
Research on Medical Security System Based on Zero Trust
Abstract
:1. Introduction
2. Related Work
2.1. Research Background
2.2. Technical Background
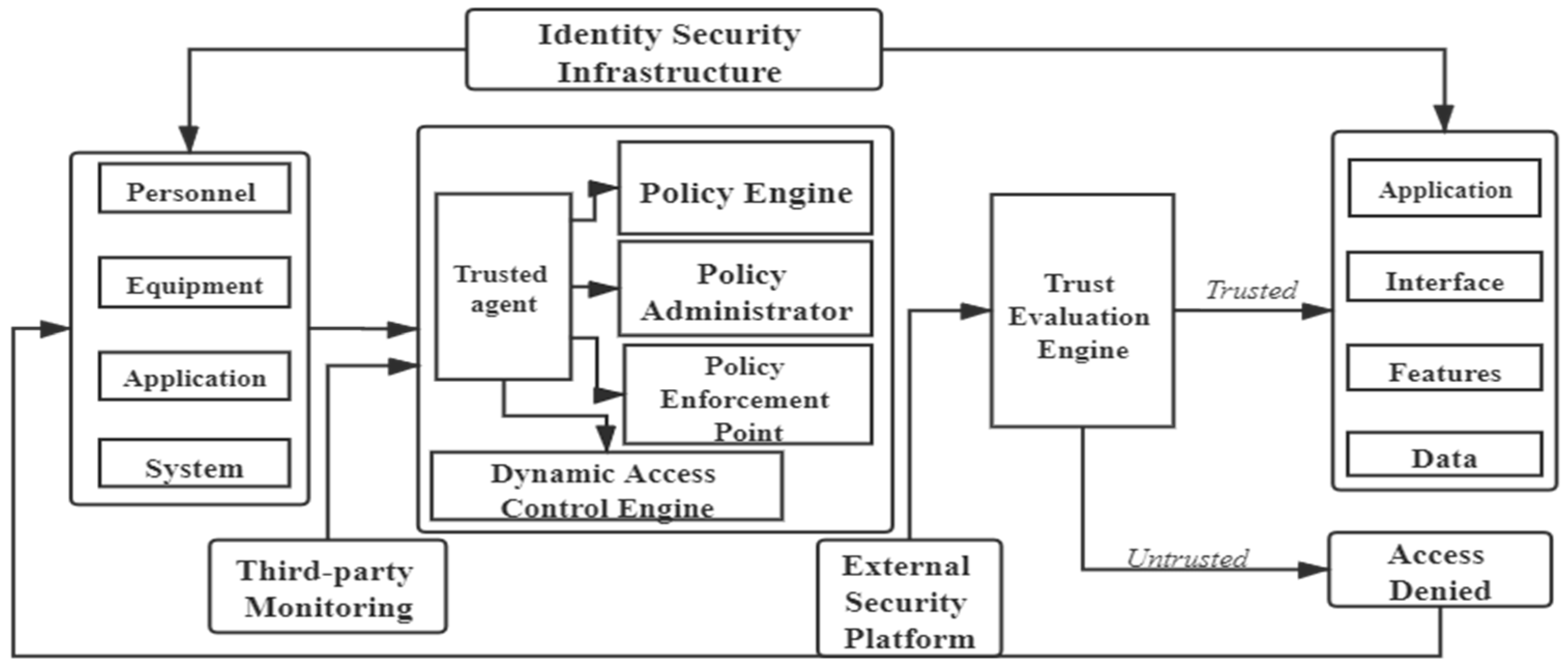
2.2.1. Zero-Trust Security Model
