I seed implantation combined with RFA or surgical treatment is unsatisfactory, and more clinical data and statistical analysis are needed to obtain a clear conclusion on the effects on survival.
Additionally, studies have examined the use of 125I seed implantation to treat PVT-formed HCC. The available data only shows that it is safe for use in these patients but does not determine whether it is effective. According to the statistical results of research by Zhang et al. on six related studies, 406 patients with HCC with PVT received 125I seed implantation treatment. The side effects of radiation included leukopenia while the adverse reactions associated with 125I seed implantation included fever, abdominal pain, bleeding, and anorexia. No stent or particle migration was reported in these patients. The results indicated that the use of 125I seed implantation is safe in patients with HCC [75], but the efficacy of the treatment needs to be determined in more clinical trials. The relevant studies and data of 125I seed implantation are detailed in Table 5.
125I seed implantation has advantages, including less trauma, a uniform distribution in the tumor, less damage to normal tissue, reduced treatment time, fewer treatments, and no isolation after treatment. This approach can be used to treat inoperable HCC or PVT-formed HCC that does not respond to TACE or sorafenib treatment. However, based on the current studies, more clinical data are needed to support the safety and efficacy of 125I seed implantation.
4. Radioimmunotherapy
Radioimmunotherapy can be used as a means to treat tumors with radionuclide-labeled antibodies. HCC-targeted antibodies labeled with 131I have been intensively studied for the treatment of HCC, with the most common antibodies including mouse anti-human monoclonal antibody fragment HAb18F(ab)2 (metuximab), ChTNT human-mouse chimeric antibody, hepama-1 HCC cell membrane monoclonal antibody, CD133 monoclonal antibody, anti-hepatitis B virus antibodies, anti-machine protein monoclonal antibody, and anti-human HCC transferrin monoclonal antibody. Radioimmunotherapy agents used for HCC with clinical trials include 131I-metuximab, 131I-chTNT, and 131I-hepama-1 monoclonal antibody [76,77].
4.1. 131I-Metuximab
Metuximab is a mouse anti-human monoclonal antibody fragment HAb18F (ab)2, the antigen of which is HAb18G/CD147, which has high expression in liver cancer, colon cancer, and cervical cancer, among others. HAb18G/CD147 is a highly glycosylated cell surface transmembrane protein belonging to the immunoglobulin superfamily. It has been reported that the high expression of CD147 is closely related to the invasion, metastasis, and growth of tumors and is a significant independent predictor. It has been reported that blocking HAb18G/CD147 expression with 131I-metuximab effectively inhibits HCC growth and metastasis in vivo [78].
Studies on the safety and efficacy of 131I-metuximab for the treatment of HCC have shown no life-threatening toxicity. In a Phase I clinical trial published by et al., the safe dose of 131I-metuximab was 27.75 MBq/kg. In the subsequent multicenter Phase II trial, of 73 tracked patients, 6 showed partial remission (8%), 14 showed mild remission (19%), and 43 were in a stable condition (59%), with a 21-month survival rate of 45% [79].
Studies have shown that combined treatment with 131I-metuximab and TACE improved the survival and delayed recurrence in patients with unresectable HCC. Ma et al. conducted a Phase IV clinical trial of 131I-metuximab along with TACE for the treatment of inoperable HCC. In this multicenter, open-label clinical trial, 341 patients with stage III/IV HCC were non-randomly assigned to the trial group (n = 167) and the control group (n = 174) to receive combination therapy of 131I-metuximab plus TACE or TACE alone. It was found that 131I-metuximab combined with TACE improved the 1-year survival rate and prolonged the time of tumor progression, and the 1-year survival rate of the experimental group was 79.47% while that of the control group was 65.59%. The time of progression in the experimental group was 6.82 ± 1.28 months, which was approximately 2 months longer than that of the control group [80]. Similar results were found in the studies of He et al., in which 185 patients with unresectable HCC were treated with 131I-metuximab plus TACE (95) or with TACE alone (90). The 1-month effective rate was 71% in the trial group and 39% in the control group. The 6-, 9-, and 12-month survival rates in the combined treatment group were 86%, 74%, and 60%, respectively, while those in the control group were 60%, 42%, and 34%, respectively. The results of this study showed that the combination of 131I-metuximab plus TACE significantly increased the efficacy within 1 month and prolonged the survival of patients with HCC compared to those with TACE alone [81].
Delaying the recurrence of HCC is the key to the treatment of HCC. Treatment with 131I- metuximab after liver transplantation or RFA is helpful to reduce recurrence. In the study by Xu et al., 60 patients with HCC with liver transplantation were randomly divided into two groups. The treatment group received 131I-metuximab at 15.4 MBq/kg 3 weeks after liver transplantation and the control group was given a placebo intravenously. At the 1-year follow-up, compared to the control group, the recurrence rate was significantly reduced by 30% and the survival rate increased by 21% in the treatment group. The results showed that 131I-metuximab is effective in reducing tumor recurrence and improving the survival rate in patients with HCC after transplantation [82]. Moreover, Bian et al. evaluated the efficacy of 131I-metuximab along with RFA for the treatment of HCC. In this study, 127 patients with HCC with stage 0-B BCLC were randomly divided into two groups. One group received RFA followed up with 131I-metuximab while the other group received only RFA. The results showed that the 1- and 2-year recurrence rates were 32% and 59% in the combined group and 56% and 71% in the RFA group, respectively. The median time of recurrence was 17 and 10 months in both groups. The results of this study suggest that the use of 131I-metuximab after RFA may be helpful in the prevention of postoperative recurrence [83].
4.2. 131I-chTNT
ChTNT is a mouse chimeric antibody. When labeled with 131I, the 131I-chTNT antibody binds to intracellular antigens in the necrotic part of the tumor. Intracellular antigen is a complex of double-stranded DNA and histone H1 antigen that is present in scattered areas of degenerated or necrotic cells within a tumor. The antibodies commonly used in targeted therapies primarily bind to antigens on the surface of tumor cells, but TNT antibodies can bind to intracellular antigens at the site of tumor necrosis. 131I acts to treat the surrounding tumor cells, causing new necrosis, while the chTNT monoclonal antibody expands to the newly necrotic area to continuously expand it to achieve the therapeutic goal. At present, 131I-chTNT is considered to have a therapeutic effect on lung cancer, brain cancer, and liver cancer, among others [76,80].
Data from patients with HCC treated with 131I-chTNT were retrospectively analyzed by Tu et al. Among 38 patients with HCC, 22 were treated with RFA only while the other 16 patients were treated with RFA plus 131I-chTNT. The median survival of the two groups was 37 and 43 months, respectively, while the 1-, 2-, and 3-year overall survival rates were 100%, 88%, and 75% (RFA plus 131I-chTNT), and 82%, 58%, and 52% (RFA). The retrospective analysis showed that RFA combined with 131I-CHTNT prolongs disease-free survival in the short term, better than RFA alone. However, a randomized controlled trial with a larger sample is needed to assess the efficacy of the treatment [84].
4.3. 131I-Hepama-1 mAb
Hepama-1 is a monoclonal antibody against the HCC cell membrane. HAb18G/CD147 is a highly glycosylated cell surface transmembrane protein belonging to the immunoglobulin superfamily. It has been reported that the high expression of CD147 is closely related to the invasion, metastasis, and growth of tumors and is a significant independent predictor. It has been reported that blocking HAb18G/CD147 expression with 131I-metuximab effectively inhibits HCC growth and metastasis in vivo [85]. Several studies in the late 1990s investigated the value of 131I-hepama-1 monoclonal antibodies in treating HCC. A Phase I trial conducted by Chen et al. treated 45 patients with HCC who could not be treated surgically with 131I-hepama-1 mAb. The results demonstrate that 131I-hepama-1 mAb is safe by intravenous injection, and the recommended dose of 131I-hepama-1 mAb is 1480–2960 MBq/10 mg [86]. The accompanying radioimmunoassay-related studies and data are detailed in Table 6.
Through an extensive literature review, it was found that the efficacy of radioimmunotherapy for the treatment of solid tumors needs to be improved. On this occasion, some in vivo studies have demonstrated the safety of radioimmunotherapy. For patients with HCC who are unamenable to surgical resection or monotherapy, a combination of radioimmunotherapy may be considered. The efficacy of the treatment is affected by several factors, including the targeting ability of monoclonal antibodies, the stability of the radioimmunoconjugate in vivo, and the mode of administration. The development of more targeted monoclonal antibodies for HCC, improvement of the radiochemical stability of the radiolabeled MAbs, and identification of suitable administration routes are future directions that require further investigations.
5. Summary and Future Prospects
TARE is well-tolerated and has few side effects in the treatment of advanced HCC. Although it has no obvious survival benefit compared to TACE or sorafenib in clinical trials, TARE can prolong disease-free survival and improve patients’ quality of life. Moreover, TARE may be considered in cases with PVT formation, failure of TACE/sorafenib therapy, bridging liver transplantation, or reduced-grade liver transplantation. 90Y-microspheres TARE is one of the most promising approaches of translating radionuclide therapy for HCC into routine treatment practice. However, the proper use of 90Y-microspheres TARE in the standardized treatment of HCC has not been cleared, and there are also uncertainties about the prognostic effect of 90Y-microspheres TARE in different HCC patients. 125I seed implantation and 131I-metuximab radioimmunotherapy for HCC have gained increasing attention, but their efficacy requires clinical validation by further randomized controlled trials. Clinical trials on nuclide treatment for liver cancer have mainly included TARE and radioactive seed implantation until now. There are 21 ongoing clinical trials of TARE for liver cancer, mainly on 90Y TARE. 90Y TARE has been demonstrated to be more effective and less toxic than TACE. In addition, clinical trials on the 166Ho radio-embolism and the combination of sorafenib with 90Y radio-embolism are also underway. There are five clinical trials on radioactive seed implantation, mainly conducted around 125I. The above information about clinical trials comes from Clinicaltrials.gov. The use of radionuclides carries a certain risk to medical staff, and how to regulate the operation during treatment for risk mitigation is worthy of attention.
Author Contributions
Formal analysis, R.L. and H.L. (Hong Li); resources, R.L. and H.L. (Hong Li); writing-original draft preparation, R.L. and H.L. (Hong Li); writing-review and editing, H.L. (Hongguang Liu) and Z.C.; visualization, R.L. and Y.Q.; supervision, H.L. (Hongguang Liu) and Z.C.; project administration, H.L. (Hongguang Liu) and Z.C.; funding acquisition, Z.C.; All authors have read and agreed to the published version of the manuscript.
Funding
We thank funding from the National Natural Science Foundation of China (U2267221) and Shanghai Municipal Science and Technology Major Project (N/A).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing not applicable.
Conflicts of Interest
The authors declare no conflict of interest, financial or otherwise.
References
- Gans, J.H.; Lipman, J.; Golowa, Y.; Kinkhabwala, M.; Kaubisch, A. Hepatic Cancers Overview: Surgical and Chemotherapeutic Options, How Do Y-90 Microspheres Fit in? Semin. Nucl. Med. 2019, 49, 170–181. [Google Scholar] [CrossRef] [PubMed]
- Lafaro, K.J.; Demirjian, A.N.; Pawlik, T.M. Epidemiology of Hepatocellular Carcinoma. Surg. Oncol. Clin. North Am. 2015, 24, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Moradpour, D.; Blum, H.E. Pathogenesis of hepatocellular carcinoma. Eur. J. Gastroenterol. Hepatol. 2005, 17, 477–483. [Google Scholar] [CrossRef]