2.2.2. Access Control Model
2.2.3. TMBRE Model
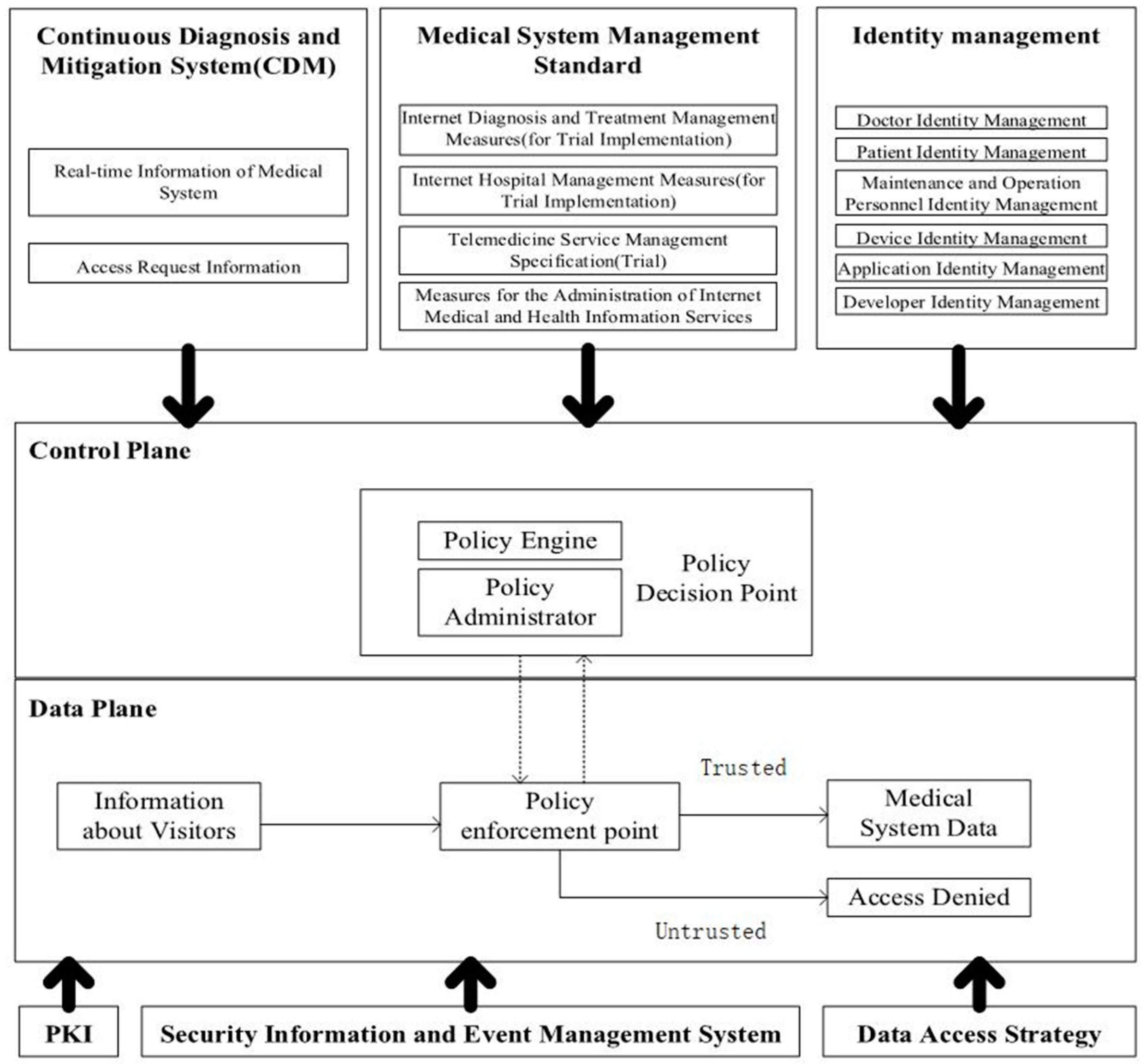
3. Medical Equipment Cyberspace Security System Based on Zero Trust
3.1. System Construction
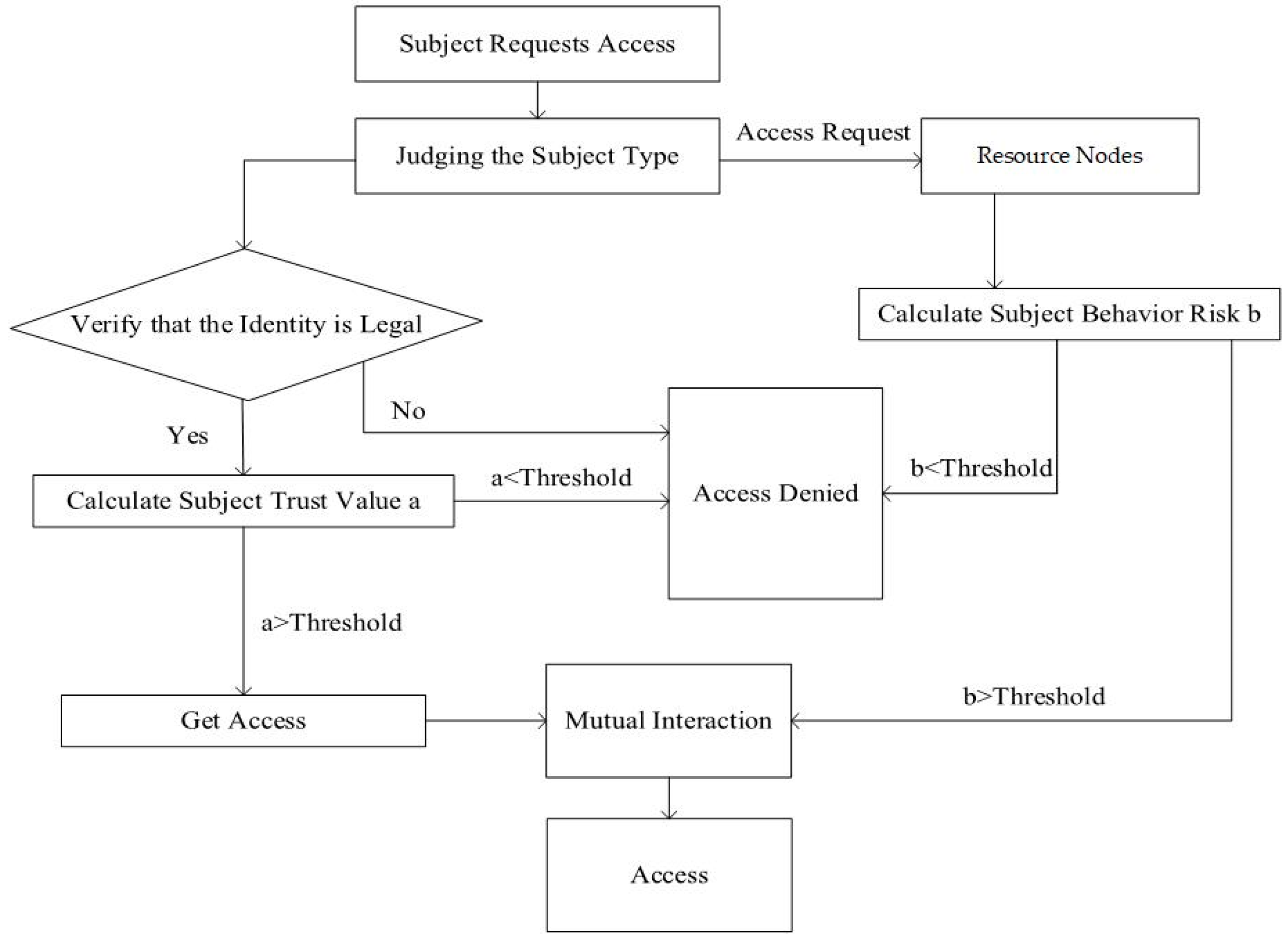