- Magnussen, A.; Parsi, M.A. Aflatoxins, hepatocellular carcinoma and public health. World J. Gastroenterol. 2013, 19, 1508–1512. [Google Scholar] [CrossRef]
- Tang, W.; Chen, Z.; Zhang, W.; Cheng, Y.; Zhang, B.; Wu, F.; Wang, Q.; Wang, S.; Rong, D.; Reiter, F.P.; et al. The mechanisms of sorafenib resistance in hepatocellular carcinoma: Theoretical basis and therapeutic aspects. Signal Transduct. Target. Ther. 2020, 5, 87. [Google Scholar] [CrossRef]
- Andreana, L.; Isgrò, G.; Marelli, L.; Davies, N.; Yu, D.; Navalkissoor, S.; Burroughs, A.K. Treatment of hepatocellular carcinoma (HCC) by intra-arterial infusion of radio-emitter compounds: Trans-arterial radio-embolisation of HCC. Cancer Treat. Rev. 2012, 38, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Willatt, J.; Ruma, J.A.; Azar, S.F.; Dasika, N.L.; Syed, F. Imaging of hepatocellular carcinoma and image guided therapies—How we do it. Cancer Imaging 2017, 17, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forner; Alejandro; Reig; María; Bruix; Jordi. Hepatocellular carcinoma. Lancet Lond. 2018, 391, 1301–1314. [Google Scholar] [CrossRef]
- Grandhi, M.S.; Kim, A.K.; Ronnekleiv-Kelly, S.M.; Kamel, I.R.; Ghasebeh, M.A.; Pawlik, T.M. Hepatocellular carcinoma: From diagnosis to treatment. Surg. Oncol. 2016, 25, 74–85. [Google Scholar] [CrossRef]
- Gbolahan, O.B.; Schacht, M.A.; Beckley, E.W.; Laroche, T.P.; O’Neil, B.H.; Pyko, M. Locoregional and systemic therapy for hepatocellular carcinoma. J. Gastrointest. Oncol. 2017, 8, 215. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Marrero, J.; Renz, J.; Lencioni, R. Hepatocellular carcinoma tumor board: Making sense of the technologies. Am. Soc. Clin. Oncol. Educ. Book 2015, 35, e213–e220. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Shen, F.; Xia, Y.; Yang, Y.F. Evolving Role of Radiopharmaceuticals in Hepatocellular Carcinoma Treatment. Anti-Cancer Agents Med. Chem. (Former. Curr. Med. Chem.-Anti-Cancer Agents) 2016, 16, 1155–1165. [Google Scholar] [CrossRef] [PubMed]
- Gallicchio, R.; Nardelli, A.; Mainenti, P.; Nappi, A.; Storto, G. Therapeutic Strategies in HCC: Radiation Modalities. BioMed Res. Int. 2016, 2016, 1295329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, S.; Hoffmann, K.; Schemmer, P. Treatment of Hepatocellular Carcinoma: A Systematic Review. Liver Cancer 2012, 1, 144–158. [Google Scholar] [CrossRef]
- Salem, R.; Gabr, A.; Riaz, A.; Mora, R.; Ali, R.; Abecassis, M.; Hickey, R.; Kulik, L.; Ganger, D.; Flamm, S. Institutional decision to adopt Y90 as primary treatment for hepatocellular carcinoma informed by a 1000-patient 15-year experience. Hepatology 2018, 68, 1429–1440. [Google Scholar] [CrossRef] [Green Version]
- Howard, R.; Lb, R.; Keith, H.; Grady, A. Studies on the Blood Supply of Tumors in Man. III. Vascular Patterns of the Liver by Hepatic Arteriography in Vivo. JNCI: J. Natl. Cancer Inst. 1951, 12, 107–131. [Google Scholar]
- Breedis, C.; Young, G. The blood supply of neoplasms in the liver. Am. J. Pathol. 1954, 30, 969–985. [Google Scholar]
- Salem, R.; Thurston, K.G. Radioembolization with 90yttrium microspheres: A state-of-the-art brachytherapy treatment for primary and secondary liver malignancies. Part 2: Special topics. J. Vasc. Interv. Radiol. 2006, 17, 1425–1439. [Google Scholar] [CrossRef] [Green Version]
- Fidelman, N.; Kerlan, R.K. Transarterial Chemoembolization and (90)Y Radioembolization for Hepatocellular Carcinoma: Review of Current Applications Beyond Intermediate-Stage Disease. Ajr Am. J. Roentgenol. 2015, 205, 742–752. [Google Scholar] [CrossRef]
- Gomaa, A.I.; Waked, I. Recent advances in multidisciplinary management of hepatocellular carcinoma. World J. Hepatol. 2015, 7, 673–687. [Google Scholar] [CrossRef]
- Wang, E.A.; Stein, J.P.; Bellavia, R.J.; Broadwell, S.R. Treatment options for unresectable HCC with a focus on SIRT with Yttrium-90 resin microspheres. Int. J. Clin. Pract. 2017, 71, e12972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, A.W.; Chawla, S.; Qu, Z.; Kashyap, R.; Milano, M.T.; Hezel, A.F. Stereotactic Hypofractionated Radiation Therapy as a Bridge to Transplantation for Hepatocellular Carcinoma: Clinical Outcome and Pathologic Correlation. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 895–900. [Google Scholar] [CrossRef] [PubMed]
- D’Huyvetter, M.; Xavier, C.; Caveliers, V.; Lahoutte, T.; Muyldermans, S.; Devoogdt, N. Radiolabeled nanobodies as theranostic tools in targeted radionuclide therapy of cancer. Expert Opin. Drug Deliv. 2014, 11, 1939–1954. [Google Scholar] [CrossRef] [PubMed]
- Bouvry, C.; Palard, X.; Edeline, J.; Ardisson, V.; Loyer, P.; Garin, E.; Lepareur, N. Transarterial Radioembolization (TARE) Agents beyond 90 Y-Microspheres. BioMed Res. Int. 2018, 2018, 1435302. [Google Scholar] [CrossRef] [Green Version]
- Lau, W.Y.; Lai, E.C.H.; Leung, T.W.T. Current role of selective internal irradiation with yttrium-90 microspheres in the management of hepatocellular carcinoma: A systematic review. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 460–467. [Google Scholar] [CrossRef]
- Tomé, W.; Fenwick, J.D. Analysis of radiation-induced liver disease using the lyman ntcp model: In regard to dawson et al. ijrobp 2002;53:810–821. Int. J. Radiat. Oncol. Biol. Phys. 2004, 58, 1318–1319. [Google Scholar] [CrossRef]
- Raoul, J.L.; Boucher, E.; Rolland, Y.; Garin, E. Treatment of hepatocellular carcinoma with intra-arterial injection of radionuclides. Nat. Rev. Gastroenterol. Hepatol. 2010, 7, 41–49. [Google Scholar] [CrossRef]
- Lintia-Gaultier, A.; Perret, C.; Ansquer, C.; Eugène, T.; Kraeber-Bodéré, F.; Frampas, E. Intra-arterial injection of 131I-labeled Lipiodol for advanced hepatocellular carcinoma: A 7 years’ experience. Nucl. Med. Commun. 2013, 34, 674–681. [Google Scholar] [CrossRef]
- Raoul, J.; Guyader, D.; Bretagne, J.; Heautot, J.; Duvauferrier, R.; Bourguet, P.; Bekhechi, D.; Deugnier, Y.M.; Gosselin, M. Prospective randomized trial of chemoembolization versus intra-arterial injection of 131I-labeled-iodized oil in the treatment of hepatocellular carcinoma. Hepatology 1997, 26, 1156–1161. [Google Scholar] [CrossRef]
- Nakakuma, K.; Tashiro, S.; Hiraoka, T.; Ogata, K.; Ootsuka, K. Hepatocellular carcinoma and metastatic cancer detected by iodized oil. Radiology 1985, 154, 15–17. [Google Scholar] [CrossRef]
- Raoul, J.L.; Messner, M.; Boucher, E.; Bretagne, J.F.; Campion, J.P.; Boudjema, K. Preoperative treatment of hepatocellular carcinoma with intra-arterial injection of 131I-labelled lipiodol. Br. J. Surg. 2003, 90, 1379–1383. [Google Scholar] [CrossRef] [PubMed]
- Boucher, E.; Corbinais, S.; Rolland, Y.; Bourguet, P.; Guyader, D.; Boudjema, K.; Meunier, B.; Raoul, J.L. Adjuvant intra-arterial injection of iodine-131-labeled lipiodol after resection of hepatocellular carcinoma. Hepatology 2003, 38, 1237–1241. [Google Scholar] [CrossRef] [PubMed]
- Dumortier, J.; Decullier, E.; Hilleret, M.N.; Bin-Dorel, S.; Valette, P.J.; Boillot, O.; Partensky, C.; Letoublon, C.; Ducerf, C.; Leroy, V. Adjuvant Intraarterial Lipiodol or 131I-Lipiodol After Curative Treatment of Hepatocellular Carcinoma: A Prospective Randomized Trial. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2014, 55, 877–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jouneau, S.; Polard, E.; Vauléon, E.; Caulet-Maugendre, S.; Volatron, A.C.; Delaval, P. 131I-labeled lipiodol-induced interstitial pneumonia. Respir. Med. CME 2011, 139, 1463–1469. [Google Scholar] [CrossRef]
- Lepareur, N.; Lacœuille, F.; Bouvry, C.; Hindré, F.; Garcion, E.; Chérel, M.; Noiret, N.; Garin, E.; Knapp, F.F.R., Jr. Rhenium-188 Labeled Radiopharmaceuticals: Current Clinical Applications in Oncology and Promising Perspectives. Front. Med. 2019, 6, 132. [Google Scholar] [CrossRef] [Green Version]
- Sundram, F.; Chau, T.C.; Onkhuudai, P.; Bernal, P.; Padhy, A.K. Preliminary results of transarterial rhenium-188 HDD lipiodol in the treatment of inoperable primary hepatocellular carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2004, 31, 250–257. [Google Scholar] [CrossRef]
- Bernal, P.; Raoul, J.L.; Vidmar, G.; Sereegotov, E.; Sundram, F.X.; Kumar, A.; Jeong, J.M.; Pusuwan, P.; Divgi, C.; Zanzonico, P.; et al. Intra-arterial rhenium-188 lipiodol in the treatment of inoperable hepatocellular carcinoma: Results of an IAEA-sponsored multination study. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 1448–1455. [Google Scholar] [CrossRef]
- Delaunay, K.; Edeline, J.; Rolland, Y.; Lepareur, N.; Laffont, S.; Palard, X.; Bouvry, C.; Le Sourd, S.; Pracht, M.; Ardisson, V.; et al. Preliminary results of the Phase 1 Lip-Re I clinical trial: Biodistribution and dosimetry assessments in hepatocellular carcinoma patients treated with Re-188-SSS Lipiodol radioembolization. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1506–1517. [Google Scholar]
- Boschi, A.; Uccelli, L.; Duatti, A.; Colamussi, P.; Cittanti, C.; Filice, A.; Rose, A.H.; Martindale, A.A.; Claringbold, P.G.; Kearney, D. A kit formulation for the preparation of 188Re-lipiodol: Preclinical studies and preliminary therapeutic evaluation in patients with unresectable hepatocellular carcinoma. Nucl. Med. Commun. 2004, 25, 691–699. [Google Scholar] [CrossRef]
- Ariel, I.M. Treatment of Inoperable Primary Pancreatic and Liver Cancer by the Intra-Arterial Administration of Radioactive Isotopes (Y Radiating Microspheres). Ann. Surg. 1965, 162, 267. [Google Scholar] [CrossRef]
- Okuda, K.; Ohnishi, K.; Kimura, K.; Matsutani, S.; Sumida, M.; Goto, N.; Musha, H.; Takashi, M.; Suzuki, N.; Shinagawa, T. Incidence of portal vein thrombosis in liver cirrhosis. An angiographic study in 708 patients. Gastroenterology 1985, 89, 279. [Google Scholar] [CrossRef]
- Xing, M.; Prajapati, H.J.; Dhanasekaran, R.; Lawson, D.H.; Kokabi, N.; Eaton, B.R.; Kim, H.S. Selective Internal Yttrium-90 Radioembolization Therapy (Y-90-SIRT) Versus Best Supportive Care in Patients With Unresectable Metastatic Melanoma to the Liver Refractory to Systemic Therapy Safety and Efficacy Cohort Study. Am. J. Clin. Oncol. Cancer Clin. Trials 2017, 40, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Lewandowski, R.J.; Kulik, L.M.; Riaz, A.; Senthilnathan, S.; Salem, R. A comparative analysis of transarterial downstaging for hepatocellular carcinoma: Chemoembolization versus radioembolization. Am. J. Transplant. 2010, 9, 1920–1928. [Google Scholar] [CrossRef] [PubMed]
- Memon, K.; Lewandowski, R.J.; Riaz, A.; Salem, R. Yttrium 90 microspheres for the treatment of hepatocellular carcinoma. Recent Results Cancer Res. 2013, 190, 207–224. [Google Scholar]
- Kallini, J.R.; Gabr, A.; Salem, R.; Lewandowski, R.J. Transarterial Radioembolization with Yttrium-90 for the Treatment of Hepatocellular Carcinoma. Adv. Ther. 2016, 33, 699–714. [Google Scholar] [CrossRef] [Green Version]