3.2. Dynamic Authentication Process
3.3. Trust Calculation
3.3.1. Calculation of User Behavior Risk Value
3.3.2. User Trust Calculation Formula
4. Simulation
4.1. Experimental Data
4.2. Analysis of the Relationship between User Behavior Risk and User Trust
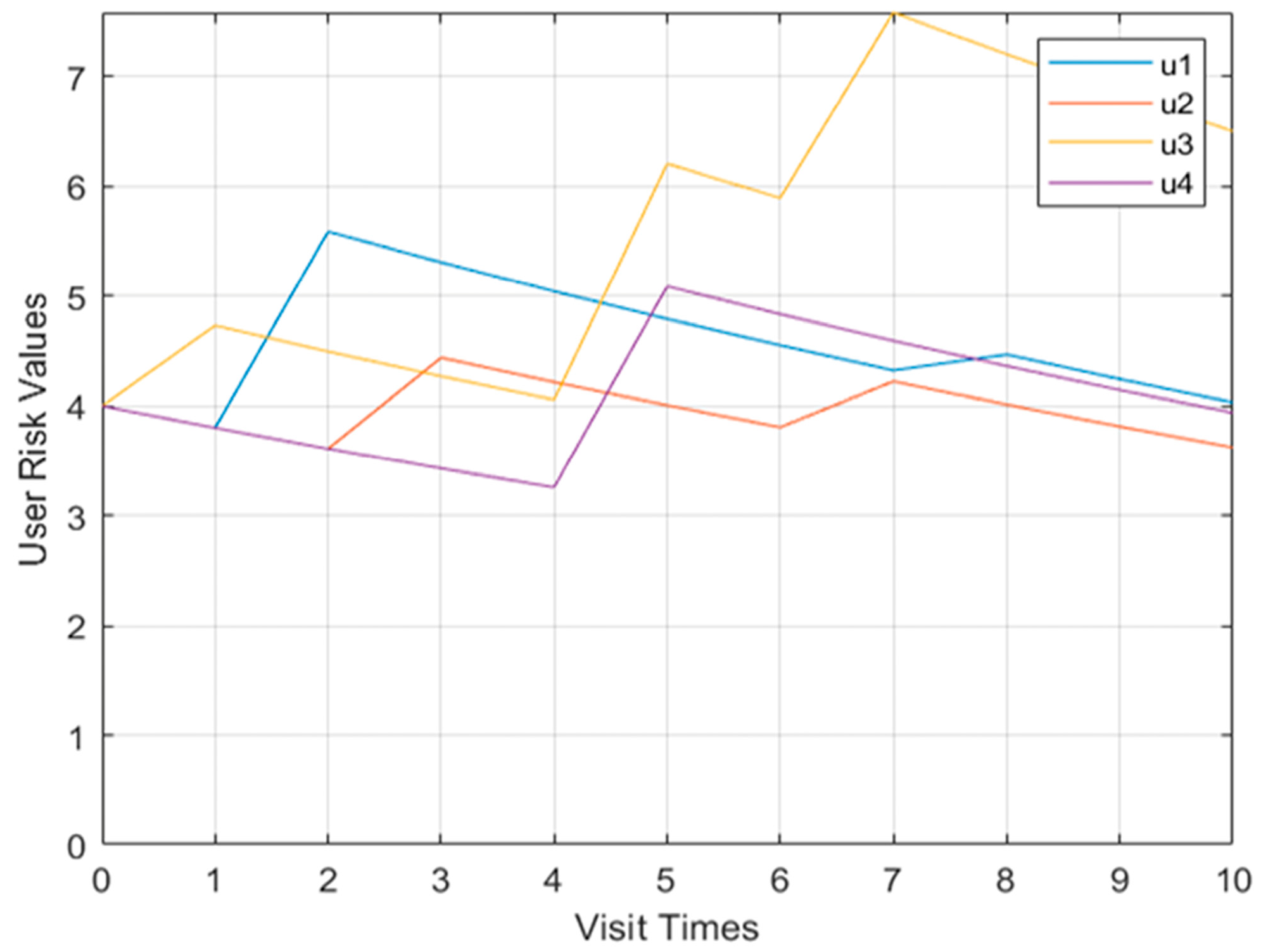
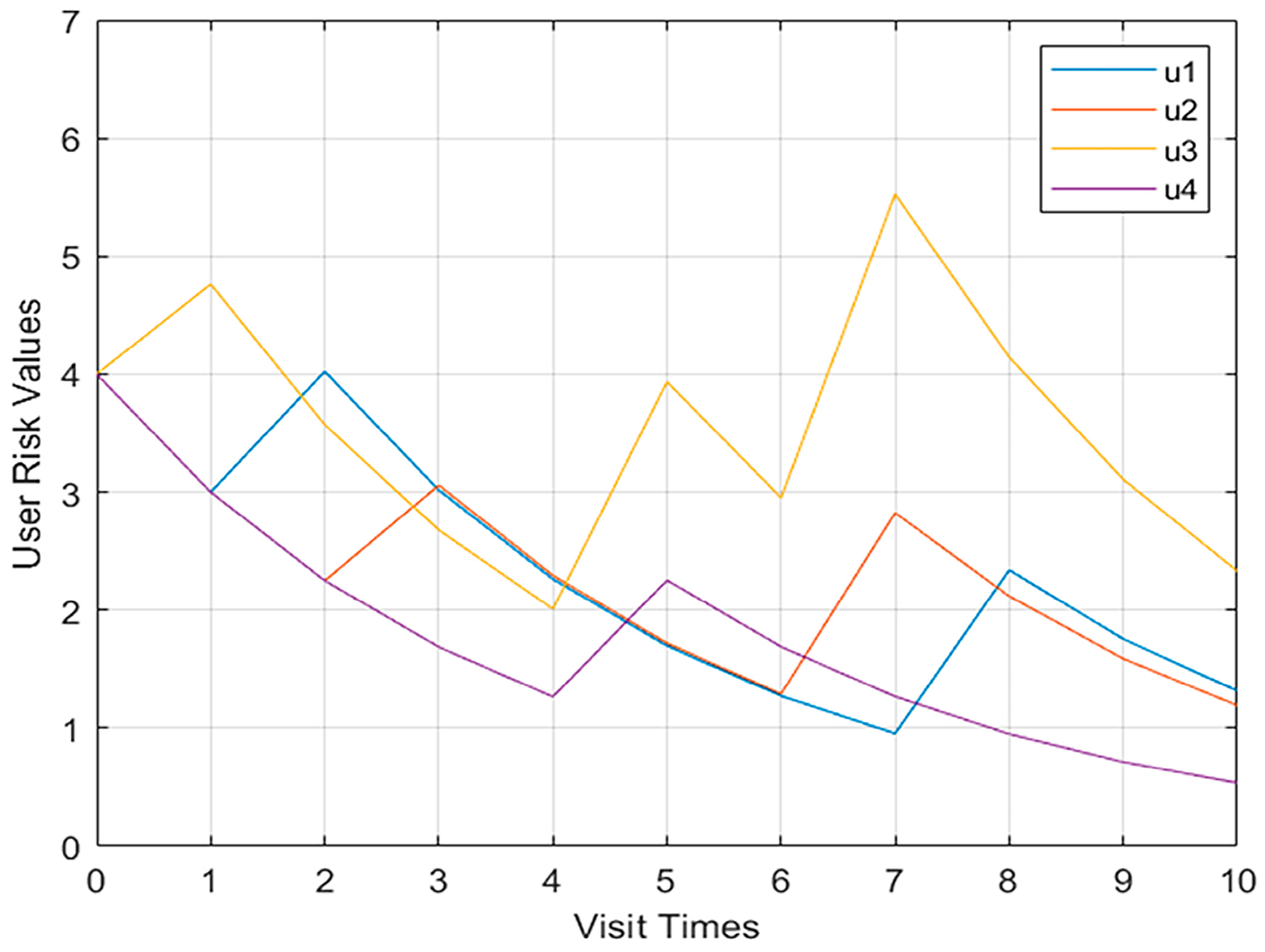
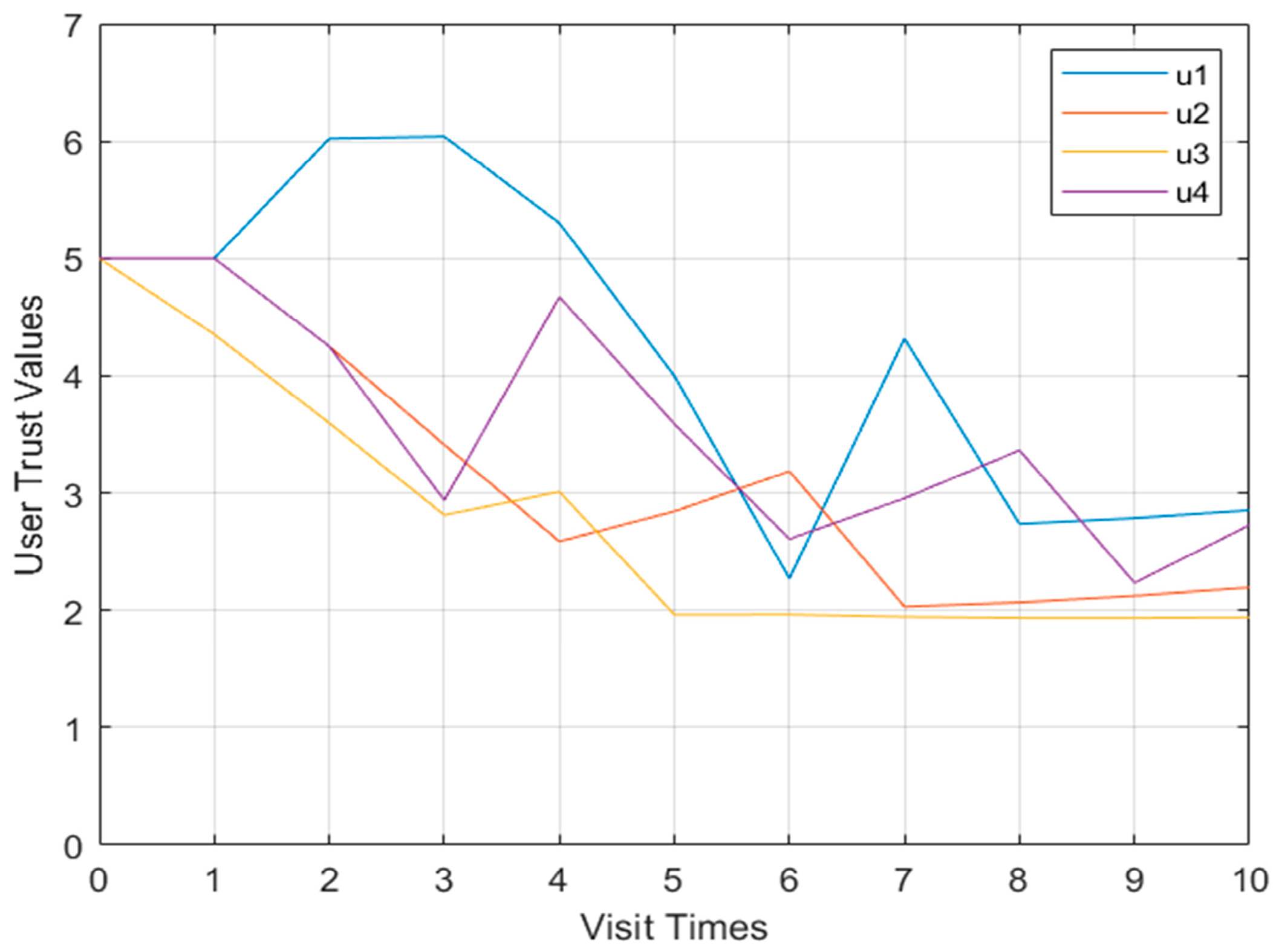
4.3. Analysis of the Relationship between Multi-User Behavior Risk and Trust
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yang, H.; Li, J.Q.; Li, X.Z.; Huang, Z.; Wu, Y. Build Internet plus health care innovation service mode–create new experience for outpatients' medical treatment. Med. Theory Pract. 2021, 34, 717–719. [Google Scholar]
- Tencent Smart Security. Medical Industry Blackmail Virus Project. Available online: https://s.tencent.com/research/report/535.html (accessed on 10 March 2023).