- Lewandowski, R.; Salem, R. Yttrium-90 radioembolization of hepatocellular carcinoma and metastatic disease to the liver. Semin. Interv. Radiol. 2006, 23, 64–72. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.M.; Salem, R.; Bui, J.T.; Courtney, A.; Barakat, O.; Sergie, Z.; Atassi, B.; Barrett, K.; Gowland, P.; Oman, B. Angiographic Considerations in Patients Undergoing Liver-directed Therapy. J. Vasc. Interv. Radiol. 2005, 16, 911–935. [Google Scholar] [CrossRef]
- Hilgard, P.; Hamami, M.; Fouly, A.E.; Scherag, A.; Müller, S.; Ertle, J.; Heusner, T.; Cicinnati, V.R.; Paul, A.; Bockisch, A.; et al. Radioembolization with yttrium-90 glass microspheres in hepatocellular carcinoma: European experience on safety and long-term survival. Hepatology 2010, 52, 1741–1749. [Google Scholar] [CrossRef]
- D’Avola, D.; Larrairaegui, M.; Bilbao, J.I.; Martinez-Cuesta, A.; Sangro, B. A retrospective comparative analysis of the effect of Y90-radioembolization on the survival of patients with unresectable hepatocellular carcinoma. Hepatogastroenterology 2009, 56, 1683–1688. [Google Scholar]
- Thornburg, B.; Mora, R.A.; Baker, T.; Borja-Cacho, D.; Katariya, N.; Ladner, D.P.; Caicedo, J.C.; Lewandowski, R.J.; Salem, R.; Alasadi, A. Liver Transplantation Following Yttrium-90 Radioembolization: 15-Year Experience in 207-Patient Cohort. Hepatology 2021, 73, 998–1010. [Google Scholar]
- Levi Sandri, G.B.; Ettorre, G.M.; Giannelli, V.; Colasanti, M.; Sciuto, R.; Pizzi, G.; Cianni, R.; D’Offizi, G.; Antonini, M.; Vennarecci, G.; et al. Trans-arterial radio-embolization: A new chance for patients with hepatocellular cancer to access liver transplantation, a world review. Transl. Gastroenterol. Hepatol. 2017, 2, 98. [Google Scholar] [CrossRef] [Green Version]
- Ozkan, Z.G.; Poyanli, A.; Ucar, A.; Kuyumcu, S.; Akyuz, F.; Keskin, S.; Saglam, S.; Yilmaz, E.; Karaca, C.; Turkmen, C. Favorable survival time provided with radioembolization in hepatocellular carcinoma patients with and without portal vein thrombosis. Cancer Biother. Radiopharm. 2015, 30, 132–138. [Google Scholar] [CrossRef]
- Iñarrairaegui, M.; Thurston, K.G.; Bilbao, J.I.; D’Avola, D.; Rodriguez, M.; Arbizu, J.; Martinez-Cuesta, A.; Sangro, B. Radioembolization with use of yttrium-90 resin microspheres in patients with hepatocellular carcinoma and portal vein thrombosis. J. Vasc. Interv. Radiol. 2010, 21, 1205–1212. [Google Scholar] [CrossRef]
- Ricke, J.; Klumpen, H.J.; Amthauer, H.; Bargellini, I.; Malfertheiner, P. Impact of combined selective internal radiation therapy and sorafenib on survival in advanced hepatocellular carcinoma. J. Hepatol. 2019, 71, 1164–1174. [Google Scholar] [CrossRef]
- Wehrenberg-Klee, E.; Goyal, L.; Dugan, M.; Zhu, A.X.; Ganguli, S. Y-90 Radioembolization Combined with a PD-1 Inhibitor for Advanced Hepatocellular Carcinoma. CardioVascular Interv. Radiol. 2018, 41, 1799–1802. [Google Scholar] [CrossRef]
- Salem, R.; Gordon, A.C.; Mouli, S.; Hickey, R.; Kallini, J.; Gabr, A.; Mulcahy, M.F.; Baker, T.; Abecassis, M.; Miller, F. Y90 Radioembolization Significantly Prolongs Time to Progression Compared With Chemoembolization in Patients WithHepatocellular Carcinoma. Gastroenterology 2016, 151, 1155–1163. [Google Scholar] [CrossRef]
- Salem, R.; Lewandowski, R.J.; Kulik, L.; Wang, E.; Riaz, A.; Ryu, R.K.; Sato, K.T.; Gupta, R.; Nikolaidis, P.; Miller, F.H. Radioembolization Results in Longer Time-to-Progression and Reduced Toxicity Compared With Chemoembolization in Patients With Hepatocellular Carcinoma. Gastroenterology 2011, 140, 497–507.e492. [Google Scholar] [CrossRef] [Green Version]
- Chow, P.; Gandhi, M.; Tan, S.B.; Khin, M.W.; Soo, K.C. SIRveNIB: Selective Internal Radiation Therapy Versus Sorafenib in Asia-Pacific Patients With Hepatocellular Carcinoma. J. Clin. Oncol. 2018, 36, 1913–1921. [Google Scholar]
- Vilgrain, V.; Pereira, H.; Assenat, E.; Guiu, B.; Ilonca, A.D.; Pageaux, G.-P.; Sibert, A.; Bouattour, M.; Lebtahi, R.; Allaham, W.; et al. Efficacy and safety of selective internal radiotherapy with yttrium-90 resin microspheres compared with sorafenib in locally advanced and inoperable hepatocellular carcinoma (SARAH): An open-label randomised controlled phase 3 trial. Lancet Oncol. 2017, 18, 1624–1636. [Google Scholar] [CrossRef]
- Sangro, B.; Gil-Alzugaray, B.; Rodriguez, J.; Sola, I.; Bilbao, J.I. Liver disease induced by radioembolization of liver tumors: Description and possible risk factors. Cancer 2008, 112, 1538–1546. [Google Scholar]
- Young, J.Y.; Rhee, T.K.; Atassi, B.; Gates, V.L.; Kulik, L.; Mulcahy, M.F.; Larson, A.C.; Ryu, R.K.; Sato, K.T.; Lewandowski, R.J. Radiation Dose Limits and Liver Toxicities Resulting from Multiple Yttrium-90 Radioembolization Treatments for Hepatocellular Carcinoma. J. Vasc. Interv. Radiol. 2007, 18, 1375–1382. [Google Scholar] [CrossRef]
- Salem, R.; Parikh, P.; Atassi, B.; Lewandowski, R.J.; Ryu, R.K.; Sato, K.T.; Gates, V.L.; Ibrahim, S.; Mulcahy, M.F.; Kulik, L. Incidence of radiation pneumonitis after hepatic intra-arterial radiotherapy with yttrium-90 microspheres assuming uniform lung distribution. Am. J. Clin. Oncol. 2008, 31, 431–438. [Google Scholar] [CrossRef]
- Rhee, T.K.; Naik, N.K.; Deng, J.; Atassi, B.; Mulcahy, M.F.; Kulik, L.M.; Ryu, R.K.; Miller, F.H.; Larson, A.C.; Salem, R. Tumor Response after Yttrium-90 Radioembolization for Hepatocellular Carcinoma: Comparison of Diffusion-weighted Functional MR Imaging with Anatomic MR Imaging. J. Vasc. Interv. Radiol. 2008, 19, 1180–1186. [Google Scholar] [CrossRef]
- Kallini, J.R.; Gabr, A.; Thorlund, K.; Balijepalli, C.; Ayres, D.; Kanters, S.; Ebrahim, S.; Mills, E.; Lewandowski, R.J.; Salem, R. Comparison of the Adverse Event Profile of TheraSphere® with SIR-Spheres® for the Treatment of Unresectable Hepatocellular Carcinoma: A Systematic Review. Cardiovasc. Interv. Radiol. 2017, 40, 1033–1043. [Google Scholar] [CrossRef]
- Reinders, M.T.M.; Smits, M.L.J.; van Roekel, C.; Braat, A.J.A.T. Holmium-166 Microsphere Radioembolization of Hepatic Malignancies. Semin. Nucl. Med. 2019, 49, 237–243. [Google Scholar] [CrossRef]
- Smits, M.L.; Nijsen, J.F.; van den Bosch, M.A.A.J.; Lam, M.G.; Vente, M.A.; Mali, W.P.; van Het Schip, A.D.; Zonnenberg, B.A. Holmium-166 radioembolisation in patients with unresectable, chemorefractory liver metastases (HEPAR trial): A phase 1, dose-escalation study. Lancet Oncol. 2012, 13, 1025–1034. [Google Scholar] [CrossRef]
- Sohn, J.H.; Choi, H.J.; Lee, J.T.; Lee, J.D.; Kim, J.H.; Moon, Y.M.; Park, K.; Park, K.B.; Kim, E.; Yoo, N.C. Phase II Study of Transarterial Holmium-166-Chitosan Complex Treatment in Patients with a Single, Large Hepatocellular Carcinoma. Oncology 2009, 76, 1–9. [Google Scholar] [CrossRef]
- Li, W.; Dai, Z.; Yao, L.; Luo, J.; Yan, Z. Chemoembolization and stenting combined with iodine-125 seed strands for the treatment of hepatocellular carcinoma with inferior vena cava obstruction. Exp. Ther. Med. 2015, 10, 973–977. [Google Scholar] [CrossRef]
- Li, S.; He, X.; Dang, L.; Xu, F.; Fang, J.; Li, F.; Wang, W. Efficacy of (125)I Versus Non-(125)I Combined with Transcatheter Arterial Chemoembolization for the Treatment of Unresectable Hepatocellular Carcinoma with Obstructive Jaundice. Dig. Dis. Sci. 2018, 63, 321–328. [Google Scholar] [CrossRef]
- Zhang, H.; Yang, A.; Zhang, J. Efficacy of transcatheter arterial chemoembolization combined with 125I seed implantation and three-dimensional conformal radiotherapy in advanced primary hepatocellular carcinoma. J. Buon. 2020, 25, 952–958. [Google Scholar]
- Fang, S.J.; Gao, R.J.; Zheng, L.Y.; Zhao, Z.W.; Fan, X.X.; Song, J.J.; Zhang, D.K.; Wu, F.Z.; Ji, J.S. Clinical value of (125)I radioactive seed implantation plus transcatheter arterial chemoembolization combined with radiofrequency ablation in treating patient with sub-capsular hepatocellular carcinoma. Chin. Med. J. 2018, 98, 3853–3857. [Google Scholar] [CrossRef]
- Chen, K.; Chen, G.; Wang, H.; Li, H.; Xiao, J.; Duan, X.; He, J.; He, K.; Xiang, G. Increased survival in hepatocellular carcinoma with iodine-125 implantation plus radiofrequency ablation: A prospective randomized controlled trial. J. Hepatol. 2014, 61, 1304–1311. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.Z.; Ji, J.S.; Ying, X.H.; Tu, J.F.; Zhao, Z.W.; Wu, X.L.; Yang, H.Y.; Zhang, D.K.; Chen, L.; Song, J.J. [Efficacy analysis of radiofrequency ablation combined with (125)I seed for multiple nodular hepatocellular carcinoma]. Chin. Med. J. 2016, 96, 693. [Google Scholar]
- Chen, K.; Xia, Y.; Wang, H.; Xiao, F.; Xiang, G.; Feng, S. Adjuvant Iodine-125 Brachytherapy for Hepatocellular Carcinoma after Complete Hepatectomy: A Randomized Controlled Trial. PLoS ONE 2013, 8, e57397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Hu, B.; Li, W.; Huang, P.; Zhang, S.; Zhong, B.; Ni, C. 125I Irradiation Stent for Hepatocellular Carcinoma with Main Portal Vein Tumor Thrombosis: A Systematic Review. Cardiovasc. Interv. Radiol. 2020, 43, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Hao, P.P.; Liu, Y.P.; Yang, C.Y.; Liang, T.; Chao, Z.; Song, J.; Han, J.K.; Hou, G.H.; Mitchell, H. Evaluation of 131I-Anti-Angiotensin II Type 1 Receptor Monoclonal Antibody as a Reporter for Hepatocellular Carcinoma. PLoS ONE 2014, 9, e85002. [Google Scholar] [CrossRef]
- Street, H.H.; Goris, M.L.; Fisher, G.A.; Wessels, B.W.; Cho, C.; Hernandez, C.; Zhu, H.J.; Zhang, Y.; Nangiana, J.S.; Shan, J.S.; et al. Phase I study of 131I-chimeric(ch) TNT-1/B monoclonal antibody for the treatment of advanced colon cancer. Cancer Biother Radiopharm. 2006, 21, 243–256. [Google Scholar] [CrossRef]
- Wu, L.; Yang, Y.F.; Ge, N.J.; Shen, S.Q.; Liang, J.; Wang, Y.; Zhou, W.P.; Shen, F.; Wu, M.C. Hepatic arterial iodine-131-labeled metuximab injection combined with chemoembolization for unresectable hepatocellular carcinoma: Interim safety and survival data from 110 patients. Cancer Biother. Radiopharm. 2010, 25, 657. [Google Scholar] [CrossRef]
- Chen, Z.-N.; Mi, L.; Xu, J.; Song, F.; Zhang, Q.; Zhang, Z.; Xing, J.-L.; Bian, H.-J.; Jiang, J.-L.; Wang, X.-H.; et al. Targeting radioimmunotherapy of hepatocellular carcinoma with iodine (131I) metuximab injection: Clinical Phase I/II trials. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 435–444. [Google Scholar] [CrossRef]
- Ma, J.; Wang, J.H. 131I-Labeled-Metuximab Plus Transarterial Chemoembolization in Combination Therapy for Unresectable Hepatocellular Carcinoma: Results from a Multicenter Phase IV Clinical Study. Asian Pac. J. Cancer Prev. 2015, 16, 7441–7447. [Google Scholar] [CrossRef]