- Liu, Y.Z.; Hao, X.H.; Ren, W.; Xiong, R.T.; Zhu, T.Q.; Choo, K.K.R.; Min, G. A blockchain-based decentralized, fair and authenticated in formation sharing scheme in zero trust internet-of-things. IEEE Trans. Comput. 2023, 72, 501–512. [Google Scholar] [CrossRef]
- Xie, L.J.; Hang, F.L.; Guo, W.; Lv, Y.; Chen, H. A micro-segmentation protection scheme based on zero trust architecture. In Proceedings of the ISCTT 2021, 6th International Conference on Information Science, Computer Technology and Transportation, Xishuangbanna, China, 26–28 November 2021; pp. 1–4. [Google Scholar]
- Zhang, P.F.; Tian, C.; Shang, T.; Liu, L.; Li, L.; Wang, W.; Zhao, Y.M. Dynamic access control technology based on zero-trust light verification network model. In Proceedings of the 2021 International Conference on Communications, Information System and Computer Engineering (CISCE), Beijing, China, 14–16 May 2021; pp. 712–715. [Google Scholar] [CrossRef]
- Chen, L.; Dai, Z.; Chen, M.; Li, N. Research on the security protection framework of power mobile internet services based on zero trust. In Proceedings of the 2021 6th International Conference on Smart Grid and Electrical Automation (ICSGEA), Kunming, China, 29–30 May 2021; pp. 65–68. [Google Scholar] [CrossRef]
- Fang, W.; Guan, X. Research on iOS remote security access technology based on zero trust. In Proceedings of the 2022 IEEE 6th Information Technology and Mechatronics Engineering Conference (ITOEC), Chongqing, China, 4–6 March 2022; pp. 238–241. [Google Scholar] [CrossRef]
- Vallathan, G.; Rajamani, V.; Harinee, M.P. Enhanced medical data security and perceptual quality for healthcare services. In Proceedings of the 2020 International Conference on System, Computation, Automation and Networking (ICSCAN), Pondicherry, India, 3–4 July 2020; pp. 1–6. [Google Scholar] [CrossRef]
- Le, T.V.; Lu, C.F.; Hsu, C.L.; Do, T.K.; Chou, Y.F.; Wei, W.C. A novel three-factor authentication protocol for multiple service providers in 6G-aided intelligent healthcare systems. IEEE Access 2022, 10, 28975–28990. [Google Scholar] [CrossRef]
- Oh, H.; Yu, J.; Kim, N.; Kim, D.; Lee, J.; Yang, J. A federated binarized neural network model for constrained de vices in IoT healthcare services. In Proceedings of the 2022 International Conference on Artificial Intelligence in Information and Communication (ICAIIC), Jeju Island, Korea, 21–24 February 2022; pp. 241–245. [Google Scholar] [CrossRef]
- Sivasangari, A.; Sonti, V.J.K.K.; Ajitha, P.; Deepa, D.; Vignesh, R. Integrated security framework for healthcare using blockchain and fog computing. In Proceedings of the 2022 2nd International Conference on Power Electronics & IoT Applications in Renewable Energy and its Control (PARC), Mathura, India, 21–22 January 2022; pp. 1–5. [Google Scholar] [CrossRef]
- Campbell, M. Beyond zero trust: Trust is a vulnerability. Computer 2020, 53, 110–113. [Google Scholar] [CrossRef]
- Tian, X.P.; Song, H.H. A zero trust method based on BLP and BIBA model. In Proceedings of the 2021 14th International Symposium on Computational Intelligence and Design (ISCID), Hangzhou, China, 11–12 December 2021; pp. 96–100. [Google Scholar] [CrossRef]
- Khan, M.F.F.; Sakamura, K. A context-policy-based approach to access control for health care data protection. In Proceedings of the 2020 International Computer Symposium (ICS), Tainan, Taiwan, 17–19 December 2020; pp. 420–425. [Google Scholar] [CrossRef]
- Miao, Y.; Sun, Y.; Chen, X.J.; Song, W. Implementation of fine-grained mandatory access control mechanism for multi-source object relational database. Comput. Appl. Softw. 2021, 38, 14–21+55. [Google Scholar]
- Yang, F.J.; Ding, T.; Fu, M.; Zhang, P.H.; Zhou, C. Research on authority complexity and reliability control model based on RBAC. Comput. Appl. Softw. 2022, 39, 30–38+59. [Google Scholar]