- He, Q.; Lu, W.S.; Liu, Y.; Guan, Y.S.; Kuang, A.R. 131I-labeled metuximab combined with chemoembolization for unresectable hepatocellular carcinoma. World J. Gastroenterol. 2013, 19, 9104–9110. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Shen, Z.Y.; Chen, X.G.; Zhang, Q.; Bian, H.J.; Zhu, P.; Xu, H.Y.; Song, F.; Yang, X.M.; Mi, L.; et al. A randomized controlled trial of Licartin for preventing hepatoma recurrence after liver transplantation. Hepatology 2007, 45, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Bian, H.; Zheng, J.S.; Nan, G.; Li, R.; Chen, C.; Hu, C.X.; Zhang, Y.; Sun, B.; Wang, X.L.; Cui, S.C.; et al. Randomized trial of [131I] metuximab in treatment of hepatocellular carcinoma after percutaneous radiofrequency ablation. J. Natl. Cancer Inst. 2014, 106, dju239. [Google Scholar] [CrossRef] [Green Version]
- Tu, J.; Ji, J.; Wu, F.; Zhang, D.; Ying, X.; Zhao, Z. [Efficacies of 131I-chTNT plus radiofrequency ablation for the treatment of advanced hepatocellular carcinoma. Chin. Med. J. 2014, 94, 3586–3588. [Google Scholar]
- Ru, N.Y.; Wu, J.; Chen, Z.N.; Bian, H. HAb18G/CD147 is involved in TGF-β-induced epithelial-mesenchymal transition and hepatocellular carcinoma invasion. Cell Biol. Int. 2015, 39, 44–51. [Google Scholar] [CrossRef]
- Chen, S.; Li, B.; Xie, H.; Xu, L.; Niu, G.; Fan, K.; Fan, Q. Phase I clinical trial of targeted therapy using 131I-Hepama-1 mAb in patients with hepatocellular carcinoma. Cancer Biother Radiopharm. 2004, 19, 589–600. [Google Scholar] [CrossRef]
Figure 1.
Adjuvant intra-arterial injection of iodine-131-labeled lipiodol after resection of HCC. (A) Disease-free survival of patients in the 2 treatment groups (p < 0.02). (B) Overall survival of patients in the 2 treatment groups (p < 0.02). Adapted with permission from [32].
Figure 1.
Adjuvant intra-arterial injection of iodine-131-labeled lipiodol after resection of HCC. (A) Disease-free survival of patients in the 2 treatment groups (p < 0.02). (B) Overall survival of patients in the 2 treatment groups (p < 0.02). Adapted with permission from [32].

Figure 2.
Radioembolization with yttrium-90 glass microspheres in hepatocellular carcinoma. (A) TTP (with progression defined according to RECIST with the recent NCI amendments) in 76 of 108 HCC patients treated by Y-90 glass microsphere radioembolization for which radiological response data were available. The solid line displays the Kaplan–Meier estimator, with marks representing censored events. The shaded area marks the limits of the pointwise 95% CIs. (B) Overall survival in 108 HCC patients treated by Y-90 glass microsphere radioembolization. The solid line displays the Kaplan–Meier estimator, with marks representing censored events. The shaded area marks the limits of the pointwise 95% CIs. Adapted with permission from [48].
Figure 2.
Radioembolization with yttrium-90 glass microspheres in hepatocellular carcinoma. (A) TTP (with progression defined according to RECIST with the recent NCI amendments) in 76 of 108 HCC patients treated by Y-90 glass microsphere radioembolization for which radiological response data were available. The solid line displays the Kaplan–Meier estimator, with marks representing censored events. The shaded area marks the limits of the pointwise 95% CIs. (B) Overall survival in 108 HCC patients treated by Y-90 glass microsphere radioembolization. The solid line displays the Kaplan–Meier estimator, with marks representing censored events. The shaded area marks the limits of the pointwise 95% CIs. Adapted with permission from [48].


{kind=link}
{kind=link}
Table 1.
Properties of radionuclides commonly used for TARE.
| Radionuclides | Ray Species | Half-Life (Days) | Mean Tissue Penetration Depth (mm) |
|---|---|---|---|
| 131I | γ, β- | 8.04 | 0.4 |
| 90Y | β- | 2.7 | 3 |
| 188Re | γ, β- | 0.708 | 4.8 |
| 166Ho | γ, β- | 1.116 | 2.5 |
| 125I | X-ray, γ | 60.1 | 20 |
Table 2.
Advances for treatment of HCC using 131I-lipiodol TARE.
| Author | Year | Experiment Type | Design | Number of Patients | Conclusion | Refs. |
|---|---|---|---|---|---|---|
| Jean-Luc Raoul | 1997 | Random control | 131I-Lipiodol vs. TACE | 129 | Better tolerance, but no significant difference in OS | [29] |
| J-L Raoul | 2003 | Retrospective analysis | Use 131I-lipiodol before surgery | 34 | Tolerability and tumor response were good | [31] |
| Eveline Boucher | 2003 | Retrospective analysis | 131I-Lipiodol after surgery vs. surgery | 38 | DFS and OS were better than the control group | [32] |
| Stéphane J Juneau | 2011 | Retrospective analysis | 131I-Lipiodol treating induced interstitial lung disease for HCC | 1000 | Of 15 people with interstitial pneumonia, 12 died | [34] |
| Alina Lintia-Gaultier | 2013 | Retrospective comparative analysis | 131I-Lipiodol vs. medical support | 86 | Overall survival (OS) was better than the control group | [28] |
| Jérôme Dumortier | 2014 | Random control | 131I-Lipiodol vs. lipiodol | 58 | Reduced postoperative recurrence, but no significant difference in OS | [33] |
Table 3.
Advances for the treatment of HCC with 188Re-lipiodol TARE.
| Author | Year | Experiment Type | Design | Number of Patients | Conclusion | Refs. |
|---|---|---|---|---|---|---|
| Felix Sundram | 2004 | Clinical Phase I | 188Re-HDD lipiodol treatment | 70 | Confirm dosage 98 GBq (265 mCi); Safe and minimal side effects | [35] |
| Patricia Bernal, MD | 2007 | Clinical Phase II | 188Re-HDD lipiodol treatment | 185 | Well-tolerated; 1-year survival rate of 46%, 2-year survival rate of 23% | [36] |
| Kostas Delaunay | 2019 | Clinical Phase I | 188Re-SSS lipiodol treatment | 6 | Good biodistribution and high stability in vivo | [37] |
Table 4.
Advances for the treatment of HCC with 90Y-microspheres TARE.
| Author | Year | Experiment Type | Design | Number of Patients | Conclusion | Refs. |
|---|---|---|---|---|---|---|
| Delia D’Avola | 2009 | Retrospective comparative analysis | 90Y-microspheres vs. usual care | 78 | Median survival was significantly higher than the usual care | [49] |
| Philip Hilgard | 2010 | Random control | 90Y-glass microspheres for advanced HCC and liver cirrhosis | 108 | Comparable efficacy to systemic therapy | [48] |
| Mercedes Inarrairaegui | 2010 | Retrospective analysis | 90Y-microspheres TARE for HCC with PVT | 25 | Well-tolerated, favorable median survival | [53] |
| Riad Salem | 2011 | Retrospective analysis | 90Y-microspheres TARE vs. TACE | 245 | The 90Y group showed an extended progression time, with no significant difference in the median survival | [57] |
| Zeynep Gozde Ozkan | 2015 | Retrospective analysis | 90Y-microspheres TARE for HCC | 29 | The median survival time of patients with HCC was unaffected | [52] |
| Giovanni Battista Levi Sandri | 2017 | Retrospective analysis | 90Y-microspheres TARE before transplantation | 178 | 90Y TARE was better than TACE | [51] |
| Riad Salem | 2016 | Random control | 90Y-microspheres TARE vs. TACE | 179 | 90Y group had a longer median progress time | [56] |
| Valérie Vilgrain | 2017 | Clinical Phase III | 90Y-microspheres TARE vs. sorafenib | 467 | No significant difference in OS | [59] |
| Joseph Ralph Kallini | 2017 | Retrospective comparative analysis | 90Y-resin microspheres or 90Y-glass microspheres for HCC | 2299 | Glass microspheres in HCC treatment of gastrointestinal tract and lungs a lower incidence of adverse events | [64] |
| Eric Wehrenberg-Klee | 2018 | Case report | 90Y-microspheres TARE + PD-1 | 1 | Successful bridge partial liver resection surgery | [55] |
| Pkh Chow | 2018 | Clinical Phase III | 90Y-microspheres TARE vs. sorafenib | 360 | No significant difference in OS | [58] |
| Jens Ricke | 2019 | Random control | 90Y-resin microspheres + sorafenib vs. sorafenib | 424 | Combination therapy did not significantly improve the patients’ survival | [54] |
| Ahmed Gabr | 2021 | prospective study | Treatment with 90Y-microspheres adjuvant before liver transplantation | 207 | Support 90Y as a neoadjuvant therapy for bridging or decreasing staging before liver transplantation | [50] |
Table 5.
Advances for the treatment of HCC using 125I seed implantation.
| Author | Year | Experiment Type | Design | Number of Patients | Conclusion | Refs. |
|---|---|---|---|---|---|---|
| Kaiyun Chen | 2013 | Random control | After HCC, 125I seed implantation vs. medical support | 68 | Disease-free survival and OS were prolonged in the experimental group | [74] |
| Kaiyun Chen | 2014 | Random control | RFA +125I seed implantation vs. RFA | 136 | The survival rate of the RFA + 125I group was significantly better than that of the RFA group | [72] |
| F Z Wu | 2016 | Random control | RFA + 125I seed implantation vs. RFA | 47 | No significant difference in OS | [73] |
| S J Fang | 2019 | Retrospective comparative analysis | 125I seed implantation+ TACE + RFA vs. TACE + RFA | 76 | Safety and efficacy of three therapeutic modalities in combination | [68] |
| Lei Zhang | 2020 | Random control | Patient with HCC with PVT accepted the 125I seed implantation | 406 | 125I implantation is safe | [75] |
| Huanyun Zhang | 2020 | Random control | TACE + 125I seed implantation + 3D conformal radiotherapy vs. TACE + 3D conformal radiotherapy | 110 | Overall and progression-free survival were significantly prolonged | [70] |
Table 6.
Advances in radioimmunotherapy for the treatment of HCC.
| Author | Year | Experiment Type | Design | Number of Patients | Conclusion | Refs. |
|---|---|---|---|---|---|---|
| Chen S | 2004 | Clinical Phase I | For patients with unresectable HCC give 131I-hepama-1 MAb | 45 | The recommended dose for clinical use is 1480–2960 MBq/10 mg | [86] |
| Zhi-Nan Chen | 2006 | Clinical Phase I | 131I-metuximab | 28, 106 | Safe dosage 27.75 MBq/kg; the survival rate of 21 months was 4454 | [79] |
| Jing Xu | 2007 | Random control | Post-transplant,131I-metuximab vs. placebo | 60 | The recurrence rate decreased while the survival rate increased | [82] |
| He Q | 2013 | Nonrandomized prospective cohort study | 131I-metuximab + TACE vs. TACE | 185 | The survival time of the patients in the combined treatment group was prolonged | [81] |
| Bian H | 2014 | Random control | Follow-up with 131I-metuximab after RFA treatment vs. RFA | 127 | Follow-up of 131I cetuximab after RFA treatment helped prevent postoperative recurrence | [83] |
| Tu J | 2014 | Retrospective comparative analysis | RFA+131I-chTNT vs. RFA | 38 | Combination therapy extended the disease-free survival of patients | [74] |
| Ma J | 2015 | Clinical Phase IV | 131I-Metoximab + TACE vs. TACE | 341 | The 1-year survival and progression time of the experimental group were longer than those of the control group | [80] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Liu, R.; Li, H.; Qiu, Y.; Liu, H.; Cheng, Z. Recent Advances in Hepatocellular Carcinoma Treatment with Radionuclides. Pharmaceuticals 2022, 15, 1339. https://doi.org/10.3390/ph15111339
AMA Style
Liu R, Li H, Qiu Y, Liu H, Cheng Z. Recent Advances in Hepatocellular Carcinoma Treatment with Radionuclides. Pharmaceuticals. 2022; 15(11):1339. https://doi.org/10.3390/ph15111339
Chicago/Turabian StyleLiu, Ruiqi, Hong Li, Yihua Qiu, Hongguang Liu, and Zhen Cheng. 2022. "Recent Advances in Hepatocellular Carcinoma Treatment with Radionuclides" Pharmaceuticals 15, no. 11: 1339. https://doi.org/10.3390/ph15111339
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.