- Zhang, R.L.; Wu, X.N.; Zhou, S.Y.; Dong, X.S. A trust model based on Entity Behavior Risk Assessment. Chin. J. Comput. 2009, 32, 688–698. [Google Scholar] [CrossRef]
- Wang, X.B. Network security solutions based on zero trust Architecture. Intell. Build. 2019, 223, 63–67. [Google Scholar]
- Amédée-Manesme, C.O.; Barthélémy, F. Ex-ante real estate value at risk calculation method. Ann. Oper. Res. 2018, 262, 257–285. [Google Scholar] [CrossRef] [Green Version]
- Jing, X.; Liu, Z.; Li, S.; Qiao, B.; Tan, G. A cloud-user behavior assessment based dynamic access control model. Int. J. Syst. Assur. Eng. Manag. 2017, 8, 1966–1975. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Notation | Description |
|---|---|
| The risk value | |
| The trust value | |
| The last recorded risk value | |
| The last recorded trust value | |
| The risk reduction factor | |
| The risk correction factor | |
| The threat coefficient | |
| The defect value of the asset | |
| The value of the asset | |
| The trust correction factor | |
| The trust correction factor | |
| The user behavior risk threshold constant | |
| α | The high-risk attenuation factor |
| CV | Medical data value |
| V | Vulnerability |
| TA | Threat behavior |
| Grade | Assignment | Describe |
|---|---|---|
| V | 8–9 | If used by threats, the damage to assets is very serious. |
| IV | 6–7 | If used by threats, serious damage to assets. |
| III | 4–5 | If used by threats, the damage to assets is generally serious. |
| II | 2–3 | If used by threats, the damage to assets is minimal. |
| I | 0–1 | If used by threats, the damage to assets can be ignored. |
| Grade | Assignment | Cloud Resources | Describe |
|---|---|---|---|
| V | 8–9 | Infrastructure | Infrastructure includes server pools, storage pools, etc. In the cloud system, the security attributes of these resources will cause very serious losses if they are destroyed. |
| IV | 6–7 | Systems software | System software includes an operating system, database, etc. In a cloud system, damage to the security attributes of these resources will cause more serious losses. |
| III | 4–5 | Shared data | Shared data include databases that need to share data. In a cloud system, the security attributes of these resources will cause moderate losses if they are compromised. |
| II | 2–3 | Application software | Application software includes common software such as OFFICE. In a cloud system, damage to the security attributes of these resources will cause a certain degree of loss. |
| I | 0–1 | Portal resources | Portal resources include daily information such as announcements. In a cloud system, the security attributes of these resources are destroyed, causing very little loss. |
| Grade | Assignment | Cloud Resources | Describe |
| III | 7–9 | Malicious security behavior | Malicious security behaviors include high-frequency applications for resources, attacks through Trojan horses, viruses, etc., which may bring huge security risks to the system and damage the system. |
| II | 4–6 | Breach of contract | Violation of agreement refers to the violation of the content of the cloud service level agreement, which may affect the normal operation of the system. |
| I | 0–3 | Abnormal behavior | Abnormal behavior includes abnormal operating habits, abnormal operating content, etc. The damage it causes to the system is small or even negligible. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Z.; Yu, X.; Xue, P.; Qu, Y.; Ju, L. Research on Medical Security System Based on Zero Trust. Sensors 2023, 23, 3774. https://doi.org/10.3390/s23073774
Wang Z, Yu X, Xue P, Qu Y, Ju L. Research on Medical Security System Based on Zero Trust. Sensors. 2023; 23(7):3774. https://doi.org/10.3390/s23073774
Chicago/Turabian StyleWang, Zhiqiang, Xinyue Yu, Peiyang Xue, Yunhan Qu, and Lei Ju. 2023. "Research on Medical Security System Based on Zero Trust" Sensors 23, no. 7: 3774. https://doi.org/10.3390/s23073